

Abstract
Background The expectation for graduate medical education programs to ensure that trainees are progressing toward competence for unsupervised practice prompted requirements for a committee to make decisions regarding residents' progress, termed a clinical competency committee (CCC). The literature on the composition of these committees and how they share information and render decisions can inform the work of CCCs by highlighting vulnerabilities and best practices.
Objective We conducted a narrative review of the literature on group decision making that can help characterize the work of CCCs, including how they are populated and how they use information.
Methods English language studies of group decision making in medical education, psychology, and organizational behavior were used.
Results The results highlighted 2 major themes. Group member composition showcased the value placed on the complementarity of members' experience and lessons they had learned about performance review through their teaching and committee work. Group processes revealed strengths and limitations in groups' understanding of their work, leader role, and information-sharing procedures. Time pressure was a threat to the quality of group work.
Conclusions Implications of the findings include the risks for committees that arise with homogeneous membership, limitations to available resident performance information, and processes that arise through experience rather than deriving from a well-articulated purpose of their work. Recommendations are presented to maximize the effectiveness of CCC processes, including their membership and access to, and interpretation of, information to yield evidence-based, well-reasoned judgments.
Introduction
Group decision making related to assessment of trainees is now a standard mechanism for graduate medical education programs to assume accountability for graduates' competence for practice. In the context of competency-based education,1 methods to assess and document trainee competence and identify performance problems are essential. The Accreditation Council for Graduate Medical Education (ACGME) expects programs to regularly report on resident performance on competencies using milestones.2 Using a combination of assessment data gathered from multiple sources, clinical competency committees (CCCs) review performance information to evaluate learners' progress on milestones and assess their competence and development toward readiness for unsupervised practice.3 However, programs face challenges in group procedures to synthesize assessment data into decisions about individual trainee performance on the educational milestones.
Groups can reach better decisions than individuals.4 Group decision making entails individuals coming together and processing information to reach a collective decision.5 Ideally, individuals sharing information results in better decisions than decisions made by an individual. This is 1 rationale for the requirement for CCCs. In undergraduate medical education, group evaluation of student performance improves alignment of narrative comments with clerkship grades6 and yields better characterization of changes in learner performance over time.7 Group discussion also increases detection of students' and residents' problematic performance and patterns of performance.8–12 However, a recent study of their early experience shows that CCCs vary in their procedures and understanding of purpose.3
The purpose of this review is to synthesize the literature on groups to extract key concepts relevant to how CCCs can best conduct their work, including how groups interact and use information to make judgments, how these interactions may influence outcomes, and how current processes align with best practices. The findings are intended to provide medical educators with information to optimize their CCC composition and process.
Methods
A diverse team of authors, including program directors, education researchers, and institutional leaders, conducted a narrative review of the literature on group decision making and qualitatively synthesized the findings from a large body of literature.13 This nonsystematic search of the English language literature focused on studies of group decision making in medical education, psychology, and organizational behavior contexts. To take advantage of the breadth and boundaries of interpretations, we included literature from across different education and occupational fields. One author (K.E.H.) searched the MEDLINE, PsycINFO, Google Scholar, and Web of Science databases through 2015, using terms related to group decision making, organizations, group dynamics, committee membership, and clinical competence. Authors manually searched bibliographies of relevant articles. Co-authors reviewed the findings and iteratively suggested additional relevant articles.
The entire team of authors identified key points in this literature related to group participants and processes that influence outcomes. The final products are the themes presented in this review.
Results
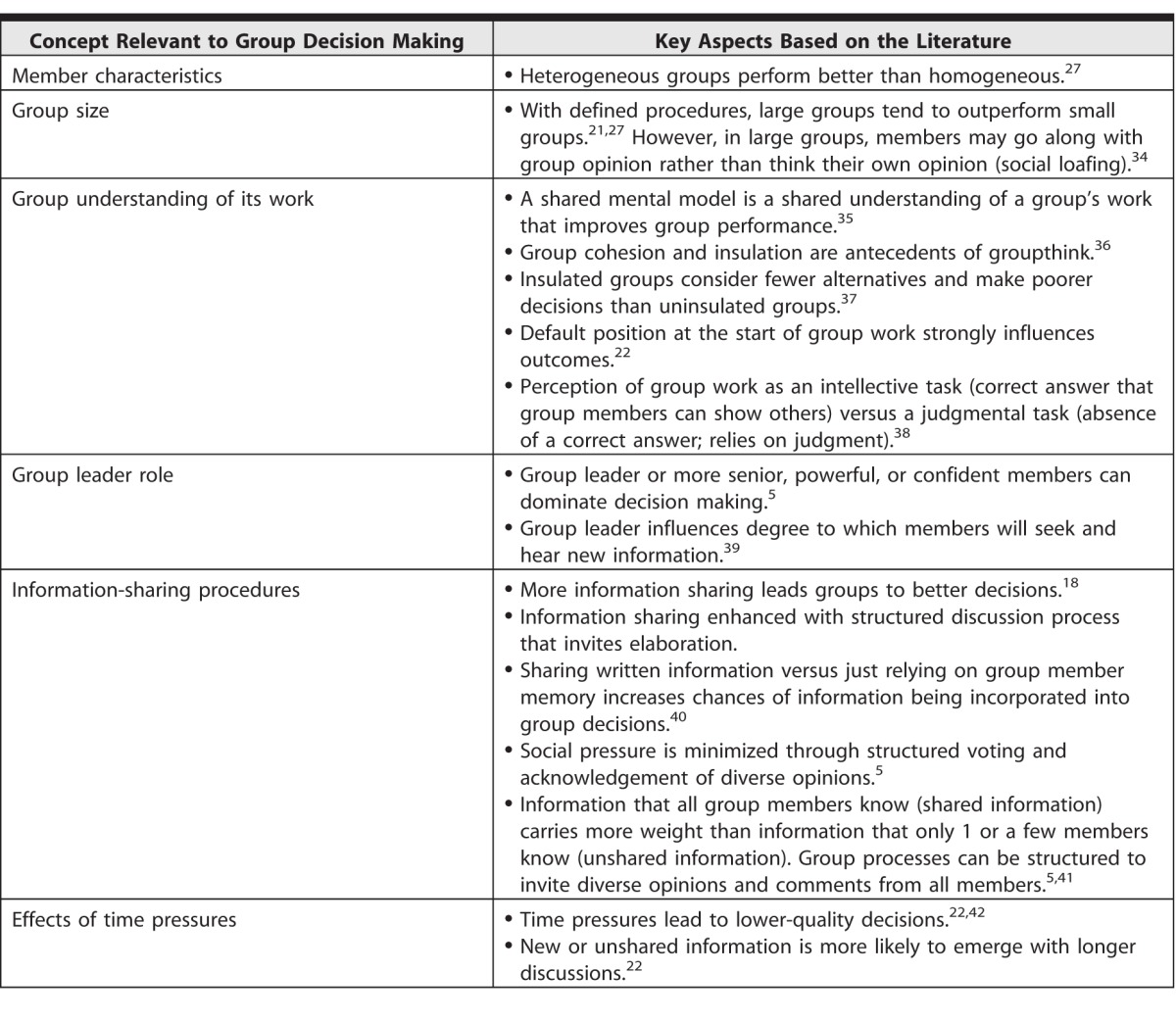
The results of our review highlight aspects of group decision making relevant to CCCs, such as social decision scheme theory, group composition, member characteristics, group size, group understanding of its work, group process (eg, information sharing procedures), time pressures, and the concept of “groupthink” (table 1).
table 1 .
Group Decision Making: Aspects of Groups That Influence Their Outcomes
Social Decision Scheme Theory
Social decision scheme (SDS) theory describes the processes by which groups move from individual preferences toward group decisions.14–16 The rules or procedures used constitute the social decision scheme; these procedures may be explicitly stated or be developed by the group as it does its work.17 SDS theory highlights the importance of distinguishing shared versus unshared information to understand group deliberations.18 Shared information is held among multiple members, whereas unshared information is known solely by 1 or a few members. SDS theory postulates that more information sharing leads to better decisions.19 However, groups tend to use information that many members already know, whereas the group benefits more from the amount of unique or distinct information known only to 1 or a few group members, which, once shared, increases the group's collective knowledge. Unique information is more likely to emerge when group discussions are highly structured. Research on SDS theory has led to recommendations to optimize information sharing, described below.20
Group Composition and Size
Group composition, which includes member attributes and group size, influences outcomes. Member characteristics determine the range of opinions present at the outset of a meeting; these preferences are major determinants of the opinions at the end of a deliberation.18,21–23 Input from members whose characteristics situate them outside the mainstream group in terms of position and/or knowledge can improve group functioning through consideration of more alternatives.20,24 “Minority dissent” describes the way that members who share divergent opinions increase the number of perspectives considered by other group members.20 However, divergent members may find it difficult to influence the group's opinions due to individuals' tendency toward conforming with the group.25 Newcomers tend to contribute more unique opinions than longstanding members, and their opinions may be more readily accepted by the group when those new members are afforded permanent rather than temporary membership.26 Member diversity, coupled with explicit group procedures to engage new and diverse views and opinions, will maximize new members' contributions and value to the group.
The literature supports the benefits of larger committees.15,27 In the 18th century, Condorcet's Jury Theorem illustrated mathematically how larger groups make better decisions than smaller ones.28 Size, however, must be weighed against the quality of membership.29 As groups become larger, members added last may contribute less substantively than initially selected members, particularly if they possess fewer qualifications, less motivation, or less required training. Because groups larger than 4 members can develop subgroups,30 training and articulated procedures are needed to avoid subdivisions and side conversations, and ensure subgroups are designated with particular charges. Commonly cited recommendations for ideal group size are 5 to 10 members.31–33
Group Processes
Effective groups share a common understanding of their work. A shared mental model is group members' collective knowledge that enables them to interpret information consistently, explain findings, and determine actions appropriately for their charge. Shared mental models encompass understanding of the task to be done and the collaboration and teamwork needed to accomplish it.35 Without a shared mental model, variations in participants' knowledge, communication, and attitudes can impede performance.43
Groups also need a shared understanding of how decisions are made, developed explicitly through articulation of procedures or implicitly through experience. Performance review decisions can be defined as judgmental or intellective. A judgmental approach requires group members, or the leader, to use their own opinions to generate decisions.44 In contrast, intellective decisions entail the use of defined expectations and structures for information sharing to foster decisions that have an evidence-based “correct” answer. These 2 forms of task understanding are not mutually exclusive. The ideal may be a combination of intellective analysis that is informed by high-quality, diverse performance data and members reviewing and interpreting data to generate a group judgment supported by evidence.38
How group leaders carry out their role can have a powerful and multifaceted effect on decision making. Leaders can shape members' understanding of their task and the need to share information to achieve optimal outcomes.45 A hierarchy with a dominant, charismatic, or autocratic leader can stifle information sharing and the introduction of new information and favor conformity.22,39,46 In contrast, a leader inviting participation counteracts the tendency for members lower on the hierarchy to be passive.
Information Sharing Procedures
Given previous research findings that greater information sharing among all group members improves decision making,5 strategies are needed to facilitate information sharing. These strategies also can address decision biases attributable to shared information (the tendency for groups to prioritize information known to more group members) and preference (the tendency for members to adhere to initial preferences).41,47 Systems to share information from multiple sources to ensure everyone has the same information can improve decision quality.48 Sharing information in a standardized way, structured similarly, enhances members' ability to incorporate and use the information. Groups who know the distribution of knowledge among their members are especially likely to elaborate on and use that information.49 Sharing information through an information system, rather than solely through the group's conversation, enhances the quantity and quality of information shared.50 When groups frame their work at least partially as an intellective task grounded in the evidence, this enhances members' openness to diverse opinions and can improve decision making.51
Time Pressures
Time pressures, common for groups, influence multiple aspects of group decision making. Time pressures constrain the amount of information sharing and change the nature of information sharing. Time constraints increase the amount of commentary related to the task at hand and decrease the focus on attention to social “niceties.”52 Time-pressured groups tend to exhibit greater cooperation and convergence in their decision making, with less incorporation of divergent views, enhancing the possibility of suboptimal decisions.53 Time pressures also exacerbate the risk of leaders or dominant members disproportionately influencing outcomes.54
Groupthink
Despite its potential benefits, group decision making can introduce biases. These can be counteracted with careful planning. Groupthink, first described by the psychologist Irving Janis,39 epitomizes bias as a vulnerability to logical thinking for groups. It describes the thinking individuals engage in to maintain harmony within a group, to the point of overriding realistic appraisals of courses of action.39,55 Group leaders play an important role by either welcoming new information and diverse opinions or promoting conformity to a preset norm.56 Groups may defer to powerful members,54 and individuals may feel pressure to be aligned with the group. Observations of conformity in health care and medical education should prompt further caution regarding physicians' potential to think or behave similarly to peers or superiors.42 While a prosocial orientation is beneficial to a group because members consequently aspire to deliberations and decisions that benefit the group rather than just the self, it must be tempered by an understanding of the risks of groupthink and excessive conformity.46 Groups with high cohesion are more likely to justify and adhere to their decisions, right or wrong, rather than remaining open to alternatives.57
Training can minimize biases for groups making decisions.47 Well-designed instructional strategies and clearly presented information can promote the use of a shared mental model to enhance group performance.58,59 For example, groups can learn, practice with, and be reminded of definitions, examples, and prior decisions. However, with time pressures or high workload, groups may resort to making decisions based on shared information and may fail to incorporate all information into a more thoughtful decision.
Discussion
This review summarizes insights about group decision making from fields beyond medical education. Group outcomes depend in large part on the information and preferences held by members and the procedures that guide members to understand and conduct their work. Member characteristics can enhance diversity and representativeness of information available in the performance review process. While the ACGME views CCCs as advisory and affords final responsibility for decisions about resident advancement to the program director,60 strategies for balancing information sharing among a committee chair and members increase the quality of the product, which ultimately is a forward-looking judgment about the committee's trust in trainee progress and, ultimately, readiness for unsupervised practice.61 The information from this narrative literature review resulted in the recommendations for CCC processes shown in table 2, and is summarized below.
table 2 .
Recommendations for Clinical Competency Committees Based on Study Findings and Literature on Group Decision Making

Our review suggests that strategies to populate CCCs with diverse members and solicit all group members' input can capitalize on the range of perspectives present in order to maximize group effectiveness. For CCCs, diverse perspectives could come from faculty teachers whose primary roles are in ambulatory or outlying settings, research, or administration, or from interprofessional members. CCCs for small programs have limited options to achieve larger committee size, but may use creative strategies to add new members, particularly junior faculty. Hierarchy may stifle junior members' participation, but strategies such as inviting junior members to speak first or expecting all members to contribute may counteract this risk. Where member diversity is not possible within the faculty, committees can seek diverse information from other educators, clinical faculty, or interprofessional colleagues to expand the available information. Framing the work of a CCC as a task grounded in evidence about trainee progress will improve decision making.52
Groups benefit from training to develop a shared understanding of the purpose of their work. For CCCs, a common understanding of resident performance using the milestones can be strengthened through frame of reference training to build shared models of what performance should look like at each level.68
The literature suggests that, over time, members are likely to develop implicit shared understandings and make decisions accordingly without being able to articulate how this process occurred.36 Group cohesiveness and long experience working together build confidence among group members that they are doing good work.36,39 However, groups high in cohesiveness and confidence can suppress opposing views in favor of group unanimity. In the case of CCCs, the confidence that the group will accurately interpret resident performance because of past experience with other residents may not be fully justified, if decisions were not based on criteria, such as the milestones, or based on optimal group procedure. CCCs may benefit from procedures to guard against groupthink.
Structured procedures to share information among everyone in the group (to ensure that everyone has the same, complete picture of a resident performance) are needed to maximize the amount of shared information. CCCs may fall short of this ideal, due to variation in who attends meetings and what they choose to share.69 This highlights the need for CCCs to have structured processes for information sharing, such as ways to disseminate written performance information among members, consistent approaches for gathering members' interpretation of the information, and methods to reconcile disparate information. Finally, for CCCs to conduct their work efficiently within inherent time constraints, strategies to simplify a decision making task, such as focusing the group on the most relevant information, can enhance the quality of decisions.23 CCCs should weigh the goals of greater information sharing, collaboration, and efficiency to optimize their outcomes.
This review has limitations. We did not conduct a systematic review, and relevant literature may have been excluded. Implications for CCCs must be considered in the context of the relatively new mandate for graduate medical educators to review resident performance within committees, and these groups are likely continuing to evolve and mature. Further study of CCCs could examine their work through direct observation of their members' characteristics and information sharing, as well as the leader role, and attempt to compare this with the quality of judgments made about residents' performance.
Conclusion
We reviewed the literature on group decision making to examine the strengths and potential vulnerabilities that CCCs face in determining residents' competence to advance toward unsupervised practice. Group members' commitment and experience, while highly valued, must be viewed cautiously and balanced with the benefits of novel perspectives. The limitations of group cohesion can be acknowledged, allowing groups to seek opportunities for new ways of reviewing information and making judgments about residents. Ongoing faculty development and refinement of understanding of the purpose of resident performance review using the milestones are needed to ensure that CCC members share a unified understanding of the purpose of their work for ensuring high-quality, safe patient care.
References
- 1. Frank JR, Snell LS, ten Cate O, Homboe ES, Carraccio C, Swing SR, et al. Competency-based medical education: theory to practice. Med Teach. 2010; 32 8: 638– 645. [DOI] [PubMed] [Google Scholar]
- 2. Nasca TJ, Philibert I, Brigham T, Flynn TC. The next GME accreditation system—rationale and benefits. N Engl J Med. 2012; 366 11: 1051– 1056. [DOI] [PubMed] [Google Scholar]
- 3. Hauer KE, Chesluk B, Iobst W, Holmboe E, Baron RB, Robert B, et al. Reviewing residents' competence: a qualitative study of the role of clinical competency committees in performance assessment. Acad Med. 2015; 90 8: 1084– 1092. [DOI] [PubMed] [Google Scholar]
- 4. Michaelsen LK, Watson WE, Black RH. A realistic test of individual versus group consensus decision making. J Appl Psychol. 1989; 74 5: 834– 839. [Google Scholar]
- 5. Kerr NL, Tindale RS. Group performance and decision making. Annu Rev Psychol. 2004; 55: 623– 655. [DOI] [PubMed] [Google Scholar]
- 6. Albritton TA, Fincher RM, Work JA. Group evaluation of student performance in a clerkship. Acad Med. 1996; 71 5: 551– 552. [DOI] [PubMed] [Google Scholar]
- 7. Battistone MJ, Milne C, Sande MA, Pangaro LN, Hemmer PA, Shomaker TS. The feasibility and acceptability of implementing formal evaluation sessions and using descriptive vocabulary to assess student performance on a clinical clerkship. Teach Learn Med. 2002; 14 1: 5– 10. [DOI] [PubMed] [Google Scholar]
- 8. Hauer KE, Mazotti L, O'Brien B, Hemmer PA, Tong L. Faculty verbal evaluations reveal strategies used to promote medical student performance. Med Educ Online. 2011; 16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Hemmer PA, Hawkins R, Jackson JL, Pangaro LN. Assessing how well three evaluation methods detect deficiencies in medical students' professionalism in two settings of an internal medicine clerkship. Acad Med. 2000; 75 2: 167– 173. [DOI] [PubMed] [Google Scholar]
- 10. Hemmer PA, Pangaro L. The effectiveness of formal evaluation sessions during clinical clerkships in better identifying students with marginal funds of knowledge. Acad Med. 1997; 72 7: 641– 643. [DOI] [PubMed] [Google Scholar]
- 11. Thomas MR, Beckman TJ, Mauck KF, Cha SS, Thomas KG. Group assessments of resident physicians improve reliability and decrease halo error. J Gen Intern Med. 2011; 26 7: 759– 764. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Schwind CJ, Williams RG, Boehler ML, Dunnington GL. Do individual attendings' post-rotation performance ratings detect residents' clinical performance deficiencies? Acad Med. 2004; 79 5: 453– 457. [DOI] [PubMed] [Google Scholar]
- 13. McGaghie WC. Varieties of integrative scholarship: why rules of evidence, criteria, and standards matter. Acad Med. 2015; 90 3: 294– 302. [DOI] [PubMed] [Google Scholar]
- 14. Davis JH. Group decision and social interaction: a theory of social decision schemes. Psychol Rev. 1973; 80 4: 302. [Google Scholar]
- 15. Stasser G. A primer of social decision scheme theory: models of group influence, competitive model-testing, and prospective modeling. Organ Behav Hum Decis Process. 1999; 80 1: 3– 20. [DOI] [PubMed] [Google Scholar]
- 16. Ven de Ven A, Delbeco AL. Nominal versus interacting group processes for committee decision-making effectiveness. Acad Manage J. 1971; 14 2: 203– 212. [Google Scholar]
- 17. Laughlin PR. Social choice theory, social decision scheme theory, and group decision-making. Group Process Intergroup Relat. 2011; 14 1: 63– 79. [Google Scholar]
- 18. Stasser G, Titus W. Effects of information load and percentage of shared information on the dissemination of unshared information during group discussion. J Pers Soc Psychol. 1987; 53 1: 81– 93. [Google Scholar]
- 19. Mesmer-Magnus JR, Dechurch LA. Information sharing and team performance: a meta-analysis. J Appl Psychol. 2009; 94 2: 535– 546. [DOI] [PubMed] [Google Scholar]
- 20. Brodbeck FC, Kerschreiter R, Mojzisch A, Frey D, Schulz-Hardt S. The dissemination of critical, unshared information in decision-making groups: the effects of pre-discussion dissent. Eur J Soc Psychol. 2002; 32 1: 35– 56. [Google Scholar]
- 21. Stasser G, Titus W. Pooling of unshared information in group decision making: Biased information sampling during discussion. J Pers Soc Psychol. 1985; 48 6: 1467– 1478. [Google Scholar]
- 22. Devine DJ. Effects of cognitive ability, task knowledge, information sharing, and conflict on group decision-making effectiveness. Small Group Research. 1999; 30 5: 608– 634. [Google Scholar]
- 23. Kelly JR, Karau SJ. Group decision making: the effects of initial preferences and time pressure. Pers Soc Psychol Bull. 1999; 25 11: 1342– 1354. [Google Scholar]
- 24. Phillips KW, Mannix EA, Neale MA. H. Gruenfeld D. Diverse groups and information sharing: the effects of congruent ties. J Exp Soc Psychol. 2004; 40 4: 497– 510. [Google Scholar]
- 25. Hornsey MJ. Social identity theory and self-categorization theory: a historical review. Soc Personal Psychol Compass. 2008; 2 1: 204– 222. [Google Scholar]
- 26. Rink FA, Ellemers N. Temporary versus permanent group membership: how the future prospects of newcomers affect newcomer acceptance and newcomer influence. Pers Soc Psychol Bull. 2009; 35 6: 764– 775. [DOI] [PubMed] [Google Scholar]
- 27. Stone P, Kagotani K. Size Matters, Difference Matters. European Political Science Association . Barcelona, Spain; 2013. [Google Scholar]
- 28. Austen-Smith D, Banks JS. Information aggregation, rationality, and the Condorcet jury theorem. Am Polit Sci Rev. 1996; 90 1: 34– 45. [Google Scholar]
- 29. Karotkin D, Paroush J. Optimum committee size: quality-versus-quantity dilemma. Soc Choice Welf. 2003; 20 3: 429– 441. [Google Scholar]
- 30. Waller BM, Hope L, Burrowes N, Morrison ER. Twelve (not so) angry men: managing conversational group size increases perceived contribution by decision makers. Group Process Intergroup Relat. 2011; 14 6: 835– 843. [Google Scholar]
- 31. Azer SA. Introducing a problem-based learning program: 12 tips for success. Med Teach. 2011; 33 10: 808– 813. [DOI] [PubMed] [Google Scholar]
- 32. Intuitor. How to design small decision making groups. http://www.intuitor.com/statistics/SmallGroups.html. Accessed January 25, 2016. [Google Scholar]
- 33. Laughlin PR, Hatch EC, Silver JS, Boh L. Groups perform better than the best individuals on letters-to-numbers problems: effects of group size. J Pers Soc Psychol. 2006; 90 4: 644– 651. [DOI] [PubMed] [Google Scholar]
- 34. Karau SJ, Williams KD. Social loafing: A meta-analytic review and theoretical integration. J Pers Soc Psychol. 1993; 65 4: 681– 706. [Google Scholar]
- 35. Jonker CM, van Riemsdijk MB, Vermeulen B. Shared mental models: a conceptual analysis. In: De Vos M, Fornara N, Pitt JV, Vouros G, eds. Coordination, Organizations, Institutions, and Norms in Agent Systems VI. Springer-Verlag Berlin Heidelberg; 2011. [Google Scholar]
- 36. Esser JK. Alive and well after 25 years: a review of groupthink research. Organ Behav Hum Decis Process. 1998; 73 2/3: 116– 141. [DOI] [PubMed] [Google Scholar]
- 37. Wittenbaum GM, Hollingshead AB, Paulus PB, Hirokawa RY, Peterson RS, Jehn KA, et al. The functional perspective as a lens for understanding groups. Small Group Research. 2004; 35 1: 17– 43. [Google Scholar]
- 38. Hodges B. Assessment in the post-psychometric era: learning to love the subjective and collective. Med Teach. 2013; 35 7: 564– 568. [DOI] [PubMed] [Google Scholar]
- 39. Janis IL. Groupthink. Psychol Today. 1971; 5: 43– 46, 74–76. [Google Scholar]
- 40. Xiao L, Eastmure V. Information use in group decision making teams. In: Proceedings of the 77th Annual Meeting of the Association for Information Science and Technology. 2014. . https://asis.org/asist2014/proceedings/submissions/posters/228poster.pdf. Accessed January 25, 2016. [Google Scholar]
- 41. Tindale RS, Kameda T. “Social sharedness” as a unifying theme for information processing in groups. Group Process Intergroup Relat. 2000; 3 2: 123– 140. [Google Scholar]
- 42. Beran TN, Kaba A, Caird J, McLaughlin K. The good and bad of group conformity: a call for a new programme of research in medical education. Med Educ. 2014; 48 9: 851– 859. [DOI] [PubMed] [Google Scholar]
- 43. Lee JD, See KA. Trust in automation: Designing for appropriate reliance. Hum Factors. 2004; 46 1: 50– 80. [DOI] [PubMed] [Google Scholar]
- 44. Laughlin PR, Ellis AL. Demonstrability and social combination processes on mathematical intellective tasks. J Exp Soc Psychol. 1986; 22 3: 177– 189. [Google Scholar]
- 45. van Ginkel WP, van Knippenberg D. Group leadership and shared task representations in decision making groups. Leadership Q. 2012; 23 1: 94– 106. [Google Scholar]
- 46. De Dreu CK, Nijstad BA, van Knippenberg D. Motivated information processing in group judgment and decision making. Pers Soc Psychol Rev. 2008; 12 1: 22– 49. [DOI] [PubMed] [Google Scholar]
- 47. Klocke U. How to improve decision making in small groups effects of dissent and training interventions. Small Group Research. 2007; 38 3: 437– 468. [Google Scholar]
- 48. Lu L, Yuan YC, McLeod PL. Twenty-five years of hidden profiles in group decision making a meta-analysis. Personal Soc Psychol Rev. 2012; 16 1: 54– 75. [DOI] [PubMed] [Google Scholar]
- 49. van Ginkel WP, van Knippenberg D. Knowledge about the distribution of information and group decision making: when and why does it work? Organ Behav Hum Decis Process. 2009; 108 2: 218– 229. [Google Scholar]
- 50. Dennis AR. Information exchange and use in small group decision making. Small Group Research. 1996; 27 4: 532– 550. [Google Scholar]
- 51. Rothmund T, Mojzisch A, Schulz-Hardt S. Effects of consensus information and task demonstrability on preference-consistent information evaluation and decision quality in group decision making. Basic Applied Soc Psychol. 2011; 33 4: 382– 390. [Google Scholar]
- 52. De Grada E, Kruglanski AW, Mannetti L, Pierro A. Motivated cognition and group interaction: need for closure affects the contents and processes of collective negotiations. J Exp Soc Psychol. 1999; 35 4: 346– 365. [Google Scholar]
- 53. Rand DG, Newman GE, Wurzbacher OM. Social context and the dynamics of cooperative choice. J Behav Decis Mak. 2015; 28 2: 159– 166. [Google Scholar]
- 54. Pierro A, Mannetti L, De Grada ED, Livi S, Kruglanski AW. Autocracy bias in informal groups under need for closure. Pers Soc Psychol Bull. 2003; 29 3: 405– 417. [DOI] [PubMed] [Google Scholar]
- 55. Aronson E. The Social Animal. San Francisco: WH Freeman; 1972. [Google Scholar]
- 56. Neck CP, Moorhead G. Groupthink remodeled: the importance of leadership, time pressure, and methodical decision-making procedures. Hum Relat. 1995; 48 5: 537– 557. [Google Scholar]
- 57. Bazerman MH, Giuliano T, Appelman A. Escalation of commitment in individual and group decision making. Organ Behav Hum Perform. 1984; 33 2: 141– 152. [Google Scholar]
- 58. Horowitz IA, ForsterLee L, Brolly I. Effects of trial complexity on decision making. J Appl Psychol. 1996; 81 6: 757– 768. [DOI] [PubMed] [Google Scholar]
- 59. Mathieu J, Maynard MT, Rapp T, Gilson L. Team effectiveness 1997–2007: a review of recent advancements and a glimpse into the future. J Manag. 2008; 34 3: 410– 476. [Google Scholar]
- 60. Accreditation Council for Graduate Medical Education. Frequently asked questions about the next accreditation system. 2012. https://jcesom.marshall.edu/media/19073/NAS_FAQ-.pdf. Accessed February 3, 2016. [Google Scholar]
- 61. Hauer KE. ten Cate O, Boscardin C, Irby DM, Iobst W, O'Sullivan PS. Understanding trust as an essential element of trainee supervision and learning in the workplace. Adv Health Sci Educ Theory Pract. 2014; 19 3: 435– 456. [DOI] [PubMed] [Google Scholar]
- 62. Schulz-Hardt S, Brodbeck FC, Mojzisch A, Kerschreiter R, Frey D. Group decision making in hidden profile situations: dissent as a facilitator for decision quality. J Pers Soc Psychol. 2006; 91 6: 1080– 1093. [DOI] [PubMed] [Google Scholar]
- 63. Scholten L, van Knippenberg D, Nijstad BA, De Dreu CKW. Motivated information processing and group decision-making: effects of process accountability on information processing and decision quality. J Exp Soc Psychol. 2007; 43 4: 539– 552. [Google Scholar]
- 64. Lewis K, Belliveau M, Herndon B, Keller J. Group cognition, membership change, and performance: Investigating the benefits and detriments of collective knowledge. Organ Behav Hum Decis Process. 2007; 103 2: 159– 178. [Google Scholar]
- 65. Canon-Bowers JA, Salas E, Converse S. Shared mental models in expert team decision making. : Castellan NJ. Individual and Group Decision Making. Hillsdale, NJ: Lawrence Erlbaum Associates; 1993: 221– 245. [Google Scholar]
- 66. Gruenfeld DH, Mannix EA, Williams KY, Neale MA. Group composition and decision making: how member familiarity and information distribution affect process and performance. Organ Behav Hum Decis Process. 1996; 67 1: 1– 15. [Google Scholar]
- 67. Marta S, Leritz LE, Mumford MD. Leadership skills and the group performance: situational demands, behavioral requirements, and planning. Leadership Q. 2005; 16 1: 97– 120. [Google Scholar]
- 68. Holmboe ES, Hawkins RE. Practical Guide to the Evaluation of Clinical Competence. Philadelphia, PA: Mosby/Elsevier; 2008. [Google Scholar]
- 69. Tversky A, Kahneman D. Judgment under uncertainty: heuristics and biases. Science. 1974; 185 4157: 1124– 1131. [DOI] [PubMed] [Google Scholar]