

Abstract
Objectives
To determine risk factors for revision in patients implanted with a commonly used metal on metal (MoM) hip replacement.
Design
Retrospective cohort study in combination with a prospective national retrieval study (Northern Retrieval Registry (NRR)).
Setting
Combined orthopaedic unit in combination with the NRR.
Participants
All patients implanted with a DePuy Pinnacle MoM hip prostheses by the 2 senior authors were invited to attend for a review which included clinical examination, blood metal ion measurements, radiographs and targeted imaging. Explanted components underwent wear analysis using validated methodology and these results were compared with those obtained from the NRR.
Results
489 MoM Pinnacle hips were implanted into 434 patients (243 females and 191 males). Of these, 352 patients attended the MoM recall clinics. 64 patients had died during the study period. For the purposes of survival analysis, non-attendees were assumed to have well-functioning prostheses. The mean follow-up of the cohort as a whole was 89 months. 71 hips were revised. Prosthetic survival for the whole cohort was 83.6% (79.9–87.3) at 9 years. The majority of explanted devices exhibited signs of taper junction failure. Risk factors for revision were bilateral MoM prostheses, smaller Pinnacle liners, and implantation in 2006 and later years. A significant number of devices were found to be manufactured out of their specifications. This was confirmed with analysis of the wider data set from the NRR.
Conclusions
This device was found to have an unacceptably high revision rate. Bilateral prostheses, those implanted into female patients and devices implanted in later years were found to be at greater risk. A significant number of explanted components were found to be manufactured with bearing diameters outside of the manufacturer's stated tolerances. Our findings highlight the clinical importance of hitherto unrecognised variations in device production.
Strengths and limitations of this study.
This is the first study to combine the results of a patient cohort with those obtained from a retrieval registry in order to better understand the performance of a device.
Previous studies of this device have reported results from centres with several surgeons and have not examined the impact of liner size on prosthetic survival nor considered variations in manufacturing processes.
The patient cohort was followed up retrospectively, with 30 patients lost to follow-up.
Background
There is general acceptance that large diameter metal on metal (MoM) total hip arthroplasty (THA) has not lived up to clinical expectations. Although the use of MoM hip devices has declined dramatically in the past 5 years,1–4 hundreds of thousands remain in situ,5 with the long-term future uncertain. Greater understanding of the mechanisms of prosthetic failure would enable management strategies to be developed in accordance with local resources as well as helping to avoid potential problems with future designs.
Failures of MoM hip arthroplasty have been attributed to:
Device factors (design): Previous publications have shown that the DePuy (Warsaw, Indiana, USA) ASR Hip System (which employs a similar taper connection to the DePuy Pinnacle system with respect to the metallurgy and morphology) failed because of: a shallow acetabular component (low coverage arc) predisposing to edge wear;11 metal debris release from the head neck taper junction (figure 1);12 and the same low diametrical clearance technology leading to an increased propensity to edge wear13 and cup loosening.14 Diametrical clearance is described in figure 2.
Figure 1.
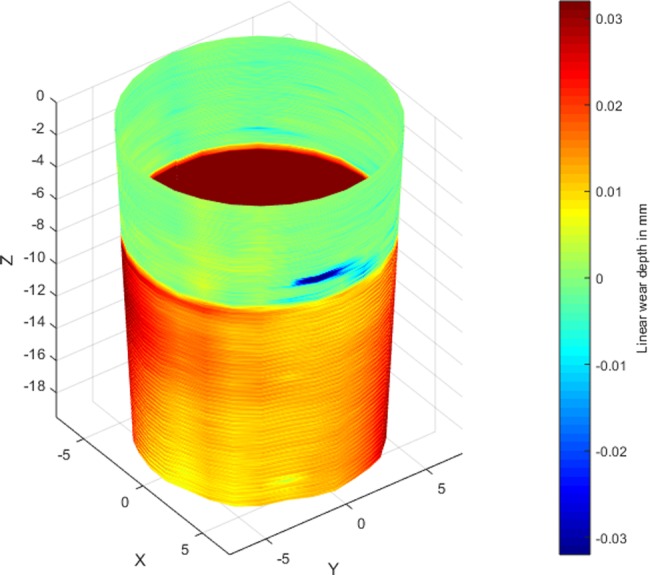
Coordinate measuring machine (CMM) generated wear map of a typical failed taper with a deep asymmetrical groove of wear corresponding to the base of the stem taper. In this case, the Corail stem has imprinted its ridged form onto the female taper surface.
Figure 2.
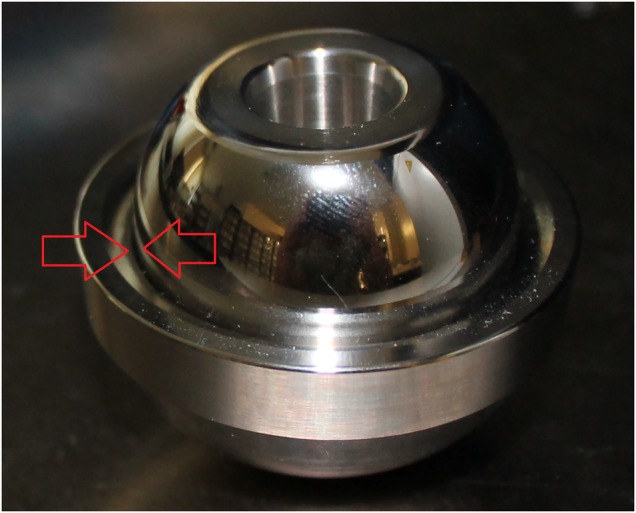
A Pinnacle head and liner. The red arrows indicate the small gap between the head and the liner surface which is the ‘clearance’. Diametrical clearance is calculated by subtracting the diameter of the head from the diameter of the liner.
Device factors (manufacturing): The Northern Retrieval Registry (NRR), directed by one of the authors, analyses explanted devices from several major hospitals in the UK on a routine basis. During this analysis, it was found that a number of Pinnacle devices were manufactured with lower diametrical clearances than was intended by the manufacturer. The rate of non-conformance appeared to increase over time, with Pinnacles manufactured from the year 2006 onwards significantly more likely to have a clearance value lower than stated to regulators.8 These results are described in figure 3 and in greater detail in online supplementary appendix 2.
Figure 3.
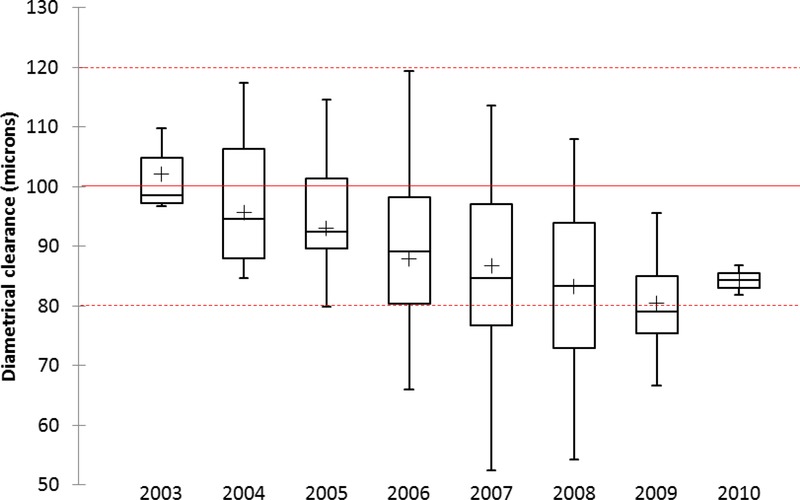
The diametrical clearances of all mated (head and cup combinations) used in Pinnacle MoM hips received at the Northern Retrieval Registry (NRR) to present date. The red unbroken line represents the nominal target clearance with the outer broken red lines indicating the upper and lower tolerance bands. Five out of the 43 (12%) hips implanted prior to 2006 were found to be below the lower tolerance band compared with 43 out of 118 (36%) implanted from 2006 onwards.
bmjopen-2015-007847supp_appendix2.pdf (1.3MB, pdf)
Surgical factors: Cup orientation has been shown to affect wear rates/metal ion release in MoM arthroplasty11 and devices with lower coverage arcs and sharper articular rims are particularly sensitive to cup position.7 16
Host factors: Our previous investigations and clinical experience have shown that: adverse reaction to metal debris (ARMD) is more common in devices with abnormal wear;17 however, soft tissue damage is more strongly related to lymphocyte-dominated reactions than wear rates;18 women appear to more readily mount a negative immune cascade than men when exposed to equivalent loads of debris;19 debris from a failing taper junction appears to be associated with a more intense inflammatory response than an equivalent dose from the bearing surface.20 In our own experience, devices with no excessive wear with associated ARMD are commonly found in patients with bilateral devices implying a process of sensitisation.21
The aim of this study was to identify variables associated with early failure of the Pinnacle 36 mm MoM system by a retrospective analysis of all patients implanted with this device by two experienced hip surgeons at our institution. After consideration of the above factors we hypothesised:
Overall failure rates would be higher in female patients, those who received bilateral prostheses and in Pinnacles implanted from 2006 onwards.
Failures related to excessive bearing surface wear would be commonest in patients implanted with the smallest sized Pinnacle shells (ie, thinnest liners).
Failures related to taper failure would be more common than those related to excessive bearing wear.
Failures related to taper malfunction would be more commonly found in patients with Corail stems due to the negative effect of a short, ridged male taper.22 23
The Pinnacle system would be relatively resistant to the effects of cup position in terms of blood metal ion release due to its smoother rim and greater arc of cover conferring protection from edge wear.11 16 By extension, ARMD would, in general, be unrelated to cup position.
Patients, implants and methods
Patients implanted with a Pinnacle MoM hip prosthesis in our group of hospitals were identified using all available records including National Joint Registry (NJR) reports, operating theatre lists and DePuy sales records. From this total group of patients, all those with a 36 mm MoM Pinnacle hip which had been used in conjunction with an SROM or Corail uncemented stem were identified. From this subgroup, only those whose components had been implanted by either of the two senior authors of this paper (RL and AVFN) were included in this study (figure 4). RL and AVFN are both specialist consultant lower limb arthroplasty surgeons. The use of the SROM stem was dependant on two factors—time and complexity of surgery. Prior to 2006, patients under 70 who were not suitable for resurfacing or patients of any age where there were concerns over anatomy (developmental dysplasia/Perthes’/SUFE/narrow femoral neck) were considered for a MoM total hip replacement (THR) using an SROM. The SROM has a modular junction which allows the surgeon to rotate the neck in order to compensate for variations in existing anatomy. From 2005 onwards, the Corail was increasingly used, with the SROM reserved for the more complex cases. Operations were performed from 2003 to 2009 at two National Health Service (NHS) hospitals and one private unit. All bilateral replacements were performed sequentially. Patients were followed up annually in the NHS. At the private unit, most patients were discharged after 1 year. From 2007 to 2011, as our awareness of ARMD began to increase,17 patients attending clinic who had developed symptoms were offered blood metal ion testing and ultrasound scanning if deemed necessary. From 2011 onwards, following general acceptance of widespread problems with MoM,2 a full recall of Pinnacle MoM patients was performed, which entailed Harris Hip Score evaluation, radiographs when necessary and routine testing of serum and whole blood chromium (Cr) and cobalt (Co) measurements using high resolution inductively coupled plasma mass spectrometry (ICPMS). Einzel-Bild-Roentgen-Analyse (EBRA) analysis of standing radiographs was performed as previously described.4
Figure 4.

A flow chart to illustrate the participants involved in the various survival analyses. NHS, National Health Service.
A general protocol was put in place based on our clinical experience. This is described in figure 5. Ultrasound scans were performed by one senior musculoskeletal radiologist with extensive experience in the diagnosis of ARMD. Revision findings were recorded according to a gross scoring system we have previously used.18 Likewise, histological findings were documented using previously published methods.24
Figure 5.

A flow chart to illustrate the investigation pathways for the participants in the study.
The Pinnacle MoM THR system
The Pinnacle shell is a porous coated titanium (Ti) alloy shell which accommodates the Ultamet metal liner which is available in varying thicknesses. The size of the implanted Pinnacle shell is largely dictated by the patient's anatomy. In this study, all patients received a standardised liner with a 36 mm internal bearing surface. As shells become larger, because the mating liner is a standardised size, by necessity the wall of the liner must become thicker in order to press fit into the larger diameter shell (figure 6). The liner and femoral head are wrought high carbon content alloys. The clearance for this bearing surface is stated as 100 µm±20 µm. The 160° subhemispherical bearing surface does not vary with the thickness of the liner. The femoral head is manufactured in two forms: The 11/13 for use with the SROM stem (the Ultamet) and the 12/14 head which can be used with the Corail stem (the Articuleze). Both stems are uncemented stems and from the same Ti alloy. The 11/13 head has a taper angle range of approximately 5.95–6.01°. The equivalent range for the 12/14 head is 5.57–5.72°.
Figure 6.

The relationship between liner thickness and shell size. On the left, the relatively thick liner of a 60 mm prosthesis is seen in comparison with a 52 mm liner. The head in both cases is the standard 36 mm diameter component. As can be seen on the right, liner walls become progressively thicker as the liner size increases.
Explant analysis
Explanted Pinnacle femoral head, head tapers and acetabular liners underwent dimensional and volumetric wear analysis using previously described methodology. This was conducted by one of the authors (DJL) at Newcastle University and North Tees Explant Centre. The accuracy of these techniques has been discussed in detail in previous publications.25 The retrieved explants were designated as exhibiting: ‘bearing failure’ if the combined mean volumetric wear rate of the head and cup was measured as ≥2 mm3 per year26 and the maximum wear depths were measured at the edge of the cup (edge wear); ‘taper failure’ if material loss from the female taper surface was ≥0.5 mm3 and the pattern of material loss showed hallmark asymmetric distribution with an obvious circumferential trough of wear (figure 1)27; ‘mixed failure’ if both of the above characteristics were present; or ‘no abnormal wear’.
The explant results presented in the main body of this paper represent only those derived from the failed prostheses of the patient group in this study. The results presented in figure 2 and supplementary appendix 2 are generated from the pool of Pinnacle MoM devices received at the NRR.
Survival analysis
Joints were censored as ‘failed’ if they had been revised or the patient had been listed for revision surgery at the time of writing. Deceased patients were assumed to have a well-functioning joint at the time of death. Patients who were lost to follow-up were also assumed to have well-functioning prostheses. Joint survival analysis of the cohort as a whole was conducted initially to determine the predicted 9-year survival of the male and female cohorts using Kaplan-Meier analysis. Differences in survival between groups were assessed for significance using the log-rank test. Cox proportional hazards modelling was then used to analyse the effect of sex, age, implantation pre-2006 or post-2006, bilaterality, liner size, surgeon and stem type on risk of revision. The model was used initially to determine the risk of early revision for all-cause clinical failure. The model was then repeated to determine the risk of biomechanical failure as determined by the results of the explant analysis, that is, the risk of revision associated with ‘bearing failure’ and risk of revision associated with ‘taper failure’. As liners of size 50 mm were only introduced from 2008 onwards, and as we were investigating the effect of early versus late implantation, there was a concern over data bias. Hazards modelling was therefore conducted using data only of patients who were followed up for at least 6 years or whose joints had failed before 6 years, resulting in the removal of 69 patients for all-cause revision, 82 for revision in association with bearing failure and 90 for revision associated with taper failure (figure 4).
It is hospital policy to consent patients prior to revision surgery for the storage and analysis of all explanted orthopaedic devices.
Results
In total, 489 Pinnacle hips were implanted into 434 patients (243 females and 191 males). Of these, 352 patients attended the MoM recall clinics. Sixty-four patients had died during the study period. For the purposes of survival analysis, non-attendees were assumed to have well-functioning prostheses. The mean follow-up of the cohort as a whole was 89 months (table 1).
Table 1.
Patient demographics
| Corail Pinnacles | SROM Pinnacles | |
|---|---|---|
| Patients | 307 | 127 |
| Joints | 348 | 141 |
| Surgeon 1 vs 2 | 254:94 | 120:21 |
| M:F joints | 140:208 | 67:74 |
| Number with bilateral MoMs | 87 (25%) | 13 (9%) |
| Mean age in years | 67 | 63 |
| Per cent with degenerative osteoarthritis | 86.7 | 80 |
| Median liner size in mm (range) | 52 (50–66) | 54 (50–66) |
| Per cent Xrays and HHS score available | 82.9 | 77.3 |
| Median inclination angle (°) of acetabular component (range) | 43.9 (26.1–61.9) | 45.6 (26.0–65.6) |
| Median anteversion angle of the acetabular component in degrees | 14.4 (0–47.3) | 18.6 (4.6–45.6) |
| Median (range) femoral head offset | 5 (−2 to +12) | 6 (0–9) |
The early (pre-2006) and late implantation cohorts are shown in table 2.
HHS, Harris Hip Score; F, female; M, male; MoM, metal on metal.
All but one of the revisions were carried out for ARMD, with one revision for a loose cup. Prosthetic survival rate for the cohort as a whole was 83.6% (79.9–87.3) at 9 years. In only one case was no abnormal fluid identified at revision. In 53 cases (75%), copious amounts of fluid were found, and in 32 (45%), it was noted to be under pressure or had fistulated through the capsule. Obvious damage to the abductor musculature was noted in 38 cases. Moderate-to-severe aseptic lymphocyte dominated vasculitis associated lesion (ALVAL) was documented on examination of retrieved tissues in 36 cases (51%). In 13 cases (19%), histological findings were solely those of metallosis with no lymphocytic infiltration identified.
Explant analysis
Volumetric wear rates of the bearing and female taper surfaces are listed in table 3. Taper wear was associated with a female taper angle at the larger end of the device's tolerance band and an increased femoral head offset. A multiple regression model using the complete NRR data set (see online supplementary appendix 1) showed, however, that duration in vivo and surface finish of the male and female taper surfaces were the dominant variables associated with taper wear. Online supplementary appendix 1 also provides a detailed analysis of the change in bearing dimensions over time, again derived from the NRR data set.
Table 3.
Details of revision cases
| Total number of joints revised | 71 | ||
| Mean time to failure (months) | 52 (11.5–112) | ||
| Failed | Non-failed | Significance | |
| Males vs females | 16:55 | 191:227 | <0.001 |
| Bilateral vs unilateral | 24:47 | 76:342 | <0.001 |
| Median age | 66 | 68 | 0.052 |
| Median (range) HHS | 66 (23–100) | 91 (28–100) | <0.001 |
| Median liner size male | 55 | 56 | 0.591 |
| Median liner size female | 52 | 52 | 0.146 |
| Median (range) acetabular inclination (°) | 42.8 (32.5–55.9) | 44.6 (26–65.6) | 0.053 |
| Median (range) acetabular anteversion (°) | 13.0 (1.8–34.8) | 16.2 (0–47.3) | 0.005 |
| Median (range) blood Cr unilaterals (µg/L) | 3.62 (0.88–26.2) | 4.580 (0.37–20.3) | <0.001 |
| Median (range) blood Co unilaterals (µg/L) | 3.62 (0.86–19.7) | 1.48 (0.33–12.5) | <0.001 |
| Median (range) blood Cr bilaterals (µg/L) | 9.72 (0.47–26.3) | 6.15 (0.8–18.4) | 0.001 |
| Median (range) blood Co bilaterals (µg/L) | 9.54 (1.42–27.0) | 3.39 (0.33–22.1) | <0.001 |
| Unilaterals | Bilaterals | Significance | |
| Median (range) bearing surface wear rates (mm3 per year) | 1.92 (0.23–8.37) | 0.88 (0.23–7.43) | 0.007 |
| Median (range) combined wear rates (mm3 per year) | 2.19 (0.35–8.43) | 1.57 (0.29–8.13) | 0.038 |
| SROM Pinnacles | Corail Pinnacles | Significance | |
| Median (range) female taper wear rates (mm3 per year) | 0.04 (0–0.50) | 0.21 (0–2.20) | <0.001 |
It can be seen that failed joints were more likely to have cups placed at lower angles of inclination and lower anteversion, though the positions in which they were placed would generally be regarded as acceptable. A full discussion of the implications of this finding is beyond the scope of this paper. It was a result, however, which was in direct contrast to our previous findings with the ASR device.15
HHS, Harris Hip Score.
bmjopen-2015-007847supp_appendix1.pdf (191.6KB, pdf)
Table 2.
Patient demographics of the early versus the late implantation cohort
| Pre-2006 (early cohort) | 2006 onwards (late) | |
|---|---|---|
| Joints | 141 | 348 |
| M:F joints | 74:67 | 133:215 |
| Number bilateral MoMs | 21 (14.9%) | 79 (22.7%) |
| Corail:SROM | 44:97 | 304:44 |
| Mean age in years | 62 | 67 |
| Median liner size in mm (range) | 54 (52–66) | 52 (50–66) |
| Predicted joint survival/survival at 8 years | 94.1% (89.1–98.1) | 81.1% (76.7–85.5) |
At the time of writing, 71 Pinnacles had been revised (table 3).
F, female; M, male; MoM, metal on metal.
Hypothesis 1: Failure rates would be higher in female patients and in those who received bilateral prostheses and in Pinnacles implanted from 2006 onwards.
Female hips, with a predicted survival of 77.9% (72.2–83.6) at 9 years had a significantly higher failure rate than male hips at the same length of follow-up (male survival 91.4% (87.4–95.5); p=0.001; figure 7). However, there were only 31 bilateral male hips compared with 69 bilateral female hips. Pinnacles in patients with bilateral MoM hips had a significantly lower survival rate than in patients with unilateral Pinnacles (73.7% (64.4–82.9) vs 86.2% (82.2–90.2; p<0.001)) at 9 years, respectively (figure 8). Cox proportional hazards model identified only the presence of bilateral joints and the late cohort as significant risk factors for all-cause revision; however, there was a trend towards increasing risk of revision with smaller liner sizes (table 4).
Figure 7.
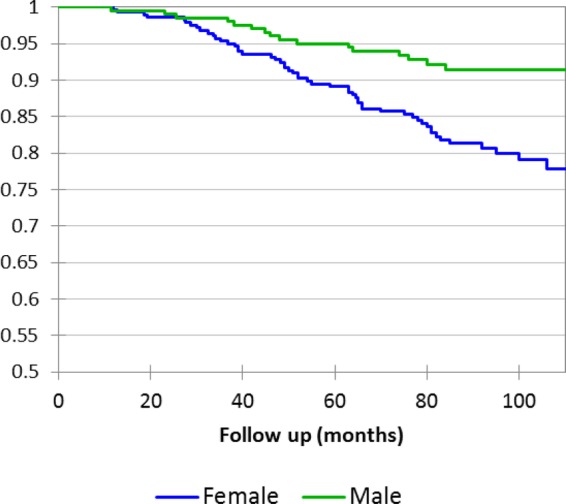
Kaplan–Meier survival curves of male and female hips, all patients included in analysis, all-cause revision.
Figure 8.
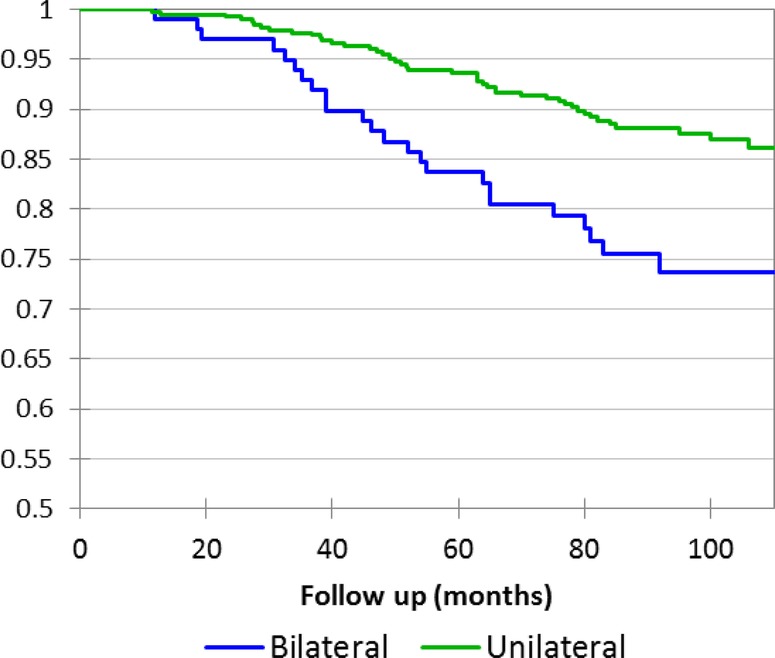
Kaplan–Meier survival curves of unilateral versus bilateral Pinnacle MoM prostheses, all patients included in analysis, all-cause revision.
Table 4.
Cox proportional hazards model results with joints censored initially for all-cause revision, then for ‘bearing failure’ and ‘taper failure’
| HR | Pr > χ2 | Lower 95% CI | Upper 95% CI | |
|---|---|---|---|---|
| Proportional hazards model for all-cause revision (N=489) | ||||
| Bilaterality | 2.408 | <0.001 | 1.478 | 3.925 |
| Liner size | 0.862 | 0.070 | 0.733 | 1.012 |
| Surgeon | 0.966 | 0.950 | 0.559 | 1.669 |
| Age | 0.984 | 0.229 | 0.959 | 1.010 |
| Male sex | 1.619 | 0.167 | 0.818 | 3.205 |
| Corail stem | 1.596 | 0.136 | 0.864 | 2.950 |
| Early cohort | 0.096 | 0.002 | 0.022 | 0.424 |
| Proportional hazards model for revision associated with bearing failure (N=407) | ||||
| Bilaterality | 1.837 | 0.162 | 0.783 | 4.306 |
| Liner size | 0.744 | 0.028 | 0.572 | 0.968 |
| Surgeon | 0.742 | 0.498 | 0.337 | 1.815 |
| Age | 0.980 | 0.130 | 0.959 | 1.005 |
| Male sex | 0.922 | 0.889 | 0.690 | 2.967 |
| SROM stem | 0.901 | 0.866 | 0.266 | 3.045 |
| Early cohort | 0.041 | 0.003 | 0.005 | 0.327 |
| Proportional hazards model for revision associated with taper failure (N=399) | ||||
| Bilaterality | 2.869 | 0.009 | 1.290 | 6.295 |
| Liner size | 0.936 | 0.530 | 0.760 | 1.152 |
| Surgeon | 0.888 | 0.793 | 0.366 | 2.154 |
| Age | 0.980 | 0.980 | 0.940 | 1.023 |
| Male sex | 0.615 | 0.401 | 0.198 | 1.910 |
| SROM stem | 1.523 | 0.45 | 0.505 | 4.593 |
| Early cohort | 0.936 | 0.033 | 0.760 | 1.152 |
Statistically significant variables are shown in bold.
With this analysis repeated using liner sizes as categorical variables, liner sizes 50 and 52 mm were found to be significant risk factors for early revision. To confirm the legitimacy of this model, a log-rank test was performed between bilateral (n=45) and unilateral female (n=86) Corail Pinnacles of the commonest female liner size (52 mm). The survival rate of the bilateral Pinnacles was significantly lower (63.1% (48.6–77.6) vs 84.9% (76.9–92.8) at 8 years (p=0.003)). As sex and liner size were clearly correlated, the impact of liner size versus sex was further investigated by including only patients with unilateral joints with liner sizes 52 and 54 mm (the liner sizes with the most even distribution of male and female patients). This analysis again found that a smaller liner size had a greater impact on prosthetic failure than patient sex (liner size 54 mm HR 0.340 (0.116–0.999; p=0.050) vs male sex HR 1.082 (p=0.859)).
Hypothesis 2: Failures related to bearing failure would be commonest in patients with smaller liners.
Larger liners and earlier date of implantation were associated with a significantly reduced risk of revision (table 4 and figure 9).
Figure 9.
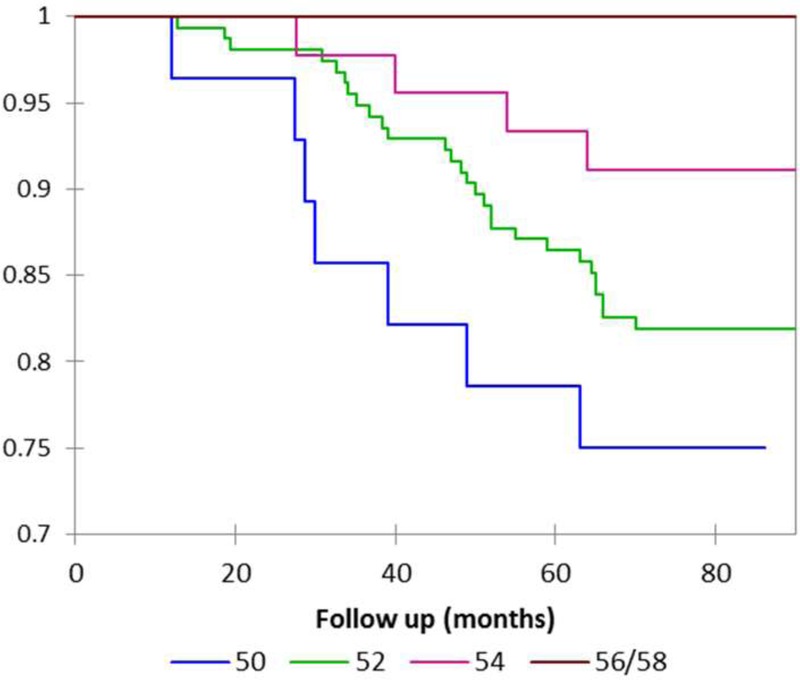
Kaplan–Meier survival curves for Pinnacle metal on metal hips implanted into female patients belonging to the late cohort (all-cause revision).
Hypothesis 3: Failures related to taper failure would be more common than those related to excessive bearing wear. Fifty of the 71 (70%) failures involved taper failure. Thirty-four failures (48%) involved bearing failure. Volumetric wear results obtained from bearing and taper surface analyses are listed in table 3. Analysis of wear rates of explants retrieved from patients with bilateral MoM prostheses revealed a significantly lower median wear rate from the CoCr surfaces than in those retrieved from unilateral patients (table 3).
Hypothesis 4: Failures related to taper failure would be more commonly found in patients with Corail stems.
The Corail stem was not significantly associated with a greater risk of taper failure than the SROM stem. Only the presence of bilateral MoM joints and later implantation date were associated with a greater risk of revision associated with taper failure (table 4).
Hypothesis 5: The Pinnacle system would be relatively resistant to the effects of cup position and ARMD would, in general, be unrelated to cup position.
The statistical analysis is described in detail in online supplementary appendix 1. The variable with the greatest power to explain the variation in blood Co and Cr was liner size (figure 10). Liner size, duration from primary procedure to venesection and cup angles of inclination and anteversion were found to explain approximately only 12% of the variation in the Cr metal ion results and only 5% of the variation in the Co results. Patients with cups placed in accordance with the latest version of the Pinnacle surgical manual28 (40–45° inclination and 10–20° of anteversion) had a median Co concentration greater than all other unilateral patients (1.89 vs 1.69 µg/L; p=0.445) and a significantly lower survival rate (69.9% (49.3–89.7) vs 82.7% (78.4–87%)) at 9 years (where X-rays were unavailable for analysis cup position was assumed optimal in order to provide the worst outcome scenario for this patient group).
Figure 10.
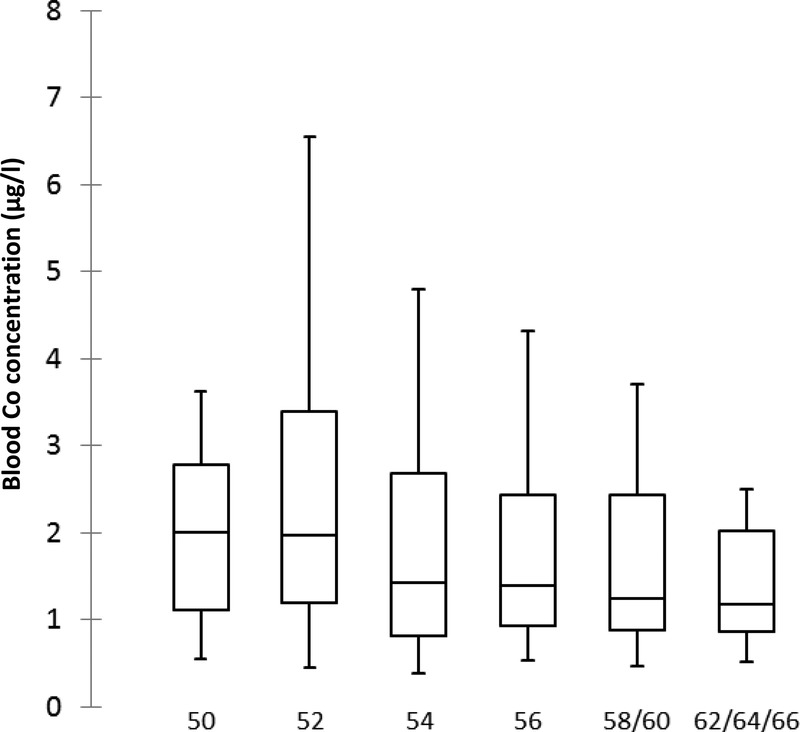
In this box and whisker chart, unilateral patients were grouped according to liner sizes and the blood Co distributions plotted (blood Co concentrations measured in µg/L).
Cumulative revision rates (for all-cause revision) with numbers at risk in the various survival analyses described above are given in online supplementary appendix 3.
bmjopen-2015-007847supp_appendix3.pdf (214.7KB, pdf)
Discussion
While the exact number of 36 mm MoM Pinnacle implantations is not publicly known, a rough estimate can be extrapolated from the information from DePuy sales records released in the ongoing DePuy litigation proceedings.29 30 Approximately 93 000 ASRs were sold globally, with around 6000 reported in the NJR of England and Wales. The 2014 Annual NJR Report lists 11 871 MoM Pinnacle implantations. If England and Wales represent the same proportion of Pinnacle as ASR implantations then it is not unreasonable to suggest that the Pinnacle MoM system has been implanted into over 180 000 patients globally, making it the most commonly used large diameter MoM THR in the world.
There is a sharp contrast between the reported performance of the Pinnacle MoM in North America compared with Europe (table 5). It is not clear why this is, although examination of the literature reveals an American preference for the use of CoCr uncemented stems and a heavier financial influence from manufacturers in American studies.29 There appears to be a stricter consensus guidance-directed follow-up in Europe following a more aggressive management stance from European regulators such as the medicines and healthcare regulatory agency (MHRA).31 Pinnacles in the American studies were also, in general, implanted earlier. This is the first study of its kind to combine clinical data, blood ion concentrations and explant analysis in an attempt to better understand the performance of this widely used device.
Table 5.
A comparison of the existing published literature on the performance of the 36 mm Pinnacle MoM hip arthroplasty system
| Authors | Source | Per cent of 36 mm diameter Pinnacles | Implantation date | Number of hips | Stems | Mean FU | Prospective | Blood Co >5 µg/L (%) | Survival | Risk factors (examined/positive) |
|---|---|---|---|---|---|---|---|---|---|---|
| Engh et al32 | USA | 100 | 2001–2002 | 131 | AML/prodigy (CoCr) | 5 years | No | Not reported | 98% at 5 years | Not examined |
| Engh et al34 | USA | 100 | 2003–2005 | 32 | AML/prodigy (CoCr) | 2 years (maximum) | Yes | Not reported | Not reported | Not examined |
| Antoniou et al42 | Canada | 100 | 2005–2006 | 58 | Prodigy (CoCr) | 1 year | Yes | 6.9% | Not reported | Not examined |
| Barrett et al43 | USA | 98.8 | 2001–2009 | 778 | Endurance prodigy replica SROM AML Summit |
4.2 years | Yes | Not reported | 97% at 5 years | Not examined |
| Smith et al40 | Canada | Not reported | Not reported | 16 | Not reported | 3.4 years | Yes | 6.25% | Not reported | Not examined |
| Bernasek et al44 | USA | 86 | 2001–2005 | 430 | Summit (Ti) | 6.8 years | No | Not reported | 95.8% at 9 years | None |
| Liudahl et al45 | USA | 97 | 2002–2006 | 169 | Summit (Ti) | 4.7 years | Yes | Not reported | 99.4% at 4 years | None |
| Matharu et al35 | Europe | 97.6 | 2004–2010 | 578 | Corail (Ti) | 5 years | No | 8.7% above 7 | 88.9 at 8 years | Sex (p=0.053) |
| Lainiala et al46 | Europe | 100 | 2002–2010 | 430 | Corail/SROM/Summit (Ti), prodigy (CoCr) | 7.5 years | No | 16.1% | 86% at 9 years | Gender; age; bilaterality; stem Sex (p=0.069) |
| Langton et al | Europe | 100 | 2003–2009 | 488 | Corail/SROM (Ti) | 7.2 years | No | 10.9% | 83.6% at 9 years | Sex; age; stem; bilaterality; liner size; year of implantation |
FU, follow-up, MoM, metal on metal.
Up until recently, the existing work on the MoM Pinnacle focused mainly on blood ion concentrations rather than survivorship. Engh et al32 reported on metal ion concentrations in patients implanted with 36 mm MoM Pinnacle devices and compared them to the results of patients with 28 mm MoM Pinnacles. Accepted tribological theory indicates that the larger 36 mm bearing should exhibit lower bearing wear rates due to an improved lubricating regime.33 In their comparison of the two groups, the authors noted: ‘although it is reassuring that the levels were not different, the question remains why the 36 mm MoM ion levels were not lower’. The same surgical group subsequently studied the incidence of adverse local tissue reactions in their patients. They described a survivorship analysis of their 945 36 mm MoM Pinnacle hips which revealed a 1% chance at 3 years that tissue retrieved at revision consistent with a reaction to a MoM bearing would be identified.34
Recently, Barrett et al published the results of a multicentre investigation into the incidence of Pinnacle MoM revision for ARMD. Barrett et al surmised that the results represented good survivorship and a low incidence of ARMD at up to 5-year follow-up. We have reservations about these conclusions as radiographic evaluation of postoperative cup inclination was obtained in only 420 (54%) of the 779 patients and in only 6 of 7 revision cases.
The survival rate of the Pinnacle MoM at our unit (83.6% at 9 years) is consistent with recent studies by investigators who conducted more rigorous follow-up in keeping with consensus guidelines.2 Matharu et al35 described a cumulative survival rate of the Corail Pinnacle MoM system at 8 years of 88.9% (78.5–93.4). Most recently, Lainiala et al36 reported an overall survival rate of 86% (82–90) at 9 years with the Pinnacle MoM bearing system used primarily in combination with the Summit stem. Both groups noted a trend, albeit a non-significant one, towards an increased failure rate in female patients. Unfortunately, neither of the studies examined the impact of liner size on prosthetic survival. The absence of liner size as a risk factor in a statistical analysis may have reduced the impact of other variables, most notably the presence of bilateral MoM joints. This may provide some explanation for the differing conclusions between authors.
In the current paper, Corail stems were associated with greater blood Co concentrations and greater taper wear rates than SROMs (see online supplementary appendices 1 and 2). However, this did not equate to an increase in taper failure identified on explant analysis or revision rate. This result is at odds with DePuy's own internal studies which found a 5-year revision rate of the Corail Pinnacle of 14.1% vs 4.78% for the SROM Pinnacle MoM systems.29 We have yet to identify clear evidence of mechanically assisted crevice corrosion37—the classical theory of taper failure—and thus do not believe that a CoCr on CoCr head stem combination protects from this mode of failure. The use of mixed metallurgy hip systems therefore should not entirely explain the difference in failure rates between the North American and European studies. Other factors appear to be more important than stem type in the success or failure of the device.
An important consideration in the failure of the Pinnacle MoM hip is that of variation brought about by manufacturing processes. Following analysis of a large collection of MoM devices obtained via the NRR, we have previously reported that a number of components used in the Pinnacle hip system were produced with diametrical clearances outside of the manufacturers’ stated tolerances.8 Components produced from 2006 onwards appeared to be the most commonly affected (figure 3 and online supplementary appendix 2). Lower clearances render bearings vulnerable to clamping/lubricant starvation should the cups deflect greater than expected when press fit into the acetabulum.38 Even in the absence of frank clamping, liner distortion can alter the tribological properties of the bearings leading to increased friction, which in turn renders a prosthesis susceptible to increased wear from the bearing or taper surfaces.39 Squire et al38 showed that Pinnacle Ti shells undergo large dimensional changes when press fit into the acetabulum. They demonstrated that shells of size 50 mm, 52 mm and 54 mm have similar stiffnesses, yet the corresponding liners have walls which decrease in thickness as shell sizes decrease. This can be seen clearly in figure 6. Smaller diameter liners therefore would likely be the most vulnerable to deflection and this is something we have shown in a small unpublished study using sawbones. Liner deflection may well explain why smaller Pinnacle liner sizes were associated with higher blood ion concentrations (figure 10) and a higher failure rate (figure 9).
We observed great variation (apparently random, varying between batches) in the as manufactured surface finish of the female taper surfaces. It appears that this surface finish, as is the case with male taper roughness, is a critical factor in material loss at this junction (see online supplementary appendix 2). Without a large number of sterile implants from the different years of manufacture, however, it is currently impossible to know whether variation in taper surface finishes in and of itself explains the difference in failure rates between the patient cohorts pre-2006 and post-2006. At present, there appears to be no clear relationship between date of manufacture and taper roughness. We therefore believe that the increased failure rate of the late cohort is more likely explained by the increasing tendency in later years to produce devices with very low clearances. This would have the knock on effect of placing the taper junction under greater stress from increased frictional forces generated from the bearing surfaces.
We did not identify a strong relationship between acetabular cup orientation and blood ion concentrations in this large data set and we can conclude definitively that failures in this series were not brought about by inaccurate cup placement. These results are consistent with Matharu et al's,35 Smith et al's40 and Lainiala et al's.36 There was however a trend towards larger blood Co concentrations with longer follow-up and in patients implanted with Corail stems. This was not the case with respect to Cr. At lower levels, increased Co concentrations relative to Cr are indicative of taper failure—direct physical evidence of which was obtained from explant analysis. This confirmed that in 50% of the explants, there was no excessive wear from the bearing surfaces, yet taper failure had occurred in 50 of 71 retrieved Pinnacles. The 5-year follow-up study on 36 mm Pinnacle metal ions by the Engh group found changes similar to ours—a Co level that rises significantly over time in the absence of a corresponding change in Cr. We believe that the patients in Engh's cohort were experiencing the phenomena we describe in this paper.41
The issue of progressive taper damage over time is disturbing as smaller amounts of taper debris are associated with greater tissue damage than equivalent doses from the bearing surfaces.20 We have stated previously that total metal dose itself does not explain the variation in soft tissue damage/extent of ARMD observation at revision surgery.18 In fact, in our experience, a patient implanted with a prosthesis experiencing extremely high rates of volumetric wear with massive concentrations of metal ions in the periprosthetic tissue develop extensive soft tissue injury relatively infrequently.19 Soft tissue damage is often associated with heavy lymphocyte infiltration implying that it is the immune response that is integral to the development of tissue necrosis rather than a direct toxic insult. It is likely therefore that debris released from taper junctions is more immunogenic. We also found that patients with bilateral joints were at significantly greater risk of developing ARMD. This observation is also compatible with the process of a patient becoming sensitised to excessive metal debris from a malfunctioning joint, with a negative immune cascade subsequently precipitated by small amounts of metal generated from a well-functioning joint.21
Female patients were at greater risk of early device failure. This is a finding reported on multiple occasions by multiple sources.10 Unfortunately, despite the standardisation of the bearing diameters in this study, the shell sizes and thus thicknesses of the liners were a critical confounding variable. Indeed the Cox proportional hazard model described herein to analyse the risk of bearing failure found that liner size and/or earlier year of liner manufacture was a greater threat to prosthetic survival than patient sex. This analysis needs to be repeated, ideally with National Joint Registry statistics.
Finally, a significant number of patients were lost to follow-up. We have assumed in our survival analyses that these patients are asymptomatic at present. This is a major assumption and joint survival rates reported herein are likely to represent ‘best outcome scenario’.
In summary, in patient cohorts undergoing contemporary MoM follow-up, the Pinnacle MoM device has a high mid-term failure rate, meaning tens of thousands of patients around the world are at risk of early revision surgery. Optimal cup orientation does not afford protection to the patient. The presence of bilateral MoM prostheses appears to increase the risk of joint failure. Other risk factors appear to be smaller liner sizes and female sex. Variations in manufacturing may play a significant role in prosthetic failure and we recommend further investigation using larger data sets. Taper failure appears to be time dependent and a rising Co level should alert the clinician.
In general, however, the wear rates of the MoM bearing surfaces retrieved from patients in this series were low. Consistent with this observation, we found that the clinical performance of unilateral Pinnacle hips produced before 2006 was extremely encouraging, providing some evidence that MoM technology can in certain circumstances be used successfully if taper junctions are suitably optimised.
Footnotes
Twitter: Follow Thomas Joyce at @metalhip_ncl
Collaborators: Thomas Joyce James Lord.
Contributors: DJL contributed to the conception and design of the study, acquisition and interpretation of the data, wrote the initial draft of the paper and gave final approval of the manuscript. RPS, PA, SW, GT, TJ, JL, NC, RL, AVFN contributed to the conception and design of the study, acquisition and interpretation of the data, revision of the initial drafts of the paper and gave approval of the final manuscript.
Funding: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: DJL, AVFN, TJ and NC are retained experts for plaintiffs in ongoing metal on metal litigation. DJL and AVFN have worked with the United States Department of Justice in litigation involving DePuy.
Ethics approval: Ethical approval for this study and the NRR data collection was given by the local research ethics council (LREC) County Durham and Tees Valley 2 under an extension of the existing project “The Assessment of Failed Hip Resurfacings” (reference number 09/H0905/41).
Provenance and peer review: Not commissioned; externally peer reviewed.
Data sharing statement: No additional data are available.
References
- 1.12th Annual Report. National Joint Registry of England and Wales 2015.
- 2.Hannemann F, Hartmann A, Schmitt J et al. European multidisciplinary consensus statement on the use and monitoring of metal-on-metal bearings for total hip replacement and hip resurfacing. Orthop Traumatol Surg Res 2013;99:263–71. 10.1016/j.otsr.2013.01.005 [DOI] [PubMed] [Google Scholar]
- 3.Bolland BJ, Culliford DJ, Langton DJ et al. High failure rates with a large-diameter hybrid metal-on-metal total hip replacement: clinical, radiological and retrieval analysis. J Bone Joint Surg Br 2011;93:608–15. 10.1302/0301-620X.93B5.26309 [DOI] [PubMed] [Google Scholar]
- 4.Malviya A, Ramaskandhan JR, Bowman R et al. What advantage is there to be gained using large modular metal-on-metal bearings in routine primary hip replacement? A preliminary report of a prospective randomised controlled trial. J Bone Joint Surg Br 2011;93:1602–9. 10.1302/0301-620X.93B12.27533 [DOI] [PubMed] [Google Scholar]
- 5.Bozic KJ, Kurtz S, Lau E et al. The epidemiology of bearing surface usage in total hip arthroplasty in the United States. J Bone Joint Surg Am 2009;91:1614–20. 10.2106/JBJS.H.01220 [DOI] [PubMed] [Google Scholar]
- 6.Theodorou EG, Provatidis CG, Babis GC et al. Large diameter femoral heads impose significant alterations on the strains developed on femoral component and bone: a finite element analysis. Open Orthop J 2011;5:229–38. 10.2174/1874325001105010229 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Griffin WL, Nanson CJ, Springer BD et al. Reduced articular surface of one-piece cups: a cause of runaway wear and early failure. Clin Orthop Relat Res 2010;468:2328–32. 10.1007/s11999-010-1383-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Langton DJ, Ngu A, Nargol AVF. Failure of the ASR and Pinnacle Metal on Metal Hip systems: Issues with Manufacturing? British Hip Society Annual Meeting; 2014. [Google Scholar]
- 9.De Haan R, Campbell PA, Su EP et al. Revision of metal-on-metal resurfacing arthroplasty of the hip: the influence of malpositioning of the components. J Bone Joint Surg Br 2008;90:1158–63. 10.1302/0301-620X.90B9.19891 [DOI] [PubMed] [Google Scholar]
- 10.Pandit H, Glyn-Jones S, McLardy-Smith P et al. Pseudotumours associated with metal-on-metal hip resurfacings. J Bone Joint Surg Br 2008;90:847–51. 10.1302/0301-620X.90B7.20213 [DOI] [PubMed] [Google Scholar]
- 11.De Haan R, Pattyn C, Gill HS et al. Correlation between inclination of the acetabular component and metal ion levels in metal-on-metal hip resurfacing replacement. J Bone Joint Surg Br 2008;90:1291–7. 10.1302/0301-620X.90B10.20533 [DOI] [PubMed] [Google Scholar]
- 12.Langton DJ, Jameson SS, Joyce TJ et al. Accelerating failure rate of the ASR total hip replacement. J Bone Joint Surg Br 2011;93:1011–16. 10.1302/0301-620X.93B8.26040 [DOI] [PubMed] [Google Scholar]
- 13.Underwood RJ, Zografos A, Sayles RS et al. Edge loading in metal-on-metal hips: low clearance is a new risk factor. Proc Inst Mech Eng H 2012;226:217–26.. 10.1177/0954411911431397 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Steele GD, Fehring TK, Odum SM et al. Early failure of articular surface replacement XL total hip arthroplasty. J Arthroplasty 2011;26(6 Suppl):14–18. 10.1016/j.arth.2011.03.027 [DOI] [PubMed] [Google Scholar]
- 15.Ardaugh BM, Graves SE, Redberg RF. The 510(k) ancestry of a metal-on-metal hip implant. N Engl J Med 2013;368:97–100. 10.1056/NEJMp1211581 [DOI] [PubMed] [Google Scholar]
- 16.Elkins JM, Kruger KM, Pedersen DR et al. Edge-loading severity as a function of cup lip radius in metal-on-metal total hips—a finite element analysis. J Orthop Res 2012;30:169–77. 10.1002/jor.21524 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Langton DJ, Jameson SS, Joyce TJ et al. Early failure of metal-on-metal bearings in hip resurfacing and large-diameter total hip replacement: a consequence of excess wear. J Bone Joint Surg Br 2010;92:38–46. 10.1302/0301-620X.92B1.22770 [DOI] [PubMed] [Google Scholar]
- 18.Langton DJ, Joyce TJ, Jameson SS et al. Adverse reaction to metal debris following hip resurfacing: the influence of component type, orientation and volumetric wear. J Bone Joint Surg Br 2011;93:164–71. 10.1302/0301-620X.93B2.25099 [DOI] [PubMed] [Google Scholar]
- 19.Langton DJ, Sidaginamale RP, Joyce TJ et al. The clinical implications of elevated blood metal ion concentrations in asymptomatic patients with MoM hip resurfacings: a cohort study. BMJ Open 2013;3:pii: e001541 10.1136/bmjopen-2012-001541 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Langton D, Sidaginamale R, Lord J et al. Metal debris release from taper junctions appears to have a greater clinical impact than debris released from metal on metal bearing surfaces. Bone Joint J Orthop Proc Suppl 2013;95(Suppl 1):28. [Google Scholar]
- 21.Madanat R, Hussey DK, Donahue GS et al. The symmetry of adverse local tissue reactions in patients with bilateral simultaneous and sequential ASR hip replacement. J Arthroplasty 2015;30:1794–8. 10.1016/j.arth.2015.04.036 [DOI] [PubMed] [Google Scholar]
- 22.Brock TM, Sidaginamale R, Rushton S et al. Shorter, rough trunnion surfaces are associated with higher taper wear rates than longer, smooth trunnion surfaces in a contemporary large head metal-on-metal total hip arthroplasty system. J Orthop Res 2015;33:1868–74. 10.1002/jor.22970 [DOI] [PubMed] [Google Scholar]
- 23.Panagiotidou A, Meswania J, Hua J et al. Enhanced wear and corrosion in modular tapers in total hip replacement is associated with the contact area and surface topography. J Orthop Res 2013;31:2032–9. 10.1002/jor.22461 [DOI] [PubMed] [Google Scholar]
- 24.Natu S, Sidaginamale RP, Gandhi J et al. Adverse reactions to metal debris: histopathological features of periprosthetic soft tissue reactions seen in association with failed metal on metal hip arthroplasties. J Clin Pathol 2012;65:409–18. 10.1136/jclinpath-2011-200398 [DOI] [PubMed] [Google Scholar]
- 25.Sidaginamale RP, Joyce TJ, Lord JK et al. Blood metal ion testing is an effective screening tool to identify poorly performing metal-on-metal bearing surfaces. Bone Joint Res 2013;2:84–95. 10.1302/2046-3758.25.2000148 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Sieber HP, Rieker CB, Köttig P. Analysis of 118 second-generation metal-on-metal retrieved hip implants. J Bone Joint Surg Br 1999;81:46–50. 10.1302/0301-620X.81B1.9047 [DOI] [PubMed] [Google Scholar]
- 27.Langton DJ, Sidaginamale R, Lord JK et al. Taper junction failure in large-diameter metal-on-metal bearings. Bone Joint Res 2012;1:56–63. 10.1302/2046-3758.14.2000047 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. http://synthes.vo.llnwd.net/o16/LLNWMB8/US%20Mobile/Synthes%20North%20America/Product%20Support%20Materials/Technique%20Guides/DSUS_JRC_0414_0026_EO_Surg%20Tech.pdf.
- 29.Herlihy-Paoli v. DePuy Orthopaedics, Inc. et al. 3:12-cv-04975 2014.
- 30.Kransky v. DePuy Orthopaedics, Inc, et al., BC456086, Superior Court of the County of Los Angeles 2012.
- 31. http://www.mhra.gov.uk/home/groups/dts bs/documents/medicaldevicealert/con155767.pdf.
- 32.Engh CA Jr, MacDonald SJ, Sritulanondha S et al. 2008 John Charnley award: metal ion levels after metal-on-metal total hip arthroplasty: a randomized trial. Clin Orthop Relat Res 2009;467:101–11. 10.1007/s11999-008-0540-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Smith SL, Dowson D, Goldsmith AA. The effect of femoral head diameter upon lubrication and wear of metal-on-metal total hip replacements. Proc Inst Mech Eng H 2001;215:161–70. 10.1243/0954411011533724 [DOI] [PubMed] [Google Scholar]
- 34.Engh CA Jr, Ho H, Engh CA. Metal-on-metal hip arthroplasty: does early clinical outcome justify the chance of an adverse local tissue reaction? Clin Orthop Relat Res 2010;468:406–12. 10.1007/s11999-009-1063-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Matharu GS, Theivendran K, Pynsent PB et al. Outcomes of a metal-on-metal total hip replacement system. Ann R Coll Surg Engl 2014;96:530–5. 10.1308/003588414X14055925058030 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Lainiala O, Eskelinen A, Elo P et al. Adverse reaction to metal debris is more common in patients following MoM total hip replacement with a 36 mm femoral head than previously thought: results from a modern MoM follow-up programme. Bone Joint J 2014;96-B:1610–17. 10.1302/0301-620X.96B12.33742 [DOI] [PubMed] [Google Scholar]
- 37.Goldberg JR, Buckley CA, Jacobs JJ et al. Corrosion testing of modular hip implants. Modularity of Orthopedic Implants, ASTM STP 1997;1301:157–76. 10.1520/STP12030S [DOI] [Google Scholar]
- 38.Squire M, Griffin WL, Mason JB et al. Acetabular component deformation with press-fit fixation. J Arthroplasty 2006;21(6 Suppl 2):72–7. 10.1016/j.arth.2006.04.016 [DOI] [PubMed] [Google Scholar]
- 39.Liu F, Chen Z, Gu Y et al. Deformation of the Durom acetabular component and its impact on tribology in a cadaveric model—a simulator study. PLoS ONE 2012;7:e45786 10.1371/journal.pone.0045786 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Smith J, Lee D, Bali K et al. Does bearing size influence metal ion levels in large-head metal-on-metal total hip arthroplasty? A comparison of three total hip systems. J Orthop Surg Res 2014;9:3 10.1186/1749-799X-9-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Engh CA, MacDonald SJ, Sritulanondha S et al. Metal ion levels after metal-on-metal total hip arthroplasty: a five-year, prospective randomized trial. J Bone Joint Surg Am 2014;96:448–55. 10.2106/JBJS.M.00164 [DOI] [PubMed] [Google Scholar]
- 42.Antoniou J, Zukor DJ, Mwale F et al. Metal ion levels in the blood of patients after hip resurfacing: a comparison between twenty-eight and thirty-six-millimeter-head metal-on-metal prostheses. J Bone Joint Surg Am 2008;90(Suppl 3):142–8. 10.2106/JBJS.H.00442 [DOI] [PubMed] [Google Scholar]
- 43.Barrett WP, Kindsfater KA, Lesko JP. Large-diameter modular metal-on-metal total hip arthroplasty: incidence of revision for adverse reaction to metallic debris. J Arthroplasty 2012;27:976–83.e1. 10.1016/j.arth.2012.01.019 [DOI] [PubMed] [Google Scholar]
- 44.Bernasek TL, Polikandriotis JA, Levering MF et al. Five-to ten-year outcomes for modular metal-on-metal total hip arthroplasty. J Arthroplasty 2013;28:1231–4. 10.1016/j.arth.2013.03.012 [DOI] [PubMed] [Google Scholar]
- 45.Liudahl AA, Liu SS, Goetz DD et al. Metal on metal total hip arthroplasty using modular acetabular shells. J Arthroplasty 2013;28:867–71. 10.1016/j.arth.2012.10.019 [DOI] [PubMed] [Google Scholar]
- 46.Lainiala O, Reito A, Elo P. Revision of metal-on-metal hip: prostheses results in marked reduction of blood cobalt and chromium ion concentrations. Clin Orthop Relat Res 2015;473:2305–13. 10.1007/s11999-015-4156-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2015-007847supp_appendix2.pdf (1.3MB, pdf)
bmjopen-2015-007847supp_appendix1.pdf (191.6KB, pdf)
bmjopen-2015-007847supp_appendix3.pdf (214.7KB, pdf)