

Abstract
Background
Transitioning into society after release from incarceration presents real challenges for male offenders; in California, up to 60% return to prison within three years following release. The risk for ongoing drug use and having sex with multiple sex partners is a significant challenge for ex-offenders preparing to enter the community.
Objectives
The aims are to describe drug use and sexual behavior (sex with multiple partners) prior to incarceration and six and 12 months following study enrollment using data obtained as part of a randomized controlled trial (RCT).
Methods
This is a planned secondary analysis of data obtained as part of an RCT designed to study the effects of intensive peer coaching and nurse case management, intensive peer coaching, and brief nurse counseling on hepatitis A and B vaccination adherence compared to a usual care control treatment that also included brief peer coaching and brief nurse counseling. Self-report data from subjects enrolled at one residential drug treatment facility in Los Angeles were captured at three time points: baseline, and six- and 12-month follow up.
Results
Findings showed substantive and significant reductions in drug use and engaging in sex with multiple partners six months following enrollment into the study compared to the baseline data, but results did not differ by study condition. At 12-month follow up, drug use and sex with multiple partners increased, but remained less than at baseline levels.
Discussion
Sustaining reductions in drug use and engaging in sex with multiple partners remains a challenge following incarceration.
Keywords: case management, drug use, forensic nursing, multiple sex partners, peer coaching, prisoners
The United States currently holds 1.5 million people within its prison system (Carson, 2014). As of August 2014, about half of all those incarcerated have drug-related offenses (Federal Bureau of Prisons, 2014). In California, the majority of the 44,335 adults are paroled once released into communities (California Department of Corrections and Rehabilitation, 2014b). As men constitute 93% of those held in prison (Carson, 2014), reducing drug use among recently released male offenders is a crucial strategy to minimize the damaging and often long-term effects of addiction. Reducing drug use behaviors is also a public health benefit that promotes the safety of society (Prendergast, 2009). However, transitioning into society after release from incarceration presents real challenges for male offenders, particularly during the first year of release (California Department of Corrections and Rehabilitation, 2013b). Ex-offenders are also more likely to suffer mental illness requiring psychiatric hospitalizations, as well as risky sexual encounters with multiple partners as compared to those not incarcerated (Kushel, Hahn, Evans, Bangsberg, & Moss, 2005). This paper reports findings from a planned, secondary analysis of drug use behaviors and multiple sex partners obtained as part of a randomized clinical trial designed to evaluate the effects of six months of intensive peer coaching and nursing case management (PC-NCM), intensive peer coaching (PC) or usual care (UC), with minimal PC and nurse involvement, on hepatitis A and B vaccine series completion among homeless men recently released on parole (Nyamathi et al., 2015).
Risky Drug and Sexual Activity
Drugs most commonly abused by state prisoners include methamphetamine, cocaine, heroin and other opiates, barbiturates, stimulants, hallucinogens, and marijuana/hashish (Mumola & Karberg, 2006). Half of federal prisoners state they used drugs before their offenses were committed (Mumola & Karberg, 2006). About two thirds (67%) of those arrested in the U.S. tested positive for at least one of five drugs (cocaine, marijuana, methamphetamine, opiates, and phencyclidine [PCP]) (Zhang, 2003). Among 627 probationers living in Illinois, half of ex-offenders interviewed reported drug use in the previous month, with 57% reporting illicit drug use in the past 12 months (Lurigio et al., 2003). Analysis of 2009 probationer data from the National Survey on Drug Use and Health (NSDUH) revealed that rates of use, abuse or dependence on illicit drugs or alcohol were approximately two to three times greater than rates among non-probationers (Feucht & Gfroerer, 2011).
Men exiting jail and prison also engage in risky sexual behaviors. In one study, 68.8% of participants upon release had unprotected sex, and over half had sex on the first day of release (Grinstead et al., 2005). In a longitudinal study among young men being released from prison, 36% had unprotected vaginal sex with more than two female partners over a six-month period (MacGowan et al., 2003).
Physical and Mental Health
Poor physical and mental health, and lack of stable shelter predict outcomes of male ex-offenders (Nyamathi, Marlow, Branson, Marfisee, & Nandy, 2012). Recently released male offenders may be managing physical injuries and poor dental health (Fickenscher, Lapidus, Silk-Walker, & Becker, 2001), as well as mental health concerns such as depression and anxiety (Staton, Leukefeld, & Webster, 2003). Male parolees with histories of chronic drug use were more likely to experience serious depression, anxiety, and trouble concentrating, while men with frequent drug use in the year before prison had more physical issues (Narevic et al., 2006). Male inmates also had higher rates of chronic medical conditions, such as hypertension, diabetes, and viral infections (HIV and hepatitis) compared to the noninstitutionalized general population, after age standardization (Wilper et al., 2009). Psychological disorders such as bipolar disorder, schizophrenia, and major depression may be four times higher in the ex-offender population as compared to the general population (Human Rights Watch, 2009). Inmates with mental health concerns have high rates of substance dependence or abuse compared to those inmates without mental health issues (James & Glaze, 2006). Finally, drug use, risky behaviors, and poor sanitation are just some of the factors which may increase the likelihood of hepatitis infection (World Health Organization [WHO], 2015), among homeless men on parole, as well as HIV and other sexually transmitted infections (Fenton, 2007; Hennessey et al., 2009).
Factors Associated With Ongoing Substance Abuse
Ex-offenders often lack adequate education and job skills (Bahr, Harris, Fisher, & Harker Armstrong, 2010), which have been linked to lifetime substance abuse (Lurigio et al., 2003). Moreover, without consistent and safe shelter the stress of homelessness and insecure living conditions may encourage injection and other illicit drug use (Seal, Margolis, Sosman, Kacanek, & Binson, 2003).
Parolees benefit from residential drug treatment (RDT) programs and length of time in treatment is important (Evans, Jaffe, Urada, & Anglin, 2012). However, many inmates never have the opportunity to participate (Sung, Mahoney, & Mellow, 2011). In the community, support services like RDT therapeutic environments have been crucial for the successful integration of recently released male offenders into society (Lim et al., 2012). Drug users on parole or probation may need assistance in managing life problems and with the transition from incarceration into the community. RDT has been found to be effective in addressing hostile or emotion-focused coping, often as a result of incarceration (Marlow et al., 2012). While at RDT sites, homeless ex-offenders are often taught coping skills designed to limit further drug use, dependence, and reduced recidivism (Marlow et al., 2012). By adjusting psychological responses to life stressors, recently released offenders may move successfully through recovery (Prendergast, 2009).
Nurse Case Management and Peer Coaching
Less understood is the placement of nurses and peer coaches within RDT programs. In particular, the impact of nurse case management (NCM) in an RDT is unknown; yet, nurse- delivered case management has been found to be effective in increasing awareness of drug-related illness among men exiting jails and prisons (Nyamathi, Marlow, Branson et al., 2012), and lowering drug use among other vulnerable populations (Nyamathi et al., 2014). Case management has been effective in reducing drug use and improving health access among opioid dependent drug users (Shanahan, Beers, Alford, Brigandi, & Samet, 2010). NCM has also been incorporated into HIV/AIDS and substance abuse programs to achieve coordinated and consistent care for clients with co-occurring disorders (Morgan & Rossi, 2007). Involvement of peer coaches (PC) is also a critical part of the solution to reduce drug use in ex-offenders. As a role model who has served time in prison and successfully transitioned into the community, the PC serves as a resource for parolees to receive support and facilitate positive change.
As presented in a paper focused on reduction of recidivism among this sample, the placement of homeless parolees in RDT programs where nurses are engaged, can further promote a time-sensitive environment where clients can access vital health care resources (Nyamathi et al., 2015). Further, peer coaching by ex-offenders, who serve as positive role models for the recently released individual, could provide a potentially useful method to empower recently released drug-using parolees to continue successful reentry into the community (Nyamathi et al., 2014).
Theoretical Framework
The comprehensive health seeking and coping paradigm (CHSCP; Nyamathi, 1989) guided this study. The CHSCP was adapted from the Lazarus and Folkman (1984) coping model and Schlotfeldt's (1981) health seeking and coping paradigm. Variables in the CHSCP including sociodemographic factors, situational, personal and social factors, and health seeking and coping strategies were thought to be related to reduction of drug use and having sex with multiple partners.
Sociodemographic factors that might relate to these outcomes include: age, education, race/ethnicity, and marital and parental status (Hennessey et al., 2009; Salem, Nyamathi, Idemundia, Slaughter, & Ames, 2013). Situational factors such as being homeless (inclusion criterion) (Nyamathi, Marlow, Zhang et al., 2012), past criminal activities, prior history of drug treatment, whether recruited from jail/prison, and severity of criminal history (level of custody and contract type) may likewise influence drug use and having sex with multiple partners. Personal factors such as engaging in substance use and having sex with multiple partners (Hennessey et al., 2009; Salem et al., 2013), and having experiencing physical and mental health problems (Nyamathi, Leake, et al., 2011) may promote risky behaviors. Having another person dependent on the ex-offender or being knowledgeable that having sex with an HIV-infected person creates risk for HIV may serve as protective factors against resuming drug use and unprotected sex with multiple persons (Nyamathi, Slagle, et al., 2011). Having low personal resources such as self-esteem can likewise impact continued drug use, aggression, antisocial behavior, and delinquency (Donnellan, Trzesniewski, Robins, Moffitt, & Caspi, 2005; Lejuez, Simmons, Aklin, Daughters, & Dvir, 2004), as well as increased sexual activities. Social factors like social support may deter these risk factors, and health seeking and coping strategies may also reduce risky behaviors of drug use and engaging in sex with multiple partners (Marlow et al., 2012).
Parent Trial: Hepatitis A and B Vaccination in Homeless Ex-Offenders
The parent randomized controlled trial (RCT) was designed to assess the impact of PC-NCM, PC, and usual care (UC) on completion of hepatitis A and B vaccination series (Nyamathi et al., 2015). Among the 345 participating exoffenders eligible for the Twinrix recombinant vaccine series, the completion rate for three or more doses was 73%; there were no differences by intervention condition, but some personal, social, and coping factors were related to vaccine noncompletion.
Among the 600 participants in the RCT, recidivism (rearrest) among participating inmates was 36.3% at six month follow up, and 51.1% at 12-month follow up; there was no association with treatment condition. Social support from drug/alcohol users (p = .004) and having used marijuana at least once a week prior to the last incarceration (p = .03) predicted rearrest. In terms of protective factors, those who participated in RDT within a substance abuse program (SAP) contract (p = .02), or spent 90 days or more in RDT (p = .001) were less likely to have been rearrested within 12 months (Nyamathi et al., 2015). These findings are interesting in that the state of California reports that nearly half (47.5%) of inmates released into the community returned to prison within six months, with 74.1% returning within 12 months (California Department of Corrections and Rehabilitation, 2013a). Our findings explained 73% variance in rearrest at either six- or 12-month follow up.
Purpose
The purpose of this secondary analysis was to assess the impact of peer coaching-nursing case management, peer coaching, and usual care on reducing drug use and multiple sexual partners among recently released male ex-offenders. These analyses complete the third critical perspective of assessing the impact of varying levels of intervention on reducing high-risk behaviors among the sample.
Methods
Participants and Setting
Prospective participants for this RCT were offenders released from Southern California prisons and county jails within the last six months and enrolled as residents in one RDT facility. The RDT facility is a nonprofit organization in Los Angeles that has existed for three decades. The focus of this facility is substance abuse treatment delivered in a therapeutic environment. The men generally stay in RDT up to six months. Inclusion and exclusion criteria, site characteristics, recruitment procedures, and randomization procedures have been described previously (Nyamathi et al., 2015). Data were collected from February 2010 to January 2013. From a total of 669 potential participants, a total of 69 men were screened out due to age outside the inclusion range, not being on parole, not released from jail or prison within the last six months prior to enrollment, or had not used drugs 12 months prior to their most recent incarceration. A total of 600 residents were recruited, and all received nominal cash incentives upon the completion of the baseline interview and follow-up questionnaires. The protocol was approved by the Institutional Review Board at the University of California Los Angeles.
Treatment Intensity Levels
Upon completion of the baseline questionnaire, ex-offenders were randomly assigned to one of three levels of intensity of treatments delivered over a six-month period: PC-NCM, PC with brief nurse counseling, and UC, which including a brief health education session by a PC and nurse counseling.
PC-NCM intervention
One dedicated nurse, trained by an expert in NCM, provided culturally competent NCM for about 20 minutes weekly over an eight-week period; sessions focused on health promotion, completion of drug treatment, hepatitis vaccination compliance (Nyamathi et al., 2015), and reduction of drug and alcohol use. Additionally, research staff spent 45 minutes each week with each assigned participant to teach him to build effective coping skills, personal assertiveness, self-management, therapeutic nonviolent communication (NVC), and self-esteem. A major focus of the sessions included ways to reduce health risks, such as illicit drug use and having multiple sexual partners. Increasing access to healthcare, building personal empowerment skills centered on seeking support, increasing assistance from community agencies, and building communication and negotiation skills were also addressed. Completion of PC-NCM sessions was 82%, while NVC sessions were 89%.
PC intervention
Participants received weekly PC interaction similar to that delivered by the PC staff of the PC-NCM program. Ninety-eight percent of sessions were completed.
UC intervention
Participants received encouragement by a nurse to complete the three series of hepatitis vaccine, which was an intervention in the main study. In addition, they received a brief 20-minute session by a PC trained on health promotion. Nearly all (99%) of the sessions were completed.
Treatment fidelity was enhanced by monitoring staff adherence to the detailed procedural manual by the project director. In addition, interventions were delivered on alternate days so staff and participants of respective programs were separated. An operations manual outlined the constructs, variables and recruitment and data collection processes. Further, the project director and principal investigator periodically monitored content delivered by means of a checklist. Maximizing the dose of the intervention is another strategy critical to maximizing fidelity. As noted above, levels of session completion were high for all programs.
Instruments
Sociodemographics
Participants responded to a structured questionnaire to report age, education, race/ethnicity, marital status, and parental status.
Situational factors
Single items asked about history of criminal activity, recruitment setting (jail or prison), and severity of criminal history (level of custody, contract type) were used to measure situational factors. Also, drug treatment programs were reported (in custody drug treatment program, residential multiservice substance care center, or parolee substance abuse program). The in custody drug treatment program (ICDTP) encompasses a total of 150 days which include 60-day in custody substance treatment program, 30 days of residential aftercare, case management and 60 day participation in community-based substance abuse programs. The residential multiservice centers (RMSC) provide basic necessities (e.g. shelter, food), substance abuse treatment, counseling, job readiness training and educational services. For those who have completed in prison substance abuse program, the substance abuse program (SAP) continues during aftercare and consists of case management (California Department of Corrections & Rehabilitation, 2007).The amount of time spent in the RDT was reported and dichotomized at the median of 90 days for analysis.
Personal factors
Self-esteem and general physical and mental health were assessed. Self-esteem was assessed by the revised Self-Esteem Inventory (SEI) (Coopersmith, 1967). The SEI is a23-item questionnaire; the reliability of scores on this scale with homeless males was .83 (Nyamathi, Flaskerud, & Leake, 1997). Reliability indexed by Cronbach's alpha was .84. Additionally, parolees were asked how they had felt about themselves as teenagers on a 5-point Likert scale ranging from 1 = liked yourself a great deal to 5 = disliked yourself a great deal. Knowledge that having sex with someone infected with HIV can lead to the person becoming HIV infected was also assessed.
Questions from the Medical Outcomes Study (MOS; Stewart, Hays, & Ware, 1988) were used to measure overall health and emotional health. Participants rated overall general health using a single item with a 5-point scale; response options were poor, fair, good, very good, and excellent, which were dichotomized as 0 = poor or fair or 1 = good, very good, or excellent. The MOS Mental Health Inventory (MHI-5) was used to measure emotional well-being (Stewart et al., 1988) on a scale of 0-100. Scores on the MHI have well-established reliability and validity. An established cut-point of 66 (Rubenstein et al., 1989) was used to identify emotional well-being (0 = no; 1 = yes).
Social factors
The 18-item MOS Social Support Survey (Sherbourne & Stewart, 1991) was used to measure four types of social support: emotional support (eight items; reliability in this sample was .95); tangible support (four items; reliability was .88); positive support (three items; reliability was .89); and affective support (three items; reliability was .90). Items had 5-point Likert-type response options ranging from 1 = none of the time to 5 = all of the time. Responses were summed for subscale formation with higher scores indicating more support. Respondents were also asked how many close friends they had outside of jail/prison which was dichotomized at the upper quartile of six for analysis. They were asked at baseline if their primary source of social support was drug users or nonusers.
Health seeking and coping
Planning coping, disengagement coping, and self-blame coping were measured using items from the Brief COPE (Carver, 1997). Item responses ranged from 1 = I do not do this at all to 4 = I do this a lot, with higher scores indicating that the respondent was more likely to practice that coping strategy.
Outcome variables
This study focused on reduction of drug use (stimulants, marijuana, and heroin) and having sex with multiple partners. Substance use was assessed by the modified version of the Texas Christian University Drug History Form (TCU/DHF; Simpson & Chatham, 1995). The TCU/DHF assessed the frequency of use of marijuana, stimulants, heroin, and seven other drugs six months prior to their most recent incarceration (baseline assessment), and repeated at six- and 12-month follow up. A nine-point ordinal response scale incorporating times per day, week, and month was used, ranging from 0 = never/not used to 8 = 4 or more times per day. Number of sexual partners was assessed by a single item that asked participants to self-report the number of different sexual partners during the six-month period prior to the last incarceration (at baseline), and at six- and 12-month follow up. This measure on sexual partners was dichotomized as multiple (defined as two or more during the six-month period) or not. The drug use measures were considered as continuous variables, as well as in terms of cessation (1 =yes or 0 = no); more specifically, participants were asked if they engaged in these behaviors during the observation period.
Data Analysis
Sample characteristics were described with frequencies and percentages, means and standard deviations, or medians. Key outcome variables of drug use (marijuana, stimulants, and heroin), and multiple sexual partners were first described in percentages at all three points in time (baseline, six months, and 12 months). Split-Plot ANOVA tests of the four outcome variables, as well as the tests of time by group interactions, were conducted based on the frequency that participants engaged in behaviors pertaining to the four outcomes during each of the three observation periods. An ordinal scale was used to capture the frequencies of these behaviors: 0 = never/not used; 1 = only 1-3 times per month; 2 = about 1 time per month; 3 = about 2-3 times per month; 4 = about 1 time per week; 5 = about 2-6 times per week; 6 = about 1 time per day; 7 = about 2-3 times per day; and 8 = about 4 or more times per day. Sexual partners were measured in the actual number of partners reported by respondents during the observation periods. Dichotomous variables were then created to identify those who reported having used the three main types of drugs at the baseline, but then stopped using during the 12-month observation period (i.e., with both six- and 12-month follow ups combined), as well as for cessation of having multiple sex partners. Those who stopped using during the follow-up period were coded as “1” and those who continued to use or started using were coded as “0.” Variables related to these key outcome variables in bivariate analyses at the p ≤ .10 level were then assessed as predictors in multiple logistic regression models. Any covariate found to be significant for any outcome was initially included in all models of drug use. For each model, predictors that were not significant at the p ≤ .10 level were then successively removed starting with the predictor with the highest p-value. The Hosmer-Lemeshow test was used to gauge model goodness of fit (Hosmer & Lemeshow, 2000).
Results
Sample Characteristics
Sample characteristics are summarized in Table 1. The 600 parolees reported a mean age of 40 and 11.5 years of education. The sample consisted predominantly of African Americans (46.3%) or Latinos (32.5%); about two thirds were never married; 65.8% reported having children (being parents). At the time of baseline interview, 46.8% spent 90 days or more in an RDT program; a majority (58.8%) were enrolled in a residential multiservice substance care-type program. Many had long histories in the justice system; 49% had spent time in juvenile detention more than half (52.7%) had 20 or more arrests prior to their most recent incarceration; more than one third (about 36.8%) reported having been locked up in local jails 20 times or more prior to their last incarceration; and more than half (54%) had been to state prison at least five times. No baseline differences were found between groups in regard to demographics, situational, personal, or social factors or health and coping factors (Table 1).
Table 1. Demographic, Social, Situational, Coping and Personal Characteristics by Intervention Condition.
| PC-NCM (n = 194) | PC (n = 196) | UC (n = 210) | ||||
|---|---|---|---|---|---|---|
|
|
|
|
||||
| Type/characteristic | M | (SD) | M | (SD) | M | (SD) |
| Demographic | ||||||
| Age | 39.7 | (10.0) | 40.9 | (10.7) | 39.5 | (10.5) |
| Education | 11.4 | (1.6) | 11.5 | (1.7) | 11.5 | (1.5) |
|
|
|
|
||||
| n | (%) | n | (%) | n | (%) | |
|
|
|
|
||||
| Race/ethnicity | ||||||
| African American | 81 | (41.7) | 105 | (53.0) | 92 | (44.2) |
| Latino | 69 | (35.6) | 57 | (26.8) | 69 | (33.2) |
| White | 30 | (15.5) | 29 | (14.7) | 31 | (14.9) |
| Other | 14 | (7.2) | 7 | (3.5) | 16 | (7.7) |
| Marital status | ||||||
| Never married | 129 | (66.5) | 130 | (66.3) | 135 | (64.6) |
| Married | 18 | (9.3) | 26 | (13.3) | 26 | (12.4) |
| SWD | 47 | (24.2) | 40 | (20.4) | 48 | (23.0) |
| Any children (baseline, yes) | 124 | (64.2) | 113 | (57.9) | 135 | (64.3) |
| Financial dependents (6 months, yes)a | 21 | (14.5) | 13 | (8.8) | 24 | (15.0) |
| Situational | ||||||
| Drug treatment | ||||||
| ICDTP-9 | 51 | (26.4) | 54 | (27.8) | 70 | (33.3) |
| RMSC | 120 | (62.2) | 117 | (60.3) | 114 | (54.3) |
| SAP | 22 | (11.4) | 23 | (11.9) | 26 | (12.4) |
| Criminal history at baseline | ||||||
| Juvenile hall (ever held, yes) | 97 | (50.0) | 105 | (53.0) | 92 | (44.2) |
| Arrests (≥ 20; yes) | 105 | (54.1) | 105 | (53.6) | 106 | (50.50 |
| Jails (≥ 20; yes) | 69 | (35.6) | 78 | (39.8) | 74 | (35.2) |
| Prison (≥ 5; yes) | 97 | (50.0) | 116 | (59.2) | 111 | (52.9) |
| Recruitment facility | ||||||
| Prison | 92 | (47.4) | 88 | (44.4) | 89 | (42.8) |
| Jail | 102 | (52.6) | 110 | (55.6) | 119 | (57.2) |
| Incarcerated during followup (yes)b, c | 97 | (58.4) | 100 | (57.1) | 111 | (58.0) |
| Drug arrests (≥ 20 lifetime; yes) | 56 | (28.9) | 64 | (32.7) | 58 | (27.6) |
|
|
|
|
||||
| M | (SD) | M | (SD) | M | (SD) | |
|
|
|
|
||||
| RDT (days)d | 118.9 | (118.7) | 134.8 | (163.8) | 124.9 | (91.4) |
| Incarcerated (days)d | 44.8 | (91.9) | 48.9 | (90.8) | 44.2 | (89.1) |
|
|
|
|
||||
| n | (%) | n | (%) | n | (%) | |
|
|
|
|
||||
| Coping | ||||||
| Planning (high use baseline, yes)e | 78 | (40.2) | 79 | (40.3) | 65 | (31.0) |
|
|
|
|
||||
| M | (SD) | M | (SD) | M | (SD) | |
|
|
|
|
||||
| Disengagement coping (baseline) | 1.8 | (0.9) | 1.8 | (0.8) | 1.9 | (0.9) |
| Self-blame coping (baseline) | 2.6 | (1.0) | 2.5 | (1.0) | 2.6 | (0.9) |
| Self-esteem inventory (total, baseline) | 13.7 | (4.4) | 14.4 | (4.7) | 13.5 | (4.5) |
| Personal | ||||||
| HIV knowledge (risk through sex)f, g | 1.2 | (0.8) | 1.2 | (0.9) | 1.1 | (0.7) |
|
|
|
|
||||
| n | (%) | n | (%) | n | (%) | |
|
|
|
|
||||
| Marijuana (yes)h, i | 80 | (48.2) | 86 | (49.1) | 86 | (45.7) |
| Heroin (yes)h, i | 12 | (7.2) | 22 | (12.6) | 24 | (12.8) |
| Stimulants (yes)h, i | 78 | (47.0) | 80 | (45.7) | 94 | (50.0) |
| Multiple sex partners (yes)h | 87 | (52.4) | 88 | (50.3) | 85 | (45.2) |
Note. All tests of association with treatment assignment were nonsignificant (p < .05). CDTP = In-custody drug treatment program; ICDTP = In Custody Drug Treatment Program; PC = peer coaching; PC-NCM = peer coaching-nursing case management; RDT = residential drug treatment; RMSC = residential multiservice substance care; SAP = substance abuse program; SD = standard deviation; SDW = separated, widowed, divorced; UC = usual care.
n = 453.
Ever, during 12 month followup period.
n = 453 (six months); n = 529 (12 months); see Table 2.
During followup, either or both periods (0-6 months, 6-12 months)
n = 598.
in 6 months.
n = 453.
in 12 months.
n = 529.
Key Outcomes
A total of 453 (75.5%) participants completed the six-month follow-up interviews and 529 (88.1%) completed the 12-month follow-up interviews. The larger sample size at the 12-month follow-up resulted from longer time for tracking and locating the subjects who had gone missing during the six-month follow-up. Three drug use outcomes (marijuana, stimulants, and heroin) and one sexual behavior outcome (multiple sexual partners; defined as having more than two or more sexual partners during a six-month period) were tracked. Results for the entire sample over time and intervention group differences, without considering covariates, are reported in this section.
Drug use
Table 2 summarizes the drug use responses at baseline, six months, and 12 months for the entire sample. Drastic reductions in drug use were noted from baseline (the six-month period prior to their most recent incarceration), and the six and 12 months following program enrollment for marijuana (p < .0001), stimulants (p < .0001), and heroin (p < .0001).
Table 2. Key Outcomes at Three Time Points (Percent Reporting “Yes”).
| Outcome | Baselinea (N = 600) | 6-months (n = 453) | 12-months (n = 529) |
|---|---|---|---|
| Drug use | |||
| Marijuana | 85.7 | 28.3 | 38.6 |
| Stimulantsb | 84.0 | 27.2 | 37.6 |
| Heroin | 36.4 | 6.0 | 8.5 |
| Multiple sex partnersc | 58.5 | 28.5 | 39.9 |
Six months prior to current incarceration.
Category includes crack, cocaine, and any amphetamine-type stimulant.
More than two during the reporting period.
As shown in Figure 1, differences in the number of times participants used each of these drugs, between the groups over time, were not significant. Split-plot ANOVA found no significant time by group interactions on any of the three drug use variables: marijuana (Wilks’ λ = .999, F (4, 764) = .068, p =.992); (2) stimulants (Wilks’ λ = .987, F (4, 890) = 1.498, p = .20); or (3) heroin (Wilks’ λ = .988, F (4, 376) = .558, p = .69). As shown in Figure 1, participants in each of the three intervention conditions were similar on average at the three time points for each of the three drugs, with noted increase in relapse found at the 12-month follow up.
Figure 1.


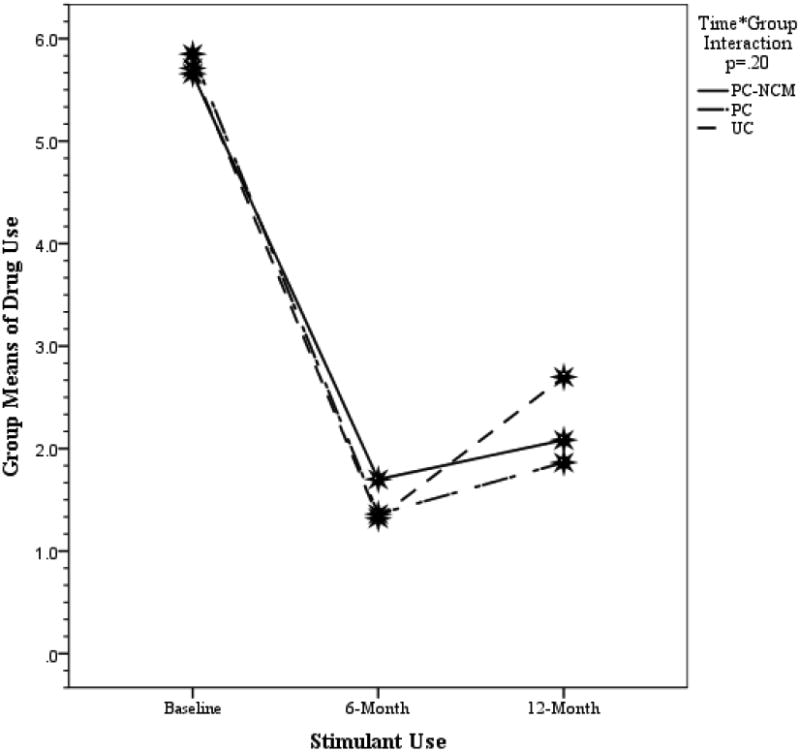

Drug use and multiple sexual partners at baseline, six months, and 12 months by treatment group
Key outcomes over time by intervention group. Group by time interactions were nonsignificant for the three drug use outcomes and the multiple sex partners outcome. (see separate file for figure) (figure will be shown with four panels)
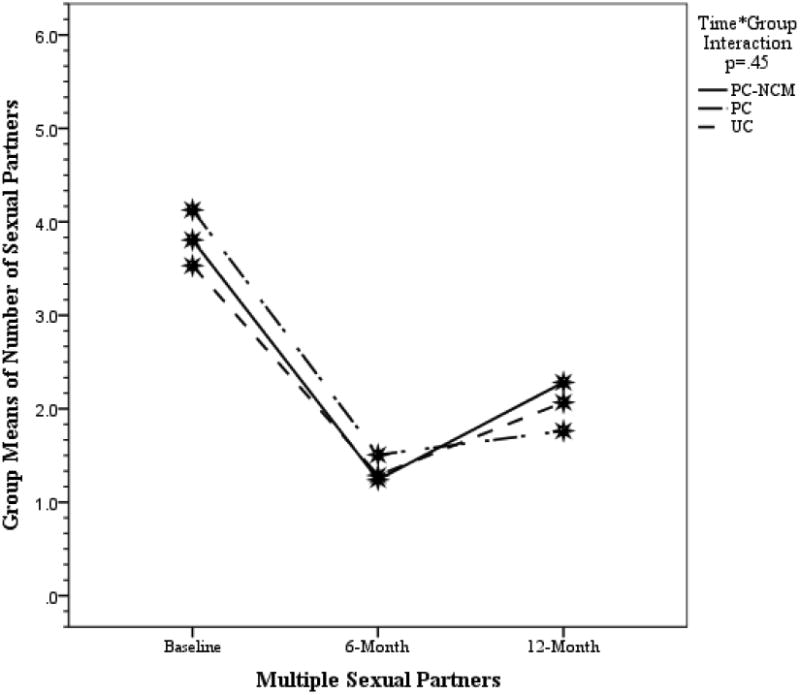
Multiple sex partners
The majority (58.5%) reported having two or more sexual partners at baseline, which decreased to 28.5% during the first six months following the enrollment into the study followed by a rise to 39.9% during the second six-month period (Table 2). Similar to drug use findings (Figure 1), while a drastic reduction in the number of sex partners was found over time (p < .0001), the group-by-time interaction was not significant (Wilks’ λ = .992, F (4, 898) = .923 p = .45). In addition, a noted increase in relapse was shown at 12 months.
Multivariate Logistic Regression
Cessation of drug use
A dichotomous variable was created to identify those who reported having used the three main types of drugs at the baseline but stopped using during the 12-month observation period (i.e., with both six and 12-month follow ups combined). Multivariate logistic regression analyses were conducted to identify factors that were significant in predicting drug cessation. As shown in Table 3, the cessation of illicit drug use was influenced by different variables, depending on the type of drugs. Knowledge that having sex with someone with HIV would likely cause HIV infection at the first six-month follow up was a significant factor only in predicting cessation of marijuana use (p = .01). Having been arrested 20 or more times was a significant predictor (p < .0001) for cessation in heroin use, but not marijuana or stimulant use. Incarceration was associated with cessation of stimulants (p < .0001) and marijuana (p = .001), whereas treatment in a substance abuse-type program was only significant in relation to marijuana use (p = .002). Coping was significant in relation to marijuana (p = .05) and heroin use (p = .02). The number of days spent in an RDT program was a significant predictor of cessation of use of all three drugs. However, intervention intensity (PC-NCM, PC, UC) was not significantly associated with cessation of drug use and was not retained in the final models for drug use cessation.
Table 3. Logistic Regressions: Key Outcomes at 12-Month Follow Up.
| Key outcome/significant predictors | OR | 95% CI | p |
|---|---|---|---|
| Stimulants (n = 465) | |||
| Incarcerated (follow up; yes) | 0.28 | [0.18, 0.44] | <.001 |
| Incarcerated (follow up; days) | 1.00 | [1.00, 1.01] | .02 |
| Marijuana use (follow up; yes) | 0.43 | [0.29, 0.64] | <.001 |
| Heroin use (follow up; yes) | 0.35 | [0.18, 0.70] | .003 |
| Constant | 2.53 | <.001 | |
| Marijuana (n = 396) | |||
| HIV risk knowledge | 0.37 | [0.17, 0.80] | .01 |
| Incarcerated (follow up; yes) | 0.41 | [0.25, 0.69] | .001 |
| SAP treatment (yes) | 2.89 | [1.46, 5.75] | .002 |
| RDT (days) | 1.01 | [1.00, 1.01] | <.00 |
| Stimulants (follow up; yes) | 0.53 | [0.33, 0.85] | .008 |
| Coping (planning high use, baseline; yes) | 0.61 | [0.38, 1.00] | .05 |
| Children (baseline; yes) | 2.04 | [1.27, 3.29] | .003 |
| Constant | 1.73 | .30 | |
| Heroin (n = 525) | |||
| Drug arrests (≥ 20, lifetime; yes) | 2.28 | [1.47, 3.55] | <.001 |
| RDT (days) | 1.00 | [1.00, 1.00] | .005 |
| Coping (disengagement, baseline; yes) | 1.55 | [1.18, 2.04] | .002 |
| Coping (self-blame, baseline; yes) | 0.79 | [0.62, 0.997] | .05 |
| Coping (planning high use, baseline; yes) | 0.58 | [0.37, 0.91] | .02 |
| Self-Esteem Inventory (baseline; total) | 1.10 | [1.04, 1.16] | .001 |
| Constant | 0.06 | <.001 | |
| Multiple sexual partners (n = 324) | |||
| Dependents (six-month follow up; yes) | 2.72 | [1.32, 5.63] | .007 |
| RDT (days) | 1.00 | [1.00, 1.01] | .005 |
| Marijuana use (follow up; yes) | 0.54 | [0.32, 0.92] | .02 |
| Stimulant use (follow up; yes) | 0.58 | [0.35, 0.98] | .04 |
| Constant | 0.44 | .006 |
Note. CI = confidence interval; HIV = human immunodeficiency virus; OR = odds ratio; RDT = residential day treatment; SAP = substance abuse program.
Multiple sexual partners
As shown in Table 3, the number of days spent in an RDT program also affected having multiple sexual partners (p = .005). The longer an ex-offender spent time in RDT, the less likely he was to have had multiple sexual partners. Use of marijuana (p = .02) or stimulants (p = .04) at any point during follow up was associated with a greater likelihood in having multiple sexual partners. Having dependents predicted a cessation of multiple sexual partners (p = .007). Level of study intervention (PC-NCM, PC, UC) did not predict the cessation of having multiple sexual partners.
Discussion
Rearrest remains a serious problem for prisoners released from California prisons; on average, about one third of parolees return to custody within one year and more than two thirds within three years (California Department of Corrections and Rehabilitation, 2014a). Parolees who are homeless, abusing drugs, and engaging in risky sexual behavior are at significant risk for rearrest and a host of health problems. Findings from this study suggest that cessation of drug use and avoidance of multiple sex partners occurs after participation in RDT programs. Although this study found that effects appeared to decline over time as ex-offenders spent time away from the RDT environment, reduction in drug use and multiple sexual partners remained significant when compared to the baseline. The challenge for the corrections field is to identify ways to prolong these beneficial effects as parolees and probationers are reintegrating back into the community in vast numbers.
Intervention condition was not associated with key outcomes. Over time, relapses in marijuana and stimulant use, but not heroin use, as well as returning to multiple sexual partners during the six- to 12-month period were statistically significant; however, reductions in drug use and having sex with multiple partners lessened by the12-month follow up. It is important to note that while we are considering the brief PC and brief nurse counseling as usual care, nurses currently do not play a role in the RDT; thus, nurses may have played a vital role in the study findings even at the most minimal interaction level. Future studies are indeed needed to determine the effect of even a brief nursing presence in the outcomes demonstrated.
While we did find a significant reduction in drug use and having sex with multiple partners, regardless of intensity of PC and NCM, the literature has supported the health benefits of using nurse case management (NCM) and peer coaching (Nyamathi, Hanson, et al., 2012; Nyamathi, Salem, et al., 2012). While our findings did not reveal that intense NCM demonstrated a superior effect on outcome, it may be that the NCM provider was directed more so to health promotion issues rather than reduction of risky behaviors. Drug use and multiple sex partners need to be addressed in future programming. This finding is critical for cost-efficient integration of nurse and PC in current RDT programs.
Further, it is important to note that those who received a SAP contract had a statistically significant likelihood to use marijuana at 12-month follow up. This is an important finding and necessitates future work on targeting marijuana use in SAP programs and reasons for continuing to use marijuana despite having been involved in an SAP program. It is plausible that marijuana is used as a coping mechanism. In one study among 61 marijuana-using young adults, those who had experienced posttraumatic stress disorder (PTSD) symptoms were more likely to use marijuana to regulate psychiatric symptoms (Bujarski et al., 2012). While our study did not particularly focus on PTSD symptoms, postincarceration syndrome may be as stressful as PTSD among those who have experienced long-term incarceration (Liem & Kunst, 2013). Perhaps PCs and RNs need to work together to address specific factors involved in marijuana use, acceptability, receptivity for abstinence, and understanding of use dangers.
A number of predictors were found for cessation of drug use and having multiple sexual factors. While the predictors varied, situational factors, such as number of days in RDT, were a strong, consistent predictor for all three drugs. Promising evidence exists that ex-offenders who spend more time in therapeutic communities and aftercare have reduced rates of rearrest (Hiller, Knight, & Simpson, 1999) and drug use (Inciardi, Martin, & Butzin, 2004).
For stimulants and marijuana, an additional predictor included having been rearrested within the study period. A clear focus by the research staff on the dangers of these popular drugs with rearrest may have led to these findings. It is interesting that use of instrumental coping was related to a decrease in stimulant use. The strong focus of the staff to the strong theoretical tenets of engagement in positive coping strategies and the importance of highlighting problem-focused coping and adjustment is of importance.
While arrests greater than 20 times was a predictor of cessation of heroin use, it is possible that participants were less likely to engage in heroin use because of fear of rearrest and another period of time behind bars. In another study focused on abstinence, lapse or relapse to heroin use among those in RDT, participants who were in the abstinent group were more likely to use more coping styles, such as cognitive, avoidance, or distraction coping, compared to those who used heroin after treatment. These findings support the importance of engaging in coping, regardless of the type of coping style utilized. The authors recommend that RDT facilities should enhance coping skills as part of the relapse prevention program (Gossop, Stewart, Browne, & Marsden, 2002).
Cessation of having sex with multiple partners was predicted by having someone dependent on the participant, days in RDT, and not using marijuana or stimulants during the follow-up period. For at least the first two predictors, we believe our focus on the importance of being a good parent and going through the RDT were helpful strategies. Wolitski (2006) likewise reported significant reduction in unprotected sexual activity by recently released men exposed to an enhanced intervention (68% as compared to a single session program 78%). More investigation is needed to assess the association of use of other drugs on reduction of risky sexual activity. Further, it is important to emphasize that while there was no treatment effect for reduction in drug use and multiple sexual partners at 12 months, a significant reduction was found for reduction of drug use from baseline to 12-month follow up in all subjects.
In addition to nursing presence, we found key factors seemed to be salient in affecting whether the cessation of drug use or avoidance of multiple sex partners would continue. Ongoing work in this area is critical as a focus on reducing erosion of program impact. For example, significant cessation of marijuana use was predicted by knowing the dangers of having sex with someone who was HIV-infected. Further, while having used marijuana predicted having sex with multiple sexual partners, longer time in RDT impacted both reduction of drug use and having sex with multiple partners over time. While it is possible that longer time in treatment may have reduced the likelihood of the participants to engage in sexual activity, participants could have left earlier if they so desired. Previous studies have also found that participants in treatment programs tended to do well while they were in the program, though treatment effects tended to wear off over time (Zhang, Roberts, & Callanan, 2006; Zhang, Roberts, & McCollister, 2011). Further work is needed in the impact of greater time in treatment and the interaction of specialized programs by peer coaches and nurses.
Limitations
It is important to acknowledge limitations of our study. First, this study is limited to homeless ex-offenders in a large, urban city who were residing in one RDT site. Further, self-report data may be affected by misclassification and recall problems and bias. Finally, a true no-treatment protocol was not possible for ethical reasons. Moreover, there were no data collected on type of partner relationship which may have explained the reduction of number of sexual partners.
Conclusion
Systematic research efforts are needed to better understand how interventions can be designed during the re-entry phase to enhance improvement in key outcomes. Policies that focus on developing funding streams and engage the community in a dialogue are essential to create and sustain therapeutic milieus which provide a meshwork of programs and services during the first year of the postrelease period and which help homeless ex-offenders reintegrate into society. Developing culturally relevant and informed care systems for this population are necessary to provide not only drug treatment, but also continued social support. Given these factors and findings from this study, we advocate for concerted policy and federal support for RDT communities which provide needed aid for ex-offenders returning to the community along with a combination of peer coaching and nurse partnered care. These are salient factors that are integral to the long-term success of community re-entry.
Acknowledgments
The authors acknowledge that this study was funded by the National Institute on Drug Abuse (NIDA; 1R01DA27213-01). The trial was registered at clinicaltrials.gov (NCT01844414).
Footnotes
The authors have no conflicts of interest to report.
Contributor Information
Adeline M. Nyamathi, University of California at Los Angeles, School of Nursing.
Sheldon Zhang, San Diego State University.
Sarah Wall, University of California at Los Angeles, School of Nursing.
Elizabeth A. Hall, University of California Los Angeles, Integrated Substance Abuse Programs.
Benissa E. Salem, University of California at Los Angeles, School of Nursing.
David Farabee, University of California Los Angeles, Integrated Substance Abuse Programs.
Mark Faucette, Amity Foundation, Los Angeles, CA.
Kartik Yadav, University of California at Los Angeles, School of Nursing.
References
- Bahr SJ, Harris L, Fisher JK, Harker Armstrong A. Successful reentry: What differentiates successful and unsuccessful parolees? International Journal of Offender Therapy & Comparative Criminology. 2010;54:667–692. doi: 10.1177/0306624×09342435. [DOI] [PubMed] [Google Scholar]
- Bujarski SJ, Feldner MT, Lewis SF, Babson KA, Trainor CD, Leen-Feldner E, et al. Bonn-Miller MO. Marijuana use among traumatic event-exposed adolescents: Posttraumatic stress symptom frequency predicts coping motivations for use. Addictive Behavior. 2012;37:53–59. doi: 10.1016/j.addbeh.2011.08.009. [DOI] [PubMed] [Google Scholar]
- California Department of Corrections and Rehabilitation. Parolee information handbook. 2013a:28. Retrieved from http://www.cdcr.ca.gov/Parole/Parolee_Handbook/pg28.html.
- California Department of Corrections and Rehabilitation. Realignment report: A one-year examination of offenders released from state prison in the first six months of public safety realignment. 2013b Retrieved from http://www.cdcr.ca.gov/realignment/docs/Realignment%206%20Month%20Report%20Final_5%2016%2013%20v1.pdf.
- California Department of Corrections and Rehabilitation. 2013 outcome evaluation report. 2014a Retrieved from http://www.cdcr.ca.gov/Adult_Research_Branch/Research_documents/Outcome_evaluation_Report_2013.pdf.
- California Department of Corrections and Rehabilitation. Weekly report of population as of midnight. 2014b Retrieved from http://www.cdcr.ca.gov/Reports_Research/Offender_Information_Services_Branch/WeeklyWed/TPOP1A/TPOP1Ad140611.pdf.
- California Department of Corrections and Rehabilitation. Recidivism Reduction Program Inventory. 2007 http://ucicorrections.seweb.uci.edu/files/2013/06/CDCR-Recidivism-Reduction-Program-Inventory.pdf.
- Carson EA. Prisoners in 2013. US Department of Justice, Office of Justice Statistics, Bureau of Justice Statistics. 2014 Sep; NCJ Report 247282. Retrieved from http://www.bjs.gov/content/pub/pdf/p13.pdf.
- Carver CS. You want to measure coping but your protocol's too long: Consider the brief COPE. International Journal of Behavioral Medicine. 1997;4:92–100. doi: 10.1207/s15327558ijbm0401_6. [DOI] [PubMed] [Google Scholar]
- Coopersmith S. The antecedents of self-esteem. San Francisco, CA: W. H. Freeman; 1967. [Google Scholar]
- Donnellan MB, Trzesniewski KH, Robins RW, Moffitt TE, Caspi A. Low self-esteem is related to aggression, antisocial behavior, and delinquency. Psychological Science. 2005;16:328–335. doi: 10.1111/j.0956-7976.2005.01535.x. [DOI] [PubMed] [Google Scholar]
- Evans E, Jaffe A, Urada D, Anglin MD. Differential outcomes of court-supervised substance abuse treatment among California parolees and probationers. International Journal of Offender Therapy & Comparative Criminology. 2012;56:539–556. doi: 10.1177/0306624×11404827. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Federal Bureau of Prisons. Offenses. 2014 Retrieved from http://www.bop.gov/about/statistics/statistics_inmate_offenses.jsp.
- Fenton KA. Changing epidemiology of HIV/AIDS in the United States: Implications for enhancing and promoting HIV testing strategies. Clinical Infectious Diseases. 2007;45:S213–S220. doi: 10.1086/522615. [DOI] [PubMed] [Google Scholar]
- Feucht TE, Gfroerer J. Data review: Mental and substance use disorders among adult men on probation or parole: Some success against a persistent challenge. SAMHSA: National Institute of Justice; 2011. Retrieved from http://www.samhsa.gov/data/2k11/MentalDisorders/MentalDisorders.pdf. [Google Scholar]
- Fickenscher A, Lapidus J, Silk-Walker P, Becker T. Women behind bars: Health needs of inmates in a county jail. Public Health Reports. 2001;116:191–196. doi: 10.1093/phr/116.3.191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gossop M, Stewart D, Browne N, Marsden J. Factors associated with abstinence, lapse or relapse to heroin use after residential treatment: Protective effect of coping responses. Addiction. 2002;97:1259–1267. doi: 10.1046/j.1360-0443.2002.00227.x. [DOI] [PubMed] [Google Scholar]
- Grinstead OA, Faigeles B, Comfort M, Seal D, Nealey-Moore J, Belcher L, Morrow K. HIV, STD, and hepatitis risk to primary female partners of men being released from prison. Women & Health. 2005;41:63–80. doi: 10.1300/J013v41n02_05. [DOI] [PubMed] [Google Scholar]
- Hennessey KA, Kim AA, Griffin V, Collins NT, Weinbaum CM, Sabin K. Prevalence of infection with hepatitis B and C viruses and co-infection with HIV in three jails: A case for viral hepatitis prevention in jails in the United States. Journal of Urban Health. 2009;86:93–105. doi: 10.1007/s11524-008-9305-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hiller ML, Knight K, Simpson DD. Prison-based substance abuse treatment, residential aftercare and recidivism. Addiction. 1999;94:833–842. doi: 10.1046/j.1360-0443.1999.9468337.x. [DOI] [PubMed] [Google Scholar]
- Hosmer DW, Lemeshow S. Applied logistic regression. 2nd. New York, NY: Wiley; 2000. [Google Scholar]
- Human Rights Watch. Mental illness, human rights, and US prisons: Human rights watch statement for the record to the senate judiciary committee subcommittee on human rights and the law. 2009 Retrieved from http://www.hrw.org/news/2009/09/22/mental-illness-human-rights-and-us-prisons.
- Inciardi JA, Martin SS, Butzin CA. Five-year outcomes of therapeutic community treatment of drug-involved offenders after release from prison. Crime & Delinquency. 2004;50:88–107. doi: 10.1177/0011128703258874. [DOI] [Google Scholar]
- James DJ, Glaze LE. Mental health problems of prison and jail inmates. Washington, D.C.: U.S. Department of Justice, Bureau of Justice Statistics; 2006. [Google Scholar]
- Kushel MB, Hahn JA, Evans JL, Bangsberg DR, Moss AR. Revolving doors: Imprisonment among the homeless and marginally housed population. American Journal of Public Health. 2005;95:1747–1752. doi: 10.2105/AJPH.2005.065094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lazarus R, Folkman S. Stress, appraisal and coping. New York, NY: Springer; 1984. [Google Scholar]
- Lejuez CW, Simmons BL, Aklin WM, Daughters SB, Dvir S. Risk-taking propensity and risky sexual behavior of individuals in residential substance use treatment. Addictive Behaviors. 2004;29:1643–1647. doi: 10.1016/j.addbeh.2004.02.035. [DOI] [PubMed] [Google Scholar]
- Liem M, Kunst M. Is there a recognizable post-incarceration syndrome among released “lifers”? International Journal of Law and Psychiatry. 2013;36:333–337. doi: 10.1016/j.ijlp.2013.04.012. [DOI] [PubMed] [Google Scholar]
- Lim S, Seligson AL, Parvez FM, Luther CW, Mavinkurve MP, Binswanger IA, Kerker BD. Risks of drug-related death, suicide, and homicide during the immediate post-release period among people released from New York City jails, 2001-2005. American Journal of Epidemiology. 2012;175:519–526. doi: 10.1093/aje/kwr327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lurigio AJ, Cho YI, Swartz JA, Johnson TP, Graf I, Pickup L. Standardized assessment of substance-related, other psychiatric, and comorbid disorders among probationers. International Journal of Offender Therapy and Comparative Criminology. 2003;47:630–652. doi: 10.1177/0306624×03257710. [DOI] [PubMed] [Google Scholar]
- MacGowan RJ, Margolis A, Gaiter J, Morrow K, Zack B, Askew J, et al. Eldridge GD. Predictors of risky sex of young men after release from prison. International Journal of STDs & AIDS. 2003;14:519–523. doi: 10.1258/095646203767869110. [DOI] [PubMed] [Google Scholar]
- Marlow E, Nyamathi A, Grajeda WT, Bailey N, Weber A, Younger J. Nonviolent communication training and empathy in male parolees. Journal of Correctional Health Care. 2012;18:8–19. doi: 10.1177/1078345811420979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morgan BD, Rossi AP. Difficult-to-manage HIV/AIDS clients with psychiatric illness and substance abuse problems: A collaborative practice with psychiatric advanced practice nurses. Journal of the Association of Nurses in AIDS Care. 2007;18:77–84. doi: 10.1016/j.jana.2007.06.001. [DOI] [PubMed] [Google Scholar]
- Mumola CJ, Karberg JC. Bureau of Justice Statistics Special Report: Drug use and dependence, state and federal prisoners, 2004. US Department of Justice. 2006 Retrieved from http://purl.access.gpo.gov/GPO/LPS85621.
- Narevic E, Garrity TF, Schoenberg NE, Hiller ML, Webster JM, Leukefeld CG, Tindall MS. Factors predicting unmet health services needs among incarcerated substance users. Substance Use & Misuse. 2006;41:1077–1094. doi: 10.1080/10826080600692167. [DOI] [PubMed] [Google Scholar]
- Nyamathi A. Comprehensive health seeking and coping paradigm. Journal of Advanced Nursing. 1989;14:281–290. doi: 10.1111/j.1365-2648.1989.tb03415.x. [DOI] [PubMed] [Google Scholar]
- Nyamathi A, Flaskerud J, Leake B. HIV-risk behaviors and mental health characteristics among homeless or drug-recovering women and their closest sources of social support. Nursing Research. 1997;46:133–137. doi: 10.1097/00006199-199705000-00003. [DOI] [PubMed] [Google Scholar]
- Nyamathi A, Hanson AY, Salem BE, Sinha S, Ganguly KK, Leake B, et al. Marfisee M. Impact of a rural village women (ASHA) intervention on adherence to antiretroviral therapy in southern India. Nursing Research. 2012;61:353–362. doi: 10.1097/NNR.0b013e31825fe3ef. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nyamathi A, Leake B, Albarran C, Zhang S, Hall E, Farabee D, et al. Faucette M. Correlates of depressive symptoms among homeless men on parole. Issues in Mental Health Nursing. 2011;32:501–511. doi: 10.3109/01612840.2011.569111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nyamathi A, Marfisee M, Khalilifard F, Leake B, Marlow E, Zhang S, et al. Faucette M. Correlates of serious violent crime for recently released parolees with a history of homelessness. Violence and Victims. 2012;27:793–810. doi: 10.1891/0886-6708.27.5.793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nyamathi AM, Marlow E, Branson C, Marfisee M, Nandy K. Hepatitis A/B vaccine completion among homeless adults with history of incarceration. Journal of Forensic Nursing. 2012;8:13–22. doi: 10.1111/j.1939-3938.2011.01123.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nyamathi A, Salem B, Marshall L, Idemundia F, Mata R, Khalilifard F, et al. Leake B. Substance use trends among younger vs. older homeless parolees. Journal of Addictive Diseases. 2014;33:124–133. doi: 10.1080/10550887.2014.909694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nyamathi A, Salem BE, Farabee D, Hall E, Zhang S, Faucette M, et al. Yadav K. Impact of an intervention for recently released homeless offenders on self-reported rearrest at six and 12 months. Manuscript submitted for publication. 2015 doi: 10.1080/10550887.2016.1147796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nyamathi A, Salem BE, Zhang S, Farabee D, Hall B, Khalilifard F, Leake B. Nursing case management, peer coaching, and hepatitis A and B vaccine completion among homeless men recently released on parole: Randomized clinical trial. Nursing Research. 2015;64:177–189. doi: 10.1097/nnr.0000000000000083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nyamathi A, Salem BE, Meyer V, Ganguly KK, Sinha S, Ramakrishnan P. Impact of an ASHA intervention on depressive symptoms among rural women living with AIDS in India: Comparison of the ASHA life and usual care program. AIDS Education & Prevention. 2012;24:280–293. doi: 10.1521/aeap.2012.24.3.280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nyamathi A, Slagle A, Thomas A, Hudson A, Kahilifard F, Avila G, et al. Cuchilla M. Art messaging to engage homeless young adults. Progress in Community Health Partnerships. 2011;5:9–18. doi: 10.1353/cpr.2011.0012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prendergast ML. Interventions to promote successful re-entry among drug-abusing parolees. Addiction Science & Clinical Practice. 2009;5:4–13. doi: 10.1151/ascp09514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rubenstein LV, Calkins DR, Young RT, Cleary PD, Fink A, Kosecoff J, et al. Brook RH. Improving patient function: A randomized trial of functional disability screening. Annals of Internal Medicine. 1989;111:836–842. doi: 10.7326/0003-4819-111-10-836. [DOI] [PubMed] [Google Scholar]
- Salem BE, Nyamathi A, Idemundia F, Slaughter R, Ames M. At a crossroads: Reentry challenges and healthcare needs among homeless female ex-offenders. Journal of Forensic Nursing. 2013;9:14–22. doi: 10.1097/JFN.0b013e31827a1e9d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schlotfeldt R. Nursing in the future. Nursing Outlook. 1981;29:295–301. [PubMed] [Google Scholar]
- Seal DW, Margolis AD, Sosman J, Kacanek D, Binson D. HIV and STD risk behavior among 18- to 25-year-old men released from U.S. prisons: Provider perspectives. AIDS & Behavior. 2003;7:131–141. doi: 10.1023/A:1023942223913. [DOI] [PubMed] [Google Scholar]
- Shanahan CW, Beers D, Alford DP, Brigandi E, Samet JH. A transitional opioid program to engage hospitalized drug users. Journal of General Internal Medicine. 2010;25:803–808. doi: 10.1007/s11606-010-1311-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sherbourne CD, Stewart AL. The MOS social support survey. Social Science & Medicine. 1991;32:705–714. doi: 10.1016/0277-9536(91)90150-B. [DOI] [PubMed] [Google Scholar]
- Simpson D, Chatham L. TCU/DATAR forms manual. Ft. Worth, TX: Institute of Behavioral Research, Texas Christian University; 1995. [Google Scholar]
- Simpson D, Knight K. TCU data collection forms for correctional residential treatment. Ft. Worth, TX: Texas Christian University, Institute of Behavioral Research; 1998. [Google Scholar]
- Staton M, Leukefeld C, Webster JM. Substance use, health, and mental health: problems and service utilization among incarcerated women. International Journal of Offender Therapy and Comparative Criminology. 2003;47:224–239. doi: 10.1177/0306624×03251120. [DOI] [PubMed] [Google Scholar]
- Stewart AL, Hays RD, Ware JE., Jr The MOS short-form general health survey: Reliability and validity in a patient population. Medical Care. 1988;26:724–735. doi: 10.1097/00005650-198807000-00007. [DOI] [PubMed] [Google Scholar]
- Sung HE, Mahoney AM, Mellow J. Substance abuse treatment gap among adult parolees: Prevalence, correlates, and barriers. Criminal Justice Review. 2011;36:40–57. doi: 10.1177/0734016810389808. [DOI] [Google Scholar]
- Wilper AP, Woolhandler S, Boyd JW, Lasser KE, McCormick D, Bor DH, Himmelstein DU. The health and health care of US prisoners: Results of a nationwide survey. American Journal of Public Health. 2009;99:666–672. doi: 10.2105/AJPH.2008.144279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolitski RJ. Relative efficacy of a multisession sexual risk-reduction intervention for young men released from prisons in 4 states. American Journal of Public Health. 2006;96:1854–1861. doi: 10.2105/ajph.2004.056044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization. Hepatitis A (Fact sheet No 328) 2015 Retrieved from http://www.who.int/mediacentre/factsheets/fs328/en/
- Zhang SX, Roberts REL, Callanan VJ. Preventing parolees from returning to prison through community-based reintegration. Crime & Delinquency. 2006;52:551–571. doi: 10.1177/0011128705282594. [DOI] [Google Scholar]
- Zhang SX, Roberts REL, McCollister KE. Therapeutic community in a California prison: Treatment outcomes after five years. Crime & Delinquency. 2011;57:82–101. doi: 10.1177/0011128708327035. [DOI] [Google Scholar]
- Zhang Z. Drug and alcohol use and related matters among arrestees. Rockville, MD: National Institute of Justice; 2003. https://www.ncjrs.gov/nij/adam/ADAM2003.pdf. [Google Scholar]