

Abstract
A new breast mass was identified in an adult woman undergoing treatment for a known ethmoid sinus alveolar rhabdomyosarcoma. Histopathological evaluation revealed alveolar rhabdomyosarcoma metastatic to the breast. Alveolar rhabdomyosarcoma, primarily described in adolescents and especially rare in adults, can uncommonly metastasize to the breast.
Case report
A 35-year-old woman with a known tissue diagnosis of primary alveolar rhabdomyosarcoma of the ethmoid sinus from an outside hospital (Fig. 1A) presented to our institution with a new palpable left breast mass.
Figure 1.

A 35-year-old woman with alveolar rhabdomyosarcoma of the ethmoid sinus metastatic to the breast. A. Coronal T1-weighted, postcontrast, fat-saturated MRI of the face shows lobulated, enhancing soft tissue involving the right ethmoidal air cells and the medial wall of the right orbit (arrow) after surgical intervention.
B. Axial, contrast-enhanced CT image of the neck shows right submandibular metastatic lymphadenopathy (arrow), enlarged compared to a prior examination.
At the time of presentation, the patient had completed two rounds of chemotherapy and two rounds of radiation therapy for the primary ethmoid sinus tumor and a metastatic right submandibular lymph node (Fig. 1B). She had been disease- and symptom-free for six months. Mammography (Fig. 2) revealed a mass measuring 8 millimeters in the subareolar region of the left breast, corresponding to a palpable abnormality.
Figure 2.

A 35-year-old woman with alveolar rhabdomyosarcoma of the ethmoid sinus metastatic to the breast. Mammography shows an 8mm left breast subareolar mass (arrow) in the region of the palpable abnormality. A. Craniocaudal view. B. Lateromedial view. C. Photographically magnified craniocaudal view. D. Photographically magnified lateromedial view.
Further evaluation with sonography of the left breast subareolar region in the area of the palpable abnormality (Fig. 3) revealed an irregular, solid, hypoechoic mass, measuring 1.2 × 0.6 × 0.5 cm, with internal vascularity and indistinct margins.
Figure 3.

A 35-year-old woman with alveolar rhabdomyosarcoma of the ethmoid sinus metastatic to the breast. Before ultrasound-guided fine-needle aspiration, targeted left-breast ultrasound, focusing on the left retroareolar palpable mass (arrow), was performed (A: Transverse view. B: Longitudinal view).
Fine-needle aspiration of the palpable left breast retroareolar mass was performed under sonographic guidance.
On cytology, smears demonstrated a discohesive population of intermediate-sized cells with an increased nuclear-to-cytoplasm ratio, prominent nucleoli, and nuclear stripping. Immunocytochemistry showed tumor cells strongly positive for desmin and myogenin and negative for pan-cytokeratin and leukocyte common antigen. These findings were consistent with metastasis from the patient's known alveolar rhabdomyosarcoma (Fig. 4).
Figure 4.
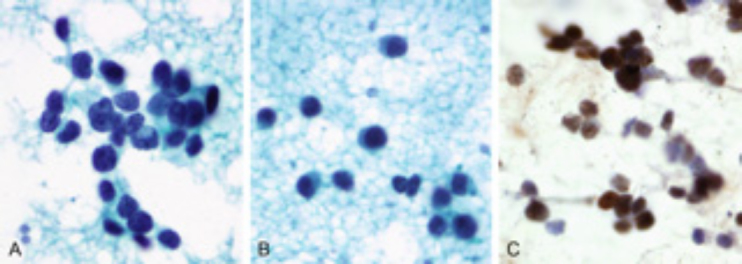
A 35-year-old woman with alveolar rhabdomyosarcoma of the ethmoid sinus metastatic to the breast. Direct smear of material from the ultrasound-guided, fine-needle aspiration of the breast mass stained by the Papanicolaou method shows a loose cluster (A) and single tumor cells (B) with fine nuclear chromatin, a high nuclear-cytoplasmic ratio, and scant cytoplasm. Immunohistochemical staining for myogenin (C) shows diffuse and strong nuclear positivity, supporting the diagnosis of rhabdomyosarcoma.
A final diagnosis of alveolar rhabdomyosarcoma from the ethmoid sinus with metastatic disease to the breast was confirmed by histopathological evaluation following left-breast segmental resection.
Discussion
Metastatic disease to the breast is a relatively rare process; several case series report an incidence from 2 to 6% (1, 2, 3, 4). The most common primary tumors that metastasize to the breast, aside from contralateral breast cancer, leukemia, and lymphoma, include melanoma, carcinoma of the lung, and (less commonly) carcinoid, carcinoma of the ovary and the cervix, and renal-cell carcinoma (5).
Rhabdomyosarcoma is primarily a disease of rhabdomyoblasts that affects children and adolescents, responsible for more than 50% of the soft-tissue sarcomas in child and adolescent populations. Rhabdomyosarcoma in adults is unusual, and it is associated with a significantly poorer prognosis when compared to rhabdomyosarcoma in adolescents (6, 7, 8). Histopathological evaluation can further categorize these tumors, using the International Classification of Rhabdomyosarcomas, with alveolar and undifferentiated subtypes associated with the least favorable prognoses (9). The alveolar subtype, which commonly originates from the extremities or the trunk, has been shown to be associated with other primary sites, including the head and the neck (10).
Histopathologic and cytologic examination of rhabdomyosarcoma typically reveals round-to oval-shaped primitive rhabdomyoblasts in nests of pseudo-alveolar structures separated by fibrous septa (11, 12). The cells may have an increased nuclear-to-cytoplasm ratio, cytoplasmic vacuolization, and prominent nucleoli. The predominant cell type of alveolar rhabdomyosarcoma stains strongly positive for desmin and myogenin. This patient's fine-needle aspiration sample from her palpable mass demonstrated all of the classically described findings.
The imaging appearance of metastatic alveolar rhabdomyosarcoma has been well documented (13). Mammographic and sonographic masses may appear lobular in shape, with well-circumscribed margins. On ultrasound, the echotexture can be variable, although metastatic lesions may be more likely to be heterogeneous and hypoechoic (14). Early ring-like enhancement on MRI has been reported (15).
Several case reports have described adolescent alveolar rhabdomyosarcoma metastatic to the breast; however, this patient's case is unique, with an unusual combination of clinical features, including a primary diagnosis of rhabdomyosarcoma in the fourth decade of life and metastasis to the breast. Although exceedingly uncommon, radiologists and clinicians should be aware of the potential for alveolar rhabdomyosarcoma to metastasize to the breast in the adult population.
Acknowledgment
We thank Crystal Allen for assistance in manuscript preparation.
Footnotes
Published: August 14, 2014
References
- 1.Toombs BD, Kalisher L. Metastatic disease to the breast: clinical, pathologic and radiographic features. Am J Roentgenol. 1977;129(4):673–676. doi: 10.2214/ajr.129.4.673. [PubMed] [DOI] [PubMed] [Google Scholar]
- 2.Amichetti M, Perani B, Boi S. Metastases to the breast from extramammary malignancies. Oncology. 1990;47(3):257–260. doi: 10.1159/000226826. [PubMed] [DOI] [PubMed] [Google Scholar]
- 3.Bohman LG, Bassett LW, Gold RH, Voet R. Breast metastases from extramammary malignancies. Radiology. 1982;144(2):309–312. doi: 10.1148/radiology.144.2.7089284. [PubMed] [DOI] [PubMed] [Google Scholar]
- 4.McCrea ES, Johnston C, Haney PJ. Metastases to the breast. Am J Roentgenol. 1983;141(4):685–690. doi: 10.2214/ajr.141.4.685. [PubMed] [DOI] [PubMed] [Google Scholar]
- 5.Vergier B, Trojani M, Mascarel I, Coindre JM, Le Treut A. Metastases to the breast: differential diagnosis from primary breast carcinoma. J Surg Oncol. 1991;48(2):112–116. doi: 10.1002/jso.2930480208. [PubMed] [DOI] [PubMed] [Google Scholar]
- 6.Persic M, Roberts JT. Alveolar rhabdomyosarcoma metastatic to the breast: long-term survivor. Clin Oncol. 1999;11(6):417–418. doi: 10.1053/clon.1999.9096. [PubMed] [DOI] [PubMed] [Google Scholar]
- 7.Sultan I, Qaddoumi I, Yaser S, Rodriguez-Gallindo C, Ferrari A. Comparing adult and pediatric rhabdomyosarcoma in the Surveillance, Epidemiology and End Results Program, 1973 to 2005: an analysis of 2,600 patients. J Clin Oncol. 2009;27(20):3391–3397. doi: 10.1200/JCO.2008.19.7483. [PubMed] [DOI] [PubMed] [Google Scholar]
- 8.Dausse F, Balu-Maestro C, Chapellier C, Leblanc-Talent P. Rhabdomyosarcoma of the breast. Clin Imaging. 2005;29(5):337–341. doi: 10.1016/j.clinimag.2005.01.028. [PubMed] [DOI] [PubMed] [Google Scholar]
- 9.Newton WA, Gehan EA, Webber BL. Classification of rhabdomyosarcoma and related sarcomas. Pathologic aspects and proposal for a new classification – an Intergroup Rhabdomyosarcoma Study. Cancer. 1995;76(6):1073–1085. doi: 10.1002/1097-0142(19950915)76:6<1073::aid-cncr2820760624>3.0.co;2-l. [PubMed] [DOI] [PubMed] [Google Scholar]
- 10.Balaji R, Ramachandran K, Somanathan T, Nair SG, Krishnakumar AS, Venugopal M. Breast metastases in an adolescent woman with alveolar rhabdomyosarcoma of the maxillary sinus. Breast J. 2007;13(4):426–428. doi: 10.1111/j.1524-4741.2007.00456.x. [PubMed] [DOI] [PubMed] [Google Scholar]
- 11.Seidal T, Mark J, Hagmar B, Angervall L. Alveolar rhabdomyosarcoma: a cytogenetic and correlated cytological and histological study. Acta Pathol Microbiol Immunol Scand A. 1982;90(5):345–354. doi: 10.1111/j.1699-0463.1982.tb00105_90a.x. [PubMed] [DOI] [PubMed] [Google Scholar]
- 12.Parham D. Pathologic classification of rhabdomyosarcomas and correlations with molecular studies. Mod Pathol. 2001;14(5):506–514. doi: 10.1038/modpathol.3880339. [PubMed] [DOI] [PubMed] [Google Scholar]
- 13.Tukel S, Dogan BE, Ozcan H. Alveolar rhabdomyosarcoma metastatic to the breast. Curr Probl Diagn Radiol. 2003;32(2):102–104. doi: 10.1067/mdr.2003.120004. [PubMed] [DOI] [PubMed] [Google Scholar]
- 14.Lee S, Park J, Kook S, Han B, Moon W. Metastatic tumors to the breast: mammographic and ultrasonographic findings. J Ultrasound Med. 2000;19(4):257–262. doi: 10.7863/jum.2000.19.4.257. [PubMed] [DOI] [PubMed] [Google Scholar]
- 15.Perlet C, Sittek H, Forstpointner R, Kessler M, Reiser M. Metastases to the breast from rhabdomyosarcoma: appearances on MRI. Eur Radiol. 1999;9(6):1113–1116. doi: 10.1007/s003300050801. [PubMed] [DOI] [PubMed] [Google Scholar]