

Abstract
Background:
Hepatitis viruses and human immunodeficiency virus (HIV) coinfection is a major cause of liver diseases worldwide. High prevalence of hepatitis B virus (HBV) and hepatitis C virus (HCV) in Asia makes it important to understand HBV and HCV coinfection with HIV in this part of the globe. This study was done with the aim of assessing the time trends of seroepidemiology of HBV and HCV coinfection in HIV patients over the last 3 years.
Materials and Methods:
Year wise retrospective analysis of data between January 2012 and December 2014 was done.
Results:
The prevalence of HIV infection among 0–20 years and >60 years age group decreased over the last 3 years (2012–2014), 8.4%, 6.4%, and 3.1% and 3.6%, 3.8%, and 1.5%, respectively. While increasing prevalence was seen among 21–40 years age group, 57.8%, 60.2%, and 67.1%, respectively in 2012, 2013, and 2014. There was no significant relationship between age/gender and HBV/HCV seropositivity among HIV-positive patients. The risk of acquiring HBV infection was more in HIV-positive patients who were >60 years of age (odds ratio = 3.3182; 95% confidence interval: 0.3669–30.005). The prevalence of HCV seropositivity is less in HIV-positive patients as only one case was anti-HCV antibody positive in last 3 years who was a male patient in the age group 21–40 years. A declining trend was observed for HIV positive cases over 2012–2014 while no significant trend change is seen in HBV/HCV seropositivity among HIV patients from 2012 to 2104.
Conclusion:
It is recommended to screen HIV patients routinely for concurrent HBV/HCV infection as hepatotropic viruses with HIV increase the risk of liver mortalities.
Keywords: Hepatitis B virus, hepatitis C virus, human immunodeficiency virus
INTRODUCTION
The emergence of human immunodeficiency virus (HIV), hepatitis B virus (HBV), and hepatitis C virus (HCV) coinfection as a major cause of morbidity due to liver diseases worldwide has been of great concern since the last two decades.[1] Since the introduction of highly active antiretroviral therapy, the survival rate of HIV positive patients has increased.[2] Hence, comorbidities like chronic liver disease due to HCV and HBV infection are significant problems. Although the presence of hepatitis viruses do not affect the overall survival of HIV-positive patients, but they do predispose to death from liver failure.[3] It has been estimated that 2–4 million people have chronic HBV coinfection and 4–5 million people have HCV coinfection among the total HIV-infected people worldwide.[2] In Europe and the USA, HIV-HBV coinfection is around 6–14%.[2,4] Most of the studies of HIV, HCV, and HBV coinfection have been done on western population. Few serological observations have been reported from India.[5,6,7] The prevalence of HBV and HCV is very high in Asian countries[1] and, therefore, it is important to understand HBV and HCV coinfection with HIV in this part of the globe. We have conducted this study in a super specialty hospital situated in New Delhi with the objective of assessing the time trends of seroepidemiology of HBV and HCV coinfection in HIV-positive patients over 3 years, i.e., 2012–2014.
MATERIALS AND METHODS
The study was carried out as a year wise retrospective analysis of data between January 2012 and December 2014 after approval of the Institutional Ethical Committee. We examined the data of all patients who were referred to us by the clinicians for HIV testing and were confirmed as having HIV infection as per national AIDS control organization (NACO) guidelines at the integrated counseling and testing center (ICTC) after pre- and post-test counseling. The samples of all these patients were also tested for hepatitis B surface antigen (HBsAg) and anti-HCV antibody.
Laboratory diagnosis of human immunodeficiency virus
The samples at our hospital were tested for HIV antibody according to the guidelines of NACO.[8] Antibodies to HIV were determined by ELISA (by J Mitra and Co., Pvt. Ltd.,) and rapid immunochromatographic test (Retroscreen-HIV, Qualpro Diagnostics). All the positive results were then referred to ICTC and confirmed thereafter pre- and post-test counseling.
Laboratory diagnosis of hepatitis B virus
The serum samples were analyzed for HBsAg by ELISA technique (TRANSASIA) and all positive samples were retested by rapid immunochromatographic test (ASPEN).
Laboratory diagnosis of hepatitis C virus
The serum samples were analyzed for anti-HCV antibodies by ELISA technique (BIORAD) and all positive samples were retested by rapid immunochromatographic test (SD BIOLINE HCV).
Statistical analysis
Two-tailed Fisher exact test was conducted for categorical variables, and odds ratio (OR), 95% confidence interval (CI) were obtained using the GraphPad software (graphpad.com/quickcalcs/contingency1.cfm) manufactured by GraphPad software, Inc, California. The level of significance was P < 0.05.
RESULTS
The total number of HIV positive cases in 2012, 2013 and 2014 were 83, 78 and 64 respectively. Among these, the prevalence of HBV seropositivity was 3.6%, 6.4% and 6.2% in 2012, 2013 and 2014, respectively while only one case (1.56% prevalence) has been reported positive for anti-HCV antibody among HIV-positive cases in the last 3 years. Age and gender wise data reveals that most of the HIV-positive cases were males and were between 21 and 40 years age group [Table 1]. The prevalence of HBV seropositivity in males was 83.3% as compared to females (16.6%). It was observed [Figure 1] that the prevalence of HIV infection among 0–20 years and >60 years age group was decreasing over the last 3 years (2012–2014), 8.4%, 6.4%, and 3.1% and 3.6%, 3.8%, and 1.5%, respectively. While increasing prevalence was seen among 21–40 years age group, 57.8%, 60.2%, and 67.1% respectively in 2012, 2013, and 2014. There was no significant relationship [Table 2] between age/gender and HBV/HCV seropositivity among HIV-positive patients. However, the risk of acquiring HBV infection was more in HIV-positive patients who were >60 years of age (OR = 3.3182; 95% CI: 0.3669–30.005). The prevalence of HCV seropositivity is less in HIV-positive patients as compared to HBV as only one case was anti-HCV antibody positive in last 3 years, i.e., in 2014 and he was a male patient in the age group 21–40 years.
Table 1.
Profile of HIV positive patients 2012-2014
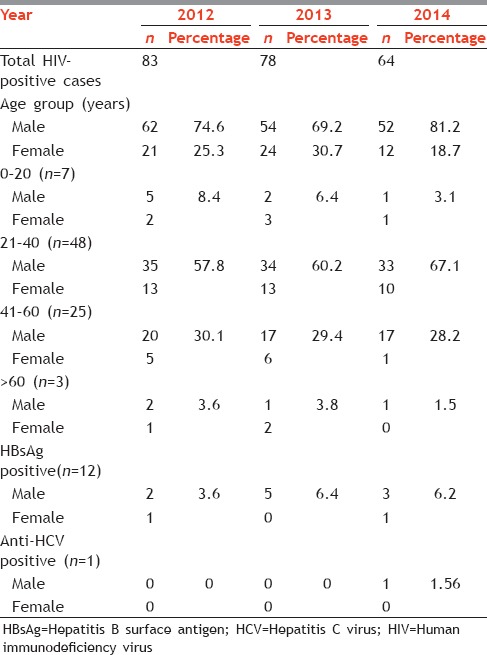
Figure 1.
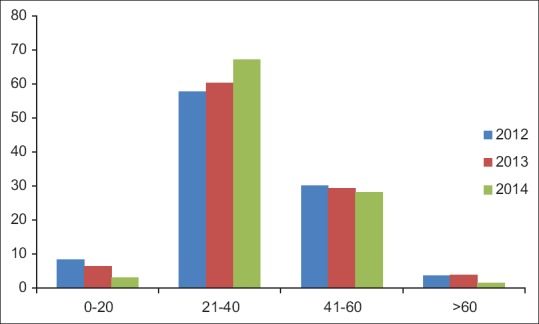
Age wise trend in human immunodeficiency virus seropositive cases 2012–2014
Table 2.
Relationship between age and gender and HBV and HCV seropositivity among HIV-positive patients
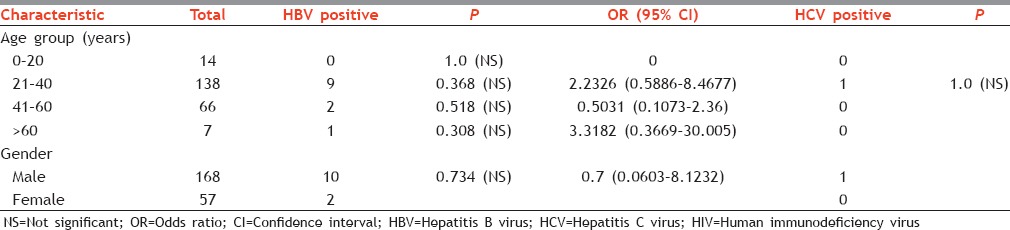
Figure 2 shows the trend in HBV and HCV seropositivity among HIV-positive patients over the last 3 years. A declining trend has been observed for HIV positive cases over 2012–2014 while no significant trend change is seen in HBV/HCV seropositivity among HIV- positive patients from 2012 to 2104.
Figure 2.
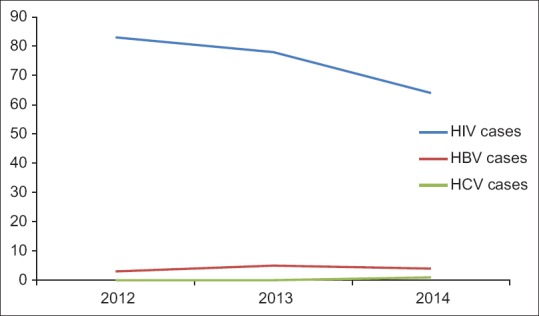
Trend in seropositivity of human immunodeficiency virus, hepatitis B virus and hepatitis C virus 2012–2014
DISCUSSION
The clinical course of HIV in infected patients may be complicated by the presence of coinfection with HBV and HCV and which may also have adverse effects on HIV treatment. Many studies have reported the prevalence of HBV/HCV coinfection in HIV.[9,10,11] One of the major determinants of prevalence is geographical location and different HIV-infected population show marked variations in the prevalence of HBV/HCV coinfections depending on the endemicity.[10,11] Only few studies on the prevalence of HBV/HCV in HIV patients have been reported from India.[5,6,7,12,13] In our study, the prevalence of HBV in HIV patients was 3.6%, 6.4%, and 6.2% in 2012, 2013, and 2014, respectively. Studies from Lucknow[12] and Chennai[5] have also reported similar prevalence (<10%) of HBV coinfection with HIV. However, one study from Nagpur[13] reported a very high prevalence (30.4%) of HBV-HIV coinfection. This data reveal that observations have been highly variable from different regions of the country. The HCV prevalence in HIV patients was very low in our study (1.56%). However, other studies in India have reported prevalence as high as 8.3%[1] and 7.2%[12] and as low as 1.6%[12] and 2.3%.[5] Studies from other countries like Nigeria[14] have reported 0.4% HBV-HIV coinfection and 0% HIV-HCV coinfection and Iran[15] have showed 14.5% HIV-HBV coinfection and 72% HIV-HCV coinfection. It is noticeable in our study that the high prevalence rate of HBV seropositivity in HIV patients in comparison with HCV seropositivity indicates poor immunization coverage because multiple vaccines are available for HBV in contrast to HCV which lacks a vaccine. One of the reasons could be that the sexual transmission of HCV is lower as compared to HBV and it is transmitted mostly via injections and in India the most common route of HIV transmission is sexual. It is recommended that all high-risk group persons should get vaccinated against HBV. In our study, majority of the HIV-positive patients and HBV/HCV seropositive patients among them were males in the age group 21–40 years which is the active sexual stage. Saha et al.[16] Have also reported similar findings as regards to age and sex. We have also reported a high prevalence of HBV seropositivity in HIV patients in males (83.3%) and even the one case of HCV seropositive was also a male patient. Similar results have been found in other studies in relation to HBV and HCV infection in HIV patients which helps in explaining why more than 80% of coinfected individuals are males.[17,18,19] Although age and gender have no statistically significant association with HBV/HCV seropositivity in HIV patients, old age plus immunodeficiency does increase the risk of acquiring hepatic infection as observed in our study that HIV-positive patients who were >60 years of age were at increased risk of becoming HBV seropositive (OR = 3.3182; 95% CI: 0.3669–30.005) as compared with other age groups.
The prevalence of HIV in India is quite high, and it has the second most number of people living with HIV.[5] However, we observed that the number of HIV-positive cases decreased from 83 cases in 2012 to 64 cases in 2014. Despite this, there has been no significant change in the prevalence of HBV/HCV seropositivity in HIV patients over last 3 years in our study. This probably explains why an estimated one-third of deaths in HIV patients are directly or indirectly related to liver diseases.[15] Rising trends in the prevalence of HBV and HCV among HIV-infected patients for 1998–2004 have been reported by a study in the USA.[20] To the best of our knowledge and literature search, no studies have been reported from India so far regarding trends in HBV/HCV seropositivity in HIV patients.
CONCLUSION
Immunodeficiency by HIV leads to a high probability of acquiring HBV and HCV infection in HIV positive patients. Therefore, it is recommended that HIV patients should be screened routinely for concurrent HBV/HCV infection because the presence of hepatotropic viruses with HIV increases the risk of cirrhosis and other liver mortalities. Furthermore, it interferes with antiretroviral therapy. The findings of our study and other similar studies might be useful for surveillance agencies in India for better understanding and management of HBV/HCV coinfections with HIV. Such scientific findings should be interpreted into sustainable prevention programs to improve public health policies, not only in India but worldwide.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest
Acknowledgment
we would like to acknowledge Dr. A S Puri, director professor and head of Gastroenterology, G B Pant hospital and his technical staff for their support.
REFERENCES
- 1.Chandra N, Joshi N, Raju YS, Kumar A, Teja VD. Hepatitis B and/or C co-infection in HIV infected patients: A study in a tertiary care centre from South India. Indian J Med Res. 2013;138:950–4. [PMC free article] [PubMed] [Google Scholar]
- 2.Alter MJ. Epidemiology of viral hepatitis and HIV co-infection. J Hepatol. 2006;44(1 Suppl):S6–9. doi: 10.1016/j.jhep.2005.11.004. [DOI] [PubMed] [Google Scholar]
- 3.Mocroft A, Monforte A, Kirk O, Johnson MA, Friis-Moller N, Banhegyi D, et al. Decline in AIDS and death rates in EUROSIDA study; an observational study. Lancet. 2003;362:22–9. doi: 10.1016/s0140-6736(03)13802-0. [DOI] [PubMed] [Google Scholar]
- 4.Rockstroh JK. Management of hepatitis B and C in HIV co-infected patients. J Acquir Immune Defic Syndr. 2003;34(Suppl 1):S59–65. doi: 10.1097/00126334-200309011-00009. [DOI] [PubMed] [Google Scholar]
- 5.Saravanan S, Velu V, Kumarasamy N, Nandakumar S, Murugavel KG, Balakrishnan P, et al. Coinfection of hepatitis B and hepatitis C virus in HIV-infected patients in south India. World J Gastroenterol. 2007;13:5015–20. doi: 10.3748/wjg.v13.i37.5015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bhattacharya S, Badrinath S, Hamide A, Sujatha S. Co-infection with hepatitis C virus and human immunodeficiency virus among patients with sexually transmitted diseases in Pondicherry, South India. Indian J Pathol Microbiol. 2003;46:495–7. [PubMed] [Google Scholar]
- 7.Saha MK, Chakrabarti S, Panda S, Naik TN, Manna B, Chatterjee A, et al. Prevalence of HCV and HBV infection amongst HIV seropositive intravenous drug users and their non-injecting wives in Manipur, India. Indian J Med Res. 2000;111:37–9. [PubMed] [Google Scholar]
- 8.National AIDS Control Organisation (NACO). Government of India. Ministry of Health and Family Welfare. National guidelines on HIV Testing (July 2015) Available from: http://www.naco.gov.in/upload/2015%20MSLNS/HIV%20Guidelines.pdf .
- 9.Thio CL, Seaberg EC, Skolasky R, Jr, Phair J, Visscher B, Muñoz A, et al. HIV-1, hepatitis B virus, and risk of liver-related mortality in the Multicenter Cohort Study (MACS) Lancet. 2002;360:1921–6. doi: 10.1016/s0140-6736(02)11913-1. [DOI] [PubMed] [Google Scholar]
- 10.Thio CL. Hepatitis B and human immunodeficiency virus coinfection. Hepatology. 2009;49(5 Suppl):S138–45. doi: 10.1002/hep.22883. [DOI] [PubMed] [Google Scholar]
- 11.Tedaldi EM, Hullsiek KH, Malvestutto CD, Arduino RC, Fisher EJ, Gaglio PJ, et al. Prevalence and characteristics of hepatitis C virus coinfection in a human immunodeficiency virus clinical trials group: The Terry Beirn Community Programs for Clinical Research on AIDS. Clin Infect Dis. 2003;36:1313–7. doi: 10.1086/374841. [DOI] [PubMed] [Google Scholar]
- 12.Tripathi AK, Khanna M, Gupta N, Chandra M. Low prevalence of hepatitis B virus and hepatitis C virus co-infection in patients with human immunodeficiency virus in Northern India. J Assoc Physicians India. 2007;55:429–31. [PubMed] [Google Scholar]
- 13.Tankhiwale SS, Khadase RK, Jalgoankar SV. Seroprevalence of anti-HCV and hepatitis B surface antigen in HIV infected patients. Indian J Med Microbiol. 2003;21:268–70. [PubMed] [Google Scholar]
- 14.Egah DZ, Banwat EB, Audu ES, Iya D, Mandong BM, Anele AA, et al. Hepatitis B surface antigen, hepatitis C and HIV antibodies in a low-risk blood donor group, Nigeria. East Mediterr Health J. 2007;13:961–6. [PubMed] [Google Scholar]
- 15.Mohammadi M, Talei G, Sheikhian A, Ebrahimzade F, Pournia Y, Ghasemi E, et al. Survey of both hepatitis B virus (HBsAg) and hepatitis C virus (HCV-Ab) coinfection among HIV positive patients. Virol J. 2009;6:202. doi: 10.1186/1743-422X-6-202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Saha K, Firdaus R, Santra P, Pal J, Roy A, Bhattacharya MK, et al. Recent pattern of co-infection amongst HIV seropositive individuals in tertiary care hospital, Kolkata. Virol J. 2011;8:116. doi: 10.1186/1743-422X-8-116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Braga WS, da Costa Castilho M, dos Santos IC, Moura MA, Segurado AC. Low prevalence of hepatitis B virus, hepatitis D virus and hepatitis C virus among patients with human immunodeficiency virus or acquired immunodeficiency syndrome in the Brazilian Amazon basin. Rev Soc Bras Med Trop. 2006;39:519–22. doi: 10.1590/s0037-86822006000600001. [DOI] [PubMed] [Google Scholar]
- 18.Treitinger A, Spada C, Ferreira LA, Neto MS, Reis M, Verdi JC, et al. Hepatitis B and hepatitis C prevalence among blood donors and HIV-1 infected patients in Florianópolis – Brazil. Braz J Infect Dis. 2000;4:192–6. [PubMed] [Google Scholar]
- 19.Oliveira SB, Merchán-Hamann E, Amorim LD. HIV/AIDS coinfection with the hepatitis B and C viruses in Brazil. Cad Saude Publica. 2014;30:433–8. doi: 10.1590/0102-311X00010413. [DOI] [PubMed] [Google Scholar]
- 20.Buskin SE, Barash EA, Scott JD, Aboulafia DM, Wood RW. Hepatitis B and C infection and liver disease trends among human immunodeficiency virus-infected individuals. World J Gastroenterol. 2011;17:1807–16. doi: 10.3748/wjg.v17.i14.1807. [DOI] [PMC free article] [PubMed] [Google Scholar]