

Abstract
Purpose
The aim of this study was to evaluate the efficacy of a multimedia informed consent (IC) presentation on the understanding and satisfaction of patients who were scheduled to receive 120-W green-light high-performance system photoselective vaporization of the prostate (HPS-PVP).
Materials and Methods
A multimedia IC (M-IC) presentation for HPS-PVP was developed. Forty men with benign prostatic hyperplasia who were scheduled to undergo HPS-PVP were prospectively randomized to a conventional written IC group (W-IC group, n=20) or the M-IC group (n=20). The allocated IC was obtained by one certified urologist, followed by a 15-question test (maximum score, 15) to evaluate objective understanding, and questionnaires on subjective understanding (range, 0~10) and satisfaction (range, 0~10) using a visual analogue scale.
Results
Demographic characteristics, including age and the highest level of education, did not significantly differ between the two groups. No significant differences were found in scores reflecting the objective understanding of HPS-PVP (9.9±2.3 vs. 10.6±2.8, p=0.332) or in subjective understanding scores (7.5±2.1 vs. 8.6±1.7, p=0.122); however, the M-IC group showed higher satisfaction scores than the W-IC group (7.4±1.7 vs. 8.4±1.5, p=0.033). After adjusting for age and educational level, the M-IC group still had significantly higher satisfaction scores.
Conclusions
M-IC did not enhance the objective knowledge of patients regarding this surgical procedure. However, it improved the satisfaction of patients with the IC process itself.
Keywords: Informed consent; Multimedia; Prostate; Prostatic hyperplasia; Surgical procedures, operative
INTRODUCTION
Informed consent (IC) is an essential prerequisite of surgical treatment [1,2,3]. Benign prostatic hyperplasia (BPH) is a benign disease that occasionally requires surgical treatment [4,5], and one for the surgical treatments for BPH is 120-W green-light high-performance system photoselective vaporization of the prostate (HPS-PVP) [4]. IC is, therefore, essential before HPS- PVP [6].
IC for HPS-PVP has different characteristics than for other procedures, as several alternative treatment methods are available for BPH [4,5]. Furthermore, it is an optional procedure, in contrast to other emergency diseases that lead to serious sequelae when a proper operation is not performed in a timely manner. Therefore, voluntary informed decision-making before HPS-PVP is more important than it is for other procedures.
The conventional method of obtaining IC is a verbal explanation provided together with a written document [7]. However, conventional written IC (W-IC) in clinical practice does not sufficiently achieve its purpose [7,8,9,10]. Most clinical practitioners cannot spend the time necessary to obtain consent due to their heavy workload, and most IC forms have so much information that patients cannot understand all the content in a short time [7]. The mean level of patient comprehension was found to be only 48% in a study using conventional W-IC [10]. Therefore, a new methodology is required to convey information about planned operations and to facilitate informed decision- making by patients [7].
Various multimedia IC (M-IC) presentations using audio, video, or interactive systems have been developed, and their efficacy has been evaluated [11,12,13,14,15,16,17,18,19]. Most studies have reported that M-IC presentations improved patient comprehension and satisfaction. The use of M-IC presentations is a positive attempt to aid in the decision-making process [17] because M-IC presentations expected to be more effective, particularly when a physician explains complicated surgical procedures [7].
In this study, we developed a M-IC presentation for HPS-PVP and evaluated its efficacy.
MATERIALS AND METHODS
1. Patients and study design
This study was approved by the Institutional Review Board of the SMG-SNU Boramae Medical Center. This prospective randomized controlled trial included 40 patients who were scheduled to receive HPS-PVP for lower urinary tract symptoms (LUTS) and BPH. The patients were randomized into a conventional W-IC group (n=20) or M-IC group (n=20). After obtaining IC, we evaluated the objective understanding of the patients using a 15-question test. Subjective understanding and satisfaction were also evaluated using a visual analogue scale (VAS).
2. Hypothesis and endpoints
The hypothesis was that the M-IC presentation would improve objective understanding about a planned operation. We proposed that the new form of IC would increase patient subjective understanding about the operation and satisfaction about the IC process itself. The primary end-point was a test assessing the patient's objective understanding of the procedure. The secondary endpoint was the extent of the patient's subjective understanding and each patient's degree of satisfaction.
3. Development of multimedia informed consent presentation
First, we reviewed existing written documents that had been used to obtain voluntary agreement for HPS-PVP. The conventional W-IC form contained an explanation of the following eight items: (1) the definition of LUTS/BPH, (2) methods of evaluating LUTS/BPH, (3) the natural prognosis of the disease without surgical treatment, (4) alternative treatment methods other than HPS-PVP, (5) the potential benefit of surgery, (6) the surgical procedure, (7) possible complications during or after treatment, and (8) postoperative management and instructions.
We developed M-IC presentation containing the same content that was used in the conventional W-IC form, maintaining the same order. The M-IC presentation had pictures, illustrations, animations, and video clips and was produced using Microsoft PowerPoint 2007 (Microsoft, Redmond, WA, USA) (Appendix). A recorded voice was not used in the presentation because both IC methods were designed to be explained by the doctors themselves. The appropriateness of the content of the conventional IC and the M-IC was evaluated by five certified urologists who did not participate in the production process. We then performed a pilot study with 10 patients using the conventional written consent form (n=5) and the M-IC presentation (n=5). The patients provided feedback about legibility and how the information was communicated. The M-IC presentation was modified based on suggestions from the patients and the urologists, and the time to obtain IC was adjusted to 15 minutes for both methods.
4. Development of a test for objective understanding
We developed a new test with 15 items evaluating patients' objective understanding of HPS-PVP. All topics and correct answers in the test were extracted from the conventional W-IC form and the M-IC presentation. The test included the following: (1) five items testing basic knowledge regarding BPH and LUTS (Q1~5; anatomy, prostate function, etiology of LUTS/BPH, symptoms of LUTS/BPH, and diagnosis of LUTS/BPH), (2) four items about treatment modalities (Q6~9; medical treatment, aim of the surgery, treatments other than HPS-PVP, and the HPS-PVP surgical procedure), (3) three items about hospital logistics and precautions after surgery (Q10~12), (4) three items on complications after the operation (Q13~15; possible complications and treatment of complications). After the initial development of the test, five certified urologists who did not participate in developing the instrument reviewed and validated the appropriateness of the test. A pilot study was then performed to 10 patients undergoing HPS-PVP after explaining the procedure with the conventional W-IC and the M-IC presentation (five for each type of IC). The highest education levels of the subjects in the pilot study were middle school (n=4), high school (n=4), and university (n=2), with a distribution that favored lower levels of education because we aimed to develop an IC presentation that could be understood by a subject whose highest education level was middle school. Items with low percentages of correct answers were modified or substituted with easier questions.
5. Sample size estimate
The mean score of objective understanding was 7.4 (highest possible score, 15) and the standard deviation of the scores was 2.9. In order to examine a minimum difference of 2 points in the scores with alpha-error of 5% and beta-error of 20%, the calculated number of patients needed for this study was 34. Based on a potential drop-out rate of 20%, 40 patients (20 patients in each group) were included in this study.
6. Obtaining informed consent and questionnaires
All patients were admitted one day before surgery, and IC was obtained on the day of admission. After randomization, one certified urologist, who was educated about the content of both IC methods and who was able to explain the same information in an equal time (15 minutes), provided information and obtained IC. Completion of the test and questionnaires about subjective understanding and satisfaction using the VAS were requested within 15 minutes after the explanation. During the process, the patients always sat to the right side of the doctor, and questions were not permitted until completing the test. If the patients were accompanied by relatives, one relative was permitted to witness the process. However, the relative was not permitted to have an aide present during the completion of the test and questionnaires. In order to ensure that each patient received identical explanations of the procedure, after the test was completed, the doctor performed one more explanation with the IC form that was not used in the first explanation.
7. Variables
Demographic details, including age, height, weight, educational level, economic status, and smoking status, were collected. In addition, disease-related variables, including hypertension, diabetes, surgical history, International Prostate Symptom Scores, prostate-specific antigen levels, maximum flow rate on uroflowmetry, post void residual urine volume, and prostate volume on transrectal ultrasonography were also included in the data collection.
8. Statistical analysis
All statistical analyses were performed using PASW statistics ver. 17.0 (IBM Co., Armonk, NY, USA). Data were presented as mean±standard deviation with the median and interquartile range for non-parametric variables. The chi-square test was used to compare categorical data, and the independent t-test was used to compare parametric numerical data. Non-parametric numeric variables were compared using the Mann-Whitney U-test. All hypotheses were evaluated in a two-sided manner, and p-values <0.05 were considered to indicate significance. In order to adjust for the influence of age and educational level, linear regression analysis was used to compare scores reflecting objective understanding, subjective understanding, and satisfaction.
RESULTS
A total of 40 male patients, with a mean age of 66.9±6.4 years, completed this study. The characteristics of the patients are presented in Table 1. Demographic parameters, underlying diseases, and BPH-related variables were all comparable between the W-IC group (n=20) and the M-IC group (n=20).
Table 1. Baseline characteristics of the patients.
| Characteristic | Total (n=40) |
Written IC (n=20) |
Multimedia IC (n=20) |
p-value |
|---|---|---|---|---|
| Age (yr) | 66.9±6.4 | 67.3±6.8 | 66.5±6.0 | 0.696 |
| 50s | 4 (10.0) | 2 (10.0) | 2 (10.0) | 0.942 |
| 60s | 23 (57.5) | 11 (55.0) | 12 (60.0) | |
| 70s | 13 (32.5) | 7 (35.0) | 6 (30.0) | |
| Height (cm) | 166.6±4.5 | 166.5±4.6 | 166.7±4.5 | 0.877 |
| Weight (kg) | 66.7±8.4 | 65.8±9.4 | 67.6±7.4 | 0.491 |
| BMI (kg/m2) | 24.0±2.6 | 23.7±3.0 | 24.3±2.3 | 0.468 |
| <25 | 24 (60.0) | 14 (70.0) | 10 (50.0) | 0.197 |
| ≥25 | 16 (40.0) | 6 (30.0) | 10 (50.0) | |
| Educational level | ||||
| Middle school or less | 15 (37.5) | 8 (40.0) | 7 (35.0) | 0.931 |
| High school | 13 (32.5) | 6 (30.0) | 7 (35.0) | |
| University or more | 12 (30.0) | 6 (30.0) | 6 (30.0) | |
| Hypertension | 0.342 | |||
| (−) | 21 (52.5) | 9 (45.0) | 12 (60.0) | |
| (+) | 19 (47.5) | 11 (55.0) | 8 (40.0) | |
| Diabetes | 0.677 | |||
| (−) | 33 (82.5) | 17 (85.0) | 16 (80.0) | |
| (+) | 7 (17.5) | 3 (15.0) | 4 (20.0) | 0.677 |
| IPSS (total) | 21.5±8.4 | 21.7±7.1 | 21.2±9.6 | 0.853 |
| IPSS (QoL) | 4.2±1.2 | 4.2±1.2 | 4.3±1.3 | 0.800 |
| PSA (ng/mL) | 25.6±5.6 | 5.3±5.1 | 6.0±6.6 | 0.716 |
| Qmax | 9.1±3.5 | 8.7±2.8 | 9.5±4.1 | 0.472 |
| PVR (mL) | 42.9±70.2 | 55.2±94.7 | 30.6±28.8 | 0.278 |
| Prostate volume (mL) | ||||
| Total | 50.4±22.9 | 53.4±26.6 | 47.4±18.8 | 0.413 |
| Transitional zone | 28.4±17.6 | 31.4±19.8 | 25.3±14.9 | 0.282 |
Values are presented as mean±standard deviation or number (%).
IC: informed consent, BMI: body mass index, IPSS: International Prostate Symptom Score, QoL: quality of life, PSA: prostate-specific antigen, Qmax: maximum flow rate, PVR: post-void residual urine volume.
1. Objective understanding
The mean score on the test evaluating the patients' objective understanding of HPS-PVP was 10.3±2.5 (out of 15) (Table 2). The mean score for objective understanding in the M-IC group was slightly higher than in the W-IC group (9.9±2.3 vs. 10.6±2.8, p=0.332). When we compared the correct answer rates of each question between the groups, only Q1, which asked about the anatomical location of the prostate, showed a significantly higher correct answer rate in the M-IC group than in the W-IC group (75.0% vs. 100.0%, p=0.047) (Fig. 1).
Table 2. Comparison between groups of parameters evaluating the effectiveness of the informed consent presentation.
| Variable | Total (n=40) | W-IC group (n=20) | M-IC group (n=20) | p-value |
|---|---|---|---|---|
| Objective understandinga | 10.3±2.5 | 9.9±2.3 | 10.6±2.8 | 0.332 |
| 10.0 (9.0~12.0) | 10.0 (8.5~11.0) | 11.0 (9.0~12.0) | ||
| Subjective understandingb | 8.0±1.9 | 7.5±2.1 | 8.6±1.7 | 0.122 |
| 8.5 (6.5~10.0) | 7.0 (5.0~10.0) | 9.0 (8.0~10.0) | ||
| Satisfactionc | 7.9±1.7 | 7.4±1.7 | 8.5±1.5 | 0.033* |
| 8.0 (7.0~10.0) | 7.0 (6.5~8.0) | 9.0 (7.0~10.0) |
Values are presented as mean±standard deviation or median (interquartile range).
W-IC: written informed consent, M-IC: multimedia informed consent.
aMaximum points=15; bMaximum points=10; cMaximum points=10. *p<0.05.
Fig. 1. Comparison of the objective understanding scores for each question. Q1: anatomy of the prostate, Q2: function of the prostate, Q3: etiology of lower urinary tract symptoms/benign prostatic hyperplasia (LUTS/BPH), Q4: symptoms of LUTS/BPH, Q5: diagnosis of LUTS/BPH, Q6: treatment modalities for LUTS/BPH, Q7: comparison of surgical treatment modalities, Q8: advantages and disadvantages of high-performance system photoselective vaporization of the prostate (HPS-PVP), Q9: HPS-PVP surgical procedure; Q10: course of hospital treatment after HPS-PVP, Q11: postoperative treatment in hospital, Q12: precautions after surgery, Q13: early complications of HPS-PVP, Q14: late complications of HPS-PVP, Q15: treatment of complications. *p<0.05.

2. Influence of age and educational level on objective understanding
Older patients tended to have lower scores for objective understanding (Spearman's coefficient=–0.241, p=0.134) (Table 3). In contrast, patients with more education had higher objective understanding scores (Spearman's coefficient=0.439, p=0.005). The difference in the mean test scores between the two groups tended to be highest in patients in their 70s. Patients whose highest level of education was high school showed the largest differences in objective understanding scores, whereas a minimal difference was observed in patients with a middle school or university education.
Table 3. Objective understanding scores by age and educational level of the patients.
| Variable | W-IC group | M-IC group | p-value | ||
|---|---|---|---|---|---|
| Number | Scores | Number | Scores | ||
| Age (yr) | |||||
| 50s | 2 | 11.5±2.1 | 2 | 11.5±3.5 | 1.000 |
| 11.5 (10.0~13.0) | 11.5 (9.0~14.0) | ||||
| 60s | 11 | 10.2±2.5 | 12 | 10.8±4.1 | 0.618 |
| 10.0 (9.5~1.5) | 11.0 (9.5~12.0) | ||||
| 70s | 7 | 9.0±3.3 | 6 | 9.8±16.6 | 0.426 |
| 9.0 (8.0~10.5) | 10.5 (8.0~12.0) | ||||
| Educational levels | |||||
| Middle school or less | 8 | 9.1±2.4 | 7 | 8.7±2.9 | 0.906 |
| 9.5 (8.5~10.0) | 9.0 (8.0~10.5) | ||||
| High school | 6 | 9.3±7.1 | 7 | 11.7±2.1 | 0.190 |
| 10.5 (6.0~11.0) | 11.0 (10.5~13.0) | ||||
| University or more | 6 | 11.5±5.1 | 6 | 11.5±5.9 | 0.935 |
| 12.0 (10.0~13.0) | 11.5 (1.0~13.0) | ||||
Values are presented as number only, mean±standard deviation, or median (interquartile range).
W-IC: written informed consent, M-IC: multimedia informed consent.
3. Subjective understanding and satisfaction
The subjective understanding scores measured by the VAS (range, 0~10) were somewhat higher in the M-IC group than in the W-IC group (Table 2). However, the satisfaction score regarding the process of giving the information and obtaining IC was significantly higher in the M-IC group than that in the W-IC group. After adjusting for the influence of patient age and educational level, the positive effect of the M-IC presentation on satisfaction scores was preserved (difference=1.098, 95% confidence interval, 0.133~2.062) (Table 4).
Table 4. Adjusted differences in outcome parameters between the groups.
| Variable | B | 95% CI | p-value |
|---|---|---|---|
| Objective understanding | |||
| Age | −1.038 | −2.231~0.155 | 0.086 |
| Educational levels | 1.274 | 0.382~2.166 | 0.006 |
| Multimedia IC | 0.584 | −0.876~2.045 | 0.422 |
| Subjective understanding | |||
| Age | −0.079 | −0.175~0.016 | 0.099 |
| Educational levels | 0.263 | −0.466~0.993 | 0.468 |
| Multimedia IC | 0.973 | −0.217~2.163 | 0.106 |
| Satisfaction | |||
| Age | −0.022 | −0.099~0.056 | 0.574 |
| Educational levels | 0.703 | 0.112~1.293 | 0.021 |
| Multimedia IC | 1.098 | 0.133~2.062 | 0.027 |
CI: confidence interval, IC: informed consent.
DISCUSSION
The conventional W-IC form for HPS-PVP served its purpose moderately well. The mean scores of objective understanding were approximately 66% in both IC groups, which was expected, as the test to evaluate objective understanding included five (1/3) highly difficult questions. Although we developed a new M-IC with more intuitive and easier-to-understand content, the M-IC did not improve patients' objective understanding. The absence of differences in the objective understanding scores suggest that the conventional method of obtaining IC was not entirely ineffective, not that M-IC is not needed. Although the M-IC presentation failed to improve objective and subjective understanding in this study, it showed better results regarding the subjective satisfaction of the patients.
Trials to improve the efficacy of IC have been performed in various studies [11,12,13,14,15,16,17,18,19]. Most of the trials used multimedia content, including audio, video, and animations or multimedia materials such as videotapes, CD-ROMs, and DVDs. Those studies found that those methods enhanced patients' objective and subjective understanding and satisfaction. M-IC, interactive multimedia programs, and multimedia DVDs improved comprehension for patients undergoing cholecystectomy [11,12,13]. These positive effects were confirmed in studies using M-IC before gastric banding surgery, ankle fracture surgery, and knee arthroscopic surgery [14,15,16].
Strategies to support and enhance informed decision-making have been tried in patients with prostate cancer [20,21]. One study evaluated the currently available educational materials about prostate cancer treatment and concluded that the information in the materials was accurate and balanced, but did not include some content that was crucial for IC [20]. In another study, when patients with prostate cancer used a decision aid and were interviewed twice, the use of the decision aid had positive effects, and the patients became more active in the decision- making process [21]. These results suggest that only providing informative material is not effective, and that an additional explanation by a physician is required. This was the reason why we did not use a recorded voice for the M-IC presentation, but instead chose to have a certified urologist convey the information contained in the M-IC presentation.
BPH is an important urologic disease, and obtaining IC before surgical treatment is crucial. First, BPH and related LUTS are very common in aging men [22]. The incidence of severe LUTS is 6% to 28%, and increases with age [22,23,24]. Since the risk of acute urinary retention in men with moderate to severe LUTS is approximately 13.7% over 10 years [25], many require surgical treatment, although the indications for surgery vary [26]. However, due to its benign nature, surgical treatment is not urgent in most cases. Delaying the surgical treatment does not lead to serious sequelae, and deciding not to receive the operation could be a reasonable option based on patient preferences. Furthermore, a range of surgical treatment modalities can be selected, including traditional transurethral prostatectomy (TURP), bipolar TURP, and various laser (e.g., rubidium titanyl phosphate, holmium, thulium, and diode) procedures [4,5]. Therefore, voluntary informed decision-making is more necessary for this optional procedure to treat benign disease.
One important finding in this study was that objective understanding was influenced by the age and educational level of the patients. Patients whose highest educational level was high school and who were in their 70s tended to have a better objective understanding of the operation. Although we developed the M-IC presentation to provide easy-to-understand information for men who only graduated middle school, the improvement in comprehension was not remarkable in these men. This may have been because they were not familiar with computer-based multimedia presentations.
Although this study was a randomized controlled study, it had several limitations. First, we could not control for self-seeking of information before IC. The large amount of information available on websites could have influenced the objective understanding scores. Second, we did not include patients whose educational level was below middle school, because most such patients do not make autonomous decisions and depend on a caregiver. Finally, we used a newly developed test to evaluate the degree of comprehension, so the results could not be compared with other studies. However, this could not be avoided because the content of the test should be extracted from the content included in the IC material. Despite these shortcomings, our results demonstrate that M-IC improved the satisfaction of patients scheduled for optional surgery. Our results could justify expanding M-IC to other procedures.
CONCLUSIONS
Both the conventional W-IC form and a newly developed M-IC presentation led to a moderate level of understanding in patients planning to undergo HPS-PVP surgery. The objective and subjective understanding scores were not significantly different between the W-IC and M-IC groups. However, the satisfaction of patients about the process of obtaining IC was higher in the M-IC group. This increase in the satisfaction score warrants the wider adoption of M-IC, and further efforts to enhance the communication of relevant information are needed.
ACKNOWLEDGEMENTS
This study was supported by a grant (No. 03-2011-12) from SMG-SNU Boramae Medical Center.
Appendix
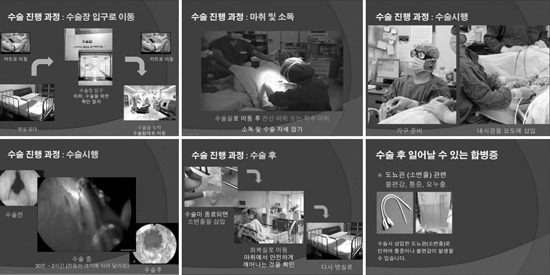
The multimedia informed consent presentation (samples from Microsoft PowerPoint). Upper left: an explanation of the transition from the ward to the operation room (an animation was used). Upper middle: a still-cut of a video clip that explained spinal anesthesia. Upper right and lower left: an explanation of the surgical procedure (video clip). Lower middle; an explanation of the postoperative procedure (an animation was used). Lower right: an explanation of one of the possible postoperative complications.
Footnotes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.
References
- 1.Angelos P. Ethics and surgical innovation: challenges to the professionalism of surgeons. Int J Surg. 2013;11(Suppl 1):S2–S5. doi: 10.1016/S1743-9191(13)60003-5. [DOI] [PubMed] [Google Scholar]
- 2.Jones B. Legal aspects of consent. BJU Int. 2000;86:275–279. doi: 10.1046/j.1464-410x.2000.00292.x. [DOI] [PubMed] [Google Scholar]
- 3.Pape T. Legal and ethical considerations of informed consent. AORN J. 1997;65:1122–1127. doi: 10.1016/s0001-2092(06)62955-4. [DOI] [PubMed] [Google Scholar]
- 4.Son H, Song SH, Paick JS. Current laser treatments for benign prostatic hyperplasia. Korean J Urol. 2010;51:737–744. doi: 10.4111/kju.2010.51.11.737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lusuardi L, Hruby S, Janetschek G. New emerging technologies in benign prostatic hyperplasia. Curr Opin Urol. 2013;23:25–29. doi: 10.1097/MOU.0b013e32835abd34. [DOI] [PubMed] [Google Scholar]
- 6.Issa MM, Setzer E, Charaf C, Webb AL, Derico R, Kimberl IJ, et al. Informed versus uninformed consent for prostate surgery: the value of electronic consents. J Urol. 2006;176:694–699. doi: 10.1016/j.juro.2006.03.037. [DOI] [PubMed] [Google Scholar]
- 7.Mulsow JJ, Feeley TM, Tierney S. Beyond consent--improving understanding in surgical patients. Am J Surg. 2012;203:112–120. doi: 10.1016/j.amjsurg.2010.12.010. [DOI] [PubMed] [Google Scholar]
- 8.Uzzaman MM, Tayeh S, Sinha S, Ratnasingham K, Stoker DL. Consenting practice for laparoscopic cholecystectomy -are we doing enough to warn patients about their operation? Int J Surg. 2011;9:643–647. doi: 10.1016/j.ijsu.2011.08.004. [DOI] [PubMed] [Google Scholar]
- 9.Masood J, Hafeez A, Wiseman O, Hill JT. Informed consent: are we deluding ourselves? A randomized controlled study. BJU Int. 2007;99:4–5. doi: 10.1111/j.1464-410X.2007.06516.x. [DOI] [PubMed] [Google Scholar]
- 10.Fink AS, Prochazka AV, Henderson WG, Bartenfeld D, Nyirenda C, Webb A, et al. Predictors of comprehension during surgical informed consent. J Am Coll Surg. 2010;210:919–926. doi: 10.1016/j.jamcollsurg.2010.02.049. [DOI] [PubMed] [Google Scholar]
- 11.Bollschweiler E, Apitzsch J, Obliers R, Koerfer A, Mönig SP, Metzger R, et al. Improving informed consent of surgical patients using a multimedia-based program? Results of a prospective randomized multicenter study of patients before cholecystectomy. Ann Surg. 2008;248:205–211. doi: 10.1097/SLA.0b013e318180a3a7. [DOI] [PubMed] [Google Scholar]
- 12.Stergiopoulou A, Birbas K, Katostaras T, Mantas J. The effect of interactive multimedia on preoperative knowledge and postoperative recovery of patients undergoing laparoscopic cholecystectomy. Methods Inf Med. 2007;46:406–409. doi: 10.1160/me0406. [DOI] [PubMed] [Google Scholar]
- 13.Wilhelm D, Gillen S, Wirnhier H, Kranzfelder M, Schneider A, Schmidt A, et al. Extended preoperative patient education using a multimedia DVD-impact on patients receiving a laparoscopic cholecystectomy: a randomised controlled trial. Langenbecks Arch Surg. 2009;394:227–233. doi: 10.1007/s00423-008-0460-x. [DOI] [PubMed] [Google Scholar]
- 14.Eggers C, Obliers R, Koerfer A, Thomas W, Koehle K, Hoelscher AH, et al. A multimedia tool for the informed consent of patients prior to gastric banding. Obesity (Silver Spring) 2007;15:2866–2873. doi: 10.1038/oby.2007.340. [DOI] [PubMed] [Google Scholar]
- 15.Rossi M, McClellan R, Chou L, Davis K. Informed consent for ankle fracture surgery: patient comprehension of verbal and videotaped information. Foot Ankle Int. 2004;25:756–762. doi: 10.1177/107110070402501011. [DOI] [PubMed] [Google Scholar]
- 16.Rossi MJ, Guttmann D, MacLennan MJ, Lubowitz JH. Video informed consent improves knee arthroscopy patient comprehension. Arthroscopy. 2005;21:739–743. doi: 10.1016/j.arthro.2005.02.015. [DOI] [PubMed] [Google Scholar]
- 17.Luck A, Pearson S, Maddern G, Hewett P. Effects of video information on precolonoscopy anxiety and knowledge: a randomised trial. Lancet. 1999;354:2032–2035. doi: 10.1016/s0140-6736(98)10495-6. [DOI] [PubMed] [Google Scholar]
- 18.Danino AM, Chahraoui K, Frachebois L, Jebrane A, Moutel G, Herve C, et al. Effects of an informational CD-ROM on anxiety and knowledge before aesthetic surgery: a randomised trial. Br J Plast Surg. 2005;58:379–383. doi: 10.1016/j.bjps.2004.10.020. [DOI] [PubMed] [Google Scholar]
- 19.Keulers BJ, Welters CF, Spauwen PH, Houpt P. Can face-to-face patient education be replaced by computer-based patient education? A randomised trial. Patient Educ Couns. 2007;67:176–182. doi: 10.1016/j.pec.2007.03.012. [DOI] [PubMed] [Google Scholar]
- 20.Fagerlin A, Rovner D, Stableford S, Jentoft C, Wei JT, Holmes-Rovner M. Patient education materials about the treatment of early-stage prostate cancer: a critical review. Ann Intern Med. 2004;140:721–728. doi: 10.7326/0003-4819-140-9-200405040-00012. [DOI] [PubMed] [Google Scholar]
- 21.Isebaert S, Van Audenhove C, Haustermans K, Junius S, Joniau S, De Ridder K, et al. Evaluating a decision aid for patients with localized prostate cancer in clinical practice. Urol Int. 2008;81:383–388. doi: 10.1159/000167833. [DOI] [PubMed] [Google Scholar]
- 22.Roehrborn CG. The epidemiology of acute urinary retention in benign prostatic hyperplasia. Rev Urol. 2001;3:187–192. [PMC free article] [PubMed] [Google Scholar]
- 23.Bosch JL, Kranse R, van Mastrigt R, Schröder FH. Reasons for the weak correlation between prostate volume and urethral resistance parameters in patients with prostatism. J Urol. 1995;153:689–693. doi: 10.1097/00005392-199503000-00039. [DOI] [PubMed] [Google Scholar]
- 24.Han DH, Choo SH, Chung JW, Hong JH, Lee SW. Can 80 W KTP laser vaporization effectively relieve the obstruction in benign prostatic hyperplasia?: a nonrandomized trial. World J Mens Health. 2012;30:160–165. doi: 10.5534/wjmh.2012.30.3.160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Parsons JK, Carter HB, Partin AW, Windham BG, Metter EJ, Ferrucci L, et al. Metabolic factors associated with benign prostatic hyperplasia. J Clin Endocrinol Metab. 2006;91:2562–2568. doi: 10.1210/jc.2005-2799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.McVary KT, Roehrborn CG, Avins AL, Barry MJ, Bruskewitz RC, Donnell RF, et al. Update on AUA guideline on the management of benign prostatic hyperplasia. J Urol. 2011;185:1793–1803. doi: 10.1016/j.juro.2011.01.074. [DOI] [PubMed] [Google Scholar]