

Abstract
Background
mHealth has become a valuable tool for providing health care services in developing countries. Despite the potential benefits of mHealth, its adoption remains a very challenge in developing countries like Bangladesh. The aim of this study is to investigate the factors that affect the adoption of mHealth services in Bangladesh using Extended Technology Acceptance Model (TAM).
Methods
Data were collected from over 250 respondents in Dhaka, Bangladesh. The data were analyzed using the Partial Least Squares (PLS) method, a statistical analysis technique based on the Structural Equation Modeling (SEM).
Results
The study found that perceived ease of use, perceived usefulness and subjective norm (p < 0.05) had significant positive impact on the intention to adopt mHealth services. Surprisingly, the effects of personal innovativeness in IT (p > 0.05) on mHealth adoption were insignificant. This study also revealed that gender was strongly associated with the adoption and use of mHealth in developing countries.
Conclusions
The findings of this study can be used by government, policy makers, and mobile phone Company to maximize the acceptance of mHealth services in Bangladesh. The paper concludes with a discussion of research results and draws several implications for future research.
Keywords: mHealth, Developing country, Adoption
Background
Over the past decade, the rapid advances in mobile and wireless technologies have paved the way to transform health service delivery across the world. The unprecedented spread of mobile technologies and their innovative application to address health priorities has developed a new field of e-Health, known as mHealth [1]. mHealth is defined as “the application of wireless technologies to transmit different data contents and services which are accessible by health workers through mobile devices such as mobile phones, PDAs, smart phones and Tablet PCs” [2]. It provides medical and health care services to both health professionals and users. The work of health professional (i.e doctors, nurses) may be better supported and user may obtain useful information and guidance to manage their health better by mHealth [3]. Moreover, mHealth has transformed the healthcare in developing countries by serving the unserved [4].
Wireless technologies and mobile phones have reached far more people than any other new advanced information and communication technologies, especially in developing countries. Although the use of internet has also increased extensively in recent years, about 31 % of the people in developing countries had internet access in 2013, whereas nearly 80 % had mobile phone subscriptions [5]. A World Health Organization (WHO) report in 2011 suggested that mobile phone coverage had reached 89 % of all Bangladeshi adults [6]. At the end of the December 2014, the total number of Mobile Phone subscribers has reached 120.350 million in Bangladesh [7]. Bangladesh Demographic and Health (DHS) surveys of 2007 and 2011 showed that household mobile phones ownership has increased from 32 to 78 %, varying from 75 % in rural areas to 89 % in urban [8, 9]. In addition, Bangladesh claimed to have the cheapest mobile phone call rates in the world [10]. Therefore, it is the golden opportunity for Bangladesh to develop mobile health services for their citizen so that they could better manage their health. Through mobile health services, user can seek medical advice; make appointment with doctors; access medical test result; and access to personal health information [11].
In recent years, the number of chronic disease among younger citizen is gradually increasing due to different factors such as smoking, intensive academic and social pressure [12]. More than 70 % world’s smokers, most of them are young, are living in just ten countries and Bangladesh is one of them. In Bangladesh, more than 50 % of younger males and 30 % of younger females consume tobacco in any form, smoking or smokeless [13]. In developing countries like Bangladesh, smoking is the main causes of different diseases which lead to premature death for young citizen. Young citizen in Bangladesh also suffer from hypertension and Type 2 diabetic which are considered to be two of the leading causes of death worldwide and risk factors for strokes, heart attacks, heart failures, cardiovascular diseases and coronary artery diseases [14].
Mobile phones based health services, commonly known as mHealth, provides personalized and tailored health care services to those who need it, especially young citizen [11]. It has been regarded as best tools for curing diseases and improving health condition [15, 16]. mHealth services leads people to manage chronic disease more effectively and improve their quality of life. It can prevent and control hypertension and Type 2 diabetic. It has been also gained popularity for smoking cessation for younger citizen in developing countries [17, 18]. mHealth intervention can reduce cost, better reach, increased interaction between patients and doctors and easier as well as faster to send messages regarding the diseases and health. Adoption of mHealth can improve health, food intake, exercise, sleep, blood sugar and other physiological states and behaviors.
Although there have been considerable benefits of mHealth services, they have encountered numerous challenges and difficulties as a newly emerging phenomenon [19]. In Bangladesh, this service is still in the infancy stage and requires extensive research on user adoption process, especially considering users who have vast knowledge (i. e young citizen) about using mobile or smart phone. However, very few to no studies consider the adoption of mHealth services with regard to young citizen in developing countries. Therefore, factors that influences the adoption of mHealth services by younger citizen must be investigated - a population that is most favorably placed in the adoption of innovations and technology. It is also important to consider the gender issues in mHealth adoption because the gender gap still exists in developing countries. Research found that female is less interested than male to use new technology, a ‘gender gap’ almost twice that for all low- and middle-income countries in South East Asia [20]. So, this study also includes gender as a moderating variable. The objective of this study is to identify the factors that influence the adoption of mHealth services among younger people in Bangladesh.
Theoretical framework
There are different theories of technology acceptance namely the theory of planned behavior (TPB), innovation diffusion theory (IDT), theory of reasoned action (TRA), technology acceptance model (TAM) and theory of innovation Adoption (TIA). Among them, the TAM is the most influential model for technology adoption. Though the basic TAM presents a rigorous explanation in predicting the user’s acceptance of technology, some studies suggest that additional explanatory variables may be needed depending on the specific technology context [21]. Therefore, this study extends the TAM (shown in Fig. 1) with two additional salient variables, subjective norm and personal innovativeness in IT, to enhance prediction of intention to use mHealth in Bangladesh context. Gender was included in the proposed model as factors to moderate the effect of dependent and independent variable.
Fig. 1.
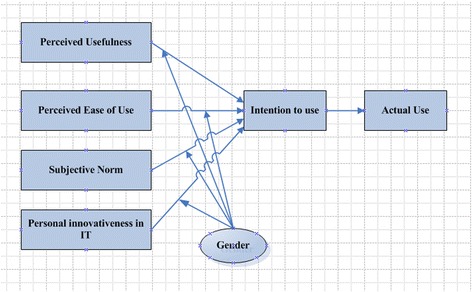
Research model
The TAM hypothesizes that the most important determinant of actual technology use is the intention to use the technology, whereas intention in turn, is predicted by perceived usefulness (PU) and perceived ease of use (PEU) [22]. TAM has received much attention from researchers and considered as a prevailing model for predicting usage intention and acceptance behavior [23]. Since the introduction of TAM, a number of studies have applied it to predict user acceptance of variety IT applications such as wireless internet [24], online shopping [25], email and voice mail [26], e-Health [27], clinical information systems [28] and mHealth [29, 30].
Perceived Usefulness (PU)
Perceived usefulness is defined as “the degree to which a person believes that use of the system will enhance his or her performance” [31]. Many existing studies have demonstrated that perceived usefulness positively influences behavioral intention to use a new technology such as online banking [32], e-ticketing [33], PDA [34], e-learning [35], mobile learning [36], online system [37] and mobile services [38]. In the context of mHealth, researchers found that PU is a vital factor which determines the adoption of mHealth since users consider its benefits [39, 40]. Based on the above literature, we proposed the following hypotheses:
: Perceived Usefulness has a positive influence on the intention to use mHealth services among younger in Bangladesh.
Perceived Ease of Use (PEU)
Perceived ease of use is defined as “the degree to which a person believes that using the system will be free of effort” [31]. The researchers have suggested that ease of use is a major attribute of mHealth applications [41], electronic health record [42], mobile banking [43], e-government [44], and online banking [45]. Consequently, the following hypothesis is suggested:
-
H2
: Perceived ease of use has a positive influence on the intention to use mHealth services among younger in Bangladesh.
Subjective norm
Subjective norm is defined as “person’s perception that most people who are important to him think he should or should not perform the behavior question” [46]. Existing research on information systems found a significant relationship between subjective norm and adoption of IS [47]. The researcher has suggested that subjective norm positively influence the intention to use electronic brokerages service [48], online services [49], e-payment [50], mobile banking [51], internet banking [52], instant messaging [53] and mHealth [54]. Consequently, the following hypothesis is suggested:
-
H3
: Subjective norm has a positive influence on the intention to use mHealth services among younger in Bangladesh.
Personal innovativeness in IT
Personal innovativeness is defined as “the degree to which an individual is relatively earlier in adopting new ideas” [55]. Agarwal and Prasad [56] empirically tested the influence of personal innovativeness in IT on information technology use. Many existing studies have demonstrated that personal innovativeness in IT significantly influences the intention to use a new technology such as internet [57], public grid computing [58], PDA [59], information systems [60] and mHealth [54]. Consequently, the following hypothesis is suggested:
-
H4
: Personal innovativeness in IT has a positive influence on the intention to use mHealth services among younger in Bangladesh.
The relationship between intention to use and actual use of technology in TAM model are also empirically examined in different studiest. The variable of “Actual Use” (AU) has been measured, by intention to use [61]. Turner et al. [62] conducted a systematic literature review on TAM based on 6 digital libraries. They found that BI is highly correlated with actual usage of 79 relevant empirical studies. Legris [63] confirmed that intention to use influence the actual use of technology. Horton et al. [64] found that higher the intention to use, the higher the actual use of intranet. BI–AU relationships are also tested by Lim et al. [30] in their study of mHealth adoption. Therefore, we propose the following hypothesis:
-
H5
: Intention to use has a positive influence on actual use of mHealth services among younger in Bangladesh.
The moderating role of gender concern
Gender, as a moderating factor, received less consideration in past technology adoption research compared with other factors such as age, culture and experience. Although gender are considered as an important factor in technology adoption, original TAM makes no references of gender differences and genders are not examined in IT acceptance model [65]. Generally, male has less anxious and more positive attitudes about technology innovations [66]. Wang et al. [67] explored that gender differences moderate the effects of learning on m-learning use intention. Gefen and Straub [25] found that male and female differ in their perception of e-mail use. Van et al. [68] suggest that man and woman would differ in their acceptance of web site and web-based shopping. Ong and Lai [69] have suggested that male’s score on the PU and PEU of e-learning is higher than scores of female. Therefore, we proposed the following hypotheses:
-
H6
: Gender has a significant moderating role in the relationship between PU and intention to use mHealth services among younger in Bangladesh.
-
H7
: Gender has a significant moderating role in the relationship between PEU and intention to use mHealth services among younger in Bangladesh.
-
H8
: Gender has a significant moderating role in the relationship between subjective norm and intention to use mHealth services among younger in Bangladesh.
-
H9
: Gender has a significant moderating role in the relationship between personal innovativeness in IT and intention to use mHealth services among younger in Bangladesh.
Methods
Research setting
The target population for this study was the younger citizen in Bangladesh. This study used convenience sampling method as survey instrument. Convenience sampling is “a type of nonprobability sampling which involves the sample being drawn from that part of the population which is close to hand” [70]. Moreover, it is cost effective and has been widely used in (Information Systems (IS) research [71]. The sample was taken from younger citizens in Dhaka City of Bangladesh, who were students at the University of Dhaka. They were considered to be suitable because of their comfortability with the use of technology for activities such as searching information, gaming in addition to simple communication. Prior to commencing the research, ethical approval was sought and obtained from the Center for Modern Information Management, School of Management, Huazhong University of Science and Technology, Wuhan, China. The author also contacted with the chairman of MIS department at University of Dhaka to seek permission to collect data from students. All participants in the research were given consent forms and information sheets which clearly explained the purpose of the study. Respondents were also made aware of their rights to withdraw participation at any time during the study. Respondents were also made aware of the fact that they may request the findings of the research once it is completed. The survey was conducted in November 2014.
Measurement
All items in this study were adopted from previous studies. The items were modified to match the context of this study related to mHealth in the context of Bangladesh. PU and PEU were measured with four items adapted from Davis [22], Chau & Hu [72]. Subjective norm with three items was adapted from Wu and Chen [73]. Personal innovativeness in IT with three items was adapted from Agarwal and Prasad, [56], Yi et al. [74]. Intention to use with three items was adapted from Venkatesh et al. [46], Davis [22]. Finally, actual use with three items was adapted from Taylor and Todd [75], Davis and Venkatesh [76]. The details of the measurement items and the source of literature for each construct are presented in Table 1.
Table 1.
Measurement items
| Items | References |
|---|---|
| Perceived Usefulness | |
| PU1: Using the mHealth services will improve my life quality | Davis (1989) [22, 31], Chau & Hu (2002) [72] |
| PU2: Using the mHealth services will make my life more convenient | |
| PU3: Using the mHealth services will make me more effective in my life | |
| PU4: Overall, I find the mHealth services to be useful in my life | |
| Perceived Ease of Use | |
| PEU1: Learning to operate the mHealth services will be easy for me | Davis (1989) [22, 31], Chau & Hu (2002) [72] |
| PEU2: I can easily become skillful at using the mHealth services | |
| PEU3: I can get the mHealth services to do what I want it to do | |
| PEU4: Overall, the mHealth services are easy to use | |
| Subjective Norm | |
| SN1. My close friends think that I can use mHealth | Wu and Chen (2005) [73] |
| SN2. My close friends think that I should use mHealth | |
| SN3. My close friends think that I must use mHealth | |
| Personal innovativeness in IT | |
| PIIT1: If I heard about a new information technology, I would look for ways to experiment with it. | Agarwal and Prasad, (1998) [56], Yi et al. (2006) [74] |
| PIIT2: Among my peers, I am usually the first to try out new information technologies. | |
| PIIT3: In general, I am not hesitant to try out new information technologies. | |
| Intention to Use | |
| INT1: I have high intention to use the mHealth service | Venkatesh et al. (2003) [46], Davis (1989) [22, 31]. |
| INT2: I intend to learn about using mHealth services | |
| INT3: I plan to use mHealth services to manage my health | |
| Actual Use | |
| ACT1: mHealth service is a pleasant experience | Taylor and Todd (1995) [75], Davis and Venkatesh (2004) [76]. |
| ACT2: I use mHealth service currently | |
| ACT3: I spend a lot of time on mHealth service |
Questionnaire design and data collection
The data for this study was collected through a structured questionnaire consisting of two parts. Part A contains the demographic information, while Part B includes previously validated questionnaires for the different constructs. The items of the construct were measured using a 5-point Likert, with answer choices ranging from (1) “strongly disagree” to (5) “strongly agree”. The questionnaires were distributed among 250 respondents in Dhaka. Out of 250 questionnaires, 234 were returned to the researcher. However, 7 incomplete questionnaires were excluded from the study.
Data analysis
Data from questionnaires were inserted into Microsoft excel and imported into SmartPLS software, a technique of Structural Equation Modeling (SEM), for statistical analysis. Structural Equation Modeling is widely accepted paradigm to gauge the validity of meaty theories with empirical data. It is an extensive statistical representation of general linear modeling. One of the notable applications of SEM is that it can be applied to explore out the relationships among latent constructs and which are indicated by multiple measures. SEM is composed of two the evaluation of twin models: measurement model and a path model. Path models is an extensive form of multiple regression model in which various multiple regression are estimated simultaneously [77]. In other words, path analysis can be regarded as a special case of SEM in which the structural relations among latent variables are molded.
Result
Demographic information
Table 2 shows the demographic characteristics of the respondents. There is no large gap between male and female respondents (59 and 41 %). About 57 % of the respondents’ ages are between the 20 and 30, half of them are less than 20 (27 %). Majority of the respondents (86 %) had less than 6 years of IT experiences, while only 3 % had more than 10 years of IT experiences. Around 42 % had Master’s degree and 26 % had Bachelor degree.
Table 2.
Demographics of respondents
| Descriptions | Frequency | Percentage | |
|---|---|---|---|
| Gender | Male | 133 | 59 % |
| Female | 94 | 41 % | |
| Educational Qualification | Bachelor | 59 | 26 % |
| Masters | 96 | 42 % | |
| Others | 72 | 32 % | |
| Age | Less than 20 | 61 | 27 % |
| 20–30 | 129 | 57 % | |
| More than 30 | 37 | 16 % | |
| IT experience | Less than 1 years | 22 | 10 % |
| 1–3 years | 68 | 30 % | |
| 4–6 years | 105 | 46 % | |
| 7–9 years | 26 | 11 % | |
| More than 10 years | 6 | 3 % | |
Measurement model
The validity and reliability of the measures should be examined before testing the hypothesis [78]. The reliability was evaluated by considering Cronbach’s alpha and composite reliability. The reliability is considered to be satisfactory when composite reliability and Cronbach’s alpha have value greater than 0.70. Convergent validity is considered to be satisfactory when measurement constructs have an average variance extracted (AVE) of at least 0.50 and items loading are well above 0.50 [79]. Table 3 presents the composite reliability, Cronbach’s alpha and average variance extracted (AVE), while Table 4 shows the item loading.
Table 3.
The measurement model
| Constructs | CR | Cronbach’s Alpha | AVE |
|---|---|---|---|
| Actual Use | 0.9200 | 0.8693 | 0.7935 |
| Intention to Use | 0.8932 | 0.8198 | 0.7364 |
| Perceived Ease of Use | 0.9176 | 0.8803 | 0.7361 |
| Perceived Usefulness | 0.8911 | 0.8380 | 0.6719 |
| Personal innovativeness in IT | 0.9449 | 0.9335 | 0.8511 |
| Subjective Norm | 0.9031 | 0.9355 | 0.7582 |
AVE average variance extracted, CR composite reliability
Table 4.
Cross-loading matrix
| ACT | INT | PEU | PI | PU | SN | |
|---|---|---|---|---|---|---|
| ACT1 | 0.8289 | 0.6314 | 0.6236 | 0.2337 | 0.4696 | −0.1106 |
| ACT2 | 0.9119 | 0.7525 | 0.7417 | 0.1027 | 0.5053 | −0.1182 |
| ACT3 | 0.9283 | 0.7993 | 0.795 | 0.1321 | 0.5379 | −0.1969 |
| INT1 | 0.6533 | 0.8102 | 0.6511 | 0.058 | 0.4363 | −0.0398 |
| INT2 | 0.6735 | 0.8519 | 0.6671 | 0.0824 | 0.4044 | −0.0084 |
| INT3 | 0.7822 | 0.9095 | 0.7347 | 0.1032 | 0.487 | −0.148 |
| PEU1 | 0.8053 | 0.7592 | 0.8788 | 0.0945 | 0.5026 | −0.1314 |
| PEU2 | 0.6453 | 0.6346 | 0.8516 | 0.1239 | 0.4231 | −0.1523 |
| PEU3 | 0.5912 | 0.599 | 0.8033 | −0.0268 | 0.3111 | −0.0417 |
| PEU4 | 0.7262 | 0.7299 | 0.8954 | −0.0484 | 0.4602 | −0.0478 |
| PI1 | 0.0896 | −0.0216 | −0.0424 | 0.8940 | 0.4666 | −0.8265 |
| PI2 | 0.1321 | 0.0492 | −0.0118 | 0.9133 | 0.4903 | −0.7864 |
| PI3 | 0.1598 | 0.0868 | 0.0492 | 0.9592 | 0.4969 | −0.8178 |
| PU1 | 0.4876 | 0.4607 | 0.4625 | 0.3904 | 0.8194 | −0.3841 |
| PU2 | 0.3983 | 0.3387 | 0.3405 | 0.3927 | 0.7878 | −0.4056 |
| PU3 | 0.4658 | 0.4253 | 0.4378 | 0.5039 | 0.8303 | −0.5416 |
| PU4 | 0.4942 | 0.4512 | 0.3865 | 0.4335 | 0.8402 | −0.455 |
| SN1 | −0.1425 | −0.037 | −0.0824 | −0.8696 | −0.488 | 0.8423 |
| SN2 | −0.1018 | −0.0485 | −0.0644 | −0.7905 | −0.5011 | 0.9776 |
| SN3 | −0.0369 | 0.0282 | 0.0007 | −0.8093 | −0.4093 | 0.7806 |
It is apparent from the Table 3 that the Cronbach’s alpha values ranged from 0.81 to 0.93, and composite reliability ranged from 0.89 to 0.94 which indicates adequate internal reliability. Item loading, ranged from 0.78 to 0.97 and AVE, ranged from 0.67 to 0.85, are greater than the recommended level. Therefore, conditions for convergent validity were met.
On the other hand, the discriminant validity was examined by the square root of the AVE and cross loading matrix. The square root of the AVE of a construct must be larger than its correlation with other construct for satisfactory discriminant validity [80]. What is interesting in this table is that the square roots of AVE, shown in Table 5, were greater than their corresponding correlation, representing that our data had good discriminant validity.
Table 5.
Correlation matrix and square root of the AVE
| ACT | INT | PEU | PI | PU | SN | |
|---|---|---|---|---|---|---|
| ACT | 0.8907 | |||||
| INT | 0.8218 | 0.8581 | ||||
| PEU | 0.8134 | 0.7986 | 0.8579 | |||
| PI | 0.1693 | 0.0956 | 0.0423 | 0.9225 | ||
| PU | 0.5671 | 0.5168 | 0.5005 | 0.5251 | 0.8197 | |
| SN | −0.1620 | −0.0798 | −0.1094 | −0.8433 | −0.5448 | 0.87075 |
The structural model
The structural model was constructed to identify the path direction and strength of relationships among the latent variable in the research model. Bootstrapping method was used to test the hypothesis. First, we tested the relationship between endogenous and exogenous variable. Then, we tested the moderating effect of gender. Table 6 showed the path coefficient (β) and t-statistics. It was found that PU (t = 4.0398, β = 0.2095), PEU (t = 15.5538, β = 0.7005) and subjective norm (t = 2.2041, β = 0.2207) had significant effect on intention to use mHealth adoption, while personal innovativeness in IT (t = 1.2845, β = 0.1216) had no significant effect on intention to use mHealth. The study also found that intention to use mHealth (t = 0.8228, β = 51.2824) had significant effect on actual use of mHealth. Therefore, among the primary hypothesis, H1, H2, H3, and H5 were supported, whereas H4 was not supported. From the table, it can be stated that the model explains 67.5 % of the variance in intention to use mHealth (R2 = .675) and 65.5 % of variance in actual use of mHealth (R2 = .655).
Table 6.
Structural model
| Path | β | t Statistics | Comments |
|---|---|---|---|
| INT - > ACT | 0.8228 | 51.2824 | Supported |
| PEU - > INT | 0.7005 | 15.5538 | Supported |
| PI - > INT | 0.1216 | 1.2845 | Not Supported |
| PU - > INT | 0.2095 | 4.0398 | Supported |
| SN - > INT | 0.2207 | 2.2041 | Supported |
The moderating effect of gender
This study found a significant moderating effect of gender on mHealth adoption. Data from the table illustrates the information that male have a higher level of mHealth adoption intention than females in terms of PEU (0.6556 versus 0.1445, t = 3.784), PI (0.6058 versus 0.0749, t = 3.334), and SN (0.8584 versus -0.3763, t = 9.512). Thus, our Hypotheses 7–9 were all supported, and we can conclude that male find it easy to adopt mHealth. But, the aspect of PU (0.3244 versus 0.0140, t = 2.104), female have a higher level of mHealth adoption intention than males (Table 7).
Table 7.
Moderating effect of gender
| Male | Female | Comparison | |||
|---|---|---|---|---|---|
| Path | β | t-statistics | β | t-statistics | t-statistics |
| PEU - > INT | 0.6556 | 5.8639 | 0.1445 | 1.6618 | 3.784 |
| PI- > INT | 0.6058 | 5.4781 | 0.0749 | 0.7133 | 3.334 |
| PU - > INT | 0.0140 | 0.5374 | 0.3244 | 2.6782 | 2.104 |
| SN - > INT | 0.8584 | 9.8919 | −0.3763 | 4.2134 | 9.512 |
Discussion
This study extended TAM model and supported it using empirical data in the context of mHealth adoption in Bangladesh. Regarding TAM related variables, the result shows that both PEU and PU had significant influence on intention to use mHealth. This finding is consistent with the existing literature on the topic that adoption of a system such as mHealth is dependent on usefulness of the systems and how easy it is to use it [81]. Teo et al. [82] also demonstrated that PU and PEU to be significant determinant of behavioural intention to use technology. This study also infers that intention to use found to be a stronger predictor of actual use of mHealth.
In addition to the TAM variables, our results show the strong positive relationship between subjective norm and intention to use mHealth in Bangladesh. Many previous researchers theorize that subjective norm has a significant effect on intention to use a system [83]. We can conclude that opinions from family members and friends affect the decision to adopt mHealth because it is relatively new applications in Bangladesh. We suggest that Telecom Company and healthcare provider can invest money and effort for promotional activities on virtual communities.
However, the results of this current study indicate that Personal innovativeness in IT has less significant effect on mHealth adoption. This finding is surprising because many previous studies confirm the relationship between Personal innovativeness in IT and technology adoption [84]. Our finding could be reflective on the fact that more innovative people do not necessarily have more intention to use technology. Another possible explanation is that that younger people in Bangladesh are not concerned about mHealth apps, although they are the user of different mobile apps. Therefore the Personal innovativeness in IT does not play a significant role in the mHealth adoption in the context of Bangladesh. Further study is needed to advance our understanding of Personal innovativeness in IT.
This study found the moderating effect of gender differences. In our study men and women were responded differently in their concern about PU, PEU, subjective norm and Personal innovativeness in IT of mHealth adoption. Venkatesh and Morris [85] indicated that compared to female, male's technology adoption decisions were more strongly influenced by their perceptions of usefulness. In contrast, female were more strongly influenced by perceptions of subjective norm and ease of use. According to the technology adoption research, male and female react differently due to their differences toward technology adoption [69].
Study limitations, future directions and conclusion
There are some limitations in this study. First, we surveyed only Dhaka City, urban areas in Bangladesh which may raise concern about the generalizability of the findings. Future research should give more attention to rural areas in Bangladesh. Future research should give more attention to rural areas in Bangladesh. Second, we surveyed only younger citizens in Bangladesh. The paper does not engage with the factors that influence the adoption of mHealth. Future research could investigate the mHealth adoption among other age group such as elderly. Finally, this study used convenience sampling method as survey instrument which may not be the representative of the entire population and results may be biased.
Although, there are some limitations, this study is the milestones and future scope for researchers in developing countries to understand the factors that influence the adoption of mHealth. This study extended TAM model to understand the factors affecting mHealth adoption in developing countries. Our findings showed that extended TAM is a valid model to understand the adoption of mHealth in developing countries. Identified factors in this study can provide necessary assistants to the development and adoption of mHealth. Successful adoption of mHealth depends on the engagement of patient, telecom industry, healthcare organization, app developer, researcher and other stakeholders. App developer and designers should design mHealth that are easy to use. Healthcare organization and telecom industry can provide adequate training and support during implementation and use of mHealth. Government should provide a facilitating environment where citizens are encouraged to use new technologies such as mHealth.
Ethics approval and consent to participate
Prior to commencing the research, ethical approval was sought and obtained from the Center for Modern Information Management, School of Management, Huazhong University of Science and Technology, Wuhan, China. The author also contacted with the chairman of MIS department at University of Dhaka to seek permission to collect data from students. All participants in the research were given consent forms and information sheets which clearly explained the purpose of the study. Respondents were also made aware of their rights to withdraw participation at any time during the study. Moreover, this study did not include any minors or vulnerable adults and therefore, no major or special ethical issues were involved in this study. The questionnaire also provided respondents with information on how to lodge a complaint with Ethics committee should they feel a need to do so. Respondents were also made aware of the fact that they may request the findings of the research once it is completed.
Consent for publication
Not applicable.
Availability of data and material
The specific data used in this study is available upon request from the authors.
Acknowledgements
The author acknowledges the constructive comments from the Associate Editor and two reviewers, which helped improve the quality of this manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Abbreviations
- ACT
Actual Use
- AVE
Average Variance Extracted
- CR
Composite Reliability
- IDT
Innovation Diffusion Theory
- INT
Intention to Use
- PEU
Perceived Ease of Use
- PIIT
Personal Innovativeness in IT
- PLS
Partial Least Squares
- PU
Perceived Usefulness
- SEM
Structural Equation Model
- SN
Subjective Norm
- TAM
Technology Acceptance Model
- TIA
Theory of Innovation Adoption
- TPB
Theory of Planned Behavior
- TRA
Theory of Reasoned Action
- WHO
World Health Organization
Footnotes
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
Md. RH contributed to the conceptualization and design of the study, the collection and analysis of the required information, and the drafting of the original and final versions of the manuscript.
References
- 1.WHO . M-Health: new horizons for health through mobile technologies. Geneva: World Health Organization; 2011. [Google Scholar]
- 2.UN . mHealth for development: the opportunity of mobile technology for healthcare in developing world. 2009. [Google Scholar]
- 3.Ramanathan N, Swendeman D, Comulada WS, Estrin D, Rotheram-Borus MJ. Identifying preferences for mobilehealth applications for self-monitoring andself-management: focus group findings from HIV-positive persons and young mothers. Int J Med Inform. 2013;82(4):e38–e46. doi: 10.1016/j.ijmedinf.2012.05.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Akter S, Ray P. mHealth―An Ultimate Platform to Serve the Unserved. IMIA Yearkbook of Medical Informatics. Schattauer, Germany: Yearb Med Inform; 2010. p. 94–100. [PubMed]
- 5.ITU . The world in 2013: ICT facts and figures. ICT data and statistics division. Geneva: Telecommunication Development Bureau, International Telecommunication Union; 2013. [Google Scholar]
- 6.WHO . New horizons for health through mobile technologies. Geneva: World Health Organization; 2011. p. 112. [Google Scholar]
- 7.BTRC . Mobilet Subscribers in Bangladesh, Bangladesh Telecommunication Regulatory Commission Report. 2014. [Google Scholar]
- 8.NIPORT, Mitra and Associates, and ICF International . Bangladesh demographic and health survey 2011. Dhaka and Calverton MA: National Institute of Population Research and Training, Mitra and Associates, and ICF International; 2013. [Google Scholar]
- 9.NIPORT, Mitra and Associates, and Macro International . Bangladesh demographic and health survey 2007. Dhaka and Calverton MA: National Institute of Population Research and Training, Mitra and Associates, and Macro International; 2009. [Google Scholar]
- 10.MHFW . Health Bulletin 2008. Ministry of Health and Family Welfare, Dhaka: Government of the People’s Republic of Bangladesh, Management Information System (MIS), Directorate General of Health Services (DGHS); 2008. [Google Scholar]
- 11.Deng Z, Mo X, Liu S. Comparison of the middle-aged and older users’ adoption of mobile health services in China. Int J Med Inform. 2014;83(3):210–224. doi: 10.1016/j.ijmedinf.2013.12.002. [DOI] [PubMed] [Google Scholar]
- 12.Ghorai K, Akter S, Khatun F, Ray P. mHealth for smoking cessation programs: a systematic review. J Personalized Med. 2014;4(3):412–423. doi: 10.3390/jpm4030412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ghorai K, Jahan S, Ray P, Chylinski M. mHealth for behaviour change: role of a smartphone–based multi–intervention service for hypertension and diabetes in Bangladesh. Int J Biomed Eng Technol. 2014;16(2):135–155. doi: 10.1504/IJBET.2014.065655. [DOI] [Google Scholar]
- 14.Ghorai K, Jahan S, Ray P, Chylinski M. Mobile phone including smart phone based persuasive system design for controlling hypertension and diabetes in Bangladesh. In: 24th Australasian Conference on Information Systems (ACIS). Australia: RMIT University; 2013. p. 1-11.
- 15.Kumar S, Nilsen WJ, Abernethy A, Atienza A, Patrick K, Pavel M, et al. Mobile health technology evaluation: the mHealth evidence workshop. Am J Prev Med. 2013;45(2):228–36. [DOI] [PMC free article] [PubMed]
- 16.Cole-Lewis H, Kershaw T. Text messaging as a tool for behavior change in disease prevention and management. Epidemiol Rev. 2010;32(1):56–69. doi: 10.1093/epirev/mxq004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Free C, Knight R, Robertson S, Whittaker R, Edwards P, Zhou W, et al. Smoking cessation support delivered via mobile phone text messaging (txt2stop): a single-blind, randomised trial. Lancet. 2011;378(9785):49–55. [DOI] [PMC free article] [PubMed]
- 18.Brendryen H, Kraft P. Happy Ending: a randomized controlled trial of a digital multi‐media smoking cessation intervention. Addiction. 2008;103(3):478–484. doi: 10.1111/j.1360-0443.2007.02119.x. [DOI] [PubMed] [Google Scholar]
- 19.Rogers EM. Diffusion of innovations. 4. New York: Free Press; 1995. [Google Scholar]
- 20.GSMA . Women & mobile: a global opportunity. A study on the mobile phone gender gap in low and middle-income countries. London: GSMA; 2010. [Google Scholar]
- 21.Cho H, Kim Y, Kim J. An acceptance model for an internet protocol television service in Korea with prior experience as a moderator. Serv Ind J. 2010;30(11):1883–1901. doi: 10.1080/02642060802627178. [DOI] [Google Scholar]
- 22.Davis FD. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS quarterly. 1989; 319–40.
- 23.Mun YY, Hwang Y. Predicting the use of web-based information systems: self-efficacy, enjoyment, learning goal orientation, and the technology acceptance model. Int J Hum Comput Stud. 2003;59(4):431–449. doi: 10.1016/S1071-5819(03)00114-9. [DOI] [Google Scholar]
- 24.Lu J, Yao JE, Yu CS. Personal innovativeness, social influences and adoption of wireless Internet services via mobile technology. J Strateg Inf Syst. 2005;14(3):245–268. doi: 10.1016/j.jsis.2005.07.003. [DOI] [Google Scholar]
- 25.Gefen D, Straub DW. Gender Differences in the Perception and Use of E-Mail: An Extension to the Technology Acceptance Model. MIS Quarterly. 1997;21(4):389–400.
- 26.Adams DA, Nelson RR, Todd PA. Perceived usefulness, ease of use, and usage of information technology: a replication. MIS Quarterly. 1992; 227-247.
- 27.Dünnebeil S, Sunyaev A, Blohm I, Leimeister JM, Krcmar H. Determinants of physicians’ technology acceptance for e-health in ambulatory care. Int J Med Inform. 2012;81(11):746–760. doi: 10.1016/j.ijmedinf.2012.02.002. [DOI] [PubMed] [Google Scholar]
- 28.Melas CD, Zampetakis LA, Dimopoulou A, Moustakis V. Modeling the acceptance of clinical information systems among hospital medical staff: An extended TAM model. J Biomed Inform. 2011;44(4):553–564. doi: 10.1016/j.jbi.2011.01.009. [DOI] [PubMed] [Google Scholar]
- 29.Xue L, Yen CC, Chang L, Chan HC, Tai BC, Tan SB, et al. An exploratory study of ageing women’s perception on access to health informatics via a mobile phone-based intervention. Int J Med Inform. 2012;81(9):637–48. [DOI] [PubMed]
- 30.Lim S, Xue L, Yen CC, Chang L, Chan HC, Tai BC, et al. A study on Singaporean women’s acceptance of using mobile phones to seek health information. Int J Med Inform. 2011;80(12):189–202. [DOI] [PubMed]
- 31.Davis FD, Bagozzi RP, Warshaw PR. User acceptance of computer technology: a comparison of two theoretical models. Manage Sci. 1989;35(8):982–1003.
- 32.Reid M, Levy Y. Integrating trust and computer self-efficacy with TAM: an empirical assessment of customers’ acceptance of banking information systems (BIS) in Jamaica. J Internet Bank Commerce. 2008;12(3):1–17.
- 33.Sulaiman A, Ng J, Mohezar S. E-ticketing as a new way of buying tickets: Malaysian perceptions. J Soc Sci. 2008;17(2):149–157. [Google Scholar]
- 34.Arning K, Ziefle M. Understanding age differences in PDA acceptance and performance. Comput Hum Behav. 2007;23(6):2904–2927. doi: 10.1016/j.chb.2006.06.005. [DOI] [Google Scholar]
- 35.Pituch KA, Lee YK. The influence of system characteristics on e-learning use. Comput Educ. 2006;47(2):222–244. doi: 10.1016/j.compedu.2004.10.007. [DOI] [Google Scholar]
- 36.Bao Y, Xiong T, Hu Z, Kibelloh M. Exploring gender differences on general and specific computer self-efficacy in mobile learning adoption. J Educ Comput Res. 2013;49(1):111–132. doi: 10.2190/EC.49.1.e. [DOI] [Google Scholar]
- 37.Ye Q, Law R, Gu B, Chen W. The influence of user-generated content on traveler behavior: an empirical investigation on the effects of e-word-of-mouth to hotel online bookings. Comput Hum Behav. 2011;27(2):634–639. doi: 10.1016/j.chb.2010.04.014. [DOI] [Google Scholar]
- 38.Nysveen H, Pedersen PE, Thorbjørnsen H. Intentions to use mobile services: antecedents and cross-service comparisons. J Acad Mark Sci. 2005;33(3):330–346. doi: 10.1177/0092070305276149. [DOI] [Google Scholar]
- 39.Kleijnen M, Wetzels M, Ruyter KD. Consumer acceptance of wireless finance. J Financ Serv Mark. 2004;8(3):206–217. doi: 10.1057/palgrave.fsm.4770120. [DOI] [Google Scholar]
- 40.Wang YS, Lin HH, Luarn P. Predicting consumer intention to use mobile service. Inf Syst J. 2006;16(2):157–179. doi: 10.1111/j.1365-2575.2006.00213.x. [DOI] [Google Scholar]
- 41.Zhang X, Guo X, Lai KH, Guo F, Li C. Understanding gender differences in m-Health adoption: a modified theory of reasoned action model. Telemed e-Health. 2014;20(1):39–46. doi: 10.1089/tmj.2013.0092. [DOI] [PubMed] [Google Scholar]
- 42.Angst CM, Agarwal R. Adoption of electronic health records in the presence of privacy concerns: the elaboration likelihood model and individual persuasion. MIS Q. 2009;33(2):339–370. [Google Scholar]
- 43.Luarn P, Lin HH. Toward an understanding of the behavioral intention to use mobile banking. Comput Hum Behav. 2005;21(6):873–891. doi: 10.1016/j.chb.2004.03.003. [DOI] [Google Scholar]
- 44.Wangpipatwong S, Chutimaskul W, Papasratorn B. Understanding citizen’s continuance intention to use e-government website: a composite view of technology acceptance model and computer self-efficacy. Electron J e-govern. 2008;6(1):55–64. [Google Scholar]
- 45.Guriting P, Oly Ndubisi N. Borneo online banking: evaluating customer perceptions and behavioural intention. Management Res News. 2006;29(1/2):6–15. doi: 10.1108/01409170610645402. [DOI] [Google Scholar]
- 46.Venkatesh V, Morris MG, Davis GB, Davis FD. User acceptance of information technology: toward a unified view. MIS Q. 2003;27(3):425–478. [Google Scholar]
- 47.Karahanna E, Straub DW, Chervany NL. Information technology adoption across time: a cross-sectional comparison of pre-adoption and post-adoption beliefs. MIS Q. 1999;23(2).
- 48.Bhattacherjee A. Acceptance of ecommerce services: the case of electronic brokerages. IEEE Transact System Man Cybernetics Part A. 2000;20(4):411–20. doi: 10.1109/3468.852435. [DOI] [Google Scholar]
- 49.Liao C, Chen J-L, Yen D. Theory of planning behavior (TPB) and customer satisfaction in the continued use of e-service: an integrated model. Comput Hum Behav. 2007;23(6):2804–22. doi: 10.1016/j.chb.2006.05.006. [DOI] [Google Scholar]
- 50.Özkan S, Bindusara G, Hackney R. Facilitating the adoption of e-payment systems: theoretical constructs and empirical analysis. J Enterp Inf Manag. 2010;23(3):305–325. doi: 10.1108/17410391011036085. [DOI] [Google Scholar]
- 51.Gu JC, Lee SC, Suh YH. Determinants of behavioral intention to mobile banking. Expert Syst Appli. 2009;36(9):11605–11616. doi: 10.1016/j.eswa.2009.03.024. [DOI] [Google Scholar]
- 52.Chan S, Lu M. Understanding internet banking adoption and use behavior: a Hong Kong perspective”. J Glob Inf Manag. 2004;12:21–43. doi: 10.4018/jgim.2004070102. [DOI] [Google Scholar]
- 53.Glass R, Li S. Social influence and instant messaging adoption. J Comput Inform Syst. 2010;51(2):24. [Google Scholar]
- 54.Wu IL, Li JY, Fu CY. The adoption of mobile health care by hospital’s professionals: an integrative perspective. Decis Support Syst. 2011;51(2):587–596. doi: 10.1016/j.dss.2011.03.003. [DOI] [Google Scholar]
- 55.Rogers EM. Lessons for guidelines from the diffusion of innovations. Joint Comm J Qual Improv. 1995;21(7):324. [DOI] [PubMed]
- 56.Agarwal R, Prasad J. A conceptual and operational definition of personal innovativeness in the domain of information technology. Inf Syst Res. 1998;9(2):204–215. doi: 10.1287/isre.9.2.204. [DOI] [Google Scholar]
- 57.Thatcher JB, Loughry ML, Lim J, McKnight DH. Internet anxiety: an empirical study of the effects of personality, beliefs, and social support. Inform Manage. 2007;44(4):353–363. doi: 10.1016/j.im.2006.11.007. [DOI] [Google Scholar]
- 58.Taylor NJ. Public grid computing participation: an exploratory study of determinants. Inform Manage. 2007;44(1):12–21. doi: 10.1016/j.im.2006.05.004. [DOI] [Google Scholar]
- 59.Mun YY, Jackson JD, Park JS, Probst JC. Understanding information technology acceptance by individual professionals: toward an integrative view. Information & Management. 2006;43(3):350–363. doi: 10.1016/j.im.2005.08.006. [DOI] [Google Scholar]
- 60.Thong JY. An integrated model of information systems adoption in small businesses. J Manag Inf Syst. 1999;15(4):187–214. doi: 10.1080/07421222.1999.11518227. [DOI] [Google Scholar]
- 61.Verkasalo H, López-Nicolás C, Molina-Castillo FJ, Bouwman H. Analysis of users and non-users of smartphone applications. Telematics Inform. 2010;27(3):242–255. doi: 10.1016/j.tele.2009.11.001. [DOI] [Google Scholar]
- 62.Turner M, Kitchenham B, Brereton P, Charters S, Budgen D. Does the technology acceptance model predict actual use? A systematic literature review. Inf Softw Technol. 2010;52(5):463–479. doi: 10.1016/j.infsof.2009.11.005. [DOI] [Google Scholar]
- 63.Legris P, Ingham J, Collerette P. Why do people use information technology? A critical review of the technology acceptance model. Information & management. 2003;40(3):191–204. doi: 10.1016/S0378-7206(01)00143-4. [DOI] [Google Scholar]
- 64.Horton RP, Buck T, Waterson PE, Clegg CW. Explaining intranet use with the technology acceptance model. J Inf Technol. 2001;16(4):237–249. doi: 10.1080/02683960110102407. [DOI] [Google Scholar]
- 65.Szajna B. Empirical evaluation of the revised technology acceptance model. Manag Sci. 1996;42(1):85–92. doi: 10.1287/mnsc.42.1.85. [DOI] [Google Scholar]
- 66.Whitley BE. Gender differences in computer-related attitudes and behavior: a meta-analysis. Comput Hum Behav. 1997;13(1):1–22. doi: 10.1016/S0747-5632(96)00026-X. [DOI] [Google Scholar]
- 67.Wang YS, Wu MC, Wang HY. Investigating the determinants and age and gender differences in the acceptance of mobile learning. Br J Educ Technol. 2009;40(1):92–118. doi: 10.1111/j.1467-8535.2007.00809.x. [DOI] [Google Scholar]
- 68.Van Slyke C, Comunale CL, Belanger F. Gender differences in perceptions of web-based shopping. Commun ACM. 2002;45(8):82–86. doi: 10.1145/545151.545155. [DOI] [Google Scholar]
- 69.Ong CS, Lai JY. Gender differences in perceptions and relationships among dominants of e-learning acceptance. Comput Hum Behav. 2006;22(5):816–829. doi: 10.1016/j.chb.2004.03.006. [DOI] [Google Scholar]
- 70.Ritchie J, Lewis J, Elam, G. Designing and selecting samples. Qualitative research practice: a guide for social science students and researchers. 2003; p.77–108.
- 71.Eze UC, Goh MH, Ling HY, Lee CH. Informatics engineering and information science. Berlin Heidelberg: Springer; 2011. Intention to use e-government services in Malaysia: Perspective of individual users; pp. 512–526. [Google Scholar]
- 72.Chau PY, Hu PJH. Investigating healthcare professionals’ decisions to accept telemedicine technology: an empirical test of competing theories. Information & management. 2002;39(4):297–311. doi: 10.1016/S0378-7206(01)00098-2. [DOI] [Google Scholar]
- 73.Wu I, Chen J. An extension of trust and TAM model with TPB in the initial adoption of on-line tax: an empirical study”. Int J Hum Comput Stud. 2005;62:784–808. doi: 10.1016/j.ijhcs.2005.03.003. [DOI] [Google Scholar]
- 74.Yi MY, Jackson JD, Park JS, Probst JC. Understanding information technology acceptance by individual professionals: toward an integrative view. Information & Management. 2006;43(3):350–363. doi: 10.1016/j.im.2005.08.006. [DOI] [Google Scholar]
- 75.Taylor S, Todd P. Assessing IT usage: the role of prior experience. MIS quarterly. 1995; 561-570.
- 76.Davis FD, Venkatesh V. Toward preprototype user acceptance testing of new information systems: implications for software project management. Eng Manage IEEE Trans. 2004;51(1):31–46. doi: 10.1109/TEM.2003.822468. [DOI] [Google Scholar]
- 77.Cohen J, Cohen P, West S G, Aiken L S Applied multiple regression/correlation analysis for the behavioral sciences. Australia: Routledge; 2013.
- 78.Bagozzi RP, Yi Y, Phillips LW. Assessing construct validity in organizational research. Adm Sci Q. 1991; 421-458.
- 79.Hair JF, Jr, Anderson RE, Tatham RL, William C. Multivariate data analysis with readings. New Jersy: Prentice Hall; 1995. [Google Scholar]
- 80.Henseler J, Ringle CM, Sinkovics RR. The use of partial least squares path modeling in international marketing. Adv Int Mark. 2009;20(1):277–319. [Google Scholar]
- 81.Manda TD, Msosa Y. e-Infrastructure and e-Services for Developing Countries. Berlin Heidelberg: Springer; 2012. Socio-technical Arrangements for mHealth: Extending the Mobile Device Use and Adoption Framework; pp. 208–217. [Google Scholar]
- 82.Teo T, Luan WS, Sing CC. A cross-cultural examination of the intention to use technology between Singaporean and Malaysian pre-service teachers: an application of the Technology Acceptance Model (TAM) J Educ Tech Soc. 2008;11(4):265–280. [Google Scholar]
- 83.Schepers J, Wetzels M. A meta-analysis of the technology acceptance model: Investigating subjective norm and moderation effects. Information & Management. 2007;44(1):90–103. doi: 10.1016/j.im.2006.10.007. [DOI] [Google Scholar]
- 84.Yang S, Lu Y, Gupta S, Cao Y, Zhang R. Mobile payment services adoption across time: an empirical study of the effects of behavioral beliefs, social influences, and personal traits. Comput Hum Behav. 2012;28(1):129–42.
- 85.Venkatesh V, Morris M. G. Why don't men ever stop to ask for directions? Gender, social influence, and their role in technology acceptance and usage behavior. MIS quarterly. 2000; 115–139.