

Abstract
Background
Bacterial sepsis remains a leading cause of morbidity and mortality in neonatal foals, but accurate diagnostic and prognostic markers are lacking. Adrenomedullin (AM) is a polypeptide with diverse biologic effects on the cardiovascular system that increases in septic humans and laboratory animals.
Hypotheses
Plasma AM concentration (p[AM]) is increased in septic neonatal foals compared to sick nonseptic and healthy control foals, and p[AM] is predictive of survival in septic neonatal foals.
Animals
Ninety critically ill (42 septic, 48 sick nonseptic) and 61 healthy foals <1 week of age.
Methods
A prospective observational clinical study was performed. Venous blood was collected from critically ill foals at admission and from healthy foals at 24 hours of age. Critically ill foals were categorized as septic or sick nonseptic based on blood culture results and sepsis score. Plasma [AM] was measured by using a commercially available ELISA for horses. Data were analyzed by using the Mann‐Whitney U‐test and P < .05 was considered significant.
Results
Plasma [AM] was not significantly different between septic and sick nonseptic foals (P = .71), but critically ill foals had significantly increased p[AM] compared to healthy controls (P < .0001). In critically ill foals, p[AM] was not predictive of survival (P = .051). A p[AM] cutoff concentration of 0.041 ng/mL provided a test sensitivity of 91% and specificity of 54% to predict illness.
Conclusions and Clinical Relevance
Plasma [AM] shows promise as a marker of health in neonatal foals, but p[AM] increases nonspecifically during perinatal illnesses and is not necessarily associated with sepsis.
Keywords: Foal, Sepsis, Survival
Abbreviations
- AM
adrenomedullin
- CBC
complete blood count
- FTPI
failure of transfer of passive immunity
- HIE
hypoxic ischemic encephalopathy
- LPS
lipopolysaccharide
- p[AM]
plasma adrenomedullin concentration
Neonatal sepsis is considered one of the most common causes of morbidity and mortality in equine neonates,1, 2, 3, 4 with mortality rate ranging from 45 to 76% despite advancements in therapeutic and intensive care.4, 5, 6 Definitive diagnosis of bacterial sepsis is obtained by microbial culture of an appropriate volume of venous blood. Unfortunately, culture and antimicrobial susceptibility results usually are not available until >72 hours after submission and, consequently, empiric treatment must be instituted before diagnosis.
Early antimicrobial treatment, although warranted in suspect cases, may adversely affect the sensitivity of blood culture as a diagnostic test. In addition, false negative blood culture results may be caused by low numbers of circulating bacteria or a relatively low volume of blood used for culture, and different blood culture systems yield variable results.7, 8 In 1 study, only 40% of gram negative infections were detected by antemortem blood culture as compared to postmortem culture.8 Given the relatively poor sensitivity of blood culture for diagnosis of sepsis in foals, a weighted scoring system currently is used as a diagnostic tool to identify sepsis. When used prospectively, this sepsis score demonstrated a sensitivity of 93% and a specificity of 86%.9 However, another study reevaluating the sepsis score reported a 67% sensitivity and a 76% specificity, suggesting that the scoring system's utility may vary based on the study population.10 Furthermore, the score failed to predict Actinobacillus bacteremia‐associated sepsis in 48% of foals.5 Finally, clinicopathologic findings have been associated with sepsis in foals, but lack of test specificity limits the usefulness of clinicopathologic changes in the diagnosis of sepsis.3, 4, 11, 12, 13, 14, 15, 16
Early and accurate diagnosis of sepsis is crucial to optimal care of critically ill patients because delay in treatment is an independent risk factor for nonsurvival, with treatment costs higher than those of other critically ill foals.6 In addition, accurate prognosis for survival is important given the rigors and expense of treatment. Thus, a simple, rapid, and reliable test that provides an early diagnosis of sepsis and predicts survival has the potential to greatly decrease morbidity, mortality, and treatment costs in affected foals.
Adrenomedullin (AM) is a vasodilatory polypeptide that was 1st isolated from human pheochromocytoma patients,17 and is synthesized by endothelial cells, vascular smooth muscle cells, and the adrenal medulla.18, 19, 20
Adrenomedullin is a potent vasodilator peptide, which along with its positive inotropic properties, helps to maintain perfusion to individual organs.21, 22 Plasma concentrations of AM increase rapidly after the onset of sepsis in humans and rodents, and contribute to hyperdynamic circulation which is characterized by decreased systemic vascular resistance, decreased mean arterial pressure, and compensatory increases in cardiac output and stroke volume.23, 24 Infusion of AM to healthy human volunteers resulted in similar hemodynamic changes, and administration of anti‐AM antibodies in rodents prevented hypotension in a sepsis model.23, 25 Finally, AM exhibits anti‐inflammatory and bactericidal properties.26, 27 Taken together, AM acts to promote tissue perfusion in septic patients by causing vasodilatation, and thus contributes to hypotension during the hyperdynamic phase of sepsis. Sepsis and septic shock leading to end‐organ damage are associated with 50‐fold increases in plasma AM concentration (p[AM]) compared to other pathologic conditions, both in clinical studies in humans28, 29 and in an experimental study in rats.30
We therefore hypothesized that p[AM] is increased in septic neonatal foals compared to sick nonseptic and healthy control foals, and that p[AM] is predictive of survival in septic neonatal foals. Based on these hypotheses, the objectives of the study were to compare p[AM] in septic, sick nonseptic, and healthy neonatal foals, and determine the prognostic value of p[AM] for survival in septic neonatal foals.
Materials and Methods
Data Collection
This study was approved by the Purdue University Institutional Animal Care Committee. Critically ill neonatal foals <1 week of age were recruited from Purdue University's Veterinary Teaching Hospital and from Hagyard Equine Medical Institute during the 2011 and 2012 foaling seasons. Jugular venous blood was collected at admission for measurement of p[AM]. Critically ill foals were categorized as septic (sepsis score >119 or positive blood culture) or sick nonseptic (sepsis score ≤11 and negative blood culture results when available). Foals euthanized because of financial constraints were excluded from the study.
Healthy control foals were recruited from the equine teaching herd at Washington State University's College of Veterinary Medicine and from a privately owned farm in Kentucky. To be included in the control group, foals had to have an uncomplicated birth after normal gestation duration (>330 days), normal physical examination findings, and blood IgG concentration >800 mg/dL at 24 hours of age.
Information obtained from the medical records of critically ill foals included signalment (year of admission, age of foal at admission [hours], breed, and sex), history of dystocia or Cesarean section, evidence of prematurity or dysmaturity, physical examination findings at presentation (behavior, mentation, rectal temperature, heart rate, respiratory rate, capillary refill time [seconds]), and fecal consistency. Admission blood l‐lactate concentrations also were recorded when available. Information obtained from healthy foals included history, signalment, physical examination findings, and blood IgG concentration at 24 hours of age.
Hematologic data (PCV, MCV, MCHC, hemoglobin concentration, total white blood cell count, segmented neutrophil count, band neutrophil count, presence of toxic neutrophils, and lymphocyte and platelet counts) and plasma fibrinogen concentration were obtained. Serum biochemical data (total CO2, total calcium, phosphorus, sodium, chloride, potassium, magnesium, glucose, creatinine, urea nitrogen, total protein, bilirubin, globulin and albumin concentrations, as well as activity of alkaline phosphatase [ALP], creatine kinase [CK], aspartate aminotransferase [AST], and gammaglutamyl transferase [GGT]) also were collected, and anion gap (AG) was calculated as AG = ([Na] + [K]) − ([Cl] + total CO2). Blood culture results (positive or negative), type of organism (gram positive, gram negative, anaerobic, or fungal), and species also were recorded when available. Treatments, complications during hospitalization, duration of hospitalization, outcome, and hospital cost also were obtained. Additional diagnostic evaluations performed in some foals included blood gas and pH analysis, mean arterial blood pressure measurement, ultrasonography, radiography, digital rectal palpation, jaundiced foal agglutination testing, fecal bacterial culture, synovial fluid analysis, and cerebrospinal fluid analysis.
Laboratory and Analytic Methods
Blood samples for culture were obtained after aseptic preparation of the skin and removal of 20–30 mL of blood into a sterile syringe from a jugular vein or after placement of an IV catheter by using aseptic technique. The sampling needle was discarded after venipuncture and a separate needle was used to transfer 3–7 mL of blood into a commercially available blood culture bottle.1
For determination of p[AM], 7–10 mL of blood was transferred into a plastic tube containing ethylenediaminetetraacetic acid (EDTA) based on manufacturer recommendations. After centrifugation at 1300 × g for 15 min at 4°C, plasma was transferred into plastic tubes and placed into a −20°C or −80°C freezer. Samples in the −20°C freezer were relocated to a −80°C freezer within 8 weeks, which is considered an acceptable time frame based on AM stability in human plasma.31 Plasma [AM] was determined in duplicate by using a previously validated, commercially available ELISA assay developed for equine AM.2 The company's reported validation data obtained from serum, heparinized plasma and EDTA plasma from horses are as follows: intra‐assay coefficient of variation (CV) <10%, interassay CV <12%, recovery 85–100%, and linearity 83‐105%. A standard curve was created for each ELISA plate in the current study. Sample concentration was determined by plotting optical density to the standard curve. The intra‐assay CV was 9.8% and the pooled interassay CV was 9.7% based on 5 plates. Assay detection range was 12–1,000 pg/mL, with an assay sensitivity of 6.5 pg/mL. Concentrations <6.5 pg/mL were reported as 6.5 pg/mL.
For routine hematologic and biochemical analyses, blood either was collected by venipuncture of a jugular vein or from a jugular catheter upon admission and before treatment was administered. Collected blood was placed into glass tubes containing EDTA for hematology, blood l‐lactate concentration and blood IgG concentration, sodium citrate or EDTA for plasma fibrinogen concentration, and serum separator tubes for serum biochemical analysis. Hemograms were performed with a commercial automated multichannel blood cell counting system3 with differential counts performed by manual cytologic examination of a blood smear. Blood l‐lactate concentration was measured with a commercially available lactate analyzer.4 Blood IgG concentration was determined semiquantitatively with a commercially available concentration immunoassay technology test5 or an automated analyzer6 with failure of transfer of passive immunity (FTPI) being defined as blood IgG concentration <400 mg/dL.32 Serum biochemistry was performed with a commercial automated analyzer.7 Plasma fibrinogen concentration was measured with a commercial automated analyzer,8 or by using the heat precipitation method.6
Statistical Analysis
Data were analyzed by using nonparametric methods because testing of data using the Shapiro‐Wilk normality test indicated that most studied variables were not normally distributed. Continuous data were expressed as median and range. A Mann‐Whitney U‐test was used to test the differences between critically ill and healthy foals, septic and sick nonseptic foals, and survivors versus nonsurvivors. The association between plasma [AM] and sepsis score and the association between plasma [AM] and age were evaluated by using Spearman's rho (r s). The optimal cutoff value for p[AM] associated with the presence or absence of critical illness was identified by using logistic regression, receiver operating characteristic (ROC) curve analysis, and calculation of the Youden index, J. Visually, this index represents the maximal vertical distance between the ROC curve and the diagonal or chance line and is calculated as J = maximum sensitivity (Se) + specificity (Sp) − 1. The adequacy of logistic regression model fit was evaluated by using the Hosmer‐Lemeshow test. Statistical analysis was performed by using commercially available software9 and a P‐value of <.05 was considered significant.
Results
Study Population
A total of 151 neonatal foals (90 critically ill, 61 healthy) <1 week of age were included. Forty‐six percent of hospitalized foals (42/90) were classified as septic and 54% (48/90) as sick nonseptic. The median age of septic and sick nonseptic foals was 10 and 8 hours, respectively, with the median age of all critically ill foals at admission being 8 hours (0–168 hours). For healthy control foals, the median age was 24 hours. The breeds represented by the critically ill foals included Thoroughbreds (75/90), Quarter Horses (8/90), Standardbreds (3/90), Clydesdales (2/90), Warmbloods (1/90), and Arabians (1/90). In the septic group, represented breeds included Thoroughbreds (33/42), Quarter Horses (4/42), Clydesdales (2/42), Standardbreds (1/42), and Arabians (1/42). In the sick nonseptic group, represented breeds included Thoroughbreds (42/48), Quarter Horses (4/48), and Standardbreds (2/48). Healthy foals consisted of Quarter Horses (31/61) and Arabians (30/61). Of the critically ill foals, 54% (49/90) were colts and 46% (41/90) were fillies. In the septic group, there were 55% (23/42) colts and 45% (19/42) fillies. In the sick nonseptic group, there were 54% (26/48) colts and 46% (22/48) fillies. In the healthy foal group, there were 54% (33/61) colts and 46% (28/61) fillies. In the sick nonseptic group, diagnoses included dystocia (22/48, 46%), hypoxic ischemic encephalopathy (HIE) (18/48, 38%), prematurity (10/48, 21%), rib fracture (7/48, 15%), enterocolitis (5/48, 10%), flexural deformity (5/48, 10%), renal failure (4/48, 8%), pneumonia (3/48, 6%), omphalophlebitis (2/48, 4%), meconium impaction (2/48, 4%), neonatal isoerythrolysis (2/48, 4%), and 1 each (2%) of patent urachus, hepatoblastoma, and herpes virus infection. Interestingly, 10 (21%) foals in the sick nonseptic group were diagnosed by the attending clinician as septic, despite a negative sepsis score or negative blood culture. The overall survival rate in the septic and sick nonseptic groups were 71% (30/42) and 79% (38/48), respectively, with an overall survival rate of 76% (68/90).
Plasma [AM] among Groups
There was no difference in p[AM] between septic and sick nonseptic foals (P = .71) or in foals that survived versus those that died (P = .051; Table 1). There was a marked difference in p[AM] between critically ill foals and healthy control foals (P < .0001; Table 1). Plasma [AM] was compared within subgroups of critically ill foals based on historic findings or final diagnoses. No particular diagnosis was associated with a significantly different p[AM] (failure of transfer of passive immunity [FTPI], P = .38; dystocia, P = .34; Cesarean section, P = .57, placentitis, P = .63; HIE, P = .74; prematurity, P = .77).
Table 1.
Comparison of plasma adrenomedullin concentration (median, range in parentheses) in healthy and critically ill foals, sick nonseptic and septic foals, and foals that survived versus foals that died. Data were compared by using the Mann‐Whitney U‐test. Number of foals in each category are presented in parentheses
| Plasma Adrenomedullin Concentration (ng/mL) | P‐Value | |
|---|---|---|
| Healthy (n = 61): 0.03 (0.01–0.54) | Critically ill (n = 90): 0.17 (0.01–0.73) | <.0001 |
| Sick nonseptic (n = 48): 0.16 (0.01–0.73) | Septic (n = 42): 0.18 (0.01–0.73) | .71 |
| Survival (n = 68): 0.15 (0.01–0.73) | Nonsurvival (n = 22): 0.24 (0.02–0.72) | .051 |
Clinical and Clinicopathologic Variables in Septic and Sick Nonseptic Foals
Significant differences were detected in the septic versus sick nonseptic groups. Septic foals had higher band neutrophil counts (P = .002), blood l‐lactate concentration (P = .004), and total serum bilirubin concentration (P = .01). Septic foals also exhibited higher incidence of FTPI (P = .02) and toxic changes in neutrophils (P = .03). There was no association between sepsis score and p[AM] (r s = +0.20; P = .058; Fig 1) or between age and p[AM] (r s = +0.046; P = .67).
Figure 1.
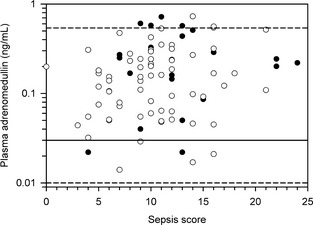
Scatterplot of relationship between plasma adrenomedullin concentration in critically ill neonatal foals (n = 90) and sepsis score on admission. The thick horizontal line is the median plasma adrenomedullin concentration in healthy neonatal foals, and the dashed horizontal lines are the 95% confidence interval for the plasma adrenomedullin concentration in healthy neonatal foals. Filled circles represent foals that did not survive and open circles represent foals that survived to discharge from the hospital.
Association of Clinical and Clinicopathologic Findings with Outcome
Surviving foals had higher rectal temperatures than nonsurvivors (P = .048). Among clinicopathologic variables, survivors exhibited lower anion gap (P = .003), MCV (P = .005), total calcium concentration (P = .023), blood l‐lactate concentration (P = .025), and higher tCO2 (P = .004) than nonsurvivors. Surviving foals had longer duration of hospitalization (P < .0001) and higher hospital cost (P < .025) compared to nonsurvivors.
Receiver Operating Characteristic Curve
A p[AM] cutoff concentration of 0.041 ng/mL provided optimal overall test performance based on the Youden index, with a sensitivity of 91% and a specificity of 54% in predicting critical illness in neonatal foals (Fig 2). The AUC was 0.75 and the Hosmer‐Lemeshow test indicated good model fit (P = .43).
Figure 2.
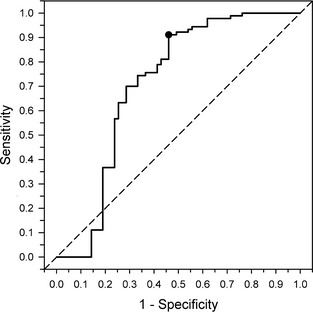
Receiver operating characteristic curve plotting test sensitivity against (1 – test specificity) at the optimal cutoff value for plasma adrenomedullin concentration (0.041 ng/mL) in differentiating healthy from critically ill nenonatal foals. The dashed diagonal line is the chance line (sensitivity [Se] = specificity [Sp] = 0.50; equivalent to tossing a coin, area under the curve = 0.50). The filled circle is the test Se (0.91) and Sp (0.54) at the optimal cutoff value for plasma adrenomedullin concentration. The area under the curve is 0.75.
Discussion
We found that p[AM] was not associated with sepsis or survival in neonatal foals, but there was a 6‐fold increase in the median p[AM] in critically ill foals compared to healthy controls. Considering that the group of critically ill foals included approximately 20 different clinical diagnoses, we conclude that p[AM] may be a marker of health rather than an indicator of a specific clinical entity in neonatal foals. There was also no significant association between sepsis score and p[AM], which may indicate lack of a true relationship between sepsis and p[AM] in neonatal foals, or it may be associated with the fact that conventional categorization using a weighted sepsis score or positive blood culture for diagnosis of sepsis was insufficiently sensitive in this study population.
Clinical studies in humans demonstrate different degrees of p[AM] changes with various clinical diseases, with up to 50‐fold increases observed in septic patients compared to healthy individuals.21, 28, 33 The presence of lipopolysaccharide (LPS) and inflammatory cytokines described in human sepsis studies indicated increased AM gene expression in various tissues. During septic shock, p[AM] was found to increase more than in any other pathologic condition.34 Experimental studies on laboratory animals show that there is a progressive and significant increase in p[AM] starting approximately 2 hours after a septic insult.24, 30 Contrary to these observations, there was no significant difference in p[AM] between septic foals and nonseptic foals in the current study. The etiopathogenesis and disease course of equine neonatal sepsis may be different compared to sepsis in humans and laboratory animals. In addition, the current methods used to define sepsis in neonatal foals may be inadequate. Several foals in the sick nonseptic group did not meet the inclusion criteria for sepsis, but were considered septic by the attending clinician. Furthermore, nearly half of the critically ill foals were <2 hours of age, and may not have reached peak concentrations of p[AM] at the time of sample collection. The increase in p[AM] is progressive and plateaus approximately 20–30 hours after the onset of sepsis.24 Therefore, it is possible that serial measurements over the course of disease would be more sensitive in detecting sepsis and determining prognosis than a single measurement.
Although p[AM] is an early predictor of organ dysfunction and outcome in human sepsis,28 there were no significant difference in p[AM] in surviving versus nonsurviving foals. Significance was nearly reached (P = .051), and it is very possible that a difference would have been detected with a higher number of subjects. Furthermore, the overall survival rate was relatively high compared to previous studies and may have played a role in the lack of significance observed. Finally, foals subjected to euthanasia because of financial reasons were excluded from the study, but it is possible that foals euthanized because of poor prognosis would have recovered and survived to hospital discharge with continuous intensive care.
Plasma [AM] was evaluated within the following subgroups: FTPI, dystocia, Caesarian section, placentitis, HIE, and prematurity. None of these clinical entities was associated with a significantly different p[AM]. In clinical trials in humans, pregnancy complications (eg, preeclampsia, preterm delivery, low birth weight) are associated with significant changes in p[AM],35 whereas in infants with birth hypoxia, p[AM] is increased.36 Plasma [AM] has been linked to numerous other pathologic conditions including cardiovascular, renal, and lung diseases,22 but these were not evaluated in this study because of statistically inadequate sample size.
We found that septic foals had higher blood l‐lactate concentration, total serum bilirubin concentration, and higher incidence of FTPI than sick nonseptic foals, which is consistent with previous findings.2, 3, 16, 37 Septic foals also had a higher prevalence of toxic changes in neutrophils and band neutrophilia. Some of these findings are mutually inclusive because of categorization used in the weighted sepsis scoring system. Increased blood l‐lactate concentration is a reflection of anaerobic metabolism secondary to decreased tissue perfusion and is likely because of systemic inflammatory response syndrome‐associated hypotension and decreased fluid intake. In 1 study, admission l‐lactate concentration was associated with bacteremia and hospital survival.3 Sepsis‐associated cholestasis because of impaired bile transport at the sinusoidal and canalicular membranes by LPS and proinflammatory cytokines may explain hyperbilirubinemia in the septic foals.38, 39 Several studies have found a strong correlation between FTPI and sepsis, because inadequate colostral antibodies allow bacterial translocation to result in widespread bacteremia.9, 10, 11, 12 One report demonstrated that among 53 clinical and clinicopathologic admission variables, high sepsis score, FTPI, and low segmented neutrophil count were the most significant predictors of overall mortality among septic foals.12 Finally, band neutrophilia and toxic changes in neutrophils reflect the bone marrow response to acute and severe bacterial infection.
Surviving foals exhibited lower anion gap, total serum calcium concentration, blood l‐lactate concentration and MCV, and higher tCO2 compared to nonsurviving foals. Increased anion gap and decreased tCO2 concentration are likely reflections of increased l‐lactic acid concentration and uremia, which have been correlated with survival in a previous study.12 Increased total serum calcium concentrations in nonsurvivors may reflect altered kidney function, placentitis, or endocrinopathies.2, 3, 4, 37 Independent of p[AM], we found that survivors had longer hospitalization days and higher hospital charges. This may be because of the higher likelihood that severely affected foals may have deteriorated very rapidly and died or were euthanized soon after presentation to the hospital.
Receiver operating characteristic curves were constructed in an attempt to characterize test performance in identifying critical illness in foals (separate from sepsis), which has not been done previously. The sepsis score developed by Brewer and Koterba was reported to have a 93% sensitivity and 86% specificity to identify septic neonates in a particular study population in the southeastern United States.9 This was re‐evaluated by Corley and Furr and resulted in different results providing lower Sp (76%) and Se (67%).10 Currently, blood IgG concentration is considered a useful and practical method of health evaluation in newborn foals. In our study, 65% of foals diagnosed with critical illness had FTPI (Se = 0.65), which is numerically lower than the Se estimate for p[AM] >0.041 ng/mL (Se = 0.91). On this basis, p[AM] may serve as a superior predictor of the presence of illness compared to blood IgG concentration in neonatal foals. The sensitivity and specificity of blood IgG concentration compared to p[AM] in detecting perinatal illnesses would require further investigation.
One major limitation of this study is the lack of age‐matched controls. It is likely that p[AM] undergoes dynamic changes during the early neonatal period. Therefore, sequential measurements and strict age‐matched controls may have provided more accurate data for diagnosis and prognosis. Although p[AM] may be increased physiologically in the first few hours of life because of foaling stress, it likely decreases to normal concentrations by 24 hours of age as is observed with plasma cortisol concentrations.40 Thus, critically ill foals that presented at <24 hours of age may have demonstrated falsely increased p[AM]. Although it is unknown if the equine placenta is a source of AM as is observed in humans and bovids,41, 42 p[AM] in young neonates may have originated from the dam. However, plasma [AM] was not associated with age in this study. Interestingly, there was no difference in p[AM] in foals born to mares diagnosed with placentitis compared to those without placentitis. In addition, transportation of critically ill foals to the hospital may have contributed to stress‐induced increases in p[AM], whereas control foals were not transported. Transport time however was typically <2 hours given the close proximity of the majority of cases to the hospital, and this is shorter than the minimum time required for significant increases in p[AM] from baseline in experimentally induced sepsis.24 Furthermore, the contribution of p[AM] by the adrenal medulla in a stressful environment is likely much lower than the contribution from endothelial and vascular smooth muscle cells. Finally, it is possible that the upper range of p[AM] in healthy foals was affected by undetected illness.
In summary, p[AM] appears to be a promising marker of perinatal health in newborn foals, but p[AM] was not associated with sepsis, specific clinical entities, or survival based on this study population. Currently, the ELISA testing kit is designed to test approximately 40 samples at once and costs approximately $900. Therefore, it is cost‐prohibitive for a single patient. A single sample ELISA (ie, SNAP test) is needed to implement routine testing for clinical cases. Additional studies are warranted to evaluate age‐related changes in p[AM] as well as the prognostic value of serial p[AM] measurements in critically ill foals.
Acknowledgments
The study was not supported by a grant. The authors thank Dr Katherine MacGillivray, Dr Michele Frazer, and Dr Kim Sprayberry for sample collection and evaluation of critically ill foals presented to Hagyard Equine Medical Institute, Dr Robert Mealey at Washington State University and Megan Lundquist at Gumz Farms for providing control foal samples, and Anisa Dunham and Tina Elam for technical assistance.
Conflict of Interest: Dr Peter Constable is a Consulting Editor for Experimental Design and Statistics with the Journal of Veterinary Internal Medicine.
Results were presented, in part, at the 2013 American College of Veterinary Internal Medicine Forum in Seattle, WA and the 2013 Dorothy Havemeyer Neonatal Workshop in Saugerties, NY.
Footnotes
BBL SEPTI‐CHEK TSB (Tryptic Soy Broth), Becton Dickinson Microbiology Systems, Beckon Dickinson and Company, Cockeysville, MA
USCN Life Technologies, Wuhan, China. http://www.uscnk.com/manual/ELISA-Kit-for-Adrenomedullin-(ADM)-E90220Eq.pdf
Cell‐Dyn 3500R, Abbott Diagnostics, Abbott Park, IL
Accutrend, Roche Diagnostics, Raritan, NJ
SNAP Foal IgG Test, Idexx Laboratories, Inc, Westbrook, ME
Olympus AU400 Beckman Coulter, Inc, Brea, CA
Vitros 5,1 FS Chemistry System, Ortho‐Clinical Diagnostics, Inc, Rochester, NY
Stago STA Compact, Diamond Diagnostics, Holliston, MA
SAS 9.3, SAS Institute Inc, Cary, NC
References
- 1. Cohen ND. Causes of and farm management factors associated with disease and death in foals. J Am Vet Med Assoc 1994;204:1644–1651. [PubMed] [Google Scholar]
- 2. Hoffman AM, Staempfli HR, Willan A. Prognostic variables for survival of neonatal foals under intensive care. J Vet Intern Med 1992;6:89–95. [DOI] [PubMed] [Google Scholar]
- 3. Corley KT, Donaldson LL, Furr MO. Arterial lactate concentration, hospital survival, sepsis and SIRS in critically ill neonatal foals. Equine Vet J 2005;37:53–59. [DOI] [PubMed] [Google Scholar]
- 4. Hurcombe SD, Toribio RE, Slovis N, et al. Blood arginine vasopressin, adrenocorticotropin hormone, and cortisol concentrations at admission in septic and critically ill foals and their association with survival. J Vet Intern Med 2008;22:639–647. [DOI] [PubMed] [Google Scholar]
- 5. Stewart AJ, Hinchcliff KW, Saville WJ, et al. Actinobacillus sp. bacteremia in foals: Clinical signs and prognosis. J Vet Intern Med 2002;16:464–471. [DOI] [PubMed] [Google Scholar]
- 6. Gayle JM, Cohen ND, Chaffin MK. Factors associated with survival in septicemic foals: 65 cases (1988‐1995). J Vet Intern Med 1998;12:140–146. [DOI] [PubMed] [Google Scholar]
- 7. Lorenzo‐Figueras M, Pusterla N, Byrne BA, et al. In vitro evaluation of three bacterial culture systems for the recovery of Escherichia coli from equine blood. Am J Vet Res 2006;67:2025–2029. [DOI] [PubMed] [Google Scholar]
- 8. Wilson WD, Madigan JE. Comparison of bacteriologic culture of blood and necropsy specimens for determining the cause of foal septicemia: 47 cases (1978‐1987). J Am Vet Med Assoc 1989;195:1759–1763. [PubMed] [Google Scholar]
- 9. Brewer BD, Koterba AM. Development of a scoring system for the early diagnosis of equine neonatal sepsis. Equine Vet J 1988;20:18–22. [DOI] [PubMed] [Google Scholar]
- 10. Corley KTF, Furr MO. Evaluation of a score designed to predict sepsis in foals. J Vet Emerg Crit Care 2003;13:149–155. [Google Scholar]
- 11. Furr M, Tinker MK, Edens L. Prognosis for neonatal foals in an intensive care unit. J Vet Intern Med 1997;11:183–188. [DOI] [PubMed] [Google Scholar]
- 12. Peek SF, Semrad S, McGuirk SM, et al. Prognostic value of clinicopathologic variables obtained at admission and effect of antiendotoxin plasma on survival in septic and critically ill foals. J Vet Intern Med 2006;20:569–574. [DOI] [PubMed] [Google Scholar]
- 13. Rohrbach BW, Buchanan BR, Drake JM, et al. Use of a multivariable model to estimate the probability of discharge in hospitalized foals that are 7 days of age or less. J Am Vet Med Assoc 2006;228:1748–1756. [DOI] [PubMed] [Google Scholar]
- 14. Gold JR, Divers TJ, Barton MH, et al. Plasma adrenocorticotropin, cortisol, and adrenocorticotropin/cortisol ratios in septic and normal‐term foals. J Vet Intern Med 2007;21:791–796. [DOI] [PubMed] [Google Scholar]
- 15. Barsnick RJ, Hurcombe SD, Smith PA, et al. Insulin, glucagon, and leptin in critically ill foals. J Vet Intern Med 2011;25:123–131. [DOI] [PubMed] [Google Scholar]
- 16. Pusterla N, Magdesian KG, Mapes S, et al. Expression of molecular markers in blood of neonatal foals with sepsis. Am J Vet Res 2006;67:1045–1049. [DOI] [PubMed] [Google Scholar]
- 17. Kitamura K, Kangawa K, Kawamoto M, et al. Adrenomedullin: A novel hypotensive peptide isolated from human pheochromocytoma. Biochem Biophys Res Commun 1993;192:553–560. [DOI] [PubMed] [Google Scholar]
- 18. Kitamura K, Sakata J, Kangawa K, et al. Cloning and characterization of cDNA encoding a precursor for human adrenomedullin. Biochem Biophys Res Commun 1993;194:720–725. [DOI] [PubMed] [Google Scholar]
- 19. Hinson JP, Kapas S, Smith DM. Adrenomedullin, a multifunctional regulatory peptide. Endocr Rev 2000;21:138–167. [DOI] [PubMed] [Google Scholar]
- 20. Eto T. A review of the biological properties and clinical implications of adrenomedullin and proadrenomedullin N‐terminal 20 peptide (PAMP), hypotensive and vasodilating peptides. Peptides 2001;22:1693–1711. [DOI] [PubMed] [Google Scholar]
- 21. Gibbons C, Dackor R, Dunworth W, et al. Receptor activity‐modifying proteins: RAMPing up adrenomedullin signaling. Mol Endocrinol 2007;21:783–796. [DOI] [PubMed] [Google Scholar]
- 22. Nishikimi T, Yoshihara F, Mori Y, et al. Cardioprotective effect of adrenomedullin in heart failure. Hypertens Res 2003;26(Suppl):S121–S127. [DOI] [PubMed] [Google Scholar]
- 23. Wang P, Ba ZF, Cioffi WG, et al. The pivotal role of adrenomedullin in producing hyperdynamic circulation during the early stage of sepsis. Arch Surg 1998;133:1298–1304. [DOI] [PubMed] [Google Scholar]
- 24. Koo DJ, Zhou M, Chaudry IH, et al. The role of adrenomedullin in producing differential hemodynamic responses during sepsis. J Surg Res 2001;95:207–218. [DOI] [PubMed] [Google Scholar]
- 25. Lainchbury JG, Troughton RW, Lewis LK, et al. Hemodynamic, hormonal, and renal effects of short‐term adrenomedullin infusion in healthy volunteers. J Clin Endocrinol Metab 2000;85:1016–1020. [DOI] [PubMed] [Google Scholar]
- 26. Allaker RP, Zihni C, Kapas S. An investigation into the antimicrobial effects of adrenomedullin on members of the skin, oral, respiratory tract and gut microflora. FEMS Immunol Med Microbiol 1999;23:289–293. [DOI] [PubMed] [Google Scholar]
- 27. Isumi Y, Kubo A, Katafuchi T, et al. Adrenomedullin suppresses interleukin‐1beta‐induced tumor necrosis factor‐alpha production in Swiss 3T3 cells. FEBS Lett 1999;463:110–114. [DOI] [PubMed] [Google Scholar]
- 28. Ueda S, Nishio K, Minamino N, et al. Increased plasma levels of adrenomedullin in patients with systemic inflammatory response syndrome. Am J Respir Crit Care Med 1999;160:132–136. [DOI] [PubMed] [Google Scholar]
- 29. Nishio K, Akai Y, Murao Y, et al. Increased plasma concentrations of adrenomedullin correlate with relaxation of vascular tone in patients with septic shock. Crit Care Med 1997;25:953–957. [DOI] [PubMed] [Google Scholar]
- 30. Wang P, Zhou M, Ba ZF, et al. Up‐regulation of a novel potent vasodilatory peptide adrenomedullin during polymicrobial sepsis. Shock 1998;10:118–122. [DOI] [PubMed] [Google Scholar]
- 31. Lewis LK, Smith MW, Yandle TG, et al. Adrenomedullin(1‐52) measured in human plasma by radioimmunoassay: Plasma concentration, adsorption, and storage. Clin Chem 1998;44:571–577. [PubMed] [Google Scholar]
- 32. Bertone JJ, Jones RL, Curtis CR. Evaluation of a test kit for determination of serum immunoglobulin G concentration in foals. J Vet Intern Med 1988;2:181–183. [DOI] [PubMed] [Google Scholar]
- 33. Oncel MY, Dilmen U, Erdeve O, et al. Proadrenomedullin as a prognostic marker in neonatal sepsis. Pediatr Res 2012;72:507–512. [DOI] [PubMed] [Google Scholar]
- 34. Hirata Y, Mitaka C, Sato K, et al. Increased circulating adrenomedullin, a novel vasodilatory peptide, in sepsis. J Clin Endocrinol Metab 1996;81:1449–1453. [DOI] [PubMed] [Google Scholar]
- 35. Lenhart PM, Caron KM. Adrenomedullin and pregnancy: Perspectives from animal models to humans. Trends Endocrinol Metab 2012;23:524–532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Di Iorio R, Marinoni E, Lituania M, et al. Adrenomedullin increases in term asphyxiated newborns developing intraventricular hemorrhage. Clin Biochem 2004;37:1112–1116. [DOI] [PubMed] [Google Scholar]
- 37. Dembek KA, Onasch K, Hurcombe SD, et al. Renin‐angiotensin‐aldosterone system and hypothalamic‐pituitary‐adrenal axis in hospitalized newborn foals. J Vet Intern Med 2013;27:331–338. [DOI] [PubMed] [Google Scholar]
- 38. Moseley RH, Wang W, Takeda H, et al. Effect of endotoxin on bile acid transport in rat liver: A potential model for sepsis‐associated cholestasis. Am J Physiol 1996;271:G137–G146. [DOI] [PubMed] [Google Scholar]
- 39. Taboada J, Meyer DJ. Cholestasis associated with extrahepatic bacterial infection in five dogs. J Vet Intern Med 1989;3:216–221. [DOI] [PubMed] [Google Scholar]
- 40. Silver M. Prenatal maturation, the timing of birth and how it may be regulated in domestic animals. Exp Physiol 1990;75:285–307. [DOI] [PubMed] [Google Scholar]
- 41. Marinoni E, Di Iorio R, Letizia C, et al. Immunoreactive adrenomedullin in human fetoplacental tissues. Am J Obstet Gynecol 1998;179:784–787. [DOI] [PubMed] [Google Scholar]
- 42. Hayashi KG, Hosoe M, Sakumoto R, et al. Temporo‐spatial expression of adrenomedullin and its receptors in the bovine placenta. Reprod Biol Endocrinol 2013;11:62. [DOI] [PMC free article] [PubMed] [Google Scholar]