

Abstract
Background:
Treatment of multidrug-resistant tuberculosis (MDR-TB) in the Programmatic Management of Drug-resistant TB program involves a standard regimen with a 6-month intensive phase and an 18-month continuation phase. However, the local drug resistance patterns in high MDR regions such as Mumbai may not be adequately reflected in the design of the regimen for that particular area.
Setting:
The study was carried out at a private Tertiary Level Hospital in Mumbai in a mycobacteriology laboratory equipped to perform the second-line drug susceptibility testing (DST).
Objective:
We attempted to analyze the impact of prescribing the standardized Category IV regimen to all patients receiving a DST at our mycobacteriology laboratory.
Materials and Methods:
All samples confirmed to be MDR-TB and tested for the second-line drugs at Hinduja Hospital's Mycobacteriology Laboratory in the year 2012 were analyzed.
Results:
A total of 1539 samples were analyzed. Of these, 464 (30.14%) were MDR-TB, 867 (56.33%) were MDR with fluoroquinolone resistance, and 198 (12.8%) were extensively drug-resistant TB. The average number of susceptible drugs per sample was 3.07 ± 1.29 (assuming 100% cycloserine susceptibility). Taking 4 effective drugs to be the cut or an effective regimen, the number of patients receiving 4 or more effective drugs from the standardized directly observed treatment, short-course plus regimen would be 516 (33.5%) while 66.5% of cases would receive 3 or less effective drugs.
Conclusion:
Our study shows that a high proportion of patients will have resistance to a number of the first- and second-line drugs. Local epidemiology must be factored in to avoid amplification of resistance.
KEY WORDS: Category IV treatment, directly observed treatment short-course plus, drug-resistant tuberculosis
INTRODUCTION
Tuberculosis (TB) is the leading infectious cause of death in India with about two people dying of the disease every 3 min.[1] There are an estimated 2.2 million new cases annually in the country. The proportion of multidrug-resistant TB (MDR-TB) (i.e., resistant to at least isoniazid and rifampicin) cases is about 2.2% in new cases and 11–19% in retreatment cases.[2] There are an estimated 99,000 annual incident cases of MDR-TB in India of which about 64,000 are from the TB cases notified to the Revised National Tuberculosis Control Programme (RNTCP).[2] The treatment of MDR-TB in the public sector involves the Programmatic Management of Drug-resistant TB (PMDT) rolling out the Directly Observed Treatment, Short-course (DOTS)-Plus program. The RNTCP recommends a standardized six drug regimens for MDR-TB patients (Category IV) involving 6–9 months of kanamycin, ethionamide, levofloxacin, cycloserine, pyrazinamide, and ethambutol followed by 18 months of ethionamide, levofloxacin, cycloserine, and ethambutol (total duration 24–27 months). Para-amino-salicylic acid (PAS), moxifloxacin, and capreomycin are available only as reserve drugs to be used in case of intolerance and/or resistance to any second-line drugs.[3]
However, the above regimen does not take into account the local epidemiological pattern of drug resistance for Mumbai and its immediate surroundings. There have been several reports of increasing levels of resistance to fluoroquinolones and other first- and second-line agents among MDR-TB patients, especially in Mumbai.[4] As per World Health Organization (WHO) guidelines for MDR-TB, an effective regimen should have at least four effective drugs including a second-line injectable and a fluoroquinolone.[5]
Most patients with drug-resistant TB (DR-TB) we encounter in our practice in Mumbai have resistance not just to isoniazid and rifampicin (i.e., MDR-TB) but, in addition, to several other first- and second-line drugs. We attempted to analyze the impact of prescribing the standardized Category IV MDR regimen to all patients receiving drug susceptibility testing (DST) at our tertiary care referral microbiology laboratory. Our intention was to determine in how many patients this standardized regimen would be appropriate (i.e., at least four effective drugs) and how many of them would end up receiving suboptimal regimens with the potential of consequent amplification of drug resistance.
MATERIALS AND METHODS
Our mycobacteriology laboratory receives about 30,000 samples for culture from both private and public sectors. However, DST requests are approximately 3500–4000. All samples sent for TB culture and DST to our microbiology laboratory between January 2012 and December 2012 were reviewed. We have a Level II mycobacterial laboratory. This laboratory was accredited for performing the first- and second-line DST by the College of American Pathologists in 2006. It has also received accreditation by the National Accreditation Board of Laboratories. The Central TB Division, Government of India, granted accreditation for the first-line DST in 2012 and the second-line DST in 2013. It is accredited at perform to perform DST for 13 drugs, viz., isoniazid, rifampicin, ethambutol, streptomycin, pyrazinamide, ethionamide, ofloxacin, moxifloxacin, PAS, kanamycin, amikacin, capreomycin, and clofazimine. It also serves as a reference laboratory for Mumbai and its immediate surroundings. TB culture is performed by the liquid culture, i.e., mycobacterial growth indicator tube (MGIT) method with DST also being performed via the same methods. The critical concentrations used for the MGIT-DST of the anti-TB drugs tested (13 in all) are as follows: Streptomycin 1 mcg/ml; isoniazid 0.1 mcg/ml; rifampicin 1 mcg/ml; ethambutol 5 mcg/ml; kanamycin 2 mcg/ml, ethionamide 5 mcg/ml; PAS 4 mcg/ml; ofloxacin 2 mcg/ml; moxifloxacin 0.25 mcg/ml; amikacin 1 mcg/ml; clofazimine 0.5 mcg/ml; capreomycin 2.5 mcg/ml, and pyrazinamide 100 mcg/ml.
All samples confirmed MDR on MGIT-DST testing and also tested for the second-line drugs (i.e., drugs used in DOTS-Plus regimen) from January 2012 to December 2012 were included for analysis. Susceptibility to moxifloxacin was taken as a surrogate marker for susceptibility to levofloxacin (as levofloxacin is not tested). Cycloserine susceptibility testing is not done at Hinduja Hospital due to its inherent unreliability. However, all samples were assumed to be susceptible to cycloserine in the final analysis of a number of effective drugs available. It is important to note that DST is only performed on request of the treating physician and not on all culture positive samples. While there is a possibility of bias with all samples not being tested for drug resistance, this was a study on only MDR-TB samples and not on drug susceptible ones who would have responded well to the first-line drugs.
For the purpose of this study, we had studied the drug susceptibility patterns of samples from patients without the knowledge of the source of these patients (public or private). Details of prior treatment were also not available to us. However, an average of 25–30% of samples received is generally from the RNTCP.
RESULTS
DST was performed on a total of 3651 samples in 2012. A total number of samples detected to be MDR which were also tested for the second-line drugs were 1539, all of which were included in our analysis. Of these, 1233 (80.1%) samples were pulmonary while 306 (19.9%) were extrapulmonary.
Of the 1539 samples, 464 were MDR-TB (30.14%), 867 (56.33%) were MDR-TB with fluoroquinolone resistance, and 198 (12.8%) were extensively drug-resistant TB (XDR-TB) (MDR + at least 1 fluoroquinolone resistance + 1 second-line injectable resistance). Of the 198 XDR-TB samples, only 4 were pure XDR-TB while 194 had resistance to other second-line drugs beyond XDR-TB.
When the individual drug susceptibility patterns of drugs used in the DOTS-Plus regimen was analyzed; among the 1539 samples, 14% were kanamycin-resistant, 66% were moxifloxacin-resistant, 58.5% were ethionamide-resistant, 77.6% were pyrazinamide-resistant, and 73.4% were ethambutol-resistant.
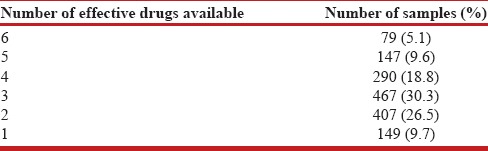
Table 1 shows the percentage of patients who would receive one, two, three, four, five, and six effective drugs in the standardized regimen. Thus, the average number of susceptible drugs per sample was 3.07 ± 1.29 (assuming 100% cycloserine susceptibility). Taking four effective drugs to be the cut or an effective regimen, the number of samples which would receive 4 or more effective drugs from the standardized DOTS-Plus regimen would be 516 (33.5%). The number of MDR-TB cases which would receive three or less effective drugs from the standardized DOTS-Plus regimen would be 1023 (66.5%). Thus, almost two-thirds of the MDR-TB cases would receive an inadequate regimen.
Table 1.
Number of samples receiving differing number of effective drugs in the standardized directly observed treatment short-course-plus regimen (assuming all samples susceptible to cycloserine)
Susceptibility levels for moxifloxacin, PAS, and clofazimine (currently included only as reserve drugs and not part of the standardized regimen) were 34%, 86%, and 99%, respectively.
DISCUSSION
India bears the burden of much of the world's DR-TB. Estimated number of MDR-TB cases in India among the notified pulmonary cases was 64,000 in 2012, overtaking China's estimate of 59,000 for the same period. A number of notified/diagnosed MDR-TB cases were 16,588 while a number of patients put on treatment for MDR-TB were 14,143. Almost 2.2% of new TB cases and almost 11–19% of retreatment cases of TB in India have MDR-TB.[2] This is much more as of 2014.
Mumbai is India's commercial capital and one of the most densely populated (population - 12,478,447) and congested cities (population density >20,000 persons/km2). The proportion of MDR-TB cases in new as well as previously treated cases is much higher compared to national estimates. A study by D'souza et al.[6] in 2009 showed that almost 24% of new cases and 41% of previously treated cases had MDR-TB. Further, of the 24% new cases, 20% had amplified resistance to 3–4 drugs while only 4% had resistance to just isoniazid and rifampicin. A report by Almeida et al.[7] in 2003 had reported that almost 51% of cases at Hinduja Hospital had MDR compared to 2% at a rural center. Although a referral bias may partly explain such high MDR-TB rates, as ours is a reference laboratory for Mumbai, it might be somewhat reflective of the disease profile of the city although it might be improper to extrapolate these findings to the whole country. Atre et al.[8] in 2011 also showed over 20% of new cases in Mumbai had MDR-TB with Beijing strain and female being risk factors for having MDR-TB at onset of therapy in new cases.
Category IV treatment via DOTS-Plus has been rolled out in India by RNTCP for MDR-TB since 2007. DOTS-Plus was started in Maharashtra from 2008 onward and the Capital of Mumbai from the year 2010. By the end of the year 2011, only 6994 patients had been started on Category IV treatment throughout the country. However, the situation improved significantly in the next year and by the end of 2012, around 20,136 patients had been started on Category IV treatment.[9] As of 2013, about 2610 patients were on Category IV treatment in Mumbai itself.
The treatment regimens for MDR-TB involve weaker and more toxic drugs for longer durations. The cure rates with these regimens vary from 38% to100% in different studies.[10] The seminal study from USA[11] in a hospitalized setting showed a success rate of 65% while Mitnick et al.[12] showed a success rate of almost 83% in a community-based DOTS set up in Peru. As per WHO, the treatment success rates for MDR-TB in the South-East Asian Region is about 50–60%.[2] Various studies including the two studies above showed that an individualized treatment regimen had a greater success rate than a standardized treatment regimen. The individualized treatments have shown to reduce amplification of resistance.[13,14] Further, in areas with high success rate of DOTS first-line therapy, cases in whom DOTS first line has not worked, standardized regimens may not work in patients with suspected MDR-TB at the outset.[15] While in countries with low exposure to the second-line drugs, a standardized approach to MDR-TB may well be justified, in countries such as India, with multiple treatment schemes in the private sector without adequate supervision, an individualized treatment regimen will offer the best results.[16,17,18,19,20] Clearly, for MDR-TB, one size does not fit all.
In any regimen, the local epidemiology and prevalent drug-resistant patterns need to be considered. There is a wide variety in patterns of resistance among MDR and XDR-TB patients which must be considered when designing their regimens. Standardized regimens are not effective for all patients. In our analysis, albeit in a bias setting, more than 50% of samples were already MDR-TB with additional fluoroquinolone resistance. Further, almost three-fourths of the samples were resistant to pyrazinamide and ethambutol. Fifty-eight percent were also resistant to ethionamide. Hence, an empiric, standardized regimen involving above drugs is likely to be ineffective with in many cases the only susceptible drugs being kanamycin and probably cycloserine (almost a quarter of the samples). Almost 12.8% of the samples were XDR at evaluation. The above-standardized regimen is thus unlikely to be effective in this population of patients and may amplify resistance.
As per the WHO guidelines,[5] the intensive phase of a treatment regimen for MDR-TB should include at least four second-line anti-TB drugs that are likely to be effective. Our study showed, even assuming 100% susceptibility for cycloserine, almost two-thirds of the samples will receive three or less effective drugs, which will make for an ineffective regimen. Such a regimen will only serve to amplify drug resistance to existing drugs to which the bacteria are susceptible such as kanamycin which will convert MDR-TB into XDR-TB.
The extended resistance patterns are by no means limited to Mumbai alone. Salvo et al.[21] showed in 2012 that in MDR-TB patients among refugees, almost 65% of the patients show additional resistance to at least one more second-line drug such as ethionamide. Similar data have emerged from China as well.[22]
The reports from New Delhi by Singla et al.[23] show a cure of 61% with a culture conversion of almost 79%. However, the drug regimen was based on a pilot project run in the preceding 3 years at the same site that represented the local drug resistance epidemiology. For the DOTS-Plus program to be effective in a country as diverse as India, local regimens must reflect the existing drug resistance epidemiology.
Our study shows that a high proportion of patients will have resistance to a number of the remaining first- and second-line drugs. Hence, the upfront empiric regimen must reflect the same.
Based on the DST data from our laboratory, we would currently recommend a Category IV regimen for Mumbai comprising the following: Kanamycin, moxifloxacin, ethionamide, PAS, cycloserine, and clofazimine although resistance to ethionamide and moxifloxacin is 58.5% and 66%, respectively but still markedly lower than resistance to pyrazinamide (77.6%) and ethambutol (73.4%). Ideally, we would recommend to continue this regimen until a DST is available following which the regimen can be individualized. This would probably have a better chance of success due to increase in number of effective drugs available. The pill burden of this proposed regimen will be eight tablets, one injection and PAS granules for the weight band of over 45 kg. The pill burden of the current standardized regimen is 13 tablets and one injection. Hence, the possibility of intolerance of the proposed regimen should not be greater than the one currently in place.
Complementing this, we must augment laboratory capacity so that there is minimal delay in diagnosis and where the second-line DST is also done upfront, especially in a place like Mumbai with high levels of resistance to these drugs. This will allow patients to be provided with individualized treatment as soon as possible. The fact that the PMDT program is contemplating implementation of individualized treatment regimens is a step in the right direction. This may provide best chances of individual cure as well as reduction in the chances for resistance amplification and transmission of DR-TB. As mentioned earlier, many studies have demonstrated that individualized regimens have the best success rates and may be the best way forward.
CONCLUSION
Our study shows that a high proportion of patients will have resistance to a number of the first and second-line drugs. Local epidemiology must be factored in while designing an empiric regimen to avoid amplification of resistance. Individualized treatment based on drug susceptibility testing may be the best way forward.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Revised National Tuberculosis Programme (RNTCP) – TBC India. [Last accessed on 2015 Feb 08]. Available from: http://www.tbcindia.nic.in/rntcp.html .
- 2.World Health Organization. Global Tuberculosis Report 2013. Geneva, Switzerland: World Health Organization; 2013. [Google Scholar]
- 3.New Delhi: Central TB Division; 2012. Revised National Tuberculosis Control Programme. Guidelines for the Programmatic Management of Drug Resistant Tuberculosis (PMDT) in India. [Google Scholar]
- 4.Agrawal D, Udwadia ZF, Rodriguez C, Mehta A. Increasing incidence of fluoroquinolone-resistant Mycobacterium tuberculosis in Mumbai, India. Int J Tuberc Lung Dis. 2009;13:79–83. [PubMed] [Google Scholar]
- 5.Geneva, Switzerland: World Health Organization; 2011. World Health Organization. Guidelines for the Programmatic Management of Drug Resistant Tuberculosis: 2011 Update. [PubMed] [Google Scholar]
- 6.D'souza DT, Mistry NF, Vira TS, Dholakia Y, Hoffner S, Pasvol G, et al. High levels of multidrug resistant tuberculosis in new and treatment-failure patients from the Revised National Tuberculosis Control Programme in an urban metropolis (Mumbai) in Western India. BMC Public Health. 2009;9:211. doi: 10.1186/1471-2458-9-211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Almeida D, Rodrigues C, Udwadia ZF, Lalvani A, Gothi GD, Mehta P, et al. Incidence of multidrug-resistant tuberculosis in urban and rural India and implications for prevention. Clin Infect Dis. 2003;36:e152–4. doi: 10.1086/374931. [DOI] [PubMed] [Google Scholar]
- 8.Atre SR, D'souza DT, Vira TS, Chatterjee A, Mistry NF. Risk factors associated with MDR-TB at the onset of therapy among new cases registered with the RNTCP in Mumbai, India. Indian J Public Health. 2011;55:14–21. doi: 10.4103/0019-557X.82536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.New Delhi: Central TB Division; 2013. Revised National Tuberculosis Control Programme. TB India 2013. [Google Scholar]
- 10.Mukherjee JS, Rich ML, Socci AR, Joseph JK, Virú FA, Shin SS, et al. Programmes and principles in treatment of multidrug-resistant tuberculosis. Lancet. 2004;363:474–81. doi: 10.1016/S0140-6736(04)15496-2. [DOI] [PubMed] [Google Scholar]
- 11.Goble M, Iseman MD, Madsen LA, Waite D, Ackerson L, Horsburgh CR., Jr Treatment of 171 patients with pulmonary tuberculosis resistant to isoniazid and rifampin. N Engl J Med. 1993;328:527–32. doi: 10.1056/NEJM199302253280802. [DOI] [PubMed] [Google Scholar]
- 12.Mitnick C, Bayona J, Palacios E, Shin S, Furin J, Alcántara F, et al. Community-based therapy for multidrug-resistant tuberculosis in Lima, Peru. N Engl J Med. 2003;348:119–28. doi: 10.1056/NEJMoa022928. [DOI] [PubMed] [Google Scholar]
- 13.5th ed. Paris: International Union against Tuberculosis and Lung Disease; 2000. International Union against Tuberculosis and Lung Disease. Management of Tuberculosis: A Guide for Low Income Countries. [Google Scholar]
- 14.Portaels F, Rigouts L, Bastian I. Addressing multidrug-resistant tuberculosis in penitentiary hospitals and in the general population of the former Soviet Union. Int J Tuberc Lung Dis. 1999;3:582–8. [PubMed] [Google Scholar]
- 15.Becerra MC, Freeman J, Bayona J, Shin SS, Kim JY, Furin JJ, et al. Using treatment failure under effective directly observed short-course chemotherapy programs to identify patients with multidrug-resistant tuberculosis. Int J Tuberc Lung Dis. 2000;4:108–14. [PubMed] [Google Scholar]
- 16.Caminero JA. Management of multidrug-resistant tuberculosis and patients in retreatment. Eur Respir J. 2005;25:928–36. doi: 10.1183/09031936.05.00103004. [DOI] [PubMed] [Google Scholar]
- 17.Boston, MA: Partners in Health; 2003. Partners in Health, Program in Infectious Disease and Social Change, Harvard Medical School. The PIH Guide to the Medical Management of Multidrug – Resistant Tuberculosis. [Google Scholar]
- 18.Iseman MD. Treatment of multidrug-resistant tuberculosis. N Engl J Med. 1993;329:784–91. doi: 10.1056/NEJM199309093291108. [DOI] [PubMed] [Google Scholar]
- 19.Caminero JA, de March P. Statements of ATS, CDC, and IDSA on treatment of tuberculosis. Am J Respir Crit Care Med. 2004;169:316–7. doi: 10.1164/ajrccm.169.2.952. [DOI] [PubMed] [Google Scholar]
- 20.Caminero JA, editor. Paris, France: International Union against Tuberculosis and Lung Disease; 2013. Guidelines for Clinical and Operational Management of Drug-Resistant Tuberculosis. [Google Scholar]
- 21.Salvo F, Dorjee K, Dierberg K, Cronin W, Sadutshang TD, Migliori GB, et al. Survey of tuberculosis drug resistance among Tibetan refugees in India. Int J Tuberc Lung Dis. 2014;18:655–62. doi: 10.5588/ijtld.13.0516. [DOI] [PubMed] [Google Scholar]
- 22.Zhao Y, Xu S, Wang L, Chin DP, Wang S, Jiang G, et al. National survey of drug-resistant tuberculosis in China. N Engl J Med. 2012;366:2161–70. doi: 10.1056/NEJMoa1108789. [DOI] [PubMed] [Google Scholar]
- 23.Singla R, Sarin R, Khalid UK, Mathuria K, Singla N, Jaiswal A, et al. Seven-year DOTS-plus pilot experience in India: Results, constraints and issues. Int J Tuberc Lung Dis. 2009;13:976–81. [PubMed] [Google Scholar]