

Abstract
Objectives:
To investigate perceptions and expectations of patients regarding hospital outpatient services by using a service quality gap model and factors influencing such gaps.
Methods:
In this cross-sectional descriptive study conducted between October and November 2014 in the outpatient waiting areas of a hospital in the Eastern Province of Saudi Arabia, a sample of 306 patients was selected by convenience sampling technique. The data was collected through an Arabic version of the service quality (SERVQUAL) questionnaire consisting of 2 parts: patients’ demographic characteristics, and 22 items scales of patients’ expectations and perceptions of SERVQUAL. The data was analyzed by confirmatory factor analysis, independent, and paired t samples tests and one way analysis of variance test.
Results:
The results showed that the proposed model for service quality dimensions had a good fit by satisfying the recommended values. The patients’ expectations exceeded perceptions in all service quality dimensions indicating statistically significant service quality gaps (t=26.3, p<0.000). Findings revealed that the empathy dimension contributed most patients’ expectations (4.7 ± 0.5) and perceptions (3.7 ± 0.8) scores, and responsiveness contributed least to expectations (4.5 ± 0.6) and perceptions (3.2 ± 0.8) scores. Prompt services showed highest service quality gap, while observation of privacy showed the smallest service quality gap in the statements. The study showed a significant association between gender, age, education, multiple visits, and service quality dimensions.
Conclusion:
The proposed model is valid and reliable and significant service quality gaps of all 5 dimensions need to be prioritized and addressed by focused improvement efforts of hospital management.
Healthcare management is under increasing pressure to demonstrate that their services are patient focused and directed to providing the best possible medical care for their patients. Therefore, it has become prudent for hospital management to understand and measure the patient’s perspectives, so that any perceived gap in delivery of service is identified and suitably addressed with constrained resources. A number of studies have been conducted to measure the service quality from the patient’s perspectives. Marković et al’s1 study conducted in a specialty hospital for rehabilitation in Croatia using 34 statements in each section of the service quality (SERVQUAL) questionnaire revealed that the patient’s expectations were higher than perceptions in all statements grouped in 4 service quality dimensions by exploratory factor analysis. Al-Borie and Damanhouri’s2 study conducted on inpatients in private and public hospitals identified that the association between demographic factors, except age, with service quality was satisfactory. Yesilada and Direktor3 showed that the service quality gap in all 3 service quality dimensions in a private hospital is narrow as compared with public hospitals in Cyprus, as people are more satisfied with the services provided by private hospitals. Brahmbhatt’s4 study used 41 paired questions to measure service quality gaps and observed that patient’s expectations were not met and they were not satisfied with the services provided by private and public hospitals. Bowling’s et al5 study conducted in outpatients and general practices in the UK showed that older, British females were more satisfied with general practices compared with hospital outpatient services. Kumaraswamy’s6 study using a service quality model in corporate and non-corporate healthcare centers revealed that patients are more satisfied with 4 service quality factors; physician attitude, supportive staff, environment, and service provision provided in corporate healthcare centers. Kayral’s7 study used 6 service quality dimensions including 34 questions to determine the provision of service quality in private and public hospitals and observed that the patients perceived quality at higher levels in public hospitals; however, physical quality was better in private hospitals. Li et al8 addressed patients’ perception related to the service quality of hospitals not considering the service quality gaps in 9 Chinese cities. Empathy and reliability emerged as strong perception predictors of service quality in Li et al’s study.8 However, perceptions of service quality varied between cities. Gronroos9 defined service quality as clinical management including diagnosis and treatment (technical quality), and the mode of delivery of services to patients, such as professional staff attitude, emotional support, and cleanliness of environment (functional quality). Parasuraman et al10-12 defined service quality as the difference between expectations and perceptions of patients’ along the 5 dimensions of quality. These studies were conducted in different places using different criteria and different settings for measuring the service quality. The outpatient department is the patients’ first point of contact in the hospital, and the service quality provided by this department establishes the hospital image. A quality outpatient service can be cost-effective by reducing the workload on the inpatient services. Based on the notion that the patients are often unable to accurately evaluate technical quality of care, this study focuses on functional quality, namely, what the patient is receiving. Unfortunately, data on patient’s perceptions and expectations on quality of outpatient services in the hospital studied, are scarce and there is a lack of studies to determine the gap in quality of service. The service quality model of Parasuraman et al,11,12 that defines the quality of outpatient service is best assessed by identifying the quality gap obtained from patients’ expectations and perceptions, is used for our study. The objective of this study was to define service quality gaps in outpatient services by assessing the patient’s expectations and perceptions and to determine the factors affecting such service quality gaps.
Methods
A cross-sectional descriptive study was conducted between October and November 2014 in the outpatient waiting areas of a hospital in the Eastern Province of Saudi Arabia. The study population was made up of patients who had visited the hospital at the time of the study. Patients who were willing to participate, visiting once or more, and >16 years of age were included and any accompanying visitor with the patient and inpatient discharged on the day of data collection and waiting for medicine from the pharmacy were excluded. Inpatient discharged on the day of data collection and waiting for medicine from the pharmacy were excluded. The convenience sampling technique was used. Probability sampling was difficult to use due to time, availability and effort needed, and presumed the higher response rate with convenience sampling technique. The decision to meet the patients in the outpatient department enabled on the spot data collection particularly from those who were in the process of receiving healthcare or those who just received care waiting for medicines from the pharmacy.
Approval for conducting this study was received from the Research and Ethics Committee of the hospital.
A total of 306 survey questionnaires were randomly distributed to patients who attended the outpatient services during the hospital working hours between 8:00 and 11:30 am in the morning shift and from 1:00 to 4:00 in the afternoon shift during this period. According to SERVQUAL, a sample size of 200 is sufficient. The following formula was used to calculate the sample size13 with 5% margin of error:
Z - level of confidence (1.96), N - required sample size, pq - estimated proportion of attribute in population, e - desired level of precision estimated at 95%. The SERVQUAL instrument by Parasuraman et al11 was adapted to collect the data for our study. The SERVQUAL instrument was reliable14 and the instrument has a concurrent validity.15 The questionnaire was first translated into the Arabic language as the majority of Saudi citizens are native speakers of Arabic. The questionnaire was piloted on 20 subjects not included as study participants. Some of the sentences were rephrased after the pilot study, and the final questionnaire was administered to the target sample through trained healthcare workers on site. Verbal informed consent was taken before giving the questionnaire to respondents. The aim of the study was explained by the healthcare workers, and confidentiality and anonymity of participants were guaranteed, and they were requested to complete the survey while at the hospital and not to take home. All questionnaires were directly collected from respondents by the trained healthcare workers after completion. Three hundred and 6 completed the questionnaires; thus, the overall response rate was 100%.
The required data collected comprised of 2 parts. The first part included questions regarding patients’ demographic characteristics such as age, gender, marital status, education level, and type of visits. The second part included 22 items representing the 5 dimensions: 1) Tangibles: physical facilities, equipment and appearance of personnel; 2) Reliability: ability to perform the promised service dependably and accurately; 3) Responsiveness: willingness to help consumers and provide prompt service; 4) Assurance: competence, courtesy and security; 5) Empathy: caring and individualized attention.
Each statement appeared twice and in the expectations section patients answered questions on the desirable status of services, and in the perception section they answered the questions related to the current status of services. The simultaneous expectations and perceptions measurement was consistent with the previous study.11 A 5-point Likert scale was used to measure the patients’ expectations and perceptions of service quality whereby one referred to strongly disagreed and 5 referred to strongly agreed. The score for the quality of service was calculated by computing the difference between the ratings that patients assigned to paired perception and expectation statements according to the formula: SERVQUAL score was provided by the equation:

Wherein SQ means overall service quality, P means performance perception, and E means service quality expectations.
A positive gap score would indicate that expectations were met or exceeded, and perceptions on the outpatient services are very high if the gap score was negative it would indicate that the provided services did not meet their expectations and perceptions regarding services are low. If no quality gap is observed, it would indicate that the expectations are met and the quality of outpatient services is satisfying. The gap score for each individual paired statement was calculated and summed up to provide an overall gap score for each dimension. The effect size (strength of association) was calculated by Eta squared statistics. The guidelines proposed by Cohen16 for interpreting the effect size were as follows: 0.01 small effect, 0.06 moderate effect, and 0.14 large effect.
The collected data were analyzed using the Statistical Package for Social Sciences (Armonk, NY: IBM Corp.) Version 20.0 for Windows and SPSS Analysis of Moment Structures (AMOS) Version 22 (IBM Corporation, Armonk, NY, USA). Data was first analyzed descriptively by computing the means and standard deviations for continuous variables and frequencies and percentages for categorical variables. Confirmatory analyses was carried out to examine the measurements of the study and their reliability and validity. Paired t-test was used to asses the gaps in service quality dimensions. Confirmatory factor analyses is estimated by means of structural equation model through SPSS AMOS version 22. Univariate analysis including analysis of variance was performed to examine the relationship between patients’ characteristics and mean gap score of expectations and means of individual items along 5 dimensions of scale. Cronbach’s alpha analysis was used to reveal the reliability of scale used in the study. The coefficient of 0.70 or higher indicated good to excellent internal consistency as recommended by George and Mallery.17
Results
The proposed service quality model of 5 dimensions is shown in Figure 1. Confirmatory factor analysis was performed to evaluate the proposed quality service model for the modeled constructs that are quality dimensions based on the collected samples. Each subscale consisting of multiple items was converted to single construct that reflected the quality dimension and it was carried out separately for expectation and perception scales for this analysis. Structural equation modelling evaluated the fitness of data with the theoretical model. The maximum likelihood method of estimation was used to estimate the CFA model.
Figure 1.
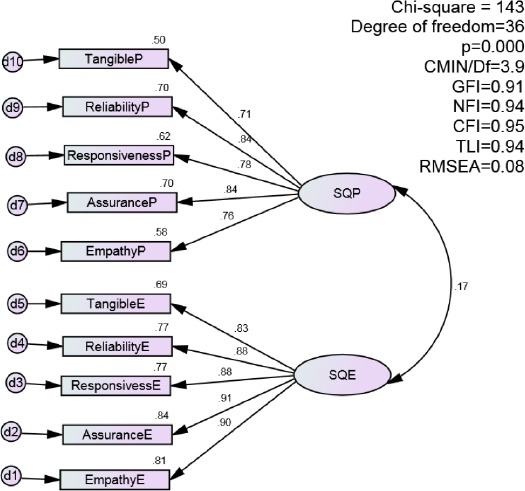
Confirmatory factor analysis of service quality dimensions. SQE - Service quality expectation, SQP - Service quality perception, GFI - goodness of fit index, NFI - normed fit index, CFI - comparative fit index, TLI - Tucker Lewis index, RMSEA - Root Mean Square Error of Approximation, CMIN/DF - negative minimum discrepancy divided by its degrees of freedom
A comparative fit index (CFI)18 of 0.95 and factor loading values of more than 0.7019 from established scales were achieved providing strong evidence of unidimensionality (how closely individual items represent the same construct) after running the CFA for all constructs. The goodness of fit indices shows a good fit between data and the model, and accepts the structural model. The overall fit measures, Chi square=143, degree of freedom=36, p=0.000, a sample size of more than 200 (300 in this study) could affect Chi-square test to indicate a significant p-value, CMIN/df (negative minimum discrepancy divided by its degrees of freedom): 3.9, goodness of fit index (GFI): 0.91, normed fit index (NFI): 0.94, comparative fit index (CFI): 0.95, Tucker Lewis index (TLI): 0.94, and Root Mean Square Error of Approximation (RMSEA): 0.08, achieved the criteria values19,20 and indicated that proposed model fit the data.
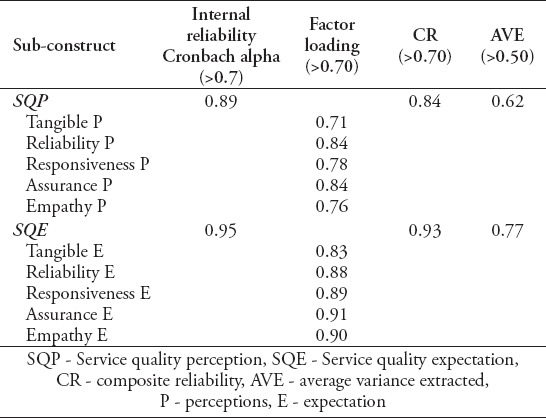
In the next step, convergent validity, composite reliability, and discriminant validity were evaluated to examine the quality of the final measurement model. The results in Table 1 shown that the value of average variance extracted (AVE)20 was greater than 0.50, and the factor loading of each item on the construct was more than 0.70.19 The composite reliability for each construct was more than 0.8, above the recommended value.19 The results revealed that the discriminant validity of the SERVQUAL measurement model is valid. The correlation between 2 sub-constructs was 0.17 and below 0.90,19,21 confirming discriminant validity of the instrument. It is evident from the results that the 2 factors with 10 composite sub-constructs achieved the psychometric value.
Table 1.
Results of convergent validity and composite reliability. (n = 306)
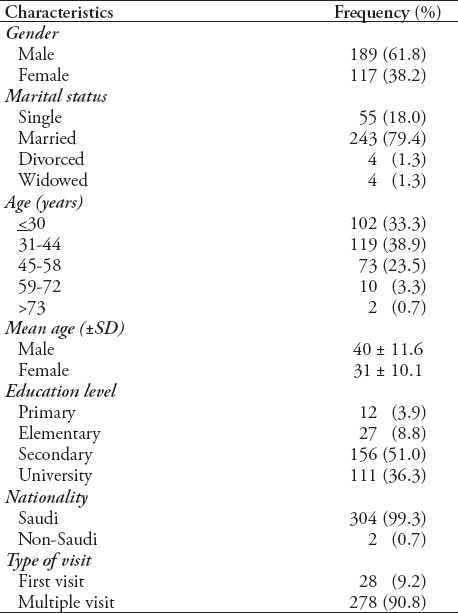
Outpatient characteristics from the analyzed sample (N=306) are as follows: 61.8% of the patients were male, whereas 38.2% were female. The mean age of male was 40 ± 11.6 years, and for females was 30 ± 10 years. Table 2 summarizes the demographic profile of patients measuring the out-patient service quality.
Table 2.
Demographic profile of patients measuring out-patient service quality (n=306).
The reliability coefficient (Cronbach’s coefficient alpha) values ranged from 0.89 for patients’ perceptions scale and 0.95 for patients’ expectations scale. None of reliability alphas for each dimension were below 0.7.17 The paired sample t test in Table 3 shows that there is a statistically significant difference between total perceptions mean scores and total expectations mean scores (t=26.3, p<0.000). The given Eta squared value of 0.69 for the difference between expectation and perception mean scores has a large effect. The negative gaps across all 5 dimensions indicated that patients’ expectations generally are not met, with the largest gap observed in tangible dimension and smallest gap in empathy. The Eta squared statistics for tangible (0.67) responsiveness (0.65), reliability (0.61), assurance (0.57), and empathy (0.41) indicated a large effect size. The highest and lowest means of patients’ perception were related to empathy, responsiveness, and tangibles dimensions. The highest and lowest means of patients’ expectations were related to empathy and responsiveness dimensions. All the dimensions are ranked according to mean scores gap between patients’ expectations and perceptions.
Table 3.
Service quality dimensions gap scores analysis.

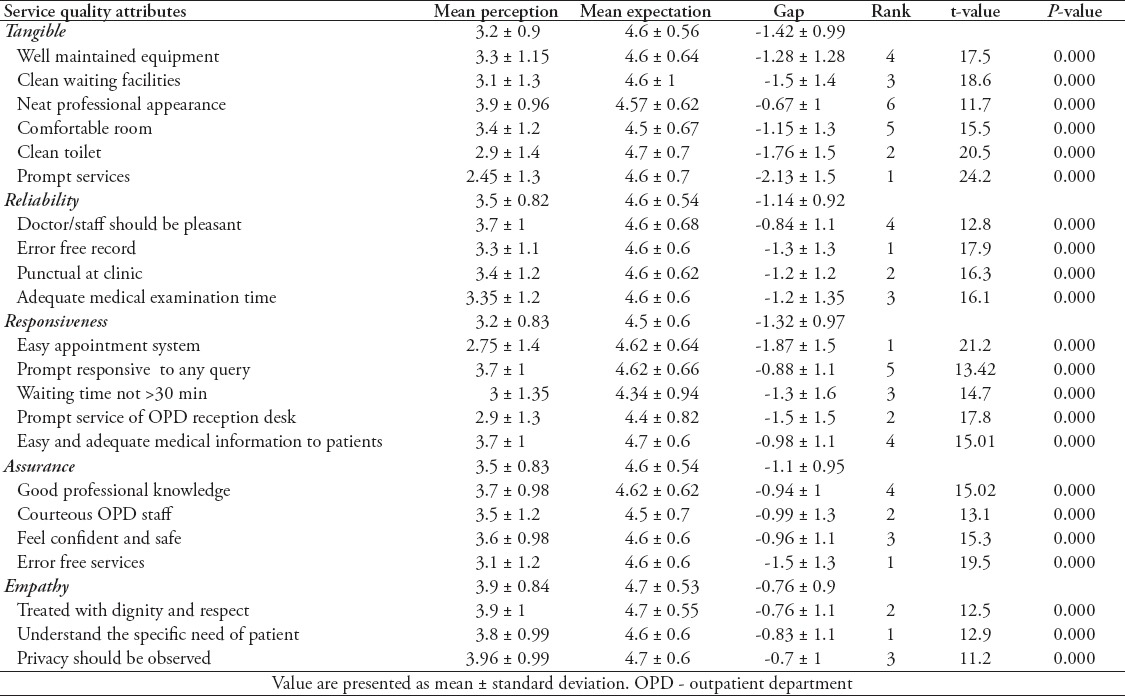
Table 4 shows the mean gap scores in expectations and perceptions statements are ranked and displayed in the respected dimensions. Generally, patients’ expectations statistically significantly exceeded perceptions in all statements (p<0.000). The patients had the highest expectations for toilet facilities that should be clean (4.7 ± 0.7) followed by doctor should explain the condition to the patient (4.7 ± 0.6), and treated with dignity and privacy (4.7 ± 0.6). The least expectation was for waiting time should not be more than 30 minutes. The highest perceptions of patients they are treated with dignity (3.9 ± 1) followed by privacy was observed during treatment (3.9 ± 0.9). There was a low perception in terms of promptness of service at appointed time (2.45 ± 1.3) and easy appointment system (2.75 ± 1.4).
Table 4.
Individual statements contributing to gap scores of service quality dimensions.
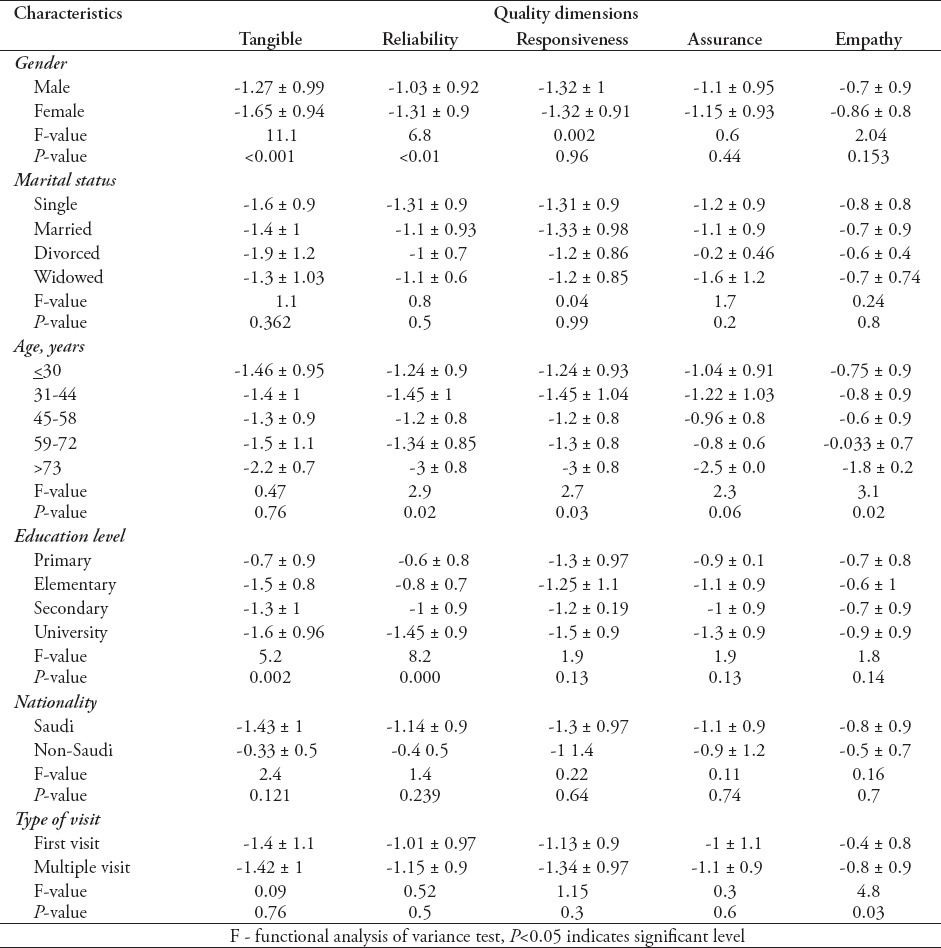
The analysis of variance (ANOVA) results in Table 5 revealed the association between demographic factors and service quality dimensions. The female expectations are statistically significantly higher compared with male expectations in tangibility (p=0.001) and reliability dimensions (p=0.01). The Eta squared statistics was 0.04 for tangibility and 0.02 for reliability dimensions, which in Cohn’s terms would be considered a small effect size. Therefore, despite reaching statistical significance, the actual difference in expectation and perception mean scores between males and females was small. Age group >73 years of age had statistically significantly higher expectations compared with other age groups in 3 dimensions. The Eta squared statistics for these dimensions were 0.04 showing a small difference. University graduate patients’ have statistically significantly higher expectations than others in tangible (p=0.002) and reliability (p=0.000) dimensions. The Eta statistics for these dimensions were 0.05 for tangible and 0.08 for reliability, showing moderate effect. The patients who have had multiple visits to outpatient services had higher expectations in empathy dimension. The Eta statistics for this dimension was 0.02, which represent a small effect. Cross tabulation of marital status and nationality revealed no significant results in all dimensions.
Table 5.
Patients’ demographic characteristics and gap scores of service quality dimensions.
Discussion
This study addressed the service quality gaps in all 5 dimensions after taking the views of patients on what they observed during a visit to the outpatient department during the study period. The study also defined the association between service quality gaps and demographic profiles of patients. The proposed quality model has shown strong evidence of unidimensionality and reliability. The 2 scales showed good validity as 2 separate measures, patients’ expectations, and perceptions of outpatient services. The study results identified that these 2 scales can be successfully implied to evaluate the extent of service quality gap. Therefore, all the 5 service quality dimensions of SERVQUAL appear to be highly suited for monitoring the expectations and perceptions of patients concerning the outpatient service quality in hospital. Chan et al’s22 study recommended 5-10 participants per estimated parameters. There were 19 estimated parameters in our study revealed by confirmatory factory analysis.22 Our study sample of 306 yielded meaningful and interpretable results. The present study using Parasuraman et al’s10,11 SERVQUAL showed that patients’ expectations (4.59 ± 0.5) were more than the perceptions (3.4 ± 0.7) of the provided services across all dimensions, possibly reflecting the new paradigm of increasing patients’ expectations and demand for good quality care. Butt and de Run,23 Anbari and Tabaraie,24 and Bahadori et al25 produced similar results in all service quality dimensions, in line with our results. Comparison of service quality gap scores suggested that the highest gap as far as patients’ assessment of service quality was in the tangibility dimension (-1.42 ± 0.99) followed by responsiveness (-1.32 + 0.97), reliability (-1.14 ± 0.92), assurance (-1.1 ± 0.9), and empathy (-0.7 ± 0.9). Zarei et al’s26 study conducted in private hospitals in Iran showed the highest average score for tangible dimension (environmental quality) and lowest average score in empathy dimension (interaction quality). Ramez27 study ranked reliability as the highest and assurance the lowest service quality dimension. Abu Kharmeh28 identified responsiveness as the most important dimension, and reliability as the least important dimension. Adebayo et al29 study observed the highest service quality gap in assurance and positive gap in empathy dimensions, indicating expectations are met in this dimension among the patients attending the dental clinic. Bahadori et al25 mentioned the largest gap in empathy and smallest gap in tangibility in contrast to our study results.
The hospital physical environment plays an important role in improving the service quality, an attractive outpatient environment, and suitable outpatient services are considered one of the most important reasons for patients coming to the hospital. Previous studies23,26,30 reported that the highest expectations and perceptions were observed in the tangible dimension, as it is concerned with the physical infrastructure of care at private hospitals in Jordan, Saudi Arabia, Iran, and Malaysia. The statement 6, services should be prompt at appointment time achieved this highest quality gap score (-2.13 ± 1.5) among all the statements. Toilet cleanliness achieved the second priority in tangible dimension. Zarei et al’s26 study revealed that the quality of tangible factors have no significant influence on patients’ trust. Ramirez et al’s31 study observed the strong impact of physical environment on the service quality. The gap in the tangible dimension is a wake up call for hospital management to drastically improve the physical environment of outpatient services.
Responsiveness refers to the level of receptiveness, openness, sensitivity, and awareness of staff in the outpatient department. The highest quality gaps between expectations and perceptions were observed for the necessity of an easy appointment system (-1.87 ± 1.5) followed by OPD reception desk are not answering outside calls promptly (-1.5 ± 1.5). This dimension has the lowest perceptions compared with other dimensions, threatening the hospital’s ability to achieve patients’ satisfaction. Ali et al’s32 study observed the lowest perception scores in this dimension similar to our study; however, high negative service quality gap scores rated this as the top dimension in contrast to our results that showed this dimension rated as second after the tangible dimension.
Reliability refers to dependability and steadiness of service. The highest gap observed that outpatient department is not maintaining an error-free record (-1.3 ± 1.3). This result is in contrast to Chakravarty33 study that showed zero gap in this statement indicating services are accurate and dependable. However, statistically significant quality gaps occurred across all the statements (p<0.000).
Assurance refers to guarantee that outpatients will receive a particular level of service. The highest gap scores (-1.5 ± 1.3) observed that services are not carried out right at the first time. The gap between patients’ expectations and perceptions in other statements were statistically significant (p<0.000). Adebayo et al’s29 study reported highest service quality gap in this dimension contrary to our study results. Marzban et al’s34 study revealed that assurance dimension was considered as the most significant dimension with highest scores in contrast to our study results.
Empathy refers to the level of understanding, sympathy, and compassion given by the staff in the outpatient department. The highest expectations (4.7 ± 0.53) and perceptions (3.9 ± 0.84) were observed across all the statements in this dimension. The smallest quality gap scores were identified in the statements indicating that patients’ expectations are nearly met as the patients’ perceived that they have been treated with full privacy and dignity, and the outpatient staff understood their needs. Anbari et al’s24 study observed the highest perception scores in this dimension similar to our study; however, negative gap scores rated third compared with our results that rated this dimension last among other dimensions.
The results of our study showed a significant association between gender and mean scores gap in tangible and reliability dimensions. The female expectations were higher across these dimensions than the male. There was a significant association between age groups and reliability, responsiveness, and empathy dimensions. The age group >73 years has higher expectations in all dimensions, but a significant difference was observed in reliability (p=0.02), responsiveness (p=0.03), and empathy (p=0.02) dimensions compared with other age groups. Bahadori et al’s25 study showed no such association. The quality gap in patients’ expectations with university education was higher than other group in tangibility and reliability dimensions. The patients who made multiple visits to outpatient services have higher expectations related to empathy dimension, as to be treated with honor in contrast with Adebayo et al’s29 study shows frequency of dental visit and gender had no statistically significant association to quality gaps analyzed. Kavitha’s35 study conducted in India to determine the factors influencing service quality gap observed no association between age, gender, education, and occupation in contrast to our results.
Study limitations
1) study design is cross-sectional, longitudinal study evaluates better understanding of variables analyzed as the patient may change opinions over a period of time, 2) this study involves only outpatient services and sampling technique was convenient sampling, limiting the generalizability of results. We excluded inpatients and providers’ perspectives, 3) study was confined to a hospital serving a special population not the general or private public, and 4) the study did not determine the association between service quality dimensions, and overall satisfaction. Although our study was cross-sectional and based on one population, our findings have merit as we performed confirmatory factor analysis using large sample size and with a broad variety of indices to judge the fitness of model to the data and assessed its reliability for measuring service quality.
In conclusion, the analysis of our study results revealed areas in which outpatient services are close to achieving the patients’ expectations, and areas in which outpatient services are short of expectations. The 3 most significant service quality gaps of patients were related to outpatient environment, promptness of services, and reliability of outpatient services. In the present study, expectations are higher than the perceptions of provided service quality, suggesting room for improvement in all quality dimensions. A gap in one dimension can have a synergistic effect on other dimensions of service quality, and leads to a decrease in those dimensions. Therefore, aside from focusing on dimensions with the largest gap, hospital management the service providers should consider the improvement of other dimensions. Finally, it provides support to the idea that although difficult, service quality in the healthcare sector can be measured and consequently be monitored to identify gaps and take corrective actions whenever possible. This study can be further extended to include the association between overall satisfaction and service quality dimensions. The views of inpatients and service providers should also be considered in future studies. It should be kept in mind that the patients’ perceptions and expectations for service quality cannot be collected by one instrument; therefore, it is important to conduct qualitative research along with quantitative method to better understand the complexity of service quality in future studies.
Acknowledgment
We would like to thank the hospital director and other associated staff who enable this study to be completed on time. We thank to Jasser Al-Shehri, Amal Jishi, Fahad Al Manjoumi, and Wafa Al Muhawish for data collection, and Abrar K. Barshaid for data entry.
Footnotes
References
- 1.Marković S, Lončarić D, Lončarić D. Service quality and customer satisfaction in the health care industry - towards health tourism market. Tourism and Hospitality Management. 2014;20:155–170. [Google Scholar]
- 2.Al-Borie HM, Damanhouri AM. Patients’ satisfaction of service quality in Saudi hospitals: a SERVQUAL analysis. Int J Health Care Qual Assur. 2013;26:20–30. doi: 10.1108/09526861311288613. [DOI] [PubMed] [Google Scholar]
- 3.Yesilada F, Direktor E. Health care service quality: A comparison of public and private hospitals. African Journal of Business Management. 2010;4:962–971. [Google Scholar]
- 4.Brahmbhatt M, Baser N, Joshi N. Adapting the SERVQUAL scale to hospital services: An empirical investigation of patients’ perceptions of service quality. International Journal of Multidisciplinary Research. 2011;1:27–42. [Google Scholar]
- 5.Bowling A, Rowe G, McKee M. Patients’ experiences of their healthcare in relation to their expectations and satisfaction: a population survey. J R Soc Med. 2013;106:143–149. doi: 10.1258/jrsm.2012.120147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kumaraswamy S. Service quality in health care centres: An empirical study. International Journal of Business and Social Science. 2012;3:141–150. [Google Scholar]
- 7.Kayral HI. Perceived Service quality in healthcare organizations and a research in Ankara by hospital type. Journal of Ankara Studies. 2014;2:22–34. [Google Scholar]
- 8.Li M, Lowrie BD, Huang YC, Lu CX, Zhu CY, Wu HX, et al. Evaluating patients’ perception of service quality at hospitals in nine Chinese cities by use of SERVQUAL scale. Asian Pac J Trop Biomed. 2015;5:497–504. [Google Scholar]
- 9.Gronroos C. A service quality model and its marketing implications. European Journal of Marketing. 1984;18:36–44. [Google Scholar]
- 10.Parasuraman A, Zeithaml VA, Berry I. A conceptual model of service quality and its implications for future research. Journal of Marketing. 1985;49:41–50. [Google Scholar]
- 11.Parasuraman A, Zeithaml VA, Berry I. “SERVQUAL: multiple item scale for measuring consumer perceptions of service quality.”. Journal of Retailing. 1988;64:12–40. [Google Scholar]
- 12.Parasuraman A, Zeithaml VA, Berry I. Refinement and reassessment of the SERVQUAL scale. Journal of Retailing. 1991;64:12–40. [Google Scholar]
- 13.Israel GD. Sampling the evidence of extension program impact. Program evaluation and organizational development, IFAS, University of Florida. [[Updated 1992 October; 2015 September]]. Available from URL: https://edis.ifas.ufl.edu/document%20pd005 .
- 14.Sulisworo D, Nora M. Integrating Kano’s Model and SERVQUAL to improve healthcare service quality. [[Cited 2015 October]]. Available from URL: https://www.researchgate.net/publication/277759782_Integrating_Kano’s_Model_and_SERVQUAL_to_Improve_Healthcare_Service_Quality .
- 15.Resnick SM, Griffiths MD. Service quality in alcohol treatment: a research note. Int J Health Care Qual Assur. 2011;24:149–163. doi: 10.1108/09526861111105103. [DOI] [PubMed] [Google Scholar]
- 16.Cohen JW. Statistical power analysis for the behavioral sciences. 2nd ed. New York (NY): Erlbaum; 1988. [Google Scholar]
- 17.George D, Mallery P. SPSS for Windows step by step: A simple guide and reference. 11.0 update. 4th ed. Boston (MA): Allyn & Bacon; 2003. [Google Scholar]
- 18.Byrne BM. Structural equation modeling with EQS and EQS/Windows. Thousand Oaks (CA): Sage Publications; 1994. [Google Scholar]
- 19.Hair JF, Black B, Babin B, Anderson RE, Tatham R. Multivariate data analysis: a global perspective. 7th ed. New Jersey (NJ): Pearson Education Inc; 2010. [Google Scholar]
- 20.Afthanorhan W, Ahmad S, Mamat I. Pooled confirmatory factor analysis using structural equation modeling on volunteerism program: A step by step approach. International Journal of Asian Social Science. 2014;5:642–653. [Google Scholar]
- 21.Fornell C, Larcker DF. Evaluating structural equation models with unobservable variables and measurement error. Journal of Marketing Research. 1981;18:39–50. [Google Scholar]
- 22.Chan F, Lee K Gloria, Lee J E, Kubota C, Allen AC. Structural equation modeling in rehabilitation counseling research. Rehabilitation Counseling Bulletin. 2007;51:53–66. [Google Scholar]
- 23.Butt MM, de Run CC. Private healthcare quality: applying a SERVQUAL model. Int J Health Care Qual Assur. 2010;23:658–673. doi: 10.1108/09526861011071580. [DOI] [PubMed] [Google Scholar]
- 24.Anbari Z, Tabaraie Y. Measurement of quality of hospital services via SERVQUAL Model. Bull Env Pharmacol Life Sci. 2013;3:51–56. [Google Scholar]
- 25.Bahadori M, Raadabadi M, Jamebozorgi HM, Salesi M, Ravangard R. Measuring the quality of provided services for patients with chronic kidney disease. Nephrourol Mon. 2014;6:e21810. doi: 10.5812/numonthly.21810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Zarei E, Daneshkohan A, Khabiri R, Arab M. The effect of hospital service quality on patient’s trust. Iran Red Crescent Med J. 2015;17:2–5. doi: 10.5812/ircmj.17505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ramez WS. Patients’ Perception of Health Care Quality, Satisfaction and Behavioral Intention: An Empirical Study in Bahrain. International Journal of Business and Social Science. 2012;3:131–141. [Google Scholar]
- 28.Abu-Kharmeh SS. Evaluating the quality of health care services in the Hashemite Kingdom of Jordan. International Journal of Business and Management. 2012;7:195–205. [Google Scholar]
- 29.Adebayo ET, Adesina BA, Ahaji LE, Hussein NA. Patient assessment of the quality of dental care services in a Nigerian hospital. Journal of Hospital Administration. 2014;3:20–28. [Google Scholar]
- 30.Al-Hawary SI. Health care services quality at private hospitals, from patients’ perspective: A comparative study between Jordan and Saudi Arabia. African Journal of Business Management. 2012;6:6516–6529. [Google Scholar]
- 31.Ramirez FC, Pineda MD. Post behavioral perceptions of service quality in a service setting;Private hospital in México. American International Journal of Social Science. 2014;3:37–40. [Google Scholar]
- 32.Ali M, Hamid A, Emadi A. Measuring and improving the quality of health care services based on patient satisfaction with provided services (improved SERVQUAL model) Journal of Applied Environmental and Biological Sciences. 2015;5:291–294. [Google Scholar]
- 33.Chakravarty A. Evaluation of service quality of hospital outpatient department services. Medical Journal Armed Forces India. 2011;67:221–224. doi: 10.1016/S0377-1237(11)60045-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Marzban S, Najafi M, Etedal MG, Moradi S, Rajaee R. The evaluation of outpatient quality services in physiotherapy in the teaching health centers of Shahid Beheshti University based on SERVQUAL tools. European Journal of Biology and Medical Science Research. 2015;3:46–53. [Google Scholar]
- 35.Kavitha R. Factors Influencing the Service Quality Gap between Expected Service and Perceived Service- A Study of Sri Gokulam Hospitals., Salem. International Journal of Business and Management Invention. 2012;1:30–36. [Google Scholar]