

Highlights
-
•
There were only two reported cases of SLE manifesting gastrointestinal perforation.
-
•
Our case is the first SLE patient who developed fatal perforation in the colon.
-
•
CMV and microembolism-induced ischemia seemed responsible for the perforation.
Keywords: Cytomegalovirus, Systemic lupus erythematosus, Steroid, Perforation
Abstract
Introduction
Cytomegalovirus (CMV) infection of the gastrointestinal tract is an uncommon illness, but can be observed in immunocompromised patients. Systemic lupus erythematosus (SLE) patients are generally at high risk of CMV infection. Here we report a subacute progressive case of colitis in SLE accompanied by cytomegalovirus infection.
Presentation of case
The patient, a 79-year-old woman, was hospitalized complaining of fever, polyarthritis, and skin ulcer that had lasted seven days. She additionally manifested vomiting, high fever, and right abdominal pain within two weeks thereafter, and was diagnosed with perforation of the intestine. Emergency operation was carried out for panperitonitis due to perforation of one of the multiple colon ulcers. Multidisciplinary postoperative treatment could not save her life. Pathological examination suggested that cytomegalovirus infection as well as cholesterin embolization contributed to the rapid progression of colitis.
Discussion
There have been only a limited number of case reports of CMV enteritis in SLE. Moreover, only two SLE patients on multiple medications have been reported to experience gastrointestinal perforation. Viral infections, including CMV, can induce clinical manifestations resembling SLE and for this reason we suspect that there are potentially many more patients misdiagnosed and/or unreported.
Conclusion
Our case underscores the importance of exploring the possibility of CMV infection as a differential diagnosis in SLE patients with obvious gastrointestinal symptoms who were treated by immunosuppressive drugs.
1. Introduction
Cytomegalovirus (CMV) infection of the gastrointestinal tract is an uncommon illness, but can be observed in immunocompromised patients.
Systemic lupus erythematosus (SLE) patients are generally at high risk of CMV infection [1], [2], [3]. On the other hand, CMV gastrointestinal infection per se can induce a variety of symptoms, such as abdominal pain, diarrhea, bleeding, and perforation, mimicking those of lupus enterocolitis [4]. Therefore, it is clinically critical to determine whether these symptoms are stemming from exacerbation of SLE or caused by CMV infection. Here we report an SLE patient on long-term steroid treatment who contracted CMV infection that progressed to fatal colonic perforation.
2. Presentation of case
A 79-year-old woman visited a local practitioner complaining of low grade fever, polyarthritis, and skin ulcers that had lasted seven days. She had been diagnosed with SLE at the age of 51 and continued to be treated with prednisolone for 28 years. Her comorbidities were severe aortic valve stenosis, coronary artery stenosis, emphysematous cystitis, hypertension, and steroid-induced diabetes. She was also medicated with aspirin and limaprost alfadex.
She was referred to our hospital for further examination to assess her symptoms. Laboratory findings showed anemia (hemoglobin 8.0 g/dL), malnutrition (total protein 4.3 g/dL, albumin 2.0 g/dL), and elevated inflammatory reaction (C-reactive protein 3.39 mg/dL). Based on a positive fecal occult blood test, she underwent total colonoscopy, which revealed multiple ulcers in various locations of the colon (Fig. 1). Three days later, vomiting, high grade fever, and right abdominal pain appeared. In addition to high levels of serum procalcitonin (70.5 ng/mL) and C-reactive protein (16.39 mg/dL), CT scan revealed massive free air in the abdominal cavity (Fig. 2). Taken together, colonic perforation was strongly suggested. During an emergency operation, a hole of 5 mm in diameter was found in the transverse colon. In addition, the nearby wall was thin and fragile, thus we performed en-bloc resection of this segment by colostomy (Fig. 3). CMV-positive cells were found at all ulcer sites of biopsied specimens by colonoscopy and surgically resected specimens (Fig. 4). Moreover, needle-like structures, presumably cholesterin crystal, were observed within microvessels at ulcer sites.
Fig. 1.
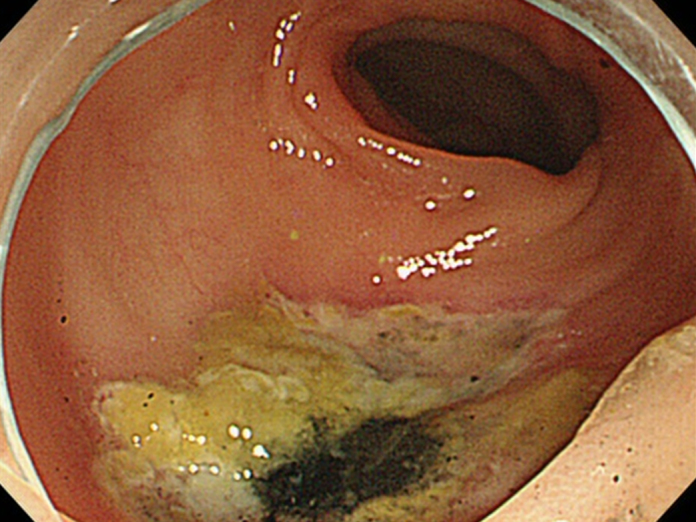
Colonoscopic findings of a typical colon ulcer.
Fig. 2.

An abdominal CT scan revealed free air in the peritoneal cavity (arrowheads).
Fig. 3.
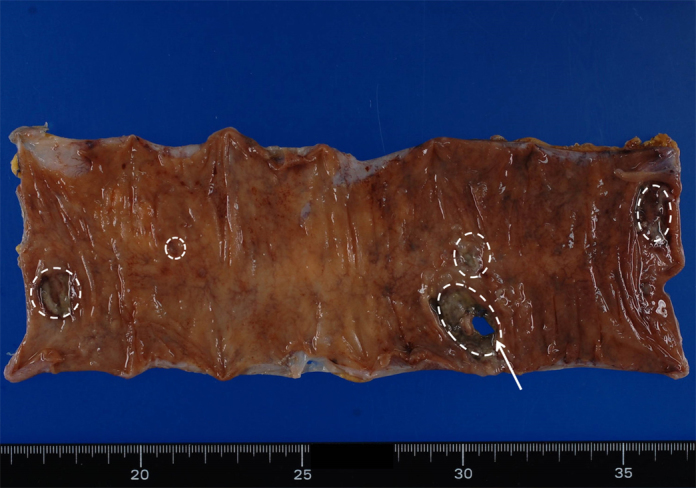
Macroscopic appearance of the excised segment of the transverse colon bearing five ulcers (dashed lines) and a perforation (arrow).
Fig. 4.
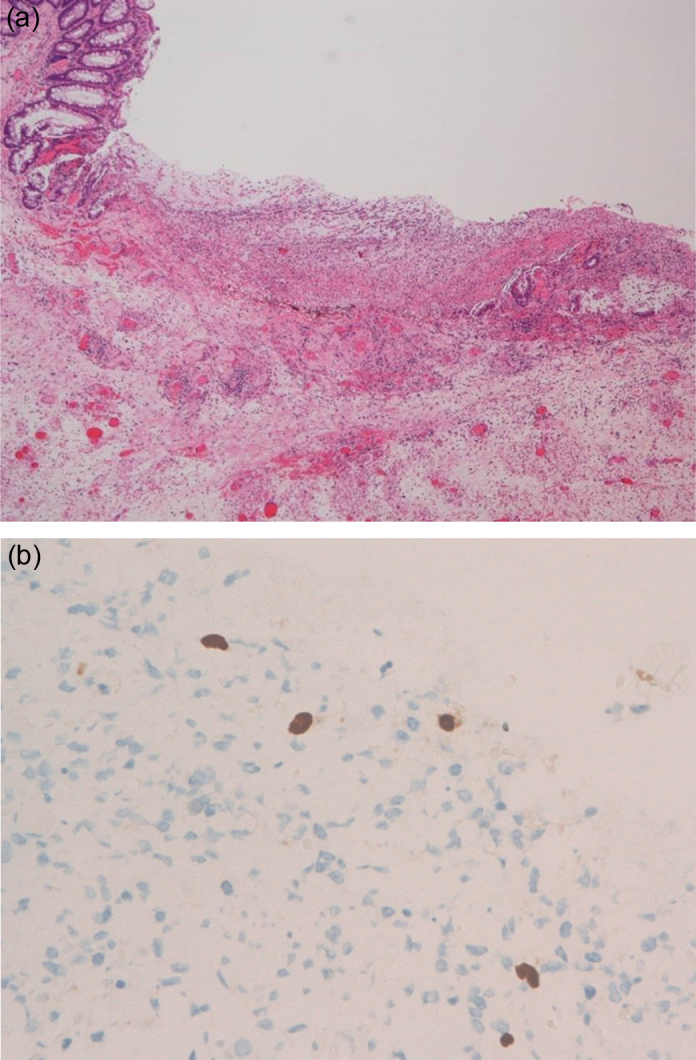
(a) Histological appearance of an ulcerative lesion of the transverse colon (hematoxylin and eosin staining, original magnification: 40×). (b) Immunohistochemical staining showed CMV-positive cells in the ulcerated lesion (original magnification: 400×).
The patient was already in shock by the end of surgery. Despite meticulous therapies, including ganciclovir administration and polymyxin B-immobilized fiber column direct hemoperfusion, her general condition gradually deteriorated and she died of subsequent multiple organ failure nine days after surgery.
3. Discussion
CMV is classified as a herpes virus, and more than a half of the adult population is thought to have antibodies for CMV [5]. Immunosuppressive drugs represent the gold standard treatment for collagen disease with major organ involvement [6]. Although the direct effect of steroid use on susceptibility to CMV infection has not been clearly established in vitro, recent clinical studies have suggested that systemic steroid use is a risk factor for CMV disease among immunocompromised patients [1], [2], [3]. A high mortality rate has been reported in CMV-positive immunocompromised hosts [7], [8]. AIDS patients co-infected with CMV have been reported to develop intestinal perforation with an 89% mortality rate [9].
Viral infections, including CMV, can induce clinical manifestations resembling SLE [4]. On the other hand, viral and bacterial infections themselves may serve as a trigger for the development and exacerbation of SLE. Ramos-Casals et al. pointed out that viral infection is not routinely investigated in SLE patients presenting with fever, which results in a delay of correct diagnosis and appropriate treatment for the infection and underlying disease [2]. The authors recommended viral serology using molecular tests and cultures from body fluids in the work-up of these patients, especially those under immunosuppression [2].
There have been only a limited number of case reports of CMV enteritis in SLE [10], [11], but we suspect that there are potentially many more patients misdiagnosed and/or unreported for the aforementioned reasons. Moreover, only two SLE patients on multiple medications, such as azathioprine and mycophenolic acid in addition to a steroid, have been reported to experience gastrointestinal perforation [12], [13]. Our patient developed CMV-induced colonic ulceration with subsequent perforation under steroid medication alone. Pathological examination revealed ischemic change in the ulcerated lesions due to cholesterin embolization. Therefore, we surmise that the perforation could have been caused by multiple factors, such as CMV infection and microembolism-induced ischemia in this patient.
4. Conclusion
Our case underscores the importance of exploring the possibility of CMV infection as a differential diagnosis in SLE patients with obvious gastrointestinal symptoms who were treated by immunosuppressive drugs.
Conflict of interest
All authors have no conflict of interest.
Funding
No funding.
Ethical approval
No available.
Authors’ contributions
Yuichi Tachikawa: Case report concept, postoperative treatment, and writing the paper.
Hiroaki Nozawa: Case report concept, surgical treatment, postoperative treatment, and writing the paper.
Junichiro Tanaka, Soichiro Ishihara, Eiji Sunami: Surgical treatment and postoperative treatment.
Takeshi Nishikawa, Toshiaki Tanaka, Tomomichi Kiyomatsu, Keisuke Hata, Kazushige Kawai, Shinsuke Kazama, Hironori Yamaguchi, Joji Kitayama: Postoperative treatment and review of the paper.
Madoka Fujisawa, Katutoshi Takahashi: Preoperative medical treatment and review of the paper.
Yoshiki Sakaguchi: Performing colonoscopy and review of the paper.
Tetsuo Ushiku, Masashi Fukayama: Histological studies.
Toshiaki Watanabe: Surgical treatment, review of the paper.
All authors read and approved the final manuscript.
Consent
We were not able to contact family members of the deceased patient reported in this paper, and to obtain a written informed consent. It is guaranteed that the paper has been sufficiently anonymised not to cause harm to the patient or their family.
Guarantor
Hiroaki Nozawa.
Contributor Information
Yuichi Tachikawa, Email: yuichi19810913@yahoo.co.jp.
Hiroaki Nozawa, Email: hiroanozawa-gi@umin.ac.jp.
Junichiro Tanaka, Email: tanakaj-sur@h.u-tokyo.ac.jp.
Takeshi Nishikawa, Email: nishikawata-sur@h.u-tokyo.ac.jp.
Toshiaki Tanaka, Email: toshi-t@venus.dti.ne.jp.
Tomomichi Kiyomatsu, Email: kiyomatsut-sur@h.u-tokyo.ac.jp.
Keisuke Hata, Email: hatak-sur@h.u-tokyo.ac.jp.
Kazushige Kawai, Email: kz-kawai@mvd.biglobe.ne.jp.
Shinsuke Kazama, Email: kaz-tky@umin.ac.jp.
Hironori Yamaguchi, Email: yamaguchih-sur@h.u-tokyo.ac.jp.
Soichiro Ishihara, Email: ishihara-1su@h.u-tokyo.ac.jp.
Eiji Sunami, Email: sunami-1su@h.u-tokyo.ac.jp.
Joji Kitayama, Email: kitayama-1su@h.u-tokyo.ac.jp.
Madoka Fujisawa, Email: mafujisawa-tky@umin.ac.jp.
Katutoshi Takahashi, Email: ktaka-tky@umin.ac.jp.
Yoshiki Sakaguchi, Email: sakaguchiy-int@h.u-tokyo.ac.jp.
Tetsuo Ushiku, Email: usikut-tky@umin.ac.jp.
Masashi Fukayama, Email: mfukayama-tky@umin.ac.jp.
Toshiaki Watanabe, Email: watanabe-1su@h.u-tokyo.ac.jp.
References
- 1.Takizawa Y., Inokuma S., Tanaka Y., Saito K., Atsumi T., Hirakata M., Kameda H., Hirohata S., Kondo H., Kumagai S., Tanaka Y. Clinical characteristics of cytomegalovirus infection in rheumatic diseases: multicentre survey in a large patient population. Rheumatology. 2008;47:1373–1378. doi: 10.1093/rheumatology/ken231. [DOI] [PubMed] [Google Scholar]
- 2.Ramos-Casals M., Cuadrado M.J., Alba P., Sanna G., Brito-Zerón P., Bertolaccini L., Babini A., Moreno A., D’Cruz D., Khamashta M.A. Acute viral infections in patients with systemic lupus erythematosus: description of 23 cases and review of the literature. Medicine. 2008;87:311–318. doi: 10.1097/MD.0b013e31818ec711. [DOI] [PubMed] [Google Scholar]
- 3.Kang I., Park S.H. Infectious complications in SLE after immunosuppressive therapies. Curr. Opin. Rheumatol. 2003;15:528–534. doi: 10.1097/00002281-200309000-00002. [DOI] [PubMed] [Google Scholar]
- 4.Sekigawa I., Nawata M., Seta N., Yamada M., Iida N., Hashimoto H. Cytomegalovirus infection in patients with systemic lupus erythematosus. Clin. Exp. Rheumatol. 2002;20:559–564. [PubMed] [Google Scholar]
- 5.Pamphilon D.H., Rider J.R., Barbara J.A., Williamson L.M. Prevention of transfusion-transmitted cytomegalovirus infection. Transfus. Med. 1999;9:115–123. doi: 10.1046/j.1365-3148.1999.00193.x. [DOI] [PubMed] [Google Scholar]
- 6.Smilek D.E., Ehlers M.R., Nepom G.T. Restoring the balance: immunotherapeutic combinations for autoimmune disease. Dis. Model Mech. 2014;7:503–513. doi: 10.1242/dmm.015099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Preiksaitis J.K., Brennan D.C., Fishman J., Allen U. Canadian society of transplantation consensus workshop on cytomegalovirus management in solid organ transplantation final report. Am. J. Transplant. 2005;5:218–227. doi: 10.1111/j.1600-6143.2004.00692.x. [DOI] [PubMed] [Google Scholar]
- 8.Sinclair J., Sissons P. Latency and reactivation of human cytomegalovirus. J. Gen. Virol. 2006;87:1763–1779. doi: 10.1099/vir.0.81891-0. [DOI] [PubMed] [Google Scholar]
- 9.Meza A.D., Bin-Sagheer S., Zuckerman M.J., Morales C.A., Verghese A. Ileal perforation due to cytomegalovirus infection. J. Natl. Med. Assoc. 1994;86:145–148. [PMC free article] [PubMed] [Google Scholar]
- 10.Ohashi N., Isozaki T., Shirakawa K., Ikegaya N., Yamamoto T., Hishida A. Cytomegalovirus colitis following immunosuppressive therapy for lupus peritonitis and lupus nephritis. Intern. Med. 2003;42:362–366. doi: 10.2169/internalmedicine.42.362. [DOI] [PubMed] [Google Scholar]
- 11.Takei M., Yamakami K., Mitamura K., Kitamura N., Matsukawa Y., Sawada S. A case of systemic lupus erythematosus complicated by alveolar hemorrhage and cytomegalovirus colitis. Clin. Rheumatol. 2007;26:274–277. doi: 10.1007/s10067-005-0139-4. [DOI] [PubMed] [Google Scholar]
- 12.Bang S., Park Y.B., Kang B.S., Park M.C., Hwang M.H., Kim H.K., Lee S.K. CMV enteritis causing ileal perforation in underlying lupus enteritis. Clin. Rheumatol. 2004;23:69–72. doi: 10.1007/s10067-003-0825-z. [DOI] [PubMed] [Google Scholar]
- 13.Strasser C., Wolf E.M., Kornprat P., Hermann J., Münch A., Langner C. Opportunistic cytomegalovirus infection causing colonic perforation in a patient with systemic lupus erythematosus. Lupus. 2012;21:449–451. doi: 10.1177/0961203311425529. [DOI] [PubMed] [Google Scholar]