

Abstract
Introduction The anterior petrosectomy is a well-defined skull base approach to lesions such as petroclival meningiomas, posterior circulation aneurysms, petrous apex lesions (chondrosarcomas, cholesteatomas), ventrolateral brainstem lesions, clival chordomas, trigeminal neurinomas, and access to cranial nerves III, IV, V, and VII.
Methods and Materials Fourteen anterior petrosectomies on eight cadaveric heads were performed in a skull base dissection laboratory. Predissection and postdissection thin-cut computed tomography scans were obtained to compare the bone resection. A computer program was used (InVivo5, Anatomage, San Jose, California, United States) to measure the bone resection and the improved viewing angle.
Results The average bone removed in each plane was as follows: anterior to posterior plane was 10.57 mm ± 2.00 mm, superior to inferior was 9.39 mm ± 1.67 mm, and lateral to medial was 17.46 mm ± 4.64 mm. The average increased angle of view was 13.01 ± 2.35 degrees (Table 1). The average volume was 1786.94 ± 827.40 mm3.
Conclusions Anterior petrosectomy is a useful approach to access the ventrolateral brainstem region. We present a cadaveric study quantitating the volume of bone resection and improvement in the viewing angle. These data provide useful preoperative information on the utility of this skull base approach and the gain in the viewing angle after bony removal.
Keywords: anterior petrosectomy, brainstem, middle fossa, skull base
Introduction
The anterior petrosectomy is a well-defined skull base approach to lesions such as petroclival meningiomas, posterior circulation aneurysms, petrous apex lesions (chondrosarcomas, cholesteatomas), ventrolateral brainstem lesions, clival chordomas, trigeminal neurinomas, and access to cranial nerves III, IV, V, and VII.1 2 3 4 5 6 7 8 9 Access is gained via a middle fossa approach with extradural dissection to expose the greater superficial petrosal nerve (GSPN) and trigeminal nerve.
Although this approach may not be used as frequently due to the advancements in endovascular therapy, it is still used routinely in tumors and cerebrovascular pathology that is not amenable to endovascular therapy. Surgical approaches to pathology hidden behind the posterior clinoid or dorsum sella and upper clivus usually require an adjunct approach to the standard craniotomy.10 The importance of maintaining skills in skull base surgery allows the surgeon to convert deep narrow operative corridors into wider shallower exposures, improving maneuverability and minimizing retraction.
With recent literature describing small variations in the traditional anterior petrosectomy, we sought to calculate how much bone resection is required to perform an anterior petrosectomy.11 With quantitative knowledge, variations and minimizing resection while achieving adequate exposure will provide a better understanding of this approach.
Methods and Materials
Cadaver Protocol
The dissections were performed in a skull base dissection laboratory. Eight formalin-fixed cadaveric heads were dissected. All dissections were performed by a single surgeon to ensure consistency. Each cadaveric head received a 1-mm acquisition thin-cut computed tomography (CT) scan prior to the dissection. Initially, two cadaveric heads underwent a unilateral anterior petrosectomy on the right side. To conserve the number of cadaveric specimens, bilateral anterior petrosectomies were performed on the following six cadaveric heads totaling 14 dissections. After the anterior petrosectomy, another thin-cut CT scan was obtained.
The radiographic images were obtained in DICOM format and uploaded to a computer software program (InVivo5, Anatomage, San Jose, California, United States). The predissection and postdissection images were superimposed to compare the amount of bone resection. In this program, the obtained images were not only available for viewing but were used to make three-dimensional reconstructions. Axial, sagittal, and coronal measurements of the bone resection were made for each anterior petrosectomy. The directions of measurements were anterior-posterior, superior-inferior, and lateral-medial, respectively (Figs. 1 and 2). To measure the increased angle of view, two lines were drawn on the coronal view of the CT where bone removal was visualized. Both lines started at the inferior edge of the craniectomy. The first line was drawn from the inferior edge of the craniectomy to the petrous ridge. This line signified the predissection view of the posterior fossa. The second line was drawn from the inferior edge of the craniectomy to the most medial portion of bony removal. This line signified the postdissection view of the posterior fossa. After superimposing the predissection and postdissection images, the angle of view gained by the dissection was calculated (Fig. 3).
Fig. 1.

Computed tomography scan with the anterior-posterior measurement on an axial view.
Fig. 2.
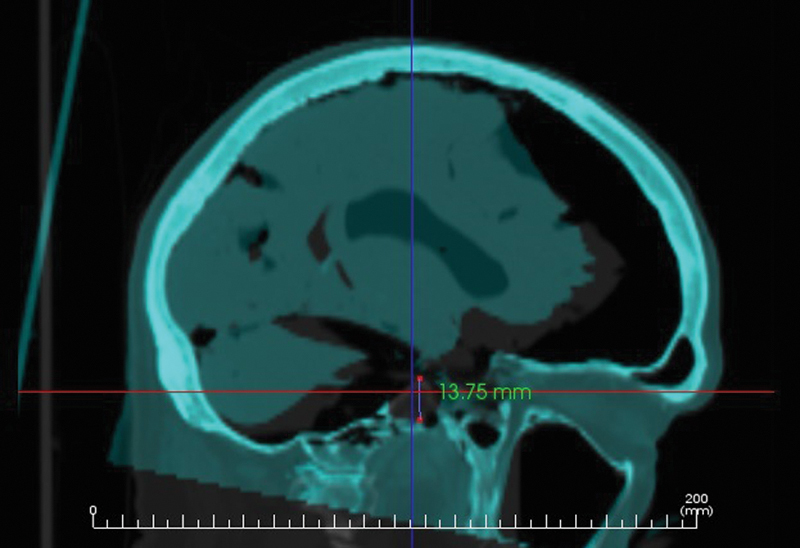
Computed tomography scan with the superior-inferior measurement on a sagittal view.
Fig. 3.

Calculation of the viewing angle. From the most inferior aspect of the craniotomy, at the floor of the middle fossa, a line was measured to the petrous apex. After the anterior petrosectomy, the line was drawn to the medial extent of the resection, thus providing an angle of view gained from the resection.
Surgical Technique for Anterior Petrosectomy
The cadaveric head was fixated in a three-point Mayfield clamp, with the floor of the middle fossa perpendicular to the ground. In the operating room, we routinely use a lumbar drain for cerebrospinal fluid (CSF) drainage to aid in separation of the dura when performing the craniotomy and extradural dissection. A curvilinear incision beginning from the root of the zygoma, anterior to the tragus, was extended superiorly above the superior temporal line. The temporalis fascia and muscle were incised at the superior temporal line, leaving a thin myofascial cuff. The muscle and fascia were dissected subperiosteally and reflected anteroinferiorly. After a temporal craniectomy was performed, excess temporal bone was removed to ensure the craniectomy was flush with the floor of the middle fossa.
The dura was dissected off the floor of the middle fossa extradurally, in a posterior to anterior fashion. The middle meningeal artery was identified entering through the foramen spinosum and subsequently divided. Careful dissection along the skull base allowed identification and preservation of the GSPN. Tracing the GSPN posteriorly will lead to the geniculate ganglion. In the operating room, this is usually performed with a facial nerve stimulator to notify the surgeon of the proximity to the GSPN.
After the mandibular branch of the trigeminal nerve (V3), trigeminal impression, and arcuate eminence were identified, the petrous apex was drilled (Fig. 4). The bony removal was localized between three structures: posterior to V3, medial to GSPN, and anterior to the arcuate eminence. The arcuate eminence indicates the location of the superior semicircular canal. The medial extent of the dissection entailed removal of the petrous ridge within the confined anterior, posterior, and lateral borders until the posterior fossa dura was identified. The borders of bone resection include GSPN laterally, V3 medially, and the arcuate eminence posteriorly (Fig. 5). In our dissections, we did not drill into the arcuate eminence because it may be unnecessary for this approach and increases the risk of hearing loss.
Fig. 4.

Three-dimensional reconstruction based on a computed tomography scan from a cadaveric dissection. With temporal lobe retraction, the trigeminal ganglion and branches of the trigeminal nerve can be visualized.
Fig. 5.

Visualization of neural structures after an anterior petrosectomy. The proximal trigeminal root in addition to cranial nerve IV and VI can be visualized.
Results
Table 1 shows each measurement and increase in angle of view. The average bone removed in each plane was as follows: anterior to posterior plane was 10.90 mm ± 2.33 mm, superior to inferior was 9.78 mm ± 2.20 mm, and lateral to medial was 18.40 mm ± 5.77 mm. The average increased angle of view was 12.01 ± 2.27 degrees. The average calculated volume was 2167.86 ± 1676.93 mm3.
Table 1. Measurements of anterior petrosectomy.
| Cadaver | Axial, mm, anterior–posterior | Sagittal, mm, superior–inferior | Coronal, mm, lateral–medial | Calculated volume, mm3 | Increased angle of view, degrees |
|---|---|---|---|---|---|
| 4535–R | 9.08 | 8.22 | 16.69 | 1245.70 | 11.7 |
| 4541–R | 14.18 | 11.65 | 22.09 | 3649.20 | 13.8 |
| 4544–L | 8.25 | 8.82 | 14.29 | 1039.81 | 11.8 |
| 4544–R | 9.4 | 12.58 | 13.95 | 1649.62 | 17.9 |
| 4545–L | 7.25 | 8.51 | 12.57 | 775.54 | 12.7 |
| 4545–R | 13.24 | 7.57 | 15.60 | 1563.54 | 11.3 |
| 4546–L | 9.01 | 10.61 | 13.76 | 1315.40 | 13.4 |
| 4546–R | 11.16 | 8.9 | 27.09 | 2690.69 | 11.8 |
| 4549–L | 12.52 | 7.75 | 17.46 | 1694.14 | 10.8 |
| 4549–R | 11.37 | 11.6 | 17.98 | 2371.42 | 14.6 |
| 4550–L | 10.7 | 10.51 | 26.6 | 2991.36 | 17.8 |
| 4550–R | 9.13 | 8.6 | 16.38 | 1286.13 | 10.8 |
| 4551–L | 10.48 | 8.6 | 13.4 | 1207.72 | 10.9 |
| 4551–R | 12.22 | 7.6 | 16.55 | 1537.03 | 12.9 |
| Average | 10.57 ± 2.00 | 9.39 ± 1.67 | 17.46 ± 4.64 | 1786.94 ± 827.40 | 13.01 ± 2.35 |
Abbreviations: L, left side; R, right side.
Note: Measurements are of amount of bone removed in three planes (axial, sagittal, and coronal) and the increased field of view.
Discussion
The anterior petrosectomy was first described by Kawase et al.4 The authors originally described the anterior petrosectomy approach for the treatment of retrosellar and upper clival basilar bifurcation aneurysms.5 6 Since the description, several modifications have been made, such as a description of partial anterior petrosectomies.11
Three bony plates are described in the anterior petrosectomy. The posterolateral triangle, also known as the Glasscock triangle, is designated by the line from the foramen spinosum to the facial hiatus, the GSPN, and the mandibular branch of the trigeminal nerve. It is within this triangle where the petrous internal carotid artery (ICA) resides. This triangle can be used to expose the petrous ICA. The posteromedial triangle, also known as the Kawase triangle, is designated by the GSPN laterally, the petrous ridge medially, and the arcuate eminence posteriorly. The meatal plane is the flat area of bone that overlies the internal auditory meatus between the geniculate ganglion and arcuate eminence.12
As the field of skull base surgery has continued to strive for minimally invasive approaches and minimal disruption of neural structures, performing anterior petrosectomies have recently gained popularity through the endonasal endoscopic route.9 13 14 15 Day et al described an expanded anterior petrosectomy by displacing V3, providing a larger surgical corridor.16 Van Gompel et al recently compared the open anterior petrosectomy approach with the endonasal endoscopic approach.13 They found the endoscopic approach provides better access to the inferior portion of the petrous apex, and the open approach provides access to the superior portion of the petrous apex.
Thorough knowledge of the anatomy is a requirement for precise skull base dissection. Despite the numerous reports on the anterior petrosectomy approach, one must be familiar with the anatomy and potential complications. A dehiscence of the floor could provide unwanted exposure of the petrous segment of the ICA.17 Facial nerve palsy is a reported consequence of the anterior petrosectomy approach, despite avoidance of the facial nerve. This could be related to activation of a latent herpes virus, manipulation of the GSPN causing traction injury of the facial nerve, small vessel spasm, or neural edema.12 18 19 20 CSF fistula with extradural dissection can occur when watertight closure of the dura is not achieved.21 Excessive removal of bone posterior to the Kawase triangle could injure the cochlea or semicircular canals causing hearing loss.17
Skull base approaches provide maximum exposure, optimal angle of approach, and optimal viewing angle while minimizing retraction. As skull base surgery has progressed, several studies have analyzed the angle of approach between various craniotomies.22 23 With lesions located near the ventrolateral brainstem, the anterior petrosectomy provides an exposure with less temporal lobe retraction in comparison with the standard pterional or subtemporal approach. Aziz et al demonstrated the anterior petrosectomy is suitable for pathology up to 18 mm below the sella turcica.10 To our knowledge, the improvement in viewing angle has not previously been quantified. Our data showed that an anterior petrosectomy improves the angle of view by 12 degrees.
A few limitations exist with this study. There is inherently substantial variability between the relatively small numbers of dissections. The method used to calculate the volume resection (length times width times height) is ideal for a cube. Although the anterior petrous bone is described as a rhomboid shape, the volume calculation is a rough approximation of the bone resection.16 Because the measurements were made with computer software, it would be difficult to translate these measurements in the operative setting. One could argue that a small ruler could be used at the skull base, but the limited exposure and added time may be undesirable. Similar measurements of bony removal could be made on the cadaver specimen, potentially translating this information to the operating room; however, the practicality of this measurement may not warrant any increased risk during the surgery.
Conclusions
Anterior petrosectomy is a useful skull base approach to access the ventrolateral brainstem region. We presented a cadaveric study quantitating the volume of bone resection and improvement in the viewing angle. This provides the surgeon with useful preoperative assessment and planning for the utility of an anterior petrosectomy based on the location of the pathology, the viewing angle needed, and the amount of bony removal.
References
- 1.Friedman R A, Pensak M L, Tauber M, Tew J M Jr, van Loveren H R. Anterior petrosectomy approach to infraclinoidal basilar artery aneurysms: the emerging role of the neuro-otologist in multidisciplinary management of basilar artery aneurysms. Laryngoscope. 1997;107(7):977–983. doi: 10.1097/00005537-199707000-00027. [DOI] [PubMed] [Google Scholar]
- 2.House W F, Hitselberger W E, Horn K L. The middle fossa transpetrous approach to the anterior-superior cerebellopontine angle. Am J Otol. 1986;7(1):1–4. [PubMed] [Google Scholar]
- 3.Kawase T, Bertalanffy H, Otani M, Shiobara R, Toya S. Surgical approaches for vertebro-basilar trunk aneurysms located in the midline. Acta Neurochir (Wien) 1996;138(4):402–410. doi: 10.1007/BF01420302. [DOI] [PubMed] [Google Scholar]
- 4.Kawase T Shiobara R Toya S Anterior transpetrosal-transtentorial approach for sphenopetroclival meningiomas: surgical method and results in 10 patients Neurosurgery 1991286869–875.; discussion 875–876 [PubMed] [Google Scholar]
- 5.Kawase T, Toya S, Shiobara R, Mine T. Transpetrosal approach for aneurysms of the lower basilar artery. J Neurosurg. 1985;63(6):857–861. doi: 10.3171/jns.1985.63.6.0857. [DOI] [PubMed] [Google Scholar]
- 6.Kawase T, Toya S. Vienna, Austria: Springer-Verlag; 1994. Anterior transpetrosal approach for basilar trunk aneurysms: further experience; pp. 255–260. [Google Scholar]
- 7.Megerian C A, Chiocca E A, McKenna M J, Harsh G F IV, Ojemann R G. The subtemporal-transpetrous approach for excision of petroclival tumors. Am J Otol. 1996;17(5):773–779. [PubMed] [Google Scholar]
- 8.Slater P W, Welling D B, Goodman J H, Miner M E. Middle fossa transpetrosal approach for petroclival and brainstem tumors. Laryngoscope. 1998;108(9):1408–1412. doi: 10.1097/00005537-199809000-00030. [DOI] [PubMed] [Google Scholar]
- 9.Zhao J C Liu J K Transzygomatic extended middle fossa approach for upper petroclival skull base lesions Neurosurg Focus 2008256E5; discussion E5 [DOI] [PubMed] [Google Scholar]
- 10.Aziz K M van Loveren H R Tew J M Jr Chicoine M R The Kawase approach to retrosellar and upper clival basilar aneurysms Neurosurgery 19994461225–1234.; discussion 1234–1236 [PubMed] [Google Scholar]
- 11.Fukuda H, Evins A I, Burrell J C. et al. Partial anterior petrosectomies for upper basilar artery trunk aneurysms: a cadaveric and clinical study. World Neurosurg. 2014;82(6):1113–1119. doi: 10.1016/j.wneu.2014.03.034. [DOI] [PubMed] [Google Scholar]
- 12.Guthikonda B Pensak M L Theodosopoulos P V Delayed facial palsy after the anterior petrosal approach: case report and review of the literature Neurosurgery 2010664E845–E846.; discussion E846 [DOI] [PubMed] [Google Scholar]
- 13.Van Gompel J J, Alikhani P, Tabor M H. et al. Anterior inferior petrosectomy: defining the role of endonasal endoscopic techniques for petrous apex approaches. J Neurosurg. 2014;120(6):1321–1325. doi: 10.3171/2014.2.JNS131773. [DOI] [PubMed] [Google Scholar]
- 14.Hofstetter C P, Singh A, Ananda V K, Kacker A, Schwartz T H. The endoscopic, endonasal, transmaxillary transpterygoid approach to the pterygopalantine fossa, infratemporal fossa, petrous apex, and the Meckel cave. Clinical article. J Neurosurg. 2010;113(5):967–974. doi: 10.3171/2009.10.JNS09157. [DOI] [PubMed] [Google Scholar]
- 15.Zanation A M, Snyderman C H, Carrau R L, Gardner P A, Prevedello D M, Kassam A B. Endoscopic endonasal surgery for petrous apex lesions. Laryngoscope. 2009;119(1):19–25. doi: 10.1002/lary.20027. [DOI] [PubMed] [Google Scholar]
- 16.Day J D Fukushima T Giannotta S L Microanatomical study of the extradural middle fossa approach to the petroclival and posterior cavernous sinus region: description of the rhomboid construct Neurosurgery 19943461009–1016.; discussion 1016 [DOI] [PubMed] [Google Scholar]
- 17.Steiger H J, Hänggi D, Stummer W, Winkler P A. Custom-tailored transdural anterior transpetrosal approach to ventral pons and retroclival regions. J Neurosurg. 2006;104(1):38–46. doi: 10.3171/jns.2006.104.1.38. [DOI] [PubMed] [Google Scholar]
- 18.Gianoli G J. Viral titers and delayed facial palsy after acoustic neuroma surgery. Otolaryngol Head Neck Surg. 2002;127(5):427–431. doi: 10.1067/mhn.2002.129817. [DOI] [PubMed] [Google Scholar]
- 19.Grant G A, Rostomily R R, Kim D K. et al. Delayed facial palsy after resection of vestibular schwannoma. J Neurosurg. 2002;97(1):93–96. doi: 10.3171/jns.2002.97.1.0093. [DOI] [PubMed] [Google Scholar]
- 20.Scheller C, Strauss C, Fahlbusch R, Romstöck J. Delayed facial nerve paresis following acoustic neuroma resection and postoperative vasoactive treatment. Zentralbl Neurochir. 2004;65(3):103–107. doi: 10.1055/s-2004-816268. [DOI] [PubMed] [Google Scholar]
- 21.Sekhar L N Kalia K K Yonas H Wright D C Ching H Cranial base approaches to intracranial aneurysms in the subarachnoid space Neurosurgery 1994353472–481.; discussion 481–483 [DOI] [PubMed] [Google Scholar]
- 22.Alaywan M, Sindou M. Fronto-temporal approach with orbito-zygomatic removal. Surgical anatomy. Acta Neurochir (Wien) 1990;104(3–4):79–83. doi: 10.1007/BF01842824. [DOI] [PubMed] [Google Scholar]
- 23.Emery E, Alaywan M, Sindou M. Respective indications of orbital and/or zygomatic arch removal combined with fronto-pteriono-temporal approaches. 58 cases [in French] Neurochirurgie. 1994;40(6):337–347. [PubMed] [Google Scholar]