

Abstract
Background
Periodontal invasion of furcation area in multirooted teeth represents one of the most demanding therapeutic challenges in periodontics. Furcation therapy includes various treatment modalities like either maintenance or elimination of furcation or increased access to furcation area. Recent treatment modalities include regenerative procedures like placement of different type of bone grafts with nonabsorbable or absorbable barrier membranes, through guided tissue regeneration. This study compared the clinical efficacy of nonabsorbable barrier membrane with absorbable membrane when used with hydroxyapatite bone graft (G-Graft) in grade II buccal furcation defects in mandibular 1st molars.
Materials and methods
Fourteen subjects with bilateral grade II buccal furcation defects in lower 1st molars were selected and treated in a split-mouth design. After phase I therapy, molars were divided randomly into two groups for the treatment with either resorbable or nonresorbable membrane in conjunction with G-Graft in both groups.
Results
All the clinical parameters recorded showed statistically significant improvement in both the groups but no significant difference between two groups was observed.
Conclusion
Both nonabsorbable and absorbable barrier membranes were equally effective in treating grade II buccal furcation defects in lower molars when used in conjunction with G-Graft except with respect to horizontal bone fill in which absorbable barrier membrane showed better results.
Keywords: Furcation, Barrier membrane, Guided tissue regeneration
1. Introduction
Periodontitis is an inflammatory disease of the supporting tissues of the teeth caused by specific microorganisms or groups of specific microorganisms, resulting in progressive destruction of periodontal ligament and alveolar bone with pocket formation, recession or both. An ultimate goal of periodontal therapy is the regeneration of the lost tissue due to periodontal disease. Resective and regenerative surgeries are two approaches that can be used to eliminate periodontal defects. Invasion of the furcation of multirooted teeth is the most common reason for the early and frequent loss of molars. Therapy for the involved furcation includes scaling, root planing, conventional flap surgery, resective procedures, and regenerative procedures. Periodontal regeneration has become a viable treatment option utilizing the principles of guided tissue regeneration (GTR).1 The use of GTR to treat human class II furcation defects was first reported by Gottlow et al. The principles of GTR are based on certain cells to repopulate the wound area to form a new attachment apparatus. Clinically, this is accomplished by placing barrier membrane over the defect thereby occluding gingival tissue and connective tissue from migrating towards the wound during healing.
Nyman et al.2 first described the case of using nonresorbable Millipore filters in an effort to achieve new attachment. The first generation of GTR barriers were nonresorbable like cellulose acetate filters (Millipore filters), rubber dam, specifically processed expanded polytetrafluoroethylene3, 4 and dense polytetrafluoroethylene (d-PTFE)5 and have to be removed in second surgical procedure. Resorbable barriers (second generation) have been introduced later on, changing GTR into a single-step procedure. Among bioresorbable membranes used are allogenic soft tissues, such as freeze dried skin and freeze dried duramater (FDDMA)6 and reconstituted collagen membranes.7
Pontoriero et al.8 presented the results of the first clinical study evaluating the effects of GTR in furcation involvement. Clinical experiences indicated that GTR has the best possibility of success in class II furcation involvement.
2. Materials and methods
The present study was conducted on fourteen subjects (9 males, 5 females) in the age group ranging from 19 to 65 years with bilateral grade II buccal furcation defects in lower 1st molars selected from the Outpateint Department of Periodontology, Faculty of Dental Sciences, King George's Medical University, Lucknow.
2.1. Selection criteria
Patients ranging between 19 and 65 years of age, with grade II buccal furcation defects in 1st lower molars who fulfilled the inclusion criteria were included in the study.
2.1.1. Inclusion criteria
-
1.
Vertical probing depth (VPD) ≥4 mm.
-
2.
Horizontal probing depth ≥4 mm.
-
3.
Furcation entrance clinically not visible.
2.1.2. Exclusion criteria
-
1.
Patients with history of systemic disease.
-
2.
Smoking.
-
3.
History of antibiotics 1 month prior to study.
-
4.
History of periodontal therapy in the last 6 months.
-
5.
Allergic to hydroxyapatite material.
-
6.
Pregnant or lactating patients.
After phase I therapy, molars were divided randomly into two groups (Group I and II) for the treatment with either nonabsorbable or absorbable barrier membranes in conjunction with HABG in both groups in split mouth design (Fig. 1). In both the groups, furcation defects were treated with conventional flap debridement and defect filled with hydroxyapatite bone graft material (G-GRAFT) followed by placement of nonabsorbable d-PTFE GTR barrier membrane (TEF GEN-FD) in the group I and absorbable barrier membrane duramater (FDDMA) in the group II.
Fig. 1.
Barrier membranes.
2.2. Clinical parameters
The following clinical parameters were recorded at baseline and 6 months postoperatively. A customized acrylic stent was fabricated with an occlusoapical groove prepared on the midbuccal aspect for the standardization of placement of probe (Fig. 2). A fixed reference point (RP) on the stent was used to record the measurements.
-
1.
Plaque Index described by Silness P. and Loe H. in 1967 was used.
-
2.
Gingival Index developed by Loe H. and Silness J. in 1963 was used.
-
3.Position of gingival margin (GM), clinical attachment level (CAL), and VPD were calculated as follows:
-
4.
Horizontal probing depth of the furcation defect was measured using UNC 15 periodontal probe with the utilization of customized stent.
-
5.
Horizontal component of furcation defect after flap elevation was measured from an imaginary line tangential to the root surface to the horizontal extent of the defect (Fig. 3).
-
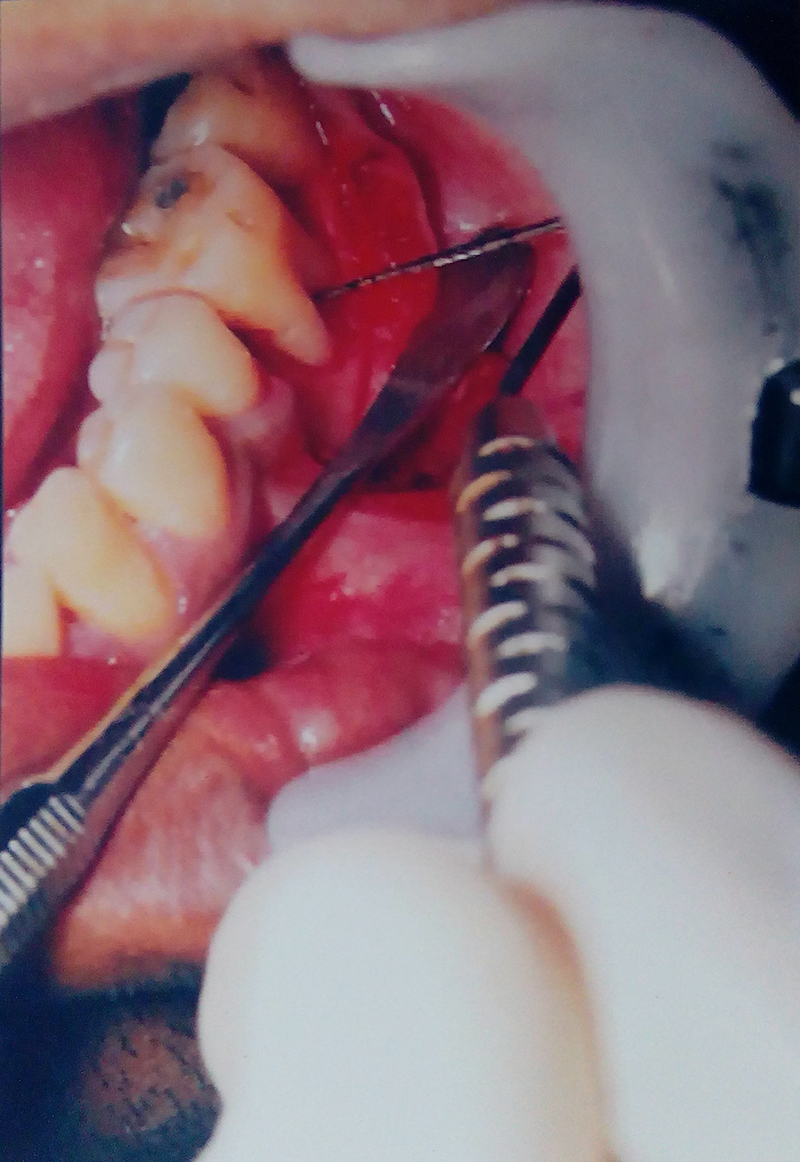
6.
Reduction in the horizontal component of furcation defect (horizontal bone fill) was measured by subtracting the horizontal component of furcation defect after flap elevation at 6 months postoperatively from the horizontal component of furcation defect after flap elevation at baseline (Fig. 4).
Fig. 2.

Customized stent.
Fig. 3.
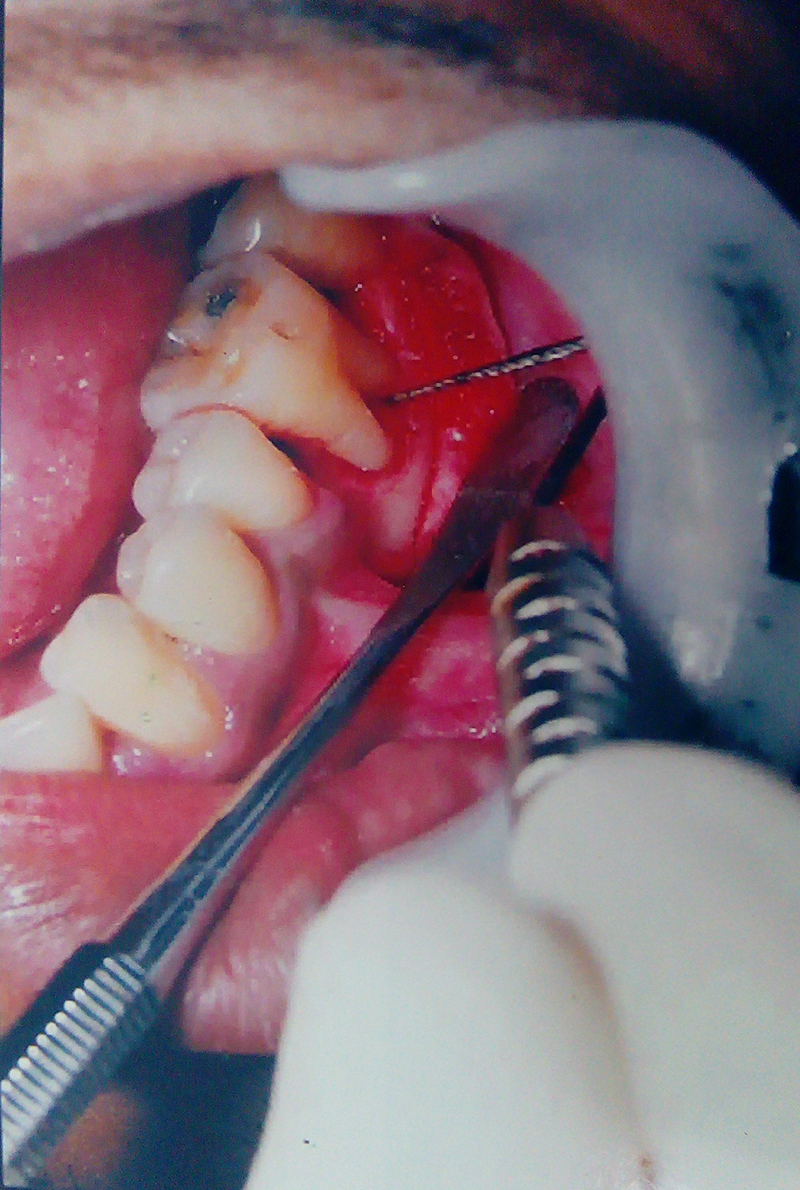
Horizontal probing depth at baseline.
Fig. 4.

Bone graft placed.
2.3. Presurgical procedure
Various plaque control measures were explained in detail to all the patients for the maintenance of good oral hygiene. After 2 weeks of phase I therapy, patients were recalled for the surgical procedure.
2.4. Surgical procedure
After initial therapy, furcation defects were randomly selected for the treatment with G-Graft and nonresorbable barrier membrane on one side (group I) and G-Graft and absorbable barrier membrane on the other side (group II). After anesthetizing the surgical area with 2% xylocaine with 1:80,000 adrenaline, a full-thickness mucoperiosteal flap was reflected. The defect was thoroughly debrided and roots were planed. The surgical area was copiously irrigated. Horizontal component of furcation defect was measured from an imaginary line tangential to the root surface to the horizontal extent of the defect at baseline.
On one side (group I), G-Graft was placed in the furcation defect (Fig. 5). G-Graft was mixed with saline using spatula and dappen dish and packed into the defect till the furcation defect was filled followed by placement of nonabsorbable barrier membrane covering the defect by at least 2–3 mm on all sides to have complete bone contact and prevention of connective tissue surface invasion below the graft material (Fig. 6). On the other side (group II), G-Graft and absorbable barrier membrane were used (Fig. 7). Both nonabsorbable and absorbable membranes were secured with absorbable sling suture. The mucoperiosteal flap was replaced and sutured. The surgical area was protected with a noneugenol dressing. Antibiotics, analgesics, and 0.2% chlorehexidine gluconate mouth wash were prescribed. The patients were given postoperative instructions and recalled after 10 days for the removal of periodontal dressing and sutures. The dressing and flap retaining sutures were removed in both groups and the surgical site was irrigated with normal saline.
Fig. 5.

Nonabsorbable barrier membrane placed.
Fig. 6.

Absorbable barrier membrane placed.
Fig. 7.
Horizontal probing depth after 6 months.
Nonabsorbable membranes in group I were removed after 4–6 weeks in a most atraumatic manner with the help of tweezer without disturbing the underlying new connective tissue formation. As there is no need for removal of absorbable membrane in group II, all the parameters were recorded after 6 months in both groups and the results were subjected to statistical analysis.
2.5. Statistical analysis
Paired ‘t’ test was done to see the difference between pre- and post-treatment values in each group (intragroup). Student ‘t’ test was employed to compare the data in two sets of groups to find out the significance of difference in their means (intergroup). Probability values (p) less than 0.05 were considered significant. A ‘p’ value less than 0.01 was considered highly significant while a ‘p’ value less than 0.001 was considered very highly significant.
3. Results
The responses of the two membranes were analyzed by comparing the plaque index, gingival index, position of GM, CAL, VPD, horizontal probing depth, and horizontal component of furcation defect after flap elevation, as summarized in Table 1, Table 2, Table 3.
Table 1.
Clinical parameters recorded at baseline in the group I.
| Group I (nonabsorbable barrier membrane) | ||||
|---|---|---|---|---|
| Clinical parameter | Baseline (Mean ± SD) |
6 months (Mean ± SD) |
‘t’ | ‘p’ |
| Position of gingival margin | 1.143 ± 1.069 | 1.857 ± 0.690 | −2.5 | 0.047,SS |
| Clinical attachment level | 5.714 ± 1.704 | 4.143 ± 1.952 | 7.778 | 0.000,SS |
| Vertical probing depth | 4.571 ± 2.149 | 2.286 ± 2.289 | 8.000 | 0.000,SS |
| Horizontal probing depth | 4.571 ± 0.787 | 3.143 ± 0.900 | 4.804 | 0.003,SS |
| Horizontal component of furcation defect after flap elevation | 4.000 ± 0.577 | 2.857 ± 0.690 | 8.000 | 0.000,SS |
SS, statistically significant.
Table 2.
Clinical parameters recorded at baseline in the group II.
| Group II (absorbable barrier membrane) | ||||
|---|---|---|---|---|
| Clinical parameter | Baseline (Mean ± SD) |
6 months (Mean ± SD) |
‘t’ | ‘p’ |
| Position of gingival margin | 1.286 ± 1.380 | 1.857 ± 0.900 | −1.549 | 0.172,NS |
| Clinical attachment level | 4.857 ± 2.116 | 3.143 ± 1.464 | 6.000 | 0.001,SS |
| Vertical probing depth | 3.571 ± 0.787 | 1.286 ± 0.951 | 12.394 | 0.000,SS |
| Horizontal probing depth | 5.857 ± 1.574 | 3.429 ± 0.976 | 5.667 | 0.001,SS |
| Horizontal component of furcation defect after flap elevation | 5.571 ± 1.718 | 3.000 ± 1.528 | 5.347 | 0.002,SS |
NS, not significant; SS, statistically significant.
Table 3.
Comparison of clinical parameters between the group I and group II at 6 months postoperatively.
| Clinical parameter | Nonabsorbable (Mean ± SD) |
Absorbable (Mean ± SD) |
‘t’ | ‘p’ |
|---|---|---|---|---|
| Change in position of gingival margin | 0.857 ± 0.690 | 0.714 ± 0.756 | 0.369 | 0.718,NS |
| Gain in clinical attachment level | 1.571 ± 0.535 | 1.714 ± 0.756 | 0.408 | 0.690,NS |
| Reduction in vertical probing depth | 2.286 ± 0.756 | 2.286 ± 0.488 | 0.000 | 1.000,NS |
| Reduction in horizontal probing depth | 1.429 ± 0.787 | 2.429 ± 1.134 | 1.917 | 0.079,NS |
| Reduction in the horizontal component of furcation defect at 6 months after flap elevation (horizontal bone bill) | 1.143 ± 0.378 | 2.571 ± 1.272 | 2.847 | 0.015,SS |
NS, not significant; SS, statistically significant.
3.1. Plaque index
In this study, a reduction in plaque index score was observed in both the groups postoperatively. The intergroup comparison did not show any statistically significant difference.
3.2. Gingival index
Reduction in gingival index score was observed in the study in both the groups postoperatively. There was no statistically significant difference on intergroup comparison.
3.3. Position of GM
There was statistically significant change in the position of GM in group I but no significant change in the group II, which signifies that there was more gingival recession in the group I.
3.4. CAL
Gain in CAL was observed in both the groups postoperatively, which was statistically significant, but on intergroup comparison, no statistically significant difference was found.
3.4.1. VPD
Reduction in probing pocket depth was observed in both the groups postoperatively, which was statistically significant, but on intergroup comparison, no statistically significant difference was found.
3.4.2. Horizontal probing depth
Reduction in horizontal probing depth was observed in both the groups postoperatively, which was statistically significant, but on intergroup comparison, it was higher in group II, but no statistically significant difference was found.
3.4.3. Horizontal component of furcation defect after flap elevation
Statistically significant reduction in horizontal component of furcation defect measured after flap reflection was observed in both the groups postoperatively. On intergroup comparison, reduction was significantly higher for group II.
Reduction in the horizontal component of furcation defect at 6 months was after flap elevation (horizontal bone fill).
Horizontal bone fill was observed in both the groups postoperatively, which was statistically significant, and on intergroup comparison, it was significantly higher in group II than group I.
4. Discussion
Predictable regeneration of osseous defects is a challenge in periodontal therapy. Numerous methods have been used to enhance regeneration of lost periodontal attachment and bone, like autogenous bone graft or allografts with GTR (combination therapy)* or GTR technique alone. It facilitates the formation of a new connective tissue attachment in vertical osseous defects and furcation defects. In this technique, the membranes were implanted between the root surface and the mucoperiosteal flap, which allow a selective proliferation of periodontal ligament cells into the defect space by excluding the cells of the gingival epithelium and connective tissue.9 It is suggested from other studies that such combination treatment may be more beneficial than using barriers alone.4
The absorbable duramater membrane used in this study is pliable when moist, and adapts better to the root trunk at the coronal margin. In addition, the collagen provides a thrombogenic surface that is sealed coronally to the root surface through the initial fibrin clot and technically less sensitive in terms of shaping and positioning. The wound margin is biologically sealed as opposed to an open wicking effect with other barriers.
The nonabsorbable d-PTFE membrane used in this study has some inherent advantages over the absorbable membrane. It gives the clinician greater control over the length of time as the membrane remain in place.10 Generally, the disadvantage of using nonabsorbable membrane is the need of second surgery for membrane removal, but as the d-PTFE is dense in nature, there is no mechanical locking of the membrane into the healing connective tissue and it can be removed by grasping the edge of the membrane. The disadvantage of d-PTFE membrane is incomplete adaptation of the membrane to the irregularity and concavities of the furcation root trunk; thus, the membrane does not completely isolate the defect from migrating connective tissue and epithelial cells.
Soft tissue measurements alone can be misleading and thus hard tissue parameters were assessed during reentry surgery. Reentry measurements of horizontal component of furcation defect (horizontal bone fill) gave a more reliable indication of treatment effectiveness.11 The results of this study indicate that class II furcations treated with both nonabsorbable and absorbable barrier membranes healed with favorable changes in the measured clinical parameters. Gain in CAL, reductions in VPD, horizontal probing depth, and horizontal component of furcation defect after flap elevation (horizontal bone fill) were clinically and statistically significant in both groups but comparison between the groups did not show statistically significant finding except horizontal bone fill, which was more favorable with group II (Table 1, Table 2, Table 3).
The mean reduction in VPD in group I can be compared to the observations made by McDonald et al.12 and Blumenthal et al.13 The VPD reduction in group II is in agreement with the observations made by Caffesse et al.14 and Yukna et al.15 Comparatively, the differences were insignificant, and found to be consistent with the studies of Evan et al.,16 Alarrayed et al.,17 and Black et al.18
The gain in CAL followed almost the same pattern as the VPD reduction, found to be consistent with Cury et al.19 and Black et al.18 However, in sites using duramater membrane, the gain in CAL values were higher but differences between both groups were not statistically significant (p ≤ 0.690). These observations were comparable with the previous reports of Hugoson et al.20 and Caffesse et al.14
The gain is horizontal probing depth amounted to be 1.43 mm in group I and 2.43 mm in group II. This finding of the study endorse the studies of Machtei et al.21 who found a gain of 1.8 mm using d-PTFE barrier and 2.5 mm using the collagen barrier membrane (Blumenthal et al.).13
At the end of the study period, in group II, where Duramater membrane was used, the GM was maintained close to presurgical level, whereas at sites using d-PTFE membrane (Group-I), the GM was located at a more apical level as compared to baseline. It can be speculated that the increased recession in group I was caused by overthinning of the flap. Since probing reduction was similar in both groups, the difference in gingival recession can most probably be explained by the lower level of attachment gain in group I.
The primary response variable in the treatment of furcation defect is the direct measurement of horizontal component of furcation defect (horizontal bone fill) during reentry surgery. There was significant improvement of horizontal bone fill in both groups. Comparison between the groups showed significant change in group II (p = 0.015). This finding compares favorably with previous studies using collagen membrane of Pal et al.,22 Yukna et al.,15 and Blumenthal et al.13
5. Conclusion
It can be concluded that both membranes resulted in clinically and statistically significant improvements in class-II mandibular furcation defects, which suggest that the success of GTR procedure is not only necessarily related to the type of membrane material used but also to many extrinsic factors, such as membrane handling characteristics, ease of placement, biological acceptance, defect morphology, and plaque removal.
However, with respect to horizontal bone fill, absorbable barrier membrane showed better results, and therefore, long-term studies with larger sample size and more advanced techniques for the assessment of changes in the parameters should be carried out for the results to be more conclusive.
Conflicts of interest
The authors have none to declare.
References
- 1.Quinones C.R., Carellas I.G., Caffessee R.G. Guided periodontal tissue regeneration (GPTR): an update. Pract Periodontics Aesthet Dent. 1996;8(2):169–180. [PubMed] [Google Scholar]
- 2.Nyman S., Lindhe J., Karring T. New attachment following surgical treatment of human periodontal disease. J Clin Periodontol. 1982;9:290–296. doi: 10.1111/j.1600-051x.1982.tb02095.x. [DOI] [PubMed] [Google Scholar]
- 3.Niederman R., Savitt E.D., Heeley J.D., Duckworth J.E. Regeneration of furca bone using Gore-Tex periodontal material. Int J Periodontics Restorative Dent. 1989;9:469–480. [PubMed] [Google Scholar]
- 4.Lekovik V., Kenney E.B., Carranza F.A., Jr. Treatment of class II furcation defects using porous hydroxyapatite in conjunction with polytetrafluoroethylene membrane. J Periodontol. 1990;61:575–578. doi: 10.1902/jop.1990.61.9.575. [DOI] [PubMed] [Google Scholar]
- 5.Crump T.B., Rivera-Hidalgo F., Harrison J.W., Williams F.E., Guo I.Y. Influence of three membrane type on healing of bone defects. Oral Surg Oral Med Oral Histol. 1996;82(4):365–374. doi: 10.1016/s1079-2104(96)80299-x. [DOI] [PubMed] [Google Scholar]
- 6.Busschop J., De Boever J. Clinical and histological characteristics of lyophilized allogenic duramater in periodontal bony defects in humans. J Clin Periodontol. 1983;10:399–411. doi: 10.1111/j.1600-051x.1983.tb01289.x. [DOI] [PubMed] [Google Scholar]
- 7.Pitaru S., Tal H., Soldinger M. Partial regeneration of periodontal tissues using collagen barriers. Initial observations in the canine. J Periodontol. 1988;59:380–386. doi: 10.1902/jop.1988.59.6.380. [DOI] [PubMed] [Google Scholar]
- 8.Pontoriero R., Lindhe J., Nyman S. Guided tissue regeneration in degree II furcations involved mandibular molars. A clinical study. J Clin Periodontol. 1988;15:247–254. doi: 10.1111/j.1600-051x.1988.tb01578.x. [DOI] [PubMed] [Google Scholar]
- 9.Isidor F., Karring T., Nyman S., Lindhe J. The significance of coronal growth of periodontal ligament tissue for new attachment formation. J Clin Periodontol. 1986;13:145–150. doi: 10.1111/j.1600-051x.1986.tb01448.x. [DOI] [PubMed] [Google Scholar]
- 10.Stephen P.W., Greenwell H., Hill M., Drisko C., Pickman K., Scheetz J.P. Comparison of porous and non-porous Teflon membrane plus a xenograft in the treatment of vertical osseous defects. A clinical re-entry study. J Periodotol. 2003;74(8) doi: 10.1902/jop.2003.74.8.1161. [DOI] [PubMed] [Google Scholar]
- 11.Machtei E.E. Outcome variables for the study of periodontal regeneration. Ann Periodontol. 1997;2:229–239. doi: 10.1902/annals.1997.2.1.229. [DOI] [PubMed] [Google Scholar]
- 12.Mac Donald F.S., Nowzari H., Contreras A., Flynn J., Morrison J., Slots J. Clinical and microbiological evaluation of a bioabsorbable and non-absorbable barrier membrane in the treatment of periodontal intraosseous lesions. J Periodontol. 1998;69:445–453. doi: 10.1902/jop.1998.69.4.445. [DOI] [PubMed] [Google Scholar]
- 13.Blumemthal N.M. A clinical comparison of collagen membranes with e-PTFE membranes in the treatment of human mandibular buccal class II furcation defects. J Periodontol. 1993;64:925–933. doi: 10.1902/jop.1993.64.10.925. [DOI] [PubMed] [Google Scholar]
- 14.Caffesse R.G., Mota L.E., Quinons C.R. Clinical comparison of resorbable and non-resorbable barrier for gingival periodontal tissue regeneration. J Clin Periodontol. 1997;24(10):747–752. doi: 10.1111/j.1600-051x.1997.tb00192.x. [DOI] [PubMed] [Google Scholar]
- 15.Yukna C.N., Yukna R.A. Multi-center evaluation of bioabsorbable collagen membrane for guided tissue regeneration in human class II furcation. J Periodontol. 1996;67:650–657. doi: 10.1902/jop.1996.67.7.650. [DOI] [PubMed] [Google Scholar]
- 16.Evan G.H., Yukna R.A., Cambre K.M., Gardiner D.L. Clinical regeneration with guided tissue regeneration. Curr Opin Periodontol. 1997;4:74–81. [PubMed] [Google Scholar]
- 17.Al-Arrayed F., Adam S., Moran J. Clinical trials of cross linked human type I collagen as a barrier material in surgical periodontal treatment. J Clin Periodontol. 1995;22:371–379. doi: 10.1111/j.1600-051x.1995.tb00163.x. [DOI] [PubMed] [Google Scholar]
- 18.Black B.S., Gher M.E., Sandifer J.B., Fucini S.E., Richardson A.C. Comparative study of collagen and expanded polyterafluorethylene membrane in the treatment of human class II furcation defect. J Periodontol. 1994;65:598–604. doi: 10.1902/jop.1994.65.6.598. [DOI] [PubMed] [Google Scholar]
- 19.Cury P.R., Sallum F.H. Long-term results of guided tissue regeneration therapy in the treatment of Class II furcation defects. A randomized clinical trial. J Periodontol. 2003;74:3–9. doi: 10.1902/jop.2003.74.1.3. [DOI] [PubMed] [Google Scholar]
- 20.Hugoson A., Ravald N., Fornell J. Treatment of Class II furcation involvement in humans with bioresorbable & non-resorbable guided tissue regeneration barriers. A randomized multi centre study. J Periodontol. 1995;66:624–634. doi: 10.1902/jop.1995.66.7.624. [DOI] [PubMed] [Google Scholar]
- 21.Machtei F.E., Dunford R.G., Norderyd O.M., Zambon J.J., Genco R.J. Guided tissue regeneration and anti-infective therapy in the treatment of class II furcation defects. J Periodontol. 1993;64:968–973. doi: 10.1902/jop.1993.64.10.968. [DOI] [PubMed] [Google Scholar]
- 22.Pal T.K., Mahajan A., Chakraburty H. Clinical evaluation of Collagen Chitosan as a barrier membrane in the treatment of periodontal osseous defects. JISP. 2003:36–45. [Google Scholar]