

Abstract
Background:
The use of complementary and alternative medicine (CAM) techniques has been growing. The National Center for Complementary and Alternative Medicine places therapeutic touch (TT) into the category of bio field energy. This literature review is aimed at critically evaluating the data from clinical trials examining the clinical efficacy of therapeutic touch as a supportive care modality in adult patients with cancer.
Methods:
Electronic databases (PubMed, Scopus, Scholar Google, and Science Direct) were searched from the year 1990 to 2015 to locate potentially relevant peer-reviewed articles using the key words therapeutic touch, touch therapy, neoplasm, cancer, and CAM. Additionally, relevant journals and references of all the located articles were manually searched for other potentially relevant studies.
Results:
The number of 334 articles was found on the basis of the key words, of which 17 articles related to the clinical trial were examined in accordance with the objectives of the study. A total of 6 articles were in the final dataset in which several examples of the positive effects of healing touch on pain, nausea, anxiety and fatigue, and life quality and also on biochemical parameters were observed.
Conclusion:
Based on the results of this study, an affirmation can be made regarding the use of TT, as a non-invasive intervention for improving the health status in patients with cancer. Moreover, therapeutic touch was proved to be a useful strategy for adult patients with cancer.
Keywords: therapeutic touch, touch therapy, cancer, literature review
1. INTRODUCTION
Cancer is a major health problem in the United States and other parts of the world (1). Cancer has been identified as a growing problem in the Middle East countries (2). Cancer is not a disease with a single cause, but rather a collection of different causes with various symptoms, treatments and prognoses (3).
Several aspects of the daily lives of cancer patients are affected which include financial situation, ability to work and family life, mood and temper, relationships with others, sleep and life quality (4). Cancer patients deal with various problems in different individual, family and social areas and also with the reduced life quality (5). Pain in patients with cancer is a stressful event which can affect patients’ life style as well as their feeling of satisfaction and comfort and also cause pain and discomfort, loss of control, fatigue, impaired quality of life and sexual activity, loss of interpersonal relationships and the concept of life, reduced performance, sleep and daily activities in them (6). Moreover, patients with cancer may also experience a feeling of anxiousness caused by the illness, treatment methods, etc., which has a negative impact on their treatment and recovery process, therefore, it is essential to be controlled and mitigated (7).
The main treatments for cancers include surgery, chemotherapy, hormone therapy, radiation therapy, and immunotherapy or biological therapy. Such treatments are used to destroy cancer cells and to restore health. Depending on the type of cancer, specialists use one or a combination of these treatments (8). Numerous studies have shown that a variety of complementary medicine can be influential in solving or reducing the problems caused by the disease in cancer patients (9). Complementary and alternative medicine (CAM) is a group of medical and health care systems, practices, and products that are not currently considered to be part of conventional medicine (10). The aim of this approach is to improve the health and quality of life as well as increased longevity by using natural approaches and different methods of alternative medicine based on clinical and research experiences (11). In a similar vein, the studies around the world indicate an increasing desire to control health through using CAM (12). According to the American Cancer Society (2011), complementary medicine for cancer includes methods that lead to the prevention, diagnosis and treatment of cancer. Some types of complementary therapies can help to relieve from some certain symptoms of cancer and side effects caused by the treatment, such as fatigue, anxiety and pain, or lead to an increased sense of well-being in a person (10). In the classification of complementary medicine, energy healing class includes treatments in which the energy emanates from the human body (biofield) or is originated from an external source such as therapeutic touch, Reiki, Qigong, polarity therapy, etc. (10)
The simplest definition of therapeutic touch (TT) is the use of hands on or near the body to help the treatment. TT is the interpretation of an old healing experience in the modern era (11). Special theories underlying TT include Dora Kunz’s model of human energy fields, electromagnetism and quantum physics, interpersonal psychology, Martha Roger’s theory of human unity, (relying on quantum and whole system theory, and Eastern science and philosophy) (13, 14). Rogers in the subject of “nursing: knowledge of human unity”, (1990), considers people as the continuous multi-dimensional energy fields that interact with the energy field of the environment. Touch therapists believe that humans are in energy fields and have open systems. Since the energy of therapists is not stopped in recipients, energy can be exchanged without any physical contact or with a very slight one (15). From the Rogers’ perspective, TT is an example of how professionals work to strengthen the integrity and perfection of humans and their environmental fields so that patients can reach an optimal health status (16). TT is a non-invasive nursing intervention which takes place by the hands and in the form of energy transfer (17). Jackson et al. by investigating twelve studies found that TT can be an acceptable method for reducing physical and psychological symptoms of patients with cancer (18).
Given the importance of TT in nursing and its potential positive outcomes in cancer patients, and also by taking into account the clinical evidence and the growing publication of articles in this field, this review study was conducted comprehensively to evaluate the results of TT clinical trials in patients with cancer.
2. METHODS
This review study was carried out by searching scientific databases including Scopus, Scholar Google, Science Direct, PubMed using key words of healing touch, therapeutic touch, touch therapy, cancer, neoplasm within the year 1990 to November, 2015. The MESH terms and keywords were exploded in the databases to the extent possible. Moreover, the reference sections in the selected articles were also manually searched.
The thematic relevance of studies was assessed by examining the titles and abstracts. In this study, the papers were selected on the basis of the availability of full texts of clinical trial articles in English, with the focus on the impact of TT in patients with cancer which had developed designs and methodologies.
Moreover, any trials with TT as part of their complex intervention, aimed at the development of methodologies for TT procedures without having any clinical outcomes, and those in which no data or statistical comparisons were reported, and healthy participants were also assessed, were excluded from the study. Furthermore, papers presented at seminars (due to the lack of having full texts and failure to complete the revision process for reviewing) were not also evaluated.
3. FINDINGS
The number of 334 articles was found on the basis of the key words, of which 317 articles were excluded after carrying out the investigation process and 17 articles related to the clinical trial were examined in accordance with the objectives of the study. Moreover, a total of 6 articles fully related to the field that had proper design and reliable data were ultimately selected and analyzed for the process of conducting the present study (Figure 1). The intervention, results and the methodology (Table 1) as well as the setting and participants (age, sex, stage of cancer, and site of cancer) were examined in each study for the process of extracting the data.
Figure 1.
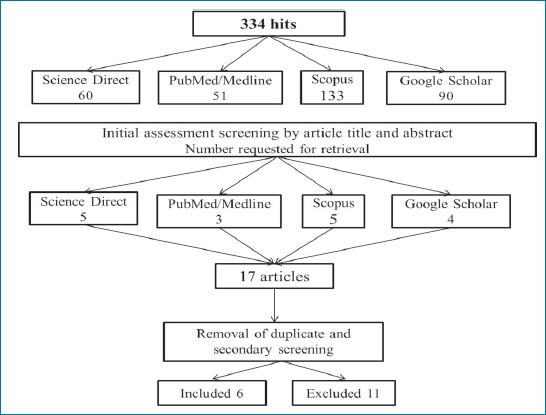
Literature search and retrieval flow diagram
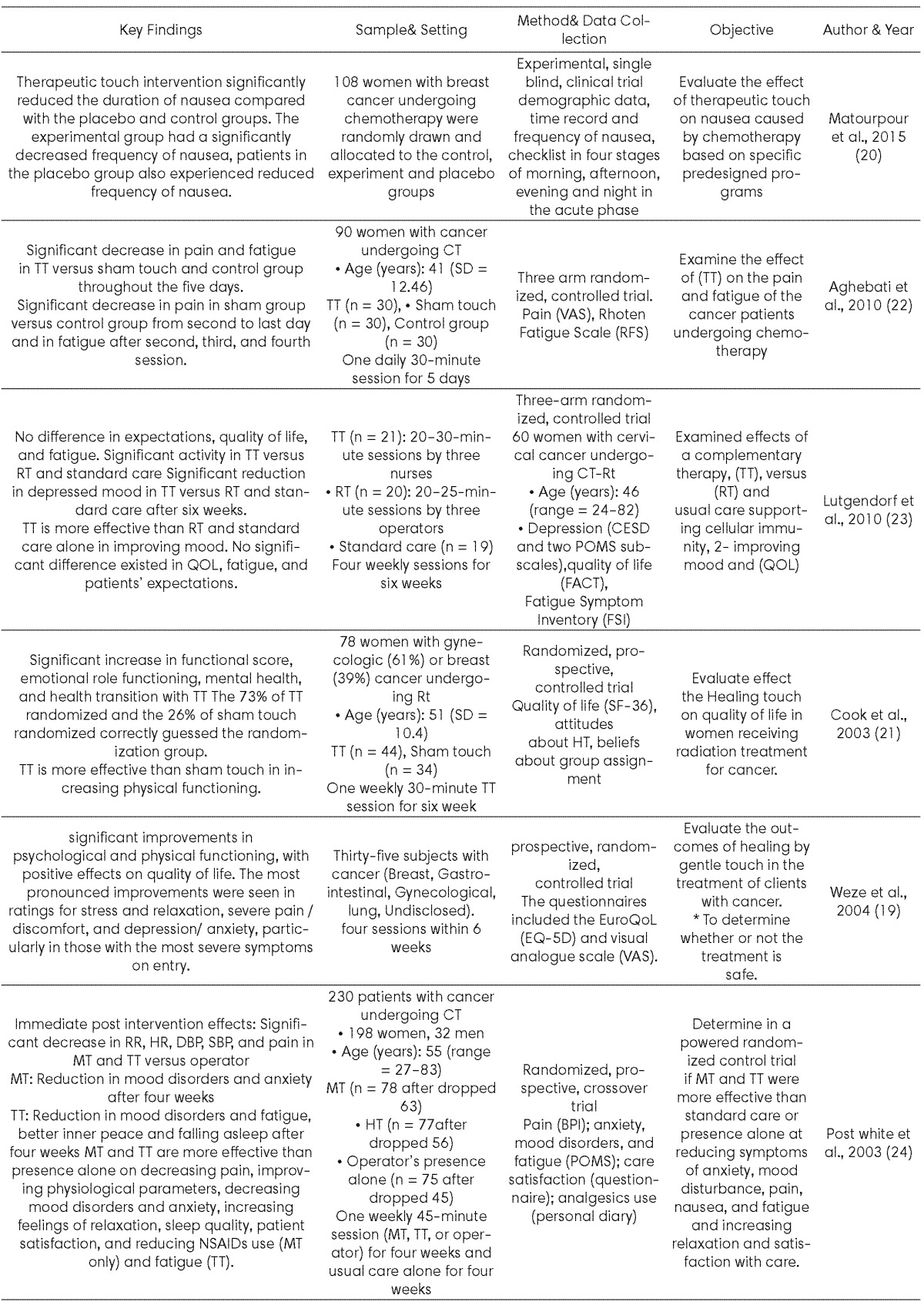
Table 1.
Summary of the basic features of the research articles included in the review. BFI - Brief Fatigue Inventory; BPI - Brief Pain Index; CT - chemotherapy; DBP - diastolic blood pressure; FACT-F - Functional Assessment of Cancer Therapy–Fatigue; FSI - Fatigue Symptom Inventory; HR - heart rate; MT - massage therapy; NSAIDS - nonsteroidal anti-inflammatory drugs; POMS - Profile of Mood States; QOL quality of life; RR - respiratory rate; Rt - radiotherapy; SBP - systolic blood pressure; TT - therapeutic touch;
Studies obtained by searching databases were organized and selected. The results indicated that most studies expressed a positive and significant association between therapeutic touch and dependent variables (nausea, pain, quality of life, fatigue and temper).
Participants and setting
The studies were undertaken in the United States (n= 3), the UK (n= 1) and Iran (n= 2) and were dated between 2003 and 2015. The sample size ranged from 35 to 164 participants. The participants were adults with an age range of 18 to 83 who had not a wide range of cancer diagnoses except in the study of Weze (breast, gastrointestinal, gynecological, lung, undisclosed) and in the study of Post-white with two breast and gynecology cancers. The total number of participants in this current review was 601, of which, 96% were females and 4% were males. All the participants in the studies varied in degree from the stage 1 up to the advanced, metastatic cancer.
All the studies had used control groups in order for comparison with the intervention and only the study by Weze was a single group study (19). The number of therapeutic touch sessions ranged from one session (20) to six sessions (21).
Outcome measures
A variety of measurement instruments were used to assess fatigue, pain, and nausea across the studies. To measure the fatigue, Aghabati (22) and Lutgendorf (23) respectively used Rhoten Fatigue Scale (RFS) and Fatigue Symptom Inventory (FSI).
To measure the pain interference and pain intensity, Post-white (24) used the Brief Pain Inventory (BPI). Other measurement instruments used for measuring pain included the Visual Analogue Scale (VAS) used by Aghabati and Weze and 36 -HRQOL short used by Cook.
Moreover, Postwhite used the Brief Nausea Index (BNI) to measure the nausea. However, Matourpour only made use of the check list.
In a single-blind clinical trial study conducted by Matourpour et al. TT was immediately performed after chemotherapy. The results showed that the nausea was significantly shorter for the intervention group compared to the placebo and the control groups. However, the TT intervention did not result in the reduced the severity of nausea in the intervention group. Moreover, the number of incidence of nausea in the acute phase was also significant in the intervention group in comparison with the other two groups (20).
Post-white et al. in their study investigated the effects of massage therapy (MT) and TT compared to the standard care on inducing relaxation and reducing symptoms in 203 patients. The results demonstrated a greater relaxed feeling and short-term pain reduction, along with less disturbed mood and fatigue in the patients in the intervention group with the touch and massage therapies compared to the patients in the control group. The researchers concluded that the use of various methods of alternative medicine to relieve pain in patients with chronic pain may be more beneficial than relying on a single approach (24).
Moreover, Cook et al. in the study reported the reduction in pain and improvement in the physical function. In this study, the intervention group had a greater improvement than the control group in terms of quality of life. Additionally, the improvement in physical function, pain and vitality was observed in the intervention group compared to the control group (21). The results of this study indicate that therapeutic touch can cause the pain reduction in the breast and oncology cancers. Furthermore, the results of a study by Weze et al. indicated positive effects of therapeutic touch on reducing pain in cancer patients (19).
4. DISCUSSION
In the studies on cancer patients, significant findings have been reported. Even in the absence of significant results in outcomes studied, therapeutic touch recipients often reported subjective benefits, including improved mood, well-being, and interpersonal relationships, reduction in pain, nausea, anxiety, and fatigue, increase in vitality, and satisfaction with the touch therapy. In a descriptive study on patients with fibromyalgia, Diener et al. found varied responses to TT treatments. Moreover, the participants reported relaxation, spiritual uplifting, and greater mobility (25).
In addition, Meehan et al. in their study also indicated that therapeutic touch can be used as a supplement in relieving pain in patients after the surgery (26). Evanoff by investigating the effect of therapeutic touch on the degree of pain in patients with osteoarthritis of the knee came to the conclusion that therapeutic touch can reduce pain and improve function in patients (27). The results obtained from four studies on elderly people proved to be positive regardless of the diagnosis. Physical status such as pain, appetite, and sleep were enhanced; behavioral markers such as worry, outbursts, and restlessness were decreased; and behaviors that made the jobs of the staff easier, such as compliance with daily routine, decreased medications, and increased functional ability, all supported the use of TT for this population (28).
Significant decreases in pain, nausea, and anxiety were immediately observed following the intervention on post-operative days one and two, and in pain and anxiety on the post-operative day three compared with the pre-intervention levels. These findings indicated that the TT intervention was feasible and acceptable to patients undergoing bariatric surgery, and significantly improved pain, nausea, and anxiety in them (29). Coakley believes that the energy therapy can be used to improve various symptoms in patients with cancer. In a similar vein, studies have also shown that such holistic interferences are greatly demanded by the patients (16). The goal of TT is to restore balance, harmony, and a sense of well-being. TT is based on a compassionate intention directed through light touch or placement of the hands just off the body which is often performed by nurses (30). Various mechanisms have been proposed to enhance the TT effectiveness. Physiologically, bio-field therapies such as TT appear to affect the autonomic nervous system, altering the high frequency to low frequency ratio of heart rate variability, reflecting a greater parasympathetic tone and decreasing the sympathetic activation (31). Some studies suggested that biofield healing may decrease stress and enhance immune function (30, 32). It is also possible for the relaxation response to help explain the effects of TT (33).
The underlying assumption of TT is that human beings are systems of energy and that the energy field extends a few inches beyond the skin’s surface. There exist three distinct phases of intervention including (a) nurses becoming aware of the helpfulness of TT for their patients, (b) the assessment phase, where a nurse uses slow, gentle, sweeping movement of their hands starting from the patient’s head and proceeding to the patient’s feet to assess the presence of any signs of energy dissymmetry, and (c) the un-ruffling phase, where a nurse uses symmetric movement of their hands over the energy field of the patient with the goal of smoothing out or relieving energy congestion (34). Therapeutic touch is a standardized biofield therapy that uses gentle touch and movements in the patient’s “energy field” with the goal of restoring balance in the patient’s energy system and strengthening the patient’s “healing capacity”(35). TT has been shown to increase well-being in cervical and breast cancer patients during radiation (21, 23) and to reduce distress and fatigue during chemotherapy (24).
TT has also a series of benefits in reducing anxiety, increasing relaxation, decreasing pain, diminishing depression, and increasing a sense of well-being (36, 37).
Although treatment for cancer is recognized as stressful and impairing to quality of life, few TT interventions have been shown to be efficacious in lessening treatment-related symptoms (38). This method allows instructors both to provide technical skills and to build a relationship with the patient so that professionals’ gratification and motivation will be improved. The ease of training and feasibility in multiple settings without the need for special tools also make touch therapy a good option for many patients and caregivers. Thus, TT might be a convenient measure for patients undergoing cancer treatment.
The current study indicates that some limitations are notable in the conducted studies. None of the studies included in this review provided a clear rationale for the treatment specificity or duration. Moreover, the studies showed substantial differences in frequency of interventions which were performed every day, once a week, and twice a week. The length of treatment sessions ranged from 10–40 minutes; however, the average time was usually from 10–45 minutes (34). In the most reviewed studies, the role of some intervening variables such as physical activity, psychological problems and gender was overlooked, or not mentioned. Moreover, methodology differences are observable in the reviewed studies, the most important of which is the failure to provide any credible references to indicate the number of TT sessions. The length of the study ranged from one day to six weeks; however, the average length was 4 - 6 weeks (11, 34)
Most samples selected in the studies were diagnosed with breast cancer which was probably due to their greater prevalence and better uniformity in the designs of the studies. Moreover, given the high incidence of cancer, it is necessary to investigate the TT function and impacts on individuals and men with various types of cancer. Participants generally reported the improved quality of life physically, emotionally, relationally, and spiritually. Studying the different research in the field of TT revealed that none of the studies had pointed to any considerable side effects. However, some patients with chronic diseases were reported to have light-headedness, dizziness, irritability following the bio-field therapy (39).
Strengths and limitations of this review
This study was conducted in the form of a literature review. A search strategy was created with the help of an information specialist. To reduce subjective selection bias, the inclusion process and the quality of the articles were carefully assessed by four independent researchers. However, there are some limitations to this study. First, the searches were limited to the period between 1990 and early 2015. Second, there was a risk of language bias as the papers in any language other than English were excluded. Third, there was a possibility for selecting only positive research due to the publication bias. Therefore, further studies are required to be conducted to reduce such limitations.
5. CONCLUSION
Based on the results of this review, an affirmation can be made regarding the use of therapeutic touch as a non-invasive intervention for improving the health status in patients with cancer. It also seems that this method can be used as a safe method in the management of physical function, pain, anxiety, and nausea in cancer patients. Training TT to those interested to the field can possibly be of great help in caring for cancer patients and reducing complications of the disease. However, further studies are needed to explore the impact of TT on additional clinically relevant measures.
Acknowledgments
The paper is derived from the PhD thesis of the first author in nursing International Branch of Shahid Beheshti University of Medical Sciences, Tehran, Iran.
REFERENCES
- 1.Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics 2014. CA Cancer J Clin. 2014;64(1):9–29. doi: 10.3322/caac.21208. [DOI] [PubMed] [Google Scholar]
- 2.Daher M. Opioids for cancer pain in the Middle Eastern countries: a physician point of view. J Pediatr Hematol Oncol. 2011;33:S23–S8. doi: 10.1097/MPH.0b013e3182121a0f. [DOI] [PubMed] [Google Scholar]
- 3.Brunner LS, Smeltzer SCC, Bare BG, Hinkle JL, Cheever KH. Brunner & Suddarth’s Textbook of Medical-surgical Nursing: Suzanne C. Smeltzer [et al.]: Wolters Kluwer Health; 2014. [Google Scholar]
- 4.Moradian S, Aledavood S, Tabatabaee A. Iranian cancer patients and their perspectives: a qualitative study. European Journal of Cancer Care. 2012;21(3):377–83. doi: 10.1111/j.1365-2354.2011.01293.x. [DOI] [PubMed] [Google Scholar]
- 5.Rassouli M, Sajjadi M. Palliative Care in Iran Moving Toward the Development of Palliative Care for Cancer. American Journal of Hospice and Palliative Medicine. 2014 doi: 10.1177/1049909114561856. 1049909114561856. [DOI] [PubMed] [Google Scholar]
- 6.Paice JA, Ferrell B. The management of cancer pain. CA Cancer J Clin. 2011;61(3):157–82. doi: 10.3322/caac.20112. [DOI] [PubMed] [Google Scholar]
- 7.Anderson JG, Taylor AG. Biofield Therapies and cancer pain. Clin J Oncol Nurs. 2012;16(1):43–8. doi: 10.1188/12.CJON.43-48. [DOI] [PubMed] [Google Scholar]
- 8.Price P, Sikora K. Treatment of Cancer. Sixth Edition. CRC Press; 2014. [Google Scholar]
- 9.De Vita V, Lawrence T. De Vita, Hellman, and Rosenberg’s Cancer: Principles and Practice of Oncology. 10 ed. Editorial Lippincott Williams and Wilkins; 2015. [Google Scholar]
- 10.National Center for Complementary and Alternative Medicine, National Institutes of Health. 2012. Available at: http://nccam.nih.gov/health/whatiscamccessed . [DOI] [PubMed]
- 11.Lindquist R, Snyder M, Tracy MF. Complementary & alternative therapies in nursing. 7 ed. Springer Publishing Company; 2014. [Google Scholar]
- 12.Sadeghi R, Heidarnia M, Zaghari Tm, Rassouli M, Soori H. Applying acupuncture for pain relief: qualitative study. Complementary medicine journal of faculty of nursing & midwifery. 2012;2(3):61–73. [Google Scholar]
- 13.Krieger D. Dolores Krieger, RN, PhD healing with therapeutic touch. Interview by Bonnie Horrigan. Altern Ther Health Med. 1998;4(1):86. [PubMed] [Google Scholar]
- 14.Rogers ME. An introduction to the theoretical basis of nursing. AJN The American Journal of Nursing. 1971;71(10):2026–7. [Google Scholar]
- 15.Meehan TC. Therapeutic touch as a nursing intervention. J Adv Nurs. 1998;28(1):117–25. doi: 10.1046/j.1365-2648.1998.00771.x. [DOI] [PubMed] [Google Scholar]
- 16.Coakley AB, Barron AM, editors. Energy therapies in oncology nursing. Semin Oncol Nurs. Elsevier. 2012 doi: 10.1016/j.soncn.2011.11.006. [DOI] [PubMed] [Google Scholar]
- 17.Kelly AE, Sullivan P, Fawcett J, Samarel N, editors. Therapeutic Touch, Quiet Time, and Dialogue: Perceptions of Women With Breast Cancer. Oncol Nurs Forum. Onc Nurs Society. 2004 doi: 10.1188/04.onf.625-631. [DOI] [PubMed] [Google Scholar]
- 18.Jackson E, Kelley M, McNeil P, Meyer E, Schlegel L, Eaton M. Does therapeutic touch help reduce pain and anxiety in patients with cancer? Clin J Oncol Nurs. 2008;12(1):113–20. doi: 10.1188/08.CJON.113-120. [DOI] [PubMed] [Google Scholar]
- 19.Weze C, Leathard HL, Grange J, Tiplady P, Stevens G. Evaluation of healing by gentle touch in 35 clients with cancer. Eur J Oncol Nurs. 2004;8(1):40–9. doi: 10.1016/j.ejon.2003.10.004. [DOI] [PubMed] [Google Scholar]
- 20.Matourypour P, Zare Z, Mehrzad V, Musarezaie A, Dehghan M, Vanaki Z. An investigation of the effects of therapeutic touch plan on acute chemotherapy-induced nausea in women with breast cancer in Isfahan, Iran 2012-2013. Journal of education and health promotion. 2015;4(61) doi: 10.4103/2277-9531.162380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Cook C, Guerrerio J, Slater VE. Healing touch and quality of life in women receiving radiation treatment for cancer: a randomized controlled trial. Altern Ther Health Med. 2003;10(3):34–41. [PubMed] [Google Scholar]
- 22.Aghabati N, Mohammadi E, Pour Esmaiel Z. The effect of therapeutic touch on pain and fatigue of cancer patients undergoing chemotherapy. Evid Based Complement Alternat Med. 2010;7(3):375–81. doi: 10.1093/ecam/nen006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lutgendorf SK, Mullen-Houser E, Russell D, DeGeest K, Jacobson G, Hart L, et al. Preservation of immune function in cervical cancer patients during chemoradiation using a novel integrative approach. Brain Behav Immun. 2010;24(8):1231–40. doi: 10.1016/j.bbi.2010.06.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Post-White J, Kinney ME, Savik K, Gau JB, Wilcox C, Lerner I. Therapeutic massage and healing touch improve symptoms in cancer. Integr Cancer Ther. 2003;2(4):332–44. doi: 10.1177/1534735403259064. [DOI] [PubMed] [Google Scholar]
- 25.Diener D. A pilot study of the effect of chakra connection and magnetic unruffle on perception of pain in people with fibromyalgia. Healing Touch Newsletter, Research Edition. 2001;1(3):7–8. [Google Scholar]
- 26.Meehan TC. Therapeutic touch and postoperative pain: a Rogerian research study. Nurs Sci Q. 1993;6(2):69–78. doi: 10.1177/089431849300600206. [DOI] [PubMed] [Google Scholar]
- 27.Evanoff A, Newton WP. Therapeutic touch and osteoarthritis of the knee. J Fam Pract. 1999;48(1):11–2. [PubMed] [Google Scholar]
- 28.Wardell DW, Weymouth KF. Review of studies of healing touch. J Nurs Scholarsh. 2004;36(2):147–54. doi: 10.1111/j.1547-5069.2004.04012.x. [DOI] [PubMed] [Google Scholar]
- 29.Anderson JG, Suchicital L, Lang M, Kukic A, Mangione L, Swengros D, et al. The effects of Healing Touch on pain, nausea, and anxiety following bariatric surgery: a pilot study. EXPLORE: The Journal of Science and Healing. 2015;11(3):208–16. doi: 10.1016/j.explore.2015.02.006. [DOI] [PubMed] [Google Scholar]
- 30.Wilkinson DS, Knox PL, Chatman JE, Johnson TL, Barbour N, Myles Y, et al. The clinical effectiveness of healing touch. The Journal of Alternative & Complementary Medicine. 2002;8(1):33–47. doi: 10.1089/107555302753507168. [DOI] [PubMed] [Google Scholar]
- 31.Sneed NV, Olson M, Bubolz B, Finch N. Influences of a relaxation intervention on perceived stress and power spectral analysis of heart rate variability. Prog Cardiovasc Nurs. 2001;16(2):57–79. doi: 10.1111/j.0889-7204.2001.00581.x. [DOI] [PubMed] [Google Scholar]
- 32.Taylor B. The effects of healing touch on the coping ability, self esteem and general health of undergraduate nursing students. Complement Ther Nurs Midwifery. 2001;7(1):34–42. doi: 10.1054/ctnm.2000.0518. [DOI] [PubMed] [Google Scholar]
- 33.Hoffman JW, Benson H, Arns PA, Stainbrook GL, Landsberg G, Young JB, et al. Reduced sympathetic nervous system responsivity associated with the relaxation response. Science. 1982;215(4529):190–2. doi: 10.1126/science.7031901. [DOI] [PubMed] [Google Scholar]
- 34.Gonella S, Garrino L, Dimonte V. Biofield therapies and cancer-related symptoms: A review. Clin J Oncol Nurs. 2014;18:568–76. doi: 10.1188/14.CJON.568-576. [DOI] [PubMed] [Google Scholar]
- 35.Mentgen JL. Healing touch. The Nursing Clinics of North America. 2001;36(1):143–58. [PubMed] [Google Scholar]
- 36.Kessler RC, Soukup J, Davis RB, Foster DF, Wilkey SA, Van Rompay MI, et al. The use of complementary and alternative therapies to treat anxiety and depression in the United States. Am J Psychiatry. 2001;158(2):289–94. doi: 10.1176/appi.ajp.158.2.289. [DOI] [PubMed] [Google Scholar]
- 37.Hutchison CP, D’Alessio B, Forward JB, Newshan G. Body-mind-spirit: Healing touch: An energetic approach. AJN The American Journal of Nursing. 1999;99(4):43–8. [PubMed] [Google Scholar]
- 38.Matthews M, Glackin M, Hughes C, Rogers K. Who accesses complementary therapies and why?: An evaluation of a cancer care service. Complement Ther Clin Pract. 2015;21(1):19–25. doi: 10.1016/j.ctcp.2014.09.005. [DOI] [PubMed] [Google Scholar]
- 39.So PS, Jiang Y, Qin Y. Touch therapies for pain relief in adults. Cochrane Database Syst Rev. 2008:4. doi: 10.1002/14651858.CD006535.pub2. [DOI] [PubMed] [Google Scholar]