

Abstract
Aims
To assess whether primary sector healthcare in the form of chiropractic care is cost-effective compared with self-management in patients with musculoskeletal chest pain, that is, a subgroup of patients with non-specific chest pain.
Methods and results
115 adults aged 18–75 years with acute, non-specific chest pain of musculoskeletal origin were recruited from a cardiology department in Denmark. After ruling out acute coronary syndrome and receiving usual care, patients with musculoskeletal chest pain were randomised to 4 weeks of community-based chiropractic care (n=59) or to a single information session aimed at encouraging self-management as complementary to usual care (n=56). Data on resource use were obtained from Danish national registries and valued from a societal perspective. Patient cost and health-related quality-adjusted life years (QALYs; based on EuroQol five-dimension questionnaire (EQ-5D) and Short Form 36-item Health Survey (SF-36)) were compared in cost-effectiveness analyses over 12 months from baseline. Mean costs were €2183 lower for the group with chiropractic care, but not statistically significant (95% CI −4410.5 to 43.0). The incremental cost-effectiveness ratio suggested that chiropractic care was cost-effective with a probability of 97%, given a threshold value of €30 000 per QALY gained. In both groups, there was an increase in the health-related quality of life, and the mean increases were similar over the 12-month evaluation period. The mean differences in QALYs between the groups were negligible.
Conclusions
Chiropractic care was more cost-effective than self-management. Therefore, chiropractic care can be seen as a good example of a targeted primary care approach for a subgroup of patients with non-specific chest pain.
Trial registration number
Key questions.
What is already known about this subject?
Patients with non-specific chest pain feel equally or more disabled than patients with cardiac chest pain and are a major burden on healthcare resources.
Patients with non-specific chest pain are an established subset of patients who present to chest pain units, and musculoskeletal problems are well recognised as a potential cause of chest pain.
There are few interventions that offer care in a cost-effective manner for this patient group.
What does this study add?
In terms of health-related quality of life, primary care in the form of chiropractic care has similar effectiveness as self-management in patients with musculoskeletal chest pain.
Community-based chiropractic care is more cost-effective than self-management as it is associated with fewer hospital admissions and lower healthcare costs.
How might this impact on clinical practice?
The results indicate that close contact with a primary care provider lowers the rate of hospitalisation, which is not achieved when patients are left to manage their condition on their own. A multifaceted, person-centred approach targeting both psychosocial and biomechanical aspects of chest pain is recommended.
Introduction
Over the past 25 years, hospital admissions for suspected acute coronary syndrome have increased in many countries.1 2 The majority of these patients are diagnosed with angina pectoris or as suffering from non-specific chest pain (NSCP), that is, coronary disease is not the cause of their pain. NSCP may account for up to 80% of visits to rapid access chest pain clinics because of new episodes of chest pain.3 4
In 2013, the mean annual societal cost per NSCP patient was estimated at ∼€10 000.5 Given that 15 million patients are admitted to a hospital with NSCP annually in the USA and Europe,6 7 the total costs exceed €150 billion annually, which is similar to the costs incurred by society for patients diagnosed with acute myocardial infarction and angina pectoris.5 6 8 9 Hospital admission days account for 70–90% of the initial healthcare costs,6 10 but patients with NSCP continue to incur costs because they often experience repeated episodes of pain,11 12 that result in further admissions,5 8 decreased quality of life,11 12 sick leave and lost productivity.5 In addition, they seek care from a range of healthcare providers outside the hospital setting3 5 12 13 at a level that exceeds those of patients who are diagnosed with chest pain associated with cardiac disease.12 The potential benefit of primary care sector healthcare and the related costs for this patient group are rarely investigated in randomised trials.14
Patients with NSCP are an established subset of patients who present to chest pain units, and musculoskeletal problems are well recognised as potential causes of chest pain, with an estimated prevalence of 10–30%15–17 among patients with NSCP. In 2012, we reported clinical outcomes of a pragmatic, randomised clinical trial evaluating the relative effectiveness of usual care in combination with a primary sector care approach (chiropractic care) compared with usual care in combination with a minimal intervention (self-management). This was in patients presenting to a Danish university hospital with an episode of acute chest pain that was first diagnosed as NSCP and subsequently diagnosed as musculoskeletal chest pain.18 19 The chiropractic care group did significantly better than the self-management group, in terms of global perceived effect after 4 weeks of treatment and pain intensity after 12 weeks; however, there were no significant differences between groups after 52 weeks. The aim of the current analysis was to evaluate the 1-year cost-effectiveness of the two approaches in terms of healthcare utilisation, medication and quality of life using self-report questionnaires and Danish national registry-based resource use data.
Methods
The design and methods of the randomised clinical trial have previously been reported.18–20 A brief overview is provided here.
Settings and participants
The trial was conducted in an emergency cardiology department at a Danish 1200-bed, urban, university hospital and at four community-based chiropractic clinics from 6 August 2006 to 31 March 2008. The study was approved by the Regional Ethics Committee of Vejle and Funen Counties, Denmark (approval number #VF 20060002) and registered at ClinicalTrials.gov (identification number NCT00462241). All patients presenting at the emergency unit with an episode of acute chest pain underwent the routine diagnostic procedures performed by specialist cardiology nurses under cardiologist supervision. When a patient was discharged from the unit, the study clinician (MJS) screened the patient's records to assess eligibility for inclusion in the trial. The eligibility criteria are presented in box 1.
Box 1. Eligibility criteria.
Inclusion criteria
▸ Participants should have had a primary complaint of acute chest pain of <7 days' duration, but not have had a diagnosis of acute coronary syndrome or another definite cardiac or medical diagnosis causing the chest pain, should be aged 18–75 years, be a resident of the local county and be able to read and understand Danish. In addition, participants should have undergone diagnostic procedures to rule out acute coronary syndrome and should not have shown significant comorbidity or contraindications for spinal manipulative therapy.
Exclusion criteria
▸ Previous acute coronary syndrome, prior percutaneous coronary intervention or coronary artery bypass grafting, inflammatory joint disease, insulin-dependent diabetes, fibromyalgia, malignant disease, major osseous anomaly, osteoporosis, apoplexy or dementia, inability to cooperate, and pregnancy. In each case, the cause of exclusion was noted.
Trial procedures
After providing written informed consent, the participants were assessed at baseline by the study clinician using a standardised and previously validated examination protocol.20–22 The baseline examination protocol consisted of four main components: patient self-report questionnaires, a detailed case history, a general health examination, and systematic palpation of the chest wall and spine. Patients were classified as having musculoskeletal chest pain if the pain was deemed to be caused by mechanical joint and muscle dysfunction related to C4-T8 somatic structures of the spine and chest wall as established by palpation.20 Only patients with a diagnosis of musculoskeletal chest pain were eligible for randomisation. Demographic and clinical information was collected through patient self-report questionnaires and checklists used by the study clinician. Detailed trial procedures, sample size estimation, randomisation and blinding have been described elsewhere.18–20
Description of interventions
At the time of discharge from the Department of Cardiology, both groups received usual care, which typically consisted of a brief (5 min) consultation with the attending cardiologist. In the case of persistent or recurrent pain, the patients were instructed to consult their general practitioner (GP).
Participants were randomised into one of two management strategies: chiropractic care or self-management.
Chiropractic care
Chiropractic consultations were offered as musculoskeletal healthcare management in the primary care sector. In Denmark, chiropractors are an integrated part of the primary healthcare sector and licensed to act as first healthcare entry for patients with musculoskeletal symptoms under the Danish National Health Insurance system.
Participants in the chiropractic care group were assigned to one of eight experienced chiropractors in their local community. Each chiropractor applied a pragmatic, individually tailored management strategy based on the age, physical condition and particular problem of each patient. A wide range of manual therapies and exercises were given, adapted to each individual patient.18 Furthermore, time was dedicated to address the patient's concerns and to give advice. A maximum of 10 20 min treatment sessions one to three times per week for 4 weeks was allowed. If the patient became pain-free sooner, the treating chiropractor could discharge the patient.
Self-management
Immediately following allocation to the self-management group, the study clinician (MJS) gave each participant a 15 min consultation consisting of reassurance and advice to address the patient's concerns and to promote self-management. Participants were told that their chest pain had a benign, self-limiting course and were given two to three home exercises.
Healthcare utilisation, medication and associated costs
The analysis was conducted from a societal perspective, that is, all relevant costs and effects were measured regardless of who paid the costs and who benefited from the effects. We included direct costs and effects. The included categories of costs are presented in figure 1. Danish national registries use unique, personal identification numbers issued to all Danish residents to record data about hospital contacts and primary sector healthcare utilisation.23–25 In Denmark, the cost of healthcare utilisation is primarily financed by the Danish National Health Service. Exceptions to this are chiropractic, physiotherapy and psychology consultations, which incur some additional out-of-pocket expenses paid by the patient. Use of prescriptive medication is registered in the Odense Pharmaco-Epidemiological Database using international Anatomical Therapeutic Chemical Classification System codes (ATC), which contain information on the dispensing of all medications prescribed by a physician and subsidised by the national health insurance at any pharmacy.26 Patient self-report questionnaires about clinical outcomes and resource use that were not available from the national registries were collected at baseline and 4, 12 and 52 weeks after baseline. Patients were asked to describe their use of complementary and alternative medicine (CAM) and non-prescriptive drugs during the previous 3 months.
Figure 1.
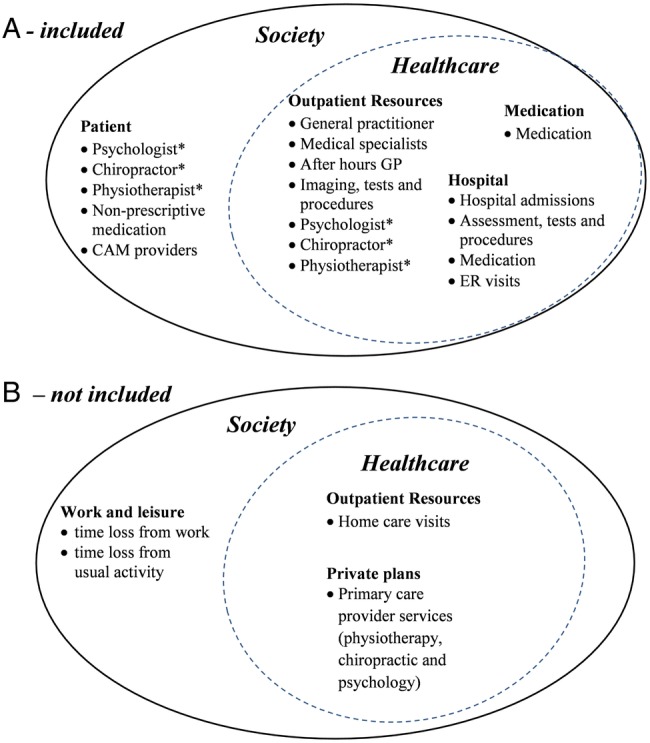
(A) The types of costs that were included in the analysis, and (B) the types of costs that were not included (modified from Torrance et al27). *Indicates that the service is paid by the patient, but partially reimbursed by the National Danish Health insurance. CAM, complementary and alternative medicine; ER, emergency room; GP, general practitioner.
Direct costs included: the intervention costs (chiropractic care and the self-management sessions); additional visits to mainstream healthcare and CAM providers; prescriptive and non-prescriptive drugs; and hospital contacts. Valuation of a chiropractic intervention was based on standard fees according to the national collective agreement between the Danish Chiropractic Association and the Danish National Health Service. A self-management session was valued as being equivalent to one standard chiropractic consultation. Costs of prescriptive medication were calculated on the basis of prices charged by the pharmacies (excluding VAT), and the costs of primary healthcare provider and hospital contacts were based on the standard patient fees paid by the Danish National Health Service. All monetary values are presented in euros at 2014 cost levels, and therefore costs were uplifted to August 2014 price levels using the Consumer Price Index maintained by Statistics Denmark.
Health-related quality of life measures
General health status was measured using the Medical Outcomes Study Short Form 36-item Health Survey (SF-36, v1US). The SF-36 is a generic health status instrument covering both physical and mental aspects of health.28 29 The six-dimensional health status short form (SF-6D) is a health status classification system that can be generated from the SF-36 responses. It is composed of six multilevel dimensions: physical functioning, role limitations, social functioning, pain, mental health and vitality. A scoring programme has been developed to transform the SF-36 responses into a single preference-weighted quality-of-life index (QoL-index) score (SF-6D); the revised Brazier algorithm being used here to score the SF-36 data into the score index on a 0–1 scale.30 The algorithm provided scores ranging from 0.160 to 1.0.31 32
The EuroQol five-dimension questionnaire (EQ-5D) is a generic utility-based health status instrument comprising five dimensions of health (mobility, self-care, usual activities, pain/discomfort, anxiety/depression), which in its original version are each divided into three levels of severity.33 34 In this study, we used five levels of severity in each dimension, as suggested by Kind and Macran35 and subsequently tested by Janssen et al.36 37 Patients were asked to describe their health status as of ‘today’. The recommended Danish scoring algorithm was applied to calculate an index score, with 0 denoting death and 1 denoting perfect health.38 This algorithm provided scores ranging from −0.624 to 1.0. The EQ-5D instrument includes health states worse than death and assigns to these values lower than 0 (negative values).39
Statistical analysis
Baseline characteristics were reported as percentages for binary variables, and as mean values and SDs for continuous variables. Multiple imputations based on fully conditional specifications were used to impute missing outcome data at follow-up. For each analysis, the imputations were based on a model that included the outcome variables at all time points and group allocation. By multiple imputation, five imputed data sets were created, each of which was analysed separately. The results of the five analyses were pooled using Rubin's rules.40
Mean values and SDs were computed for each of the two QoL-index outcome measures in each treatment group. The difference in mean values was assessed using change scores adjusted for baseline differences using analysis of covariance and reported with 95% CIs. The incremental health-related quality of life (HRQoL) was calculated as the mean difference-in-difference in the QoL-index between the intervention groups. Quality-adjusted life years (QALYs) were also calculated based on the two QoL-indices. The 1-year QALYs were calculated by multiplying the utilities with the amount of time a patient spent in a particular health state. Transitions between health states were linearly interpolated.
Healthcare utilisation was reported as the number and proportion of patients visiting a healthcare provider group or using a service, total and mean number of visits or services, and associated total and mean costs. The two groups were compared at follow-up using χ2 test for proportions and t test (two-sided) for total and mean number of visits. Differences in mean costs per user and per patient in the intervention groups, respectively, were computed using pairwise comparisons of means and reported together with 95% CIs.
To facilitate comparison between self-report and registry-based costs, costs from the self-report questionnaires were extrapolated to estimate annual costs. Data from the 12 weeks follow-up were extrapolated forwards to estimate the first 26 weeks, and data from the 12-month follow-up were extrapolated backwards to estimate the last 26 weeks.
The average costs per person and treatment effects, as well as the incremental cost-effectiveness ratio between the two groups were calculated and graphically displayed in the cost-effectiveness plane using bias-corrected bootstrapping with 1000 repetitions. Acceptability curves were constructed to show the probability that the chiropractor intervention was cost-effective at different threshold values for a QALY. The probability that the intervention was cost-effective compared with the control was reported for a given maximum acceptable ceiling ratio of €30 000 per QALY and €100 000 per QALY.
These statistical analyses were performed on the basis of the intention-to-treat principle, that is, patients were analysed in the group to which they were allocated. Analyses were performed using STATA (Stata Statistical Software: release V.13.1. Stata Corp, College Station, Texas, USA). Transformation of the SF-36 to the QoL-index was performed using IBM SPSS Statistics release V.21.0.0.0.
Results
One hundred and fifteen patients were included and randomised, 59 patients to chiropractic care, and 56 to self-management. Randomisation resulted in two groups with similar baseline values for the clinical variables. In the chiropractic care group, n=0 (0%), n=8 (14%) and n=9 (15%) were lost to self-report follow-up at 4, 12 and 52 weeks, compared with n=9 (16%), n=8 (14%) and n=16 (29%) in the self-management group. All 115 patients (100%) were followed over 1 year using national registries. The flow of participants through the trial is provided in online supplementary figure S1. Table 1 shows the baseline characteristics of the chiropractic care and self-management groups.
Table 1.
Baseline patient characteristics. Data are expressed as means and ±SDs or absolute numbers and relative frequencies (in parentheses)
| Chiropractic care n=59 |
Self-management n=56 |
|
|---|---|---|
| Age, years±SD | 51.4±10.0 | 50.8±12.1 |
| Female, n (%) | 26 (44.0) | 22 (39.3) |
| Maximum chest pain (0–10),* ±SD | 6.7±2.4 | 5.9±2.3 |
| EQ-5D, mean±SD | 0.738±0.021 | 0.718±0.022 |
| SF-6D, mean±SD | 0.695±0.015 | 0.676±0.016 |
| Married/living with someone, n (%) | 51 (86.4) | 50 (90.9) |
| Working, n (%) | 44 (75.9) | 35 (63.6) |
| College graduate, n (%) | 16 (27.6) | 16 (30.2) |
| Expectation of treatment† | ||
| Chiropractic care±SD | 2.2±0.5 | 2.1±0.6 |
| Self-management±SD | 2.3±0.5 | 2.3±0.6 |
*Pain intensity was reported on an 11-point numeric rating scale ranging from 0=no pain to 10=worst possible pain.
†Expectation was reported as average ratings on a five-point box scale (much better=1 to much worse=5).
EQ-5D, EuroQol five-dimension questionnaire; SF-6D, six-dimensional health status short form.
openhrt-2015-000334supp_figures.pdf (189.4KB, pdf)
Clinical outcomes
Table 2 presents the HRQoL scores at baseline and at the three follow-up time points. In both groups, there was an increase in the HRQoL scores, but there were no statistically significant differences between the two groups at any of the time points or any trends in favour of either group. The group difference in QALYs was negligible.
Table 2.
Multiple imputed clinical outcomes at follow-up
| Outcome | Chiropractic care (n=59) |
Self-management (n=56) |
Difference* |
|---|---|---|---|
| Mean (SD) | Mean (SD) | Δ (95% CI) | |
| EQ-5D | |||
| Baseline | 0.738±0.021 | 0.718±0.022 | |
| 4 weeks | 0.786 (0.021) | 0.796 (0.018) | −0.021 (−0.065 to 0.023) |
| 12 weeks | 0.811 (0.023) | 0.792 (0.020) | 0.009 (−0.044 to 0.062) |
| 52 weeks | 0.826 (0.023) | 0.823 (0.024) | −0.033 (−0.069 to 0.062) |
| 1-year QALY (EQ-5D) | 0.811 (0.019) | 0.802 (0.017) | 0.0094 (−0.041 to 0.060) |
| SF-36 | |||
| Baseline | 0.695±0.015 | 0.676±0.016 | |
| 4 weeks | 0.742 (0.018) | 0.727 (0.020) | 0.004 (−0.039 to 0.047) |
| 12 weeks | 0.757 (0.018) | 0.754 (0.021) | −0.010 (−0.056 to 0.035) |
| 52 weeks | 0.788 (0.018) | 0.774 (0.021) | 0.003 (−0.045 to 0.051) |
| 1-year QALY (SF-6D) | 0.765 (0.0157) | 0.756 (0.0190) | 0.0092 (−0.039 to 0.058) |
*The mean outcome differences between chiropractic care and self-management were adjusted for the baseline difference.
EQ-5D, EuroQol five-dimension questionnaire; QALY, quality-adjusted life year; SF-6D, six-dimensional health status short form; SF-36, Short Form 36-item Health Survey.
Healthcare utilisation and medication
Online supplementary table S1 lists the healthcare utilisation and associated costs in the chiropractic care and self-management groups. As part of the intervention, the chiropractic care patients had an average of 7.0 chiropractic visits (minimum=1, maximum=10), and 19 patients (32%) had an X-ray performed. All patients in the self-management group (n=56) completed the information session. Overall, fewer chiropractic care patients used healthcare services and those that did had a lower mean number of visits for some of these services compared with the self-management patients: GP after-hours service (12% vs 29% (p=0.03), 1.1 vs 2.0 visits (p=0.11)), admissions to cardiology departments (3% vs 18% (p=0.01), 1.0 vs 1.3 admissions (p=0.28)), cardiology ambulatory visits (14% vs 30% (p=0.03), 1.1 vs 1.5 visits (p=0.13)) and other ambulatory visits (34% vs 41% (p=0.43), 2.3 vs 4.0 visits (p=0.02)). For visits to primary care musculoskeletal providers (chiropractors and physiotherapists), the chiropractic care group showed a trend towards a higher proportion of patients visiting chiropractors (32% vs 18% (p=0.08), 4.6 vs 5.8 visits (p=0.07)) in the follow-up period compared with the self-management group, but a slightly lower proportion visiting physiotherapists (10% vs 14% (p=0.50), 5.8 vs 35.1 visits (p=0.27)). For both provider types, the chiropractic care group had a statistically non-significant lower mean number of visits. Use of non-prescriptive and prescriptive medication was similar for the two groups, except for non-prescriptive mild analgesics (32% vs 13% (p=0.01)) and herbal medicine (15% vs 0% (p=0.002)), which were significantly higher in the chiropractic care group, and lower for prescriptive opioids (7% vs 13% (p=0.3)) and lipid-modifying drugs (9% vs 17% (p=0.05); see online supplementary table S2).
openhrt-2015-000334supp_tables.pdf (708.8KB, pdf)
Costs
The mean intervention cost of the chiropractic care was higher than the cost of self-management (€403.7 vs €44.8, mean difference €358.9, 95% CI (321.4 to 396.4); see online supplementary tables S1 and S4). Subsequent healthcare costs relating to primary care were overall similar between the groups (€409.4 vs €502.9, mean difference −€93.5; 95% CI (−321.6 to 134.7)), whereas costs of hospital care were lower in the chiropractic care group (€1919.5 vs €4305.8, mean difference −€2386.3, 95% CI (−4580.5 to −192.0)).
Total 1-year costs in the chiropractic care group were €2183 lower than in the self-management group, but this difference was not statistically significant (95% CI (−4410.5 to 43.0); table 3). The main contributor to the cost difference was admissions to hospital (see online supplementary table S1).
Table 3.
The total and mean costs of the interventions, healthcare utilization and 1-yer total costs per person (€) with 95% CIs
| Chiropractic care n=59 |
Self-management n=56 |
Mean difference | |||
|---|---|---|---|---|---|
| Total costs | Mean costs per patient (95% CI) |
Total costs | Mean costs per patient (95% CI) |
Δ (95% CI) | |
| Intervention costs | 23 821 | 404 (367 to 441) | 2511 | 45 (45 to 45) | 359 (321 to 396) |
| Healthcare costs | 155 604 | 2637 (1942 to 3333) | 290 082 | 5180 (2990 to 7370) | −2543 (−4767 to −319) |
| Total 1-year costs | 179 426 | 3041 (2337 to 3745) | 292 593 | 5225 (3035 to 7415) | −2184 (−4411 to 43) |
Cost-effectiveness
The incremental costs were −€2184 (savings) and the incremental effect was 0.0092 and 0.0096 QALY using the EQ-5D and SF-36, respectively. This indicates that the chiropractor intervention dominated the information intervention by providing similar (or slightly improved) health utility at an overall lower cost.
The joint distribution of costs and effects (EQ-5D) are presented in figure 2. Sixty-five per cent of the bootstrapped incremental cost–effect pairs fall in the southeast quadrant indicating a positive QALY gain at lower costs by chiropractic care compared with self-management. Thirty-three per cent falls in the southwest quadrant, indicating less health utility but at lower costs. Consequently, there is a 65% probability that chiropractic care generates better outcomes and is less costly than self-management. These findings are similar when the SF-36 was used as the utility measure (data not shown). The cost-effectiveness acceptability curve using EQ-5D is presented in online supplementary figure S2. Given a maximum acceptable ceiling ratio of €30 000 per QALY gained, the probability that chiropractic care is cost-effective compared with self-management is 0.972. At €100 000 per QALY gained, the probability is 0.881. When using SF-36, the probability that chiropractic care is cost-effective compared with self-management is 0.958 and 0.874 given a maximum acceptable ceiling ratio of €30 000 and €100 000 per QALY gained, respectively (data not shown).
Figure 2.
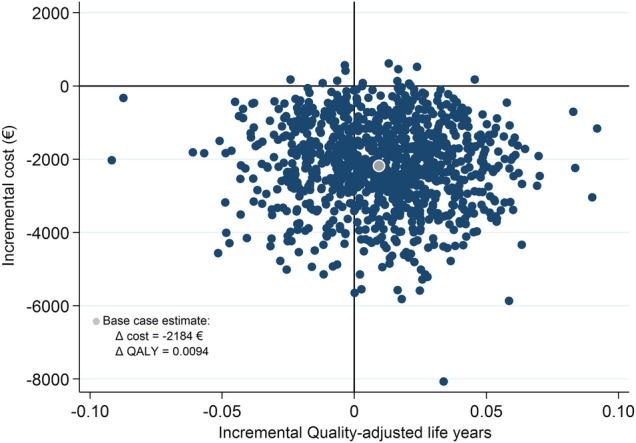
Scatter plot of estimated joint density of incremental costs and incremental effects (quality-adjusted life years (EuroQol five-dimension questionnaire, EQ-5D)) of chiropractic care versus self-management obtained by bootstrap resampling.
Discussion
In this analysis of data from a randomised clinical trial assessing the cost-effectiveness of two strategies to reduce pain and improve quality of life in patients with musculoskeletal chest pain, we observed no statistically significant differences between the two strategies in QALYs gained. We did, however, observe lower total healthcare costs in the chiropractic care group during the first year after enrolment in the trial (−€2184; 95% CI −4411 to 43). Assuming identical gains in HRQoL, the study showed that chiropractic care is more cost-effective when compared with self-management in patients presenting with an acute episode of musculoskeletal chest pain. Similar results, when using the two utility measures, support the robustness of these findings. The study showed that this patient group with musculoskeletal chest pain has a high use of healthcare resources with high associated costs.
Using registry-based data on healthcare utilisation, prescriptions and associated costs have two major advantages. First, using the unique personal identification number assigned to each Danish resident, we were able to track all hospital and public primary care utilisation and medication use over the 1-year follow-up period with no loss to follow-up. We were not able to track the use of primary care utilisation covered by private insurance plans (primarily use of chiropractic, physiotherapy and psychology services), but compared with hospital costs, the costs of these private plans are negligible and not likely to influence the results. Second, the presented costs are actual incurred costs, which reduced the uncertainty regarding the cost estimates. Compared with Swedish reports,5 annual average costs were lower in our study (€3000–€5200); however, this difference may be explained by the lower mean age in our study or perhaps the subset of patients with NSCP suffering from musculoskeletal chest pain incurs fewer costs compared with a mixed group with NSCP. We did not take into account indirect costs, such as sick leave and lost productivity. According to Mourad et al,5 costs of sick leave, disability pension and reduced productivity are approximately one-third of total costs. This means that future research into NSCP interventions should address not only healthcare costs, but also how the intervention impacts on work life.
The two groups reported similar HRQoL at all time points, and they were all clinically relevant improvements that were above the minimal important difference41 for the EQ-5D and SF-36 scores, with the largest improvement after 4 weeks. Despite these improvements, both groups reported HRQoL outcomes below the age-matched and sex-matched Danish population norms42 at baseline and at all three follow-ups which confirm that NSCP has an important impact on psychological health and quality of life.43 The statistically significant difference in clinical improvement (pain intensity and global perceived effect) in favour of the chiropractic care group seen in the previous reports of this clinical trial18 19 was not reflected in the HRQoL measures. This may indicate that the two interventions provided similar effects in HRQoL in patients with musculoskeletal chest pain. Alternatively, it could be that the HRQoL measures, which were originally designed to measure change in chronic conditions, are not sufficiently responsive to reflect change in pain intensity or reflect those changes that caused these patients to report a global effect in this acute chest pain condition. This study was powered to detect a difference in the primary outcomes (maximum chest pain and global perceived effect at 4 weeks). It is likely that the study is underpowered to detect a difference in HRQoL at 1-year follow-up with the accompanying risk of a type 2 error. Owing to the limited follow-up of 1 year, we were not able to observe potentially long-term adverse effects of reduced hospital admission in the chiropractic care group; however, we have previously shown that the risk of future cardiac events is low in patients with NSCP and will likely occur within the first year after hospitalisation, if at all.44
This study was designed as a pragmatic trial with a 12-month follow-up period that was conducted in the real-life context of a large university hospital in Denmark and four community-based chiropractic practices, which strengthens the external validity of our results.45 The main contributor to the lower cost of the chiropractor care group was the lower rate of hospitalisation in that group. We are not able to elucidate why, but psychological factors frequently influence healthcare-seeking generally and have been suggested in chest pain patients specifically.46 47 In particular, fear of activities that cause physical (somatic) sensation with normal activities and ‘normal’ discomfort (interoceptive fear) are an important factor in understanding the persistent medical-seeking behaviours of some patients with NSCP.43 47 48 We suggest that the key factors in the success of the chiropractic care were the close contact with a primary healthcare provider, who targeted unmet distress, the consideration of psychological and physical factors together, and the neurological and analgesic effect of manual therapy. In any case, it is clear that offering a series of consultations with a musculoskeletal healthcare provider may have positive economic implications that are not achieved when patients are left to manage their condition on their own.
NSCP is defined as the absence of coronary disease and is not a unitary diagnosis but contains a number of diverse subgroups.3 Patients with NSCP may have evidence of gastro-oesophageal, musculoskeletal, psychiatric or psychological abnormalities, and signs of one or more co-occurring conditions. It has been argued that the ability to provide adequate care is limited by a lack of information on the characteristics of patients with NSCP.3 By means of a systematic clinical assessment of this patient group, we were able to identify a subset of patients with suspected musculoskeletal chest pain, and we have demonstrated the cost-effectiveness of a safe and low-tech management strategy for this specific patient group. Considering the large number of people with NSCP, a recommendation in future clinical guidelines of primary care treatment for musculoskeletal chest pain from clinicians, such as chiropractors or similar professions, could result in considerable savings to societies, provided that a multifaceted, person-centred approach was used. In our clinical trial, that comprehensive approach included manual treatment, exercises and advice targeting both psychosocial and biomechanical aspects of chest pain. Future research should evaluate the generalisability of our results to other settings, look into understanding the potentially multifactorial causes of NSCP and recognise the potential for multiple coexisting and potentially mutually reinforcing causes, in diagnosis and treatment.
Conclusion
We observed no significant difference in HRQoL, but we did observe significant cost-savings relating to hospital contacts in patients who received usual care in combination with community-based chiropractic care compared with usual care and self-management. This suggests that offering a series of consultations with a musculoskeletal healthcare provider is a more cost-effective approach compared with leaving patients to manage the condition themselves.
Acknowledgments
The authors thank Eleanor Boyle, PhD, for help with the transformation of the SF-36 to the QoL-index and for statistical advice.
Footnotes
Contributors: MJS, WV, HWC, PFH-C and JH contributed to the concept and design of the clinical components of the study, which was led by MJS. MJS, JS and JH developed the economic component of the study. MJS, JS and WV developed the analytic plan for the study. MJS and JS analysed its results. MJS drafted the manuscript and all authors critically revised the article for important intellectual content and gave final approval of the version to be published. MJS is the guarantor. All authors had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding: This research was partly funded by the Region of Southern Denmark (former Funen County), the Danish Chiropractic Foundation, and the Scott Haldeman Award.
Competing interests: None declared.
Ethics approval: Obtained from the Regional Ethics Committee of Vejle and Funen Counties, Denmark (approval number #VF 20060002), the Danish Data Protection Agency (journal number #2013-41-2012) and registered at ClinicalTrials.gov (identification number NCT00462241). All participants gave written informed consent.
Provenance and peer review: Not commissioned; internally peer reviewed.
Data sharing statement: No additional data are available.
References
- 1.Fagring AJ, Lappas G, Kjellgren KI et al. Twenty-year trends in incidence and 1-year mortality in Swedish patients hospitalised with non-AMI chest pain. Data from 1987–2006 from the Swedish hospital and death registries. Heart 2010;96:1043–9. 10.1136/hrt.2010.193748 [DOI] [PubMed] [Google Scholar]
- 2.Murphy NF, MacIntyre K, Capewell S et al. Hospital discharge rates for suspected acute coronary syndromes between 1990 and 2000: population based analysis. BMJ 2004;328:1413–14. 10.1136/bmj.38111.650741.F7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Marks EM, Chambers JB, Russell V et al. The rapid access chest pain clinic: unmet distress and disability. QJM 2014;107:429–34. 10.1093/qjmed/hcu009 [DOI] [PubMed] [Google Scholar]
- 4.Goodacre S, Cross E, Arnold J et al. The health care burden of acute chest pain. Heart 2005;91:229–30. 10.1136/hrt.2003.027599 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mourad G, Alwin J, Strömberg A et al. Societal costs of non-cardiac chest pain compared with ischemic heart disease—a longitudinal study. BMC Health Serv Res 2013;13:403 10.1186/1472-6963-13-403 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Groarke J, O'Brien J, Go G et al. Cost burden of non-specific chest pain admissions. Ir J Med Sci 2013;182:57–61. 10.1007/s11845-012-0826-5 [DOI] [PubMed] [Google Scholar]
- 7.Nawar EW, Niska RW, Xu J. National Hospital Ambulatory Medical Care Survey: 2005 emergency department summary. Adv Data 2007;(386):1–32. [PubMed] [Google Scholar]
- 8.Leise MD, Locke GR III, Dierkhising RA et al. Patients dismissed from the hospital with a diagnosis of noncardiac chest pain: cardiac outcomes and health care utilization. Mayo Clin Proc 2010;85:323–30. 10.4065/mcp.2009.0428 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Tew R, Guthrie EA, Creed FH et al. A long-term follow-up study of patients with ischaemic heart disease versus patients with nonspecific chest pain. J Psychosom Res 1995;39:977–85. 10.1016/0022-3999(95)00065-8 [DOI] [PubMed] [Google Scholar]
- 10.Forberg JL, Henriksen LS, Edenbrandt L et al. Direct hospital costs of chest pain patients attending the emergency department: a retrospective study. BMC Emerg Med 2006;6:6 10.1186/1471-227X-6-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chambers JB, Marks EM, Russell V et al. A multidisciplinary, biopsychosocial treatment for non-cardiac chest pain. Int J Clin Pract 2015;69:922–7. 10.1111/ijcp.12533 [DOI] [PubMed] [Google Scholar]
- 12.Eslick GD, Talley NJ. Non-cardiac chest pain: predictors of health care seeking, the types of health care professional consulted, work absenteeism and interruption of daily activities. Aliment Pharmacol Ther 2004;20:909–15. 10.1111/j.1365-2036.2004.02175.x [DOI] [PubMed] [Google Scholar]
- 13.Glombiewski JA, Rief W, Bösner S et al. The course of nonspecific chest pain in primary care: symptom persistence and health care usage. Arch Intern Med 2010;170:251–5. 10.1001/archinternmed.2009.474 [DOI] [PubMed] [Google Scholar]
- 14.Burgstaller JM, Jenni BF, Steurer J et al. Treatment efficacy for non-cardiovascular chest pain: a systematic review and meta-analysis. PLoS ONE 2014;9:e104722 10.1371/journal.pone.0104722 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Parkash O, Almas A, Hameed A et al. Comparison of non cardiac chest pain (NCCP) and acute coronary syndrome (ACS) patients presenting to a tertiary care center. J Pak Med Assoc 2009;59:667–71. [PubMed] [Google Scholar]
- 16.Knockaert DC, Buntinx F, Stoens N et al. Chest pain in the emergency department: the broad spectrum of causes. Eur J Emerg Med 2002;9:25–30. 10.1097/00063110-200203000-00007 [DOI] [PubMed] [Google Scholar]
- 17.Fruergaard P, Launbjerg J, Hesse B et al. The diagnoses of patients admitted with acute chest pain but without myocardial infarction. Eur Heart J 1996;17:1028–34. 10.1093/oxfordjournals.eurheartj.a014998 [DOI] [PubMed] [Google Scholar]
- 18.Stochkendahl MJ, Christensen HW, Vach W et al. Chiropractic treatment vs self-management in patients with acute chest pain: a randomized controlled trial of patients without acute coronary syndrome. J Manipulative Physiol Ther 2012;35:7–17. 10.1016/j.jmpt.2010.11.004 [DOI] [PubMed] [Google Scholar]
- 19.Stochkendahl MJ, Christensen HW, Vach W et al. A randomized clinical trial of chiropractic treatment and self-management in patients with acute musculoskeletal chest pain: 1-year follow-up. J Manipulative Physiol Ther 2012;35:254–62. 10.1016/j.jmpt.2012.04.003 [DOI] [PubMed] [Google Scholar]
- 20.Stochkendahl MJ, Christensen HW, Vach W et al. Diagnosis and treatment of musculoskeletal chest pain: design of a multi-purpose trial. BMC Musculoskelet Disord 2008;9:40 10.1186/1471-2474-9-40 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Brunse MH, Stochkendahl MJ, Vach W et al. Examination of musculoskeletal chest pain—an inter-observer reliability study. Man Ther 2010;15:167–72. 10.1016/j.math.2009.10.003 [DOI] [PubMed] [Google Scholar]
- 22.Christensen HW, Vach W, Gichangi A et al. Cervicothoracic angina identified by case history and palpation findings in patients with stable angina pectoris. J Manipulative Physiol Ther 2005;28:303–11. 10.1016/j.jmpt.2005.04.002 [DOI] [PubMed] [Google Scholar]
- 23.Pedersen CB. The Danish Civil Registration System. Scand J Public Health 2011;39(Suppl 7):22–5. 10.1177/1403494810387965 [DOI] [PubMed] [Google Scholar]
- 24.Lynge E, Sandegaard JL, Rebolj M. The Danish National Patient Register. Scand J Public Health 2011;39(Suppl 7):30–3. 10.1177/1403494811401482 [DOI] [PubMed] [Google Scholar]
- 25.Andersen JS, Olivarius Nde F, Krasnik A. The Danish National Health Service Register. Scand J Public Health 2011;39(Suppl 7):34–7. 10.1177/1403494810394718 [DOI] [PubMed] [Google Scholar]
- 26.Gaist D, Sorensen HT, Hallas J. The Danish prescription registries. Dan Med Bulletin 1997;44:445–8. [PubMed] [Google Scholar]
- 27.Torrance GW, Raynauld JP, Walker V et al. A prospective, randomized, pragmatic, health outcomes trial evaluating the incorporation of hylan G-F 20 into the treatment paradigm for patients with knee osteoarthritis (Part 2 of 2): economic results. Osteoarthritis Cartilage 2002;10:518–27. 10.1053/joca.2001.0513 [DOI] [PubMed] [Google Scholar]
- 28.Bjorner JB, Kreiner S, Ware JE et al. Differential item functioning in the Danish translation of the SF-36. J Clin Epidemiol 1998;51:1189–202. 10.1016/S0895-4356(98)00111-5 [DOI] [PubMed] [Google Scholar]
- 29.Bjorner JB, Damsgaard MT, Watt T et al. Tests of data quality, scaling assumptions, and reliability of the Danish SF-36. J Clin Epidemiol 1998;51:1001–11. 10.1016/S0895-4356(98)00092-4 [DOI] [PubMed] [Google Scholar]
- 30.Brazier JE, Rowen D, Hanmer J. Revised SF-6D scoring programmes: a summary of improvements. Patient Reported Outcomes Newsletter 2008:14–15. http://www.pro-newsletter.com/images/PDF_articles/sf-6d.pdf (accessed 8 Sep 2015).
- 31.Kharroubi SA, Brazier JE, Roberts J et al. Modelling SF-6D health state preference data using a nonparametric Bayesian method. J Health Econ 2007;26:597–612. 10.1016/j.jhealeco.2006.09.002 [DOI] [PubMed] [Google Scholar]
- 32.Brazier JE, Roberts J. The estimation of a preference-based measure of health from the SF-12. Med Care 2004;42:851–9. 10.1097/01.mlr.0000135827.18610.0d [DOI] [PubMed] [Google Scholar]
- 33.Brooks R, Rabin R, de Charro F. The measurement and valuation of health status using EQ-5D: A European perspective: evidence from the EuroQol BIO MED research programme. Dordrecht, The Netherlands: Kluwer Academic Publishers, 2003. [Google Scholar]
- 34.Gudex C, Sørensen J. EQ-SD: A generic health status instrument [in Danish]. Maanedsskrift Praktisk Laegegerning 1998;76:1339–45. [Google Scholar]
- 35.Kind P, Macran S. A five-level version of EQ-5D. Value Health 2004;7:650 10.1016/S1098-3015(10)65676-8 [DOI] [Google Scholar]
- 36.Janssen MF, Birnie E, Haagsma JA et al. Comparing the standard EQ-5D three-level system with a five-level version. Value Health 2008;11:275–84. 10.1111/j.1524-4733.2007.00230.x [DOI] [PubMed] [Google Scholar]
- 37.Janssen MF, Birnie E, Bonsel GJ. Quantification of the level descriptors for the standard EQ-5D three-level system and a five-level version according to two methods. Qual Life Res 2008;17:463–73. 10.1007/s11136-008-9318-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Oppe M, Devlin NJ, Szende A. EQ-5D value sets: inventory, comparative review and user guide. Dordrecht, The Netherlands: Springer, 2007. [Google Scholar]
- 39.Wittrup-Jensen KU, Lauridsen J, Gudex C et al. Generation of a Danish TTO value set for EQ-5D health states. Scand J Public Health 2009;37:459–66. 10.1177/1403494809105287 [DOI] [PubMed] [Google Scholar]
- 40.Rubin DB. Multiple imputation after 18+ years. J Am Stat Assoc 1996;91:473–89. 10.1080/01621459.1996.10476908 [DOI] [Google Scholar]
- 41.Walters SJ, Brazier JE. Comparison of the minimally important difference for two health state utility measures: EQ-5D and SF-6D. Qual Life Res 2005;14:1523–32. 10.1007/s11136-004-7713-0 [DOI] [PubMed] [Google Scholar]
- 42.Sørensen J, Davidsen M, Gudex C et al. Danish EQ-5D population norms. Scand J Public Health 2009;37:467–74. 10.1177/1403494809105286 [DOI] [PubMed] [Google Scholar]
- 43.Webster R, Norman P, Goodacre S et al. The prevalence and correlates of psychological outcomes in patients with acute non-cardiac chest pain: a systematic review. Emerg Med J 2012;29:267–73. 10.1136/emermed-2011-200526 [DOI] [PubMed] [Google Scholar]
- 44.Stochkendahl MJ, Mickley H, Vach W et al. Clinical characteristics, myocardial perfusion deficits, and clinical outcomes of patients with non-specific chest pain hospitalized for suspected acute coronary syndrome: a 4-year prospective cohort study. Int J Cardiol 2015;182:126–31. 10.1016/j.ijcard.2014.12.054 [DOI] [PubMed] [Google Scholar]
- 45.Ramsey S, Willke R, Briggs A et al. Good research practices for cost-effectiveness analysis alongside clinical trials: the ISPOR RCT-CEA Task Force report. Value Health 2005; 8:521–33. 10.1111/j.1524-4733.2005.00045.x [DOI] [PubMed] [Google Scholar]
- 46.Mourad G, Strömberg A, Johansson P et al. Depressive symptoms, cardiac anxiety, and fear of body sensations in patients with non-cardiac chest pain, and their relation to healthcare-seeking behavior: a cross-sectional study. Patient 2016;9:69–77. 10.1007/s40271-015-0125-0 [DOI] [PubMed] [Google Scholar]
- 47.Hadlandsmyth K, Rosenbaum DL, Craft JM et al. Health care utilisation in patients with non-cardiac chest pain: a longitudinal analysis of chest pain, anxiety and interoceptive fear. Psychol Health 2013;28:849–61. 10.1080/08870446.2012.762100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Robertson N, Javed N, Samani NJ et al. Psychological morbidity and illness appraisals of patients with cardiac and non-cardiac chest pain attending a rapid access chest pain clinic: a longitudinal cohort study. Heart 2008;94:e12 10.1136/hrt.2006.100537 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
openhrt-2015-000334supp_figures.pdf (189.4KB, pdf)
openhrt-2015-000334supp_tables.pdf (708.8KB, pdf)