

Abstract
Objective
The objective of this study was to review the published literature and investigate whether E-cadherin gene is a prognostic factor in head and neck squamous cell carcinoma by conducting a meta-analysis.
Methods
Studies were identified from the databases Embase, Medline, and Cochrane Library by using the keywords “E-cadherin gene” and “head and neck cancer”. Overall survival (OS) and disease-free survival (DFS) were the primary outcome measurements.
Results
Our literature review identified 1,458 articles; 19 studies with a total number of 2,012 cases were eligible for inclusion in the meta-analysis. The hazard ratio (HR) for OS of patients with decreased expression of E-cadherin gene was 0.57 (95% CI =0.37, 0.89; P=0.000). However, statistical heterogeneity was unacceptably high (I2=74.5%, P=0.000). After sensitivity analysis, heterogeneity became acceptable, and the effect measure was still significant (I2=7.0%; HR =0.52; 95% CI =0.40, 0.66; P=0.000). The HR for DFS was 0.53 (95% CI =0.42, 0.67; P=0.000).
Conclusion
This meta-analysis showed clear evidence that high E-cadherin gene expression is a positive prognostic factor of head and neck squamous cell carcinoma, resulting in better OS and DFS. However, this conclusion must be interpreted with caution due to a few limitations.
Keywords: E-cadherin gene, prognosis, head and neck squamous cell carcinoma, immunohistochemistry
Introduction
Head and neck squamous cell carcinoma (HNSCC) is the most common cancer in the world and accounts for ~3% of all cancer cases.1,2 Although significant advancements have been made in prevention, diagnostics, and treatment strategies for HNSCC, the survival rates in patients with progressive or metastatic disease have remained poor over the last 20 years.3–5 Prognostic markers remain the basis for early detection and accurate survival evaluation for oral squamous cell carcinoma patients.
Numerous studies suggest that E-cadherin gene is a predictor of oral squamous cell carcinoma prognosis.6–24 E-cadherin is a 120 kDa transmembrane glycoprotein that mediates homotypic Ca2+-dependent intercellular adhesion in dissimilar epithelia. Moreover, E-cadherin is a pivotal factor for managing cell-to-cell adhesion in epithelial tissues.25 At present, downregulation or aberrant expression of E-cadherin gene is associated with cancer invasion and poor prognosis in various carcinomas, including HNSCC. In addition, a multitude of existing studies have investigated the effect of E-cadherin gene on prognosis in HNSCC. However, E-cadherin gene has no consistent prognostic value for HNSCC. Additionally, most of the published literature includes studies that are small in size,8,18–20 heterogeneous,14,19,22 and conflicting in their results.17,19,22,23 Thus, we performed a meta-analysis to systematically estimate the value of E-cadherin gene as a prognostic factor in HNSCC.
Methods
Literature search
A literature search was performed using Embase, Medline, and Cochrane Library. The database was searched with the following keywords (and/or MeSH words): E-cadherin gene, tongue cancer (squamous cell carcinoma), buccal cancer (squamous cell carcinoma), oral cancer (squamous cell carcinoma), mouth cancer (squamous cell carcinoma), tonsil cancer (squamous cell carcinoma), oropharynx cancer (squamous cell carcinoma), hypopharynx cancer (squamous cell carcinoma), nasopharynx cancer (squamous cell carcinoma), larynx cancer (squamous cell carcinoma), neck cancer (squamous cell carcinoma), and head and neck cancer (squamous cell carcinoma). Reference lists within the relevant articles were used as potentially eligible sources.
Inclusion criteria
Studies were included if they met all the following inclusion criteria: a) patients were diagnosed with HNSCC and biopsy confirmed (no age limit); b) focused on the evaluation of E-cadherin gene expression in primary tumor and the correlation between E-cadherin gene expression and survival outcomes; and c) outcome indicators included overall survival (OS) or disease-free survival (DFS).
Exclusion criteria
Studies were excluded if they met any of the following exclusion criteria: a) no clear follow-up and survival analysis or could not provide sufficient data required for prognostic estimation of patients; b) no use of immunohistochemistry to assess the expression of E-cadherin gene; c) case reports, comments, letters to the author, reviews, and meta-analyses; and d) were not written in English.
Quality assessment and data analysis
The quality and risk of bias of all the included trials were assessed independently by two reviewers, Xusheng Ren and Jianning Wang, based on the Cochrane Handbook for Systematic Reviews of Interventions. Assessment of risk of bias was evaluated as “low risk of bias,” “unclear risk of bias,” or “high risk of bias” in each part, with notes explaining the specific reasons for each assessment in the risk of bias table. Any contradictions in opinion were resolved by discussion.
We extracted data from the eligible studies using an extraction form (Review Manager 5.3). We attempted to contact study authors for relevant missing or unclear data. We also attempted to contact the authors to confirm whether the study was duplicated or if there was any doubt whether the studies shared the same patients. We excluded studies that did not meet the inclusion criteria in terms of study design. One reviewer extracted the data, which was checked by another reviewer, and all conflicts were resolved by discussion.
Statistical analysis
All individual outcomes were pooled using Stata 12.0. The hazard ratio (HR) and its 95% confidence interval (CI) were used for meta-analysis of OS or DFS. We performed a random-effects model to merge HR when the heterogeneity was acceptable (I2<50%) and a fixed-effects model when the heterogeneity was unacceptable (I2≥50%). Statistical heterogeneity, which is the variation in results between studies, was assessed using the chi-square distributed Q statistic. Subgroup analyses and sensitivity analyses were performed when the heterogeneity was unacceptable.
Results
Search findings
Our literature review identified 1,458 articles, including 1,385 articles from Medline, Embase, and Cochrane Library and 73 articles from the reference lists of articles obtained. A total of 1,410 articles were excluded after reviewing the titles and abstracts. The remaining 48 articles were further evaluated for eligibility and another 29 articles were eventually excluded. Figure 1 shows the flowchart of literature retrieval and lists the reasons for their exclusion. Nineteen studies with a total number of 2,012 cases were eligible for inclusion in the meta-analysis. Seven studies had data for both OS and DFS, nine studies had data only for OS, and three studies had data only for DFS. We could get all the needed data from these 19 studies and did not need to contact the authors.
Figure 1.

A flow diagram of literature search.
Study characteristics and treatment
As shown in Table 1, in these 19 studies, there were ten studies6,10,12,16,17,19,20,22–24 that reported only using surgery. Six studies8,9,11,13,15,18 reported that all the patients were treated with surgery and some patients were treated with radiotherapy. Two studies7,13 reported that all the patients were treated with surgery and some patients were treated with radiotherapy and/or chemotherapy. Only one study20 reported that all the patients were treated with surgery and some patients were treated with chemotherapy.
Table 1.
The features of included studies
| Author | Year | Country | Size of study | Tumor locations | Tumor stage | Treatment | Data of OS or DFS |
|---|---|---|---|---|---|---|---|
| da Silva et al6 | 2015 | Brazil | 102 | OSCC | I–IV | Surgery | OS (DSS) |
| Ahmed et al7 | 2014 | Egypt | 75 | LSCC | I–IV | Surgery, radiotherapy, and chemotherapy | OS and DFS |
| Pectasides et al8 | 2014 | USA | 67 | HNSCC | I–IV | Surgery and radiotherapy | DFS (PFS) |
| Psyrri et al9 | 2014 | Greece | 289 | LSCC | I–IVa | Surgery and radiotherapy | OS and DFS |
| Fan et al10 | 2013 | Taiwan | 112 | OSCC | In situ–IV | Surgery | OS |
| Kaur et al11 | 2013 | India | 72 | OSCC | I–IVa | Surgery and radiotherapy | DFS |
| Imajyo et al12 | 2012 | Japan | 152 | OSCC | NA | Surgery | OS and DFS |
| Li et al13 | 2012 | People’s Republic of China | 64 | LSCC | I–IV | Surgery and radiotherapy | OS and DFS |
| Ukpo et al14 | 2012 | USA | 154 | Oropharyngeal SCC | I–IV | Surgery, radiotherapy, and chemotherapy | OS |
| Zhao et al15 | 2012 | People’s Republic of China | 98 | OSCC | I–IV | Surgery and radiotherapy | OS and DFS |
| Liu et al16 | 2010 | People’s Republic of China | 83 | OSCC | I–IV | Surgery | OS |
| Zou et al17 | 2010 | People’s Republic of China | 150 | LSCC | I–IV | Surgery | DFS |
| Diniz-Freitas et al18 | 2006 | Spain | 47 | OSCC | I–IV | Surgery and radiotherapy | OS and DFS |
| Hung et al19 | 2006 | People’s Republic of China | 45 | OSCC | III–IV | Surgery | OS |
| Kurtz et al20 | 2006 | USA | 45 | HNSCC | I–IV | Surgery | OS and DFS |
| Ueda et al21 | 2006 | Japan | 131 | OSCC | I–IV | Surgery and chemotherapy | DFS |
| Bosch et al22 | 2005 | Germany | 151 | HNSCC | I–IV | Surgery | OS |
| Lim et al23 | 2005 | South Korea | 84 | OSCC | I–IV | Surgery | OS |
| Nakanishi et al24 | 2004 | Japan | 91 | OTSCC | II–IV | Surgery | OS |
Abbreviations: OS, overall survival; DFS, disease-free survival; OSCC, oral squamous cell carcinoma; DSS, disease-specific survival; LSCC, laryngeal squamous cell carcinoma; HNSCC, head and neck squamous cell carcinoma; PFS, progression-free survival; SCC, squamous cell carcinoma; OTSCC, oral tongue squamous cell carcinoma; NA, not available.
Methodology assessment of E-cadherin gene expression
The detection method of E-cadherin gene was immunohistochemistry, and all studies except the study by Psyrri et al9 provided immunohistochemistry staining figures.
Meta-analysis
E-cadherin gene expression and OS
In this meta-analysis, there were seven studies7,9,10,19,20,23,24 that provided HR values and 95% CI. Therefore, we directly utilized them for the evaluation of E-cadherin gene expression and OS. There were another nine studies6,8,12–18 from which the HR values and their corresponding 95% CI could be calculated according to the data provided by the investigators.26 There was significant heterogeneity between each study (I2=74.5%, P=0.000). The HR for OS was 0.57 (95% CI =0.37, 0.89; P=0.000). However, statistical heterogeneity was unacceptably high, driven by one study.22 When this study was excluded, heterogeneity became acceptable, and the effect measure was still significant (I2=7.0%; HR =0.52; 95% CI =0.40, 0.66; P=0.000; Figure 2).
Figure 2.

A forest plot for overall survival.
Notes: The difference between the two groups was significant (HR =0.57; 95% CI =0.37, 0.89; P=0.000). However, there was great statistical heterogeneity (I2=74.5%, P=0.000). After sensitivity analysis, heterogeneity became acceptable (I2=7.0%) and the effect measure remained significant (HR =0.52; 95% CI =0.40, 0.66; P=0.000). “1” means after sensitivity analysis and “1+2” means before sensitivity analysis. Weights are from random effects analysis.
Abbreviations: HR, hazard ratio; CI, confidence interval.
E-cadherin gene expression and DFS
In this meta-analysis, there were five studies7,9,11,15,21 that provided HR values and 95% CI. Therefore, we directly utilized them for the evaluation of E-cadherin gene expression and DFS. There were another five studies12,13,17,18,20 from which the HR values and their corresponding 95% CI could be calculated according to the data provided by the authors. There was no significant heterogeneity between each study (I2=0.0%, P=0.860). The HR for DFS was 0.53 (95% CI =0.42, 0.67; P=0.000; Figure 3).
Figure 3.

A forest plot for overall survival.
Note: The difference between the high E-cadherin group and the low E-cadherin group was significant (HR =0.53; 95% CI =0.42, 0.67; P=0.000) and the heterogeneity was acceptable (I2=0.0%, P=0.860).
Abbreviations: HR, hazard ratio; CI, confidence interval.
Publication bias analysis
Publication bias of this meta-analysis was analyzed by the use of Stata 12.0 software. According to the funnel plots (Figures 4 and 5), there was an asymmetry, either visually or from Begg’s test (OS: P=0.753; DFS: P=0.210). This indicates that there was no obvious publication bias and the result of the study was stable and credible.
Figure 4.
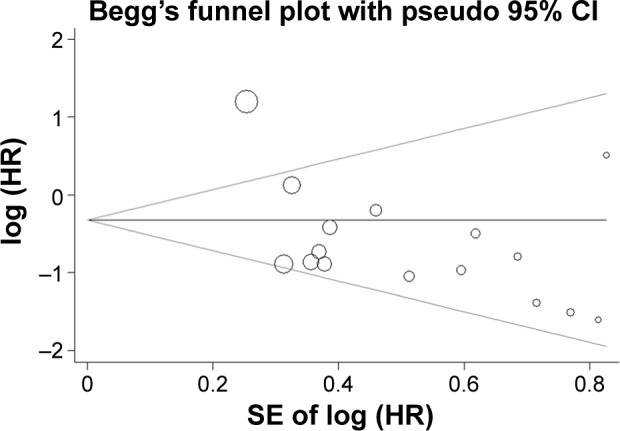
A funnel plot of meta-analysis of overall survival.
Note: According to the funnel plot, there is an asymmetry.
Abbreviations: HR, hazard ratio; SE, standard error; CI, confidence interval.
Figure 5.
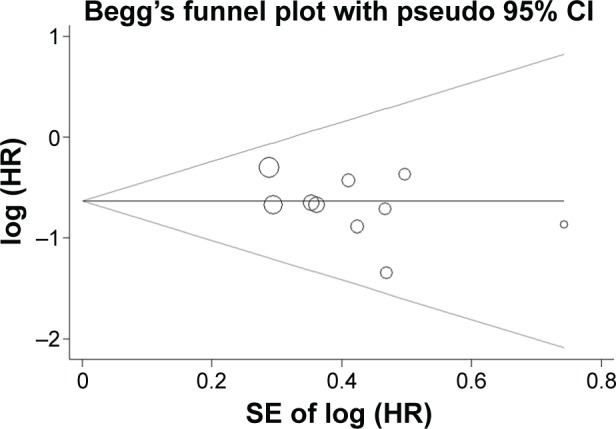
A funnel plot of meta-analysis of disease-free survival.
Note: According to the funnel plot, there is an asymmetry.
Abbreviations: HR, hazard ratio; SE, standard error; CI, confidence interval.
Discussion
Numerous studies have reported that E-cadherin gene is a predictor for cancer prognosis.27–30 The low expression of E-cadherin gene is a characteristic of loss of epithelial cell adhesion, which has been correlated with the phenotypic changes of increased invasiveness and motility of cancer cells. Some studies have shown that high expression of E-cadherin gene is associated with good prognosis in many epithelial cancers.29,30 However, the prognostic value of E-cadherin gene in patients with HNSCC is still controversial. Some studies8,10,15,23 report that high E-cadherin gene expression is a positive prognostic factor of HNSCC and exhibits better OS or DFS. The reports of Diniz-Freitas et al18 and Kurtz et al20 were also in line with the findings mentioned above. However, Bosch et al22 showed that low E-cadherin gene expression is a positive prognostic factor of HNSCC. In addition, many scholars harbored the idea that E-cadherin gene expression was not an independent prognostic factor of HNSCC. Moreover, most studies included in this meta-analysis6,7,9,11–14,16,17,19,21,24 also reported that E-cadherin gene expression was not significantly associated with OS or DFS. The aim of this meta-analysis was retrospective analysis of published literatures to assess the prognostic value of E-cadherin gene expression in patients with HNSCC.
In the present study, we selected 19 studies that were clear regarding not only diagnostic criteria but also inclusion criteria and exclusion criteria. OS and DFS were the primary outcome measures. HR values and their corresponding 95% CIs were the statistical indicators to evaluate the impact of E-cadherin gene expression on prognosis of patients with HNSCC.
This meta-analysis confirmed that high E-cadherin gene expression was significantly associated with favorable OS. The HR for OS was 0.57 (95% CI =0.37, 0.89). However, statistical heterogeneity was obvious, driven by one study.22 After sensitivity analysis, heterogeneity became acceptable, and the effect measure was still significant (HR =0.52; 95% CI =0.40, 0.66). Differences in immunohistochemical scoring criteria may have contributed to the large heterogeneity between the study by Bosch et al and other included studies. As is known to all, it would make more sense to run a meta-analysis per individual anatomic site rather than lumping together sites that are known for heterogeneity in molecular signature, different standard of care, and different outcomes. Furthermore, the standard of care and outcome vary dramatically according to the HNSCC stage; thus, meta-analysis per early versus advanced stage carcinomas would have been much more valuable. Because this study had impeccable protocol and strict inclusion criteria, we did not have the above problems. Moreover, this meta-analysis also confirmed that high E-cadherin gene expression was significantly associated with improved DFS. The HR for DFS was 0.53 (95% CI =0.42, 0.67).
Although a meta-analysis was previously published29 that had a similar theme as our study, it was published 3 years ago and therefore did not include over half of the studies included in our meta-analysis. Compared with the study by Zhao et al, we analyzed more outcome measures and included more information than the previous meta-analysis. In addition, based on our judgment, the data extraction and statistical analysis of this meta-analysis by Zhao et al had some small flaws.
Every meta-analysis, including our own, has its internal limitations.31 First, all the included studies were retrospective studies, rather than prospective. Additionally, some of these included studies did not provide the HR values and the 95% CI. We could not directly utilize them for the evaluation of E-cadherin gene expression and OS, and had to calculate HR values and their 95% CI according to the data provided by the researchers. Owing to various reasons, the results may have deviated slightly. Also, there was obvious heterogeneity among these studies. Additionally, selective reporting of individual research also limited this meta-analysis. Owing to various reasons, obtaining all data for a complete review of E-cadherin gene in HNSCC is impossible. To resolve these problems, we calculated HR values and their 95% CI according to reported methods.26 This allowed us to increase the sample size for this study and make the findings more reliable. All these factors might affect the outcomes measured and might have influenced the findings. More studies with better designed criteria are required to further confirm our results.
Conclusion
In conclusion, this meta-analysis showed clear evidence that high E-cadherin gene expression is a positive prognostic factor of HNSCC and is associated with better OS and DFS. However, some limitations weakened the power of this meta-analysis, and the conclusions should be interpreted with caution.
Footnotes
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. doi: 10.3322/caac.20107. [DOI] [PubMed] [Google Scholar]
- 2.Ren ZH, Xu JL, Fan TF, Ji T, Wu HJ, Zhang CP. The harmonic scalpel versus conventional hemostasis for neck dissection: a meta-analysis of the randomized controlled trials. PLoS One. 2015;10:e0132476. doi: 10.1371/journal.pone.0132476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Silverman S., Jr Demographics and occurrence of oral and pharyngeal cancers. The outcomes, the trends, the challenge. J Am Dent Assoc. 2001;132(suppl):7S–11S. doi: 10.14219/jada.archive.2001.0382. [DOI] [PubMed] [Google Scholar]
- 4.Chandler K, Vance C, Budnick S, Muller S. Muscle invasion in oral tongue squamous cell carcinoma as a predictor of nodal status and local recurrence: just as effective as depth of invasion? Head Neck Pathol. 2011;5:359–363. doi: 10.1007/s12105-011-0296-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ren ZH, Wu HJ, Zhang S, et al. A new surgical strategy for treatment of tongue squamous cell carcinoma based on anatomic study with preliminary clinical evaluation. J Craniomaxillofac Surg. 2015;43:1577–1582. doi: 10.1016/j.jcms.2015.07.034. [DOI] [PubMed] [Google Scholar]
- 6.da Silva SD, Morand GB, Alobaid FA, et al. Epithelial-mesenchymal transition (EMT) markers have prognostic impact in multiple primary oral squamous cell carcinoma. Clin Exp Metastasis. 2015;32:55–63. doi: 10.1007/s10585-014-9690-1. [DOI] [PubMed] [Google Scholar]
- 7.Ahmed RA, Shawky Ael A, Hamed RH. Prognostic significance of cyclin D1 and E-cadherin expression in laryngeal squamous cell carcinoma. Pathol Oncol Res. 2014;20:625–633. doi: 10.1007/s12253-014-9741-6. [DOI] [PubMed] [Google Scholar]
- 8.Pectasides E, Rampias T, Sasaki C, et al. Markers of epithelial to mesenchymal transition in association with survival in head and neck squamous cell carcinoma (HNSCC) PLoS One. 2014;9:e94273. doi: 10.1371/journal.pone.0094273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Psyrri A, Kotoula V, Fountzilas E, et al. Prognostic significance of the Wnt pathway in squamous cell laryngeal cancer. Oral Oncol. 2014;50:298–305. doi: 10.1016/j.oraloncology.2014.01.005. [DOI] [PubMed] [Google Scholar]
- 10.Fan CC, Wang TY, Cheng YA, et al. Expression of E-cadherin, twist, and p53 and their prognostic value in patients with oral squamous cell carcinoma. J Cancer Res Clin Oncol. 2013;139:1735–1744. doi: 10.1007/s00432-013-1499-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kaur J, Sawhney M, DattaGupta S, et al. Clinical significance of altered expression of beta-catenin and E-cadherin in oral dysplasia and cancer: potential link with ALCAM expression. PLoS One. 2013;8:e67361. doi: 10.1371/journal.pone.0067361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Imajyo I, Sugiura T, Kobayashi Y, et al. T-box transcription factor Brachyury expression is correlated with epithelial-mesenchymal transition and lymph node metastasis in oral squamous cell carcinoma. Int J Oncol. 2012;41:1985–1995. doi: 10.3892/ijo.2012.1673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Li JJ, Zhang GH, Yang XM, et al. Reduced E-cadherin expression is associated with lymph node metastases in laryngeal squamous cell carcinoma. Auris Nasus Larynx. 2012;39:186–192. doi: 10.1016/j.anl.2011.04.003. [DOI] [PubMed] [Google Scholar]
- 14.Ukpo OC, Thorstad WL, Zhang Q, Lewis JS., Jr Lack of association of cadherin expression and histopathologic type, metastasis, or patient outcome in oropharyngeal squamous cell carcinoma: a tissue microarray study. Head Neck Pathol. 2012;6:38–47. doi: 10.1007/s12105-011-0306-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zhao D, Tang XF, Yang K, Liu JY, Ma XR. Over-expression of integrin-linked kinase correlates with aberrant expression of Snail, E-cadherin and N-cadherin in oral squamous cell carcinoma: implications in tumor progression and metastasis. Clin Exp Metastasis. 2012;29:957–969. doi: 10.1007/s10585-012-9485-1. [DOI] [PubMed] [Google Scholar]
- 16.Liu LK, Jiang XY, Zhou XX, Wang DM, Song XL, Jiang HB. Upregulation of vimentin and aberrant expression of E-cadherin/beta-catenin complex in oral squamous cell carcinomas: correlation with the clinicopathological features and patient outcome. Mod Pathol. 2010;23:213–224. doi: 10.1038/modpathol.2009.160. [DOI] [PubMed] [Google Scholar]
- 17.Zou J, Yang H, Chen F, et al. Prognostic significance of fascin-1 and E-cadherin expression in laryngeal squamous cell carcinoma. Eur J Cancer Prev. 2010;19:11–17. doi: 10.1097/CEJ.0b013e32832f9aa6. [DOI] [PubMed] [Google Scholar]
- 18.Diniz-Freitas M, Garcia-Caballero T, Antunez-Lopez J, Gandara-Rey JM, Garcia-Garcia A. Reduced E-cadherin expression is an indicator of unfavourable prognosis in oral squamous cell carcinoma. Oral Oncol. 2006;42:190–200. doi: 10.1016/j.oraloncology.2005.07.010. [DOI] [PubMed] [Google Scholar]
- 19.Hung KF, Chang CS, Liu CJ, Lui MT, Cheng CY, Kao SY. Differential expression of E-cadherin in metastatic lesions comparing to primary oral squamous cell carcinoma. J Oral Pathol Med. 2006;35:589–594. doi: 10.1111/j.1600-0714.2006.00474.x. [DOI] [PubMed] [Google Scholar]
- 20.Kurtz KA, Hoffman HT, Zimmerman MB, Robinson RA. Decreased E-cadherin but not beta-catenin expression is associated with vascular invasion and decreased survival in head and neck squamous carcinomas. Otolaryngol Head Neck Surg. 2006;134:142–146. doi: 10.1016/j.otohns.2005.08.026. [DOI] [PubMed] [Google Scholar]
- 21.Ueda G, Sunakawa H, Nakamori K, et al. Aberrant expression of beta- and gamma-catenin is an independent prognostic marker in oral squamous cell carcinoma. Int J Oral Maxillofac Surg. 2006;35:356–361. doi: 10.1016/j.ijom.2005.07.023. [DOI] [PubMed] [Google Scholar]
- 22.Bosch FX, Andl C, Abel U, Kartenbeck J. E-cadherin is a selective and strongly dominant prognostic factor in squamous cell carcinoma: a comparison of E-cadherin with desmosomal components. Int J Cancer. 2005;114:779–790. doi: 10.1002/ijc.20782. [DOI] [PubMed] [Google Scholar]
- 23.Lim J, Kim JH, Paeng JY, et al. Prognostic value of activated Akt expression in oral squamous cell carcinoma. J Clin Pathol. 2005;58:1199–1205. doi: 10.1136/jcp.2004.024786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Nakanishi Y, Akimoto S, Sato Y, Kanai Y, Sakamoto M, Hirohashi S. Prognostic significance of dysadherin expression in tongue cancer: immunohistochemical analysis of 91 cases. Appl Immunohistochem Mol Morphol. 2004;12:323–328. doi: 10.1097/00129039-200412000-00006. [DOI] [PubMed] [Google Scholar]
- 25.Takeichi M. Cadherin cell adhesion receptors as a morphogenetic regulator. Science. 1991;251:1451–1455. doi: 10.1126/science.2006419. [DOI] [PubMed] [Google Scholar]
- 26.Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials. 2007;8:16. doi: 10.1186/1745-6215-8-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Jamieson NB, Carter CR, McKay CJ, Oien KA. Tissue biomarkers for prognosis in pancreatic ductal adenocarcinoma: a systematic review and meta-analysis. Clin Cancer Res. 2011;17:3316–3331. doi: 10.1158/1078-0432.CCR-10-3284. [DOI] [PubMed] [Google Scholar]
- 28.Gould Rothberg BE, Bracken MB. E-cadherin immunohistochemical expression as a prognostic factor in infiltrating ductal carcinoma of the breast: a systematic review and meta-analysis. Breast Cancer Res Treat. 2006;100:139–148. doi: 10.1007/s10549-006-9248-2. [DOI] [PubMed] [Google Scholar]
- 29.Zhao Z, Ge J, Sun Y, et al. Is E-cadherin immunoexpression a prognostic factor for head and neck squamous cell carcinoma (HNSCC)? A systematic review and meta-analysis. Oral Oncol. 2012;48:761–767. doi: 10.1016/j.oraloncology.2012.02.024. [DOI] [PubMed] [Google Scholar]
- 30.Luo SL, Xie YG, Li Z, Ma JH, Xu X. E-cadherin expression and prognosis of oral cancer: a meta-analysis. Tumour Biol. 2014;35:5533–5537. doi: 10.1007/s13277-014-1728-0. [DOI] [PubMed] [Google Scholar]
- 31.Ren ZH, Xu JL, Li B, Fan TF, Ji T, Zhang CP. Elective versus therapeutic neck dissection in node-negative oral cancer: evidence from five randomized controlled trials. Oral Oncol. 2015;51:976–981. doi: 10.1016/j.oraloncology.2015.08.009. [DOI] [PubMed] [Google Scholar]