

Abstract
Purpose:
This study aimed at conducting a systematic review in health professions education of determinants, mediators and outcomes of students’ motivation to engage in academic activities based on the self-determination theory’s perspective.
Methods:
A search was conducted across databases (MEDLINE, CINHAL, EMBASE, PsycINFO, and ERIC databases), hand-search of relevant journals, grey literature, and published research profile of key authors. Quantitative and qualitative studies were included if they reported research in health professions education focused on determinants, mediators, and/or outcomes of motivation from the self-determination and if meeting the quality criteria.
Results:
A total of 17 studies met the inclusion and quality criteria. Articles retrieved came from diverse locations and mainly from medical education and to a lesser extent from psychology and dental education. Intrapersonal (gender and personality traits) and interpersonal determinants (academic conditions and lifestyle, qualitative method of selection, feedback, and an autonomy supportive learning climate) have been reported to have a positive influence on students’ motivation to engage in academic activities. No studies were found that tested mediation effects between determinants and students’ motivation. In turn, students’ self-determined motivation has been found to be positively associated with different cognitive, affective, and behavioural outcomes.
Conclusion:
This study has found that generally, motivation could be enhanced by changes in the educational environment and by an early detection of students’ characteristics. Doing so may support future health practitioners’ self-determined motivation and positively influence how they process information and their emotions and how they approach their learning activities.
Keywords: Cognition, Medical education, Motivation, Personal autonomy, Review literature as topic
Introduction
Motivation is increasingly becoming a major area of interest within the field of health professions’ education as it has been suggested to have a pivotal role for students’ academic success and wellbeing and for patients’ outcomes [1]. Amongst the several motivational theories, the self-determination theory (SDT) has gathered special attention in recent years, generating evidence across numerous domains, such as education, health, and psychology [2]. Moreover, several authors have stressed the role of SDT and its implications for health education, suggesting that many of its principles may explain why students thrive in clinical education settings [1,3].
SDT investigates the roles of self-determined and controlled behaviours in different environments, postulating motivation as a multidimensional construct based on three different quality types; in a continuum ranging from the least to the most self-determined forms there is amotivation, controlled motivation, and autonomous motivation [2,4] (Fig. 1). Autonomous and controlled motivation refer to an individual’s intention to act (though leading to different outcomes), conversely amotivation refers to the lack of it. The latter is therefore represented by a non-regulation state that results from an individual not valuing a behaviour or outcome, in other words, what students’ do seems to be unrelated to the consequences derived from their actions.
Fig. 1.

The self-determination theory continuum of motivation. From Ryan et al. Contemp Educ Psychol 2000;25:54-67, with permission from Elsevier [4].
Following the continuum, controlled motivation refers to pursuing an activity out of a sense of obligation, or as a means to an end. It has been subdivided into two types of regulation that can be ordered along the continuum. The lower self-determined form is external regulation, in which students engage in activities mainly to obtain rewards or to avoid punishment. This is followed by introjected regulation, in which individuals begin to internalize the reasons for their actions; however, behaviour is still regulated by external demands or requirements from the environment to avoid internal conflict, such as shame or guilt [5].
Autonomous motivation refers to engaging out of pleasure and satisfaction and/or by valuing the importance of an activity. It has also been subdivided into two types of regulation, on the one hand there is identified regulation, in which behaviour becomes valued, important and emitted out of choice, and although the locus of causality is somewhat internal it stills represents an instrument to achieve an objective. On the other hand, there is internal regulation, which is usually referred to as intrinsic motivation, being this the most self-determined form of behaviour and denoting the drive to pursue an activity simply for the pleasure or satisfaction derived from it, without internal or external pressures [5]. Intrinsic Motivation has been considered as a global construct with three subdivisions being at the same level and not following a continuum, but categorized as subtypes. Firstly, there is intrinsic motivation to know, which relates to concepts such as curiosity or motivation to learn; secondly, there is intrinsic motivation towards accomplishments, which reflects commitment towards an activity for the pleasure and satisfaction gained when one attempts to accomplish or create something; and finally, there is intrinsic motivation to experience stimulation, which indicates engagement for fun, excitement, and positive sensations.
These concepts are important, as they explain large part of students’ behaviour and lead to significant and varied outcomes. As such, past research has shown that cognitive, behavioural, and affective outcomes become increasingly positive as actions are endorsed following the continuum pattern of motivation, from the lowest to the highest self-determined type [2]. For instance, several studies in higher education have found that internalisation of students’ motivation towards an autonomous form is associated with positive educational outcomes, e.g., deep study strategies, enhanced conceptual learning, and creativity. In contrast, least self-determined forms of motivation, such as controlled motivation and amotivation, have been associated with more negative outcomes, e.g., low competence and poor wellbeing [1].
From the above, the question that arises is how motivation is influenced and what makes a student adopt a certain type of regulation. SDT postulates that motivation is influenced by both intrapersonal and interpersonal factors [5]. Intrapersonal factors refer to an individual’s inherent characteristics (e.g., gender, age, or ethnicity) and to personality traits. On the other hand, interpersonal forces are represented by social factors, in other words, by social experiences in which others have powerful impact on our motivation. Previous studies have highlighted, in educational contexts, the influence of interpersonal factors such as teachers’ autonomy-support, extent of responsibility, selection procedure, and early patient contact [6,7].
In addition, SDT proposes that all individuals have the need to feel autonomous, competent, and related to the surrounding social environment in order to be self-determined in their actions [2]. Therefore, the effects of social factors on motivation are suggested to be indirect. Previous research has reported that social factors are mediated by how they facilitate or prevent an individual’s perception of the three basic psychological needs of autonomy, competence, and/or relatedness [1]; this facilitation supports and maintenances optimal motivation, leading to positive developmental and psychological outcomes. In contrast, social factors that do not facilitate individual’s perceptions of these needs will yield less optimal forms of motivation, leading to more negative outcomes. In the case of health professions education, the facilitation of self-determined forms of motivation is expected to contribute towards students becoming better practitioners.
Consequently, by studying different determinants and outcomes of motivation, educators may plan and implement interventions that stimulate students to engage in activities in a more self-determined fashion, which in turn may lead to positive outcomes benefiting themselves and their patients. The aim of this study, therefore, was to conduct a systematic review to answer the following questions in the context of health professions education: first, what is the evidence on different intrapersonal and interpersonal determinants of self-determined motivation and how are these associations characterised?; second, is there evidence for the mediating effect of the basic psychological needs satisfaction on the relationship between determinants and self-determined motivation?: and third, what is the evidence on different cognitive, affective, and behavioural outcomes of self-determined motivation and how are these associations characterised?
While Kusurkar et al. [8] conducted a literature review on motivation studies focusing on medical education from a general perspective, a growing body of literature has been developed in health professions’ education explicitly based on SDT. Therefore this review builds on previous research and focuses on determinants and outcomes of motivation in SDT-based research expanding the scope to all health professions and providing detailed evidence synthesis on what the current knowledge is, the identification of gaps, recommendations for future research, and stressing the crucial role that motivation has on the educational decision-making processes of future health professionals.
Methods
The review was conducted during June and September 2015, following the ‘structured approach to the reporting in healthcare education of evidence synthesis statement’ [9]. Ethics approval was obtained from the Medical School of the University of Glasgow, as being part of a larger project (project number: 200140106).
Data collection
The systematic search was conducted in four phases. Firstly, a comprehensive search was conducted throughout the Medline, CINHAL, Embase, PsycINFO, and ERIC databases. Three essential concepts were identified for the search strategy: ‘motivation based on SDT,’ ‘determinants, mediators, and outcomes,’ and ‘health professions education.’ These were expanded considering synonyms, alternative spelling, and related terms. Nevertheless, each database has its own indexed subject headings; therefore we adapted our keyword combination according to each thesaurus. The core search strategy for Medline is presented in Table 1.
Table 1.
Medline search strategy
| Search strategy | |
|---|---|
| Search based on concept 1: motivation based on SDT | - Subject headings: (MH "motivation+”) OR (MH "personal autonomy”) |
| - Free text search: academic motivation OR (intrinsic OR extrinsic OR controlled OR autonomous) w1 motivation OR self w1 determination w1 theory OR self w1 determination OR SDT OR self w1 regulation | |
| Search based on concept 2: determinants, mediators, and outcomes | - Subject headings: (MH "cognition”) OR (MH "behavior”) OR (MH "emotions+”) |
| - Free text search: determinants OR antecedents OR autonomy w1 support OR mediator OR mediation OR psychological w1 mediators OR autonomy OR competence OR relatedness OR outcome* OR consequence* OR (cognitive OR behavioural OR affective) w1 (outcome* OR consequence*) | |
| Search based on concept 3: health professions education | - Subject headings: (MH "education+”) OR (MH "education, Medical, undergraduate”) |
| - Free text search: 'postgraduate student*' OR (dental OR medical OR psychology OR nursing) w1 (education OR student OR school) OR health w1 professions w1 education OR clinical w1 teach* | |
| Search 1 AND Search 2 AND Search 3 |
3SDT, self-determination theory; MH, subject heading; +, explode function; w1, proximity command;
truncation.
Secondly, relevant journals were hand-searched through their printed/online versions, and articles were selected based on the relevance of their titles based on the PRISMA statement [10] (Fig. 2). Thirdly, to account for publication bias, unpublished and grey literature were accessed through the ‘system for information on grey literature in Europe’ (www.opengrey.eu) using the aforementioned set of keywords.
Fig. 2.

Flow chart summarising the review process with number of articles reviewed and retained at each stage. From Moher et al. PLoS Med 2009;6: e1000097 [10]. a)Academic Medicine, Advances in Health Science Education, Educational and Psychological Measurements, Educational Psychology, Education for Health, European Journal of Dental Education, Journal of Dental Education, Journal of Educational Evaluation for Health Professions, Journal of Personality, Medical Education, Medical Teacher, and Motivation and Emotions.
Finally, the publications of experts in the field were reviewed by accessing key authors’ ‘Research Gate’ profiles (www.researchgate.net) and through the publications of the faculty list on the ‘SDT Website’ (www.selfdeterminationtheory.org/faculty). In total, 4,058 article tittles were scoped, corresponding to the profiles of 93 researchers from areas such as general education, psychology, medicine and dentistry. This approach provided a useful way to systematically review SDT-related publications from leading authors and also provided a fast and simple way of contacting them when additional information was required.
To be included in the review, all references were assessed based on the inclusion/exclusion criteria described in Table 2. All retrieved articles were exported to a reference manager for selection procedures. This stage was divided in three phases conducted by two authors independently and moderated by a third author whenever in disagreement. In phase one, duplicates and irrelevant titles were removed. In phase two the abstracts of the remaining articles were reviewed using the inclusion/exclusion criteria. When there was doubt on the exclusion of a particular article, it was advanced to phase three, so it could be assessed based on the full text rather than on the abstract. In phase three, the full text of each article was screened, enabling a final decision. Subsequently, applying the same three phases, an ancestry search of the selected articles’ references was conducted through the Web of Science.
Table 2.
Setting the scope of the search: inclusion and exclusion criteria
| Inclusion criteria | Exclusion criteria |
|---|---|
| 1. Empirical studies based on the SDT perspective, focusing on determinants, mediating variables, or outcomes of motivation. | 1. Studies not empirical in nature like viewpoints, editorials, opinions or books. |
| 2. Empirical studies that report research on students or teachers in undergraduate or postgraduate health professions education. | 2. Studies on populations other than students or teachers in health professions education. |
| 3. Valid and reliable quantitative research. | 3. Studies not focusing on motivation from the SDT perspective and not considering determinants, mediating variables, or outcomes of motivation. |
| 4. Credible and dependable qualitative research. | 4. Studies referring to motivation in undergraduate or postgraduate contexts without a focus on health professions education. |
| 5. Articles available in English, Spanish and French language. | 5. Studies published in languages other than English, Spanish, or French. |
| 6. Studies published from 1971 (first SDT-related publication) to 2015. | 6. Studies published before year 1971. |
SDT, self-determination theory.
As a mixture of qualitative and quantitative papers were expected to emerge, we opted for the semi-structured quality analysis ‘Questions to ask of research or evaluation evidence,’ published in the first BEME guide [11]. This appraisal instrument is applicable to several methods; it has 17 items responding to a ‘yes/no’ question aimed at analysing the quality of different areas of a research paper.
Data analysis
A meta-analysis of results was not possible due to methodological heterogeneity, therefore we approached the review as a narrative synthesis through a thematic analysis using the Nvivo ver. 10.0 software (QSR International, Doncaster, Australia). A data extraction form was developed including key methodological information, selected findings, and comments relevant to the research question (Table 3). The thematic analysis facilitated the translation of concepts between studies by identifying prominent themes and summarising their findings under recurrent headings, therefore allowing the integration of qualitative and quantitative evidence [12].
Table 3.
Summary of key study characteristics
| Author(s) (year, country) [reference] | Research topics | Type of study | Sample | Data collection Instrumentsa) | Data analysis method* | Selected findings & comments on determinants, mediators and/or outcomes of self-determined motivation |
|---|---|---|---|---|---|---|
| Bailey & Phillips (2016, Australia) [26] | Explore relationships between motivation, university adaptation, wellbeing, and academic performance | Cross-sectional correlational | 184 First-year psychology students, 73% females, mean age 19.3 | Self-report of academic performance, academic motivation scale, student adaptation to college guestionnaire, the anxiety and depression subscales of general health guestionnaire, meaning in life guestionnaire, satisfaction with life scale and positive and negative affect schedule | Correlations and hierarchical regression | Outcomes: intrinsic motivation was positively associated with wellbeing, meaning in life, positive emotions and academic performance, and negatively associated with negative emotions. Amotivation had the reverse pattern. Introjected Regulation showed a positive association with positive emotions and with anxiety. Motivational orientations predicted wellbeing, mental health, and academic performance. |
| Baker (2004, UK) [27] | Examine relations between motivation and adjustment to university, stress, well-being and academic performance | Cross-sectional correlational | 91 Second-year psychology students, 78% females, mean age 19.5 | Self-report of academic performance, academic motivation scale, college adaptation guestionnaire, general health guestionnaire, and perceived stress scale | Correlations and hierarchical regression | Outcomes: Controlling for gender and age, amotivation led to worse psychosocial adjustment to university, higher levels of perceived stress, and greater psychological. Intrinsic motivation (to know) was associated with lower levels of stress. Neither extrinsic nor intrinsic motivation, nor amotivation were related to academic achievement. |
| Kusurkaretal. (2011,The Netherlands) [20] | Validity of the Strength of motivation for medical school guestionnaire | Cross-sectional Psychometric | 1,494 Medical students from two universities, 72% females | Strength of motivation for medical school guestionnaire, academic motivation scale and exhaustion subscale of Maslach burnout inventory | Correlations, group differences and exploratory factor analysis | Determinants: overall strength of motivation and its subscales of willingness to sacrifice, readiness to start and persistence correlations were positively correlated with autonomous motivation, and it decreased and became negative as moving towards controlled motivation and amotivation. |
| Kusurkaretal. (2013,The Netherlands) [17] | Explore relationships between motivation, study strategy, effort and academic performance by gender and method ofadmission | Cross-sectional correlational | 383 Second-to-six year medical students, 72% females, mean age 23.3 | Method ofadmission and academic performance provided by university. Study effort, academic motivation scale and revised study process guestionnaire | Correlations, regression, group differences and structured eguation modelling | Outcomes: relative autonomous motivation was positively associated with good study strategy, which was positively associated with high study effort and better performance. Females and gualitative selection procedures showed a higher self-determined profile. |
| Kusurkaretal. (2013,The Netherlands) [14] | Implications of gender on motivation, performance, learning approaches, exhaustion, autonomy support and perceived competence | Cross-sectional correlational | 95 Fourth year medical students, 71.5% females | Academic performance provided by university. Academic motivation scale, revised study process guestionnaire, Maslach burnout inventory, learning climate guestionnaire and perceived competence guestionnaire | Group differences | Determinants: males reported higher controlled motivation and higher perceived competence even when reporting higher surface learning strategy, lower deep learning strategy and lower or egual performance. |
| Kusurkaretal. (2013,The Netherlands) [16] | Generate motivational profiles and test associations with different outcomes | Quantitative, Cross-sectional correlational | 844 Year one-to-six medical students, 71.5% females | Academic performance provided by university. Academic motivation scale, study hours per week, study process guestionnaire, and exhaustion subscale of Maslach burnout inventory | Correlations, K-cluster, analysis ofvariance and multivariate analysis of covariance | Outcomes: high intrinsic low controlled motivation was associated with good study hours, deep learning strategy, good academic performance and low exhaustion. High intrinsic high controlled motivation was associated with a good learning profile, except showing high surface strategy. Low intrinsic high controlled and low intrinsic low controlled motivation were associated with least desirable learning behaviours. |
| Orsini etal. (2016, Chile) [23] | Understand how clinical teachers encourage intrinsic motivation | Phenomenology | 9 Clinical dental teachers, 7 males, mean age of teaching experience 15 | Semi-structured interviews on how teachers supported students'needs for autonomy, competence, and relatedness | Thematic analysis | Determinants: teachers emphasise the influence that the learning climate has on students'intrinsic motivation, stressing the relevance of empowering, supporting and building a horizontal relationship.Themes included: transference of responsibility; personal interests; constructive feedback; vicarious learning experience; teamwork, and safe environment. |
| Orsini etal. (2015, Chile) [18] | Validity of the academic motivation scale in a dental students sample | Cross-sectional Psychometric | 989 Year one-to-six dental students, 62% females, mean age 22.5 | Academic performance provided by university. Academic motivation scale, deep and surface motives subscales of revised study process guestionnaire, academic subscale of abbreviated five-factor self-concept guestionnaire, and positive subscale of positive and negative affect schedule | Confirmatory factor analysis, correlations and group differences | Determinants: third and fourth years showed the highest amotivation scores. |
| Outcomes: intrinsic and identified regulation showed positive correlations with deep motives, academic self-concept and positive affect, and negative correlation with surface motives. Amotivation showed the reverse pattern. | ||||||
| Park etal, (2012, Republic of Korea) [19] | Examine relationships between stress, motivation, personality, academic performance, and depression | Cross-sectional correlational | 160 First year medical students, 72.5% males | Academic performance provided by university. Academic motivation scale, medical stress scale, personality inventory, Beck depression inventory, and Hamilton depression scale | Correlations, group difference, regression and path analyses | Determinants: psychopathological was negatively correlated with self-determined motivation. |
| Sobral (2004, Brazil) [15] | Describe medical students'motivation relationships with different learning outcomes | Cross-sectional correlational with a longitudinal panel design component | 297 Second year medical students, 57% males, mean age 20.4 | Academic performance provided by university. Academic motivation scale, reflection-in-learning scale, approaches to studying inventory, 4 semesters follow-up on peer tutoring activity, and intention to continue studies | Correlations, K-cluster and group differences | Outcomes: autonomous motivation was associated with higher levels of meaning orientation, reflection in learning, academic achievement, cross-year peer-tutoring, and intention to continue with studies, and had negative relationship with reproductive orientation to learning. Amotivation showed the reverse pattern and controlled motivation was positively related to reproductive orientation. |
| Outcomes: self-determined motivation was positively associated with performance and negatively associated with depression. Stress was positively correlated with amotivation and identified regulation and negatively correlated with intrinsic motivation and with external regulation. | ||||||
| Stoeberetal. (2011, UK) [28] | Investigate relationships between passion for studying, academic engagement, burnout and motivation | Cross-sectional correlational | 103 Second-year psychology students, 89% females, mean age 20 | Passion scale, Utrecht Work Engagement Scale-student, Maslach burnout inventory, and Sheldon's idio-graphic method for motivational analysis | Correlations, multiple analysis ofvariance, multiple regression | Outcomes: autonomous motivation showed positive association with harmonious passion and engagement for studying, and negative significant association with burnout. Controlled motivation showed the reverse pattern. |
| Tanaka etal. (2009, Japan) [13] | Examine relationships between personality traits and intrinsic motivation | Cross-sectional correlational | 119 Second year medical students, 70% males, mean age 20.5 | Temperament and character inventory and intrinsic motivation scale toward learning. | Regression analyses | Determinants: on simple regression, persistence, self-direct-edness, cooperativeness and self-transcendence were positively associated with intrinsic motivation. On multiple regressions, adjusted for age and gender, persistence, self-directedness, and self-transcendence were positively associated with intrinsic motivation. |
| Tanaka etal. (2011 Japan) [21] | Examine relationships between academic and family conditions and intrinsic motivation | Cross-sectional correlational | 120 Second year medical students, 69% females, mean age 20.5 | Self-report of lifestyle, family and academic conditions, and intrinsic motivation scale toward learning. | Regression analyses | Determinants: spending time with family, taking pleasure in school and learning, understanding lectures, and attending school regularly, were positively associated with intrinsic motivation. |
| Williams & Deci (1996, USA) [7] | Exploration of SDT in students'adoption of psychosocial values and an autonomy-supportive style in patient interviewing skills | Longitudinal-pan-el design | Study 1:91 second-year medical students | Data collection: two times over 24 weeks on study 1 and five times on study 2 (three within the course, after 6 months, and after 2 years) | Correlations and regression analyses | Determinants and outcomes: positive relations between autonomous motivation, psychosocial beliefs, and perceived competence at interviewing before starting the course; perceived autonomy supportiveness of instructors promoted autonomous motivation, perceived competence, psychosocial beliefs, and behaving more autonomy-supportive with simulated patients. Increased relative autonomy mediated relations between instructors'autonomy support and the enhancement of psychosocial values and perceived competence. |
| Study 2:56 second-year medical students and course instructors | Instruments: physician psychosocial belief scale, general causality orientations scale, learning climate guestionnaire, learning self-regulation guestionnaire, interviewing competence scale, instructors'psychosocial beliefs, and health-care climate guestionnaire | |||||
| Williams etal. (1994, USA) [25] | Compare effects of facilitating students'interest' versus'controlling students learning'during internal medicine clerkship | Cross-sectional correlational | 89 Fourth year medical students at two Universities | Modified learning climate guestionnaire, competence in internal medicine scale, interest in internal medicine scale, pressure, tension scale, internal medicine career choice, and prior likelihood for career choice | Correlations, and structured eguation modelling | Determinants and outcomes: an autonomy supportive learning climate predicted increased perceived competence and interest, which in turn predicted specialty choice. Conversely, a controlling learning climate did not predict perceived competence or interest. |
| Williams etal. (1997, USA) [24] | Examine relationships between a utonomy-support, perceived competence, interest, prior likelihood and choosing internal medicine or surgery as a career | Cross-sectional correlational | 210 Fourth year medical students at three Universities, 61% males, mean age 27.4 | Modified learning climate guestionnaire, competence in internal medicine and surgery scale, interest in internal medicine scale, internal medicine and surgery career choice, and prior likelihood for career choice | Correlations, multiple regression and structured eguation modelling | Determinants and outcomes: perceived autonomy support predicted students'choices of internal medicine or surgery, even after the effects of prior (and actual) likelihood had been removed. |
| Wouters etal. (2014, The Netherlands) [22] | Investigate type of motivation and differences between selected and non-selected applicants of medical school. | Phenomenology | 96 Applicants, 72% females, mean age 23 | Document review of motivation statements | Thematic and content analysis, and fre-guencyand group comparison | Determinants: selected and non-selected applicants did not differ in types of motivation, reporting mainly autonomous motivation for applying. Findings raise guestions on the validity and reliability of the statement on motivation as a tool for selection. |
All studies collected self-reported demographics and conducted descriptive analyses.
The unit of analysis was focused on the identification and establishment of relations between determinants, mediators, and educational outcomes of motivation based on SDT. The thematic analysis was organised in three phases. The first phase was an open coding stage based on constant comparison and mainly aimed at reducing the data, extracting the essential ideas and resulting in the grouping of segments into different categories, i.e., determinants, mediators, and outcomes. The second phase was a central coding stage, aimed at combining and relating different categories amongst each other and grouping them into themes and subthemes. Finally, the third phase was an interpretative stage aimed at drawing conclusions and reflecting on the findings.
Results
Electronic and additional sources identified 2,966 references. When duplicates and irrelevant titles were removed, 385 papers were forwarded for abstract screening and later full-text assessment. Of these, 17 met the eligibility criteria. Subsequently, 570 titles were screened in the ancestry search, from which no new articles were included. Finally, all 17 papers were rated as of good quality evidence and were included in the review. Fig. 2 presents a flow chart summarising the review process.
All selected studies stated clear objectives and were found to be relevant for the study of self-determined motivation in health professions education. Table 3 provides a summary of the key findings. Reports came from different locations, such as North and South America, Australia, Europe, and Asia, thus providing evidence of the topic’s relevance for different health professions education settings. In terms of the specific subjects, the majority of the research has been dedicated to explore motivation in medical education (n=12, 71%), and to a lesser extent in psychology (n=3, 18%), and dental education (n=2, 11%) (Table 3).
Determinants, mediators, and outcomes of self-determined motivation
Fig. 3 shows a summary of the identified variables and their overall relationships with autonomous motivation. Determinants were divided into intrapersonal and interpersonal, and outcomes were divided into cognitive, affective, and behavioural.
Fig. 3.
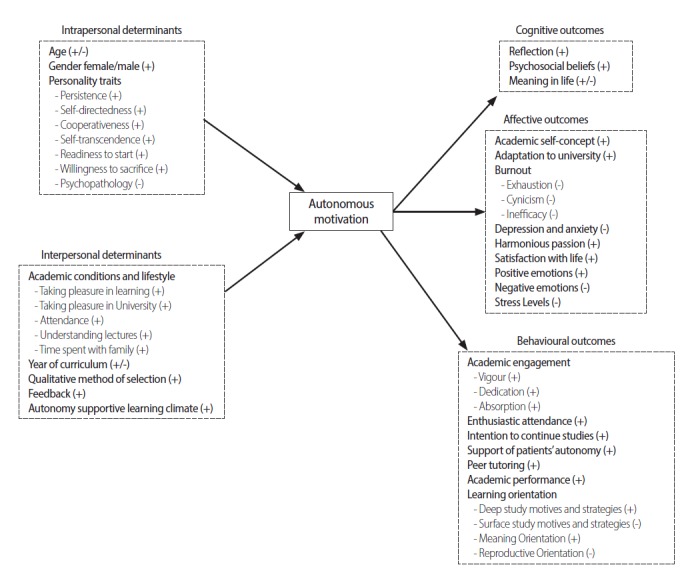
Summary of determinants and outcome variables and their relationship with autonomous motivation. (+), overall positive correlation; (-), overall negative correlation; (+/-), inconclusive correlation.
Intrapersonal determinants
Age: Inconclusive evidence was reported on the association between age and medical students’ motivation. While a study conducted with American medical students [7] reported that older students exhibited a more autonomous profile, endorsing less impersonal reasons, studies with Japanese and Dutch medical students [13,14] have reported non-significant associations in regression analyses.
Gender: Women have shown a more self-determined profile than men. Five studies [7,14, 15, 16,17] found that gender was significantly associated with autonomous motivation of medical students, and that women and men reported, respectively, higher autonomous motivation and higher controlled motivation. Two studies reported inconclusive findings. Nevertheless, they were limited by their motivation instrument, aimed at secondary school students [13], and by the small effect sizes reported by dental students [18].
Personality traits: Three studies analysed the relationship between personality traits and self-determined motivation. Psychopathological levels of personality (i.e., mental illness) were negatively associated with self-determined motivation in Korean medical students [19], while persistence, self-directedness, cooperativeness, self-transcendence, readiness to start/enter medical school, and willingness of a student to sacrifice for his/her medical study were positively associated with Dutch and Japanese medical students’ autonomous forms of motivation and showed contrary findings for controlled motivation and amotivation [13,20].
Interpersonal determinants
Academic conditions and lifestyle: One study found significant associations between intrinsic motivation and Japanese students’ taking pleasure in learning and in university, attending university and being able to understand lectures. Additionally, in the same study, time spent with family (≥1 hour per day) was found to be a positive predictor of intrinsic motivation [21].
Year of curriculum: Students’ progression throughout the curriculum showed inconclusive associations with motivation. For instance, Chilean dental students’ autonomous and controlled forms of regulation and amotivation showed significant differences per year of study [18]; however, amotivation showed an increasing pattern, with the highest scores corresponding to the fourth year i.e., when students start their clinical and patient-based learning, and decreased from that point until the end of the sixth year. The reverse pattern was reported for intrinsic motivation. Additionally, a study on Dutch medical students reported year of curriculum as a non-significant predictor of autonomous motivation [17].
Qualitative method of selection: Qualitative vs. weighted lottery system of medical students was found to affected relative autonomous motivation [17]. Indeed, students that underwent a qualitative method of selection showed higher autonomous motivation as well as lower amotivation scores than weighted lottery selected students. When integrated into a model, qualitative selected students’ autonomous motivation showed a positive indirect effect on grade point average through good study strategies (β=0.32, P<0.01), which was stronger than the effect reported for weighted lottery selected students (β=0.18, P<0.01). When applying to medical school, both selected and non-selected students’ statement for application showed strong autonomous reasons, therefore its validity and reliability was questioned, as it tends to emphasize socially desirable answers highlighting autonomous reasons and underreporting controlled motivation [22].
Feedback: Dental teachers reported the relevance of providing timely and constructive feedback as a way of supporting students’ intrinsic motivation and encouraging their perception of competence in one-on-one clinical teaching situations [23]. In their experience, feedback had to be given as a dialogue, highlighting the good things and what should be improved, and focusing on the task rather than on the person.
Autonomy supportive learning climate: Four studies informed about the significance of an autonomy supportive learning climate to support students’ autonomous motivation. The autonomy supportiveness of teachers predicted American medical students’ higher autonomous self-regulation towards a 24-week patient-interview course and over a two and one-half-year period [7]. Likewise, but in a different setting, learning in an autonomy supportive climate for a specific subject predicted students’ autonomous motivation to follow a surgery or an internal medicine residency path, even after the effects of prior and actual likelihood for that specialty were removed [24,25]. Dental faculty defined an autonomy supportive climate as a teaching style that supports the transfer of responsibility, refocuses uninteresting activities, identifies and encourages personal interests, and supports proactivity and choice [23].
Mediators
No studies were found to test the mediation effect of students’ perception of the basic psychological needs between determinants and motivation.
Cognitive outcomes
Reflection: As Brazilian medical students’ motivation became more self-determined, the correlation with reflection in learning became stronger [15]. Therefore, as students’ self-determined motivation increased, so did their metacognitive expertise.
Psychosocial beliefs: The biopsychosocial approach to medicine highlights the importance of practitioners being empathic, patient-centred, and sensitive to patients’ psychological and social needs to provide high-quality care. In a 24-week patient-interviewing course, students who mostly engaged out of an autonomous orientation showed stronger psychosocial beliefs at the end of the course (r=0.25) than students who engaged mostly out of controlled orientation (r=-0.14) or expressing an impersonal orientation (r=-0.27). Furthermore, when controlling for gender, an autonomous orientation and an impersonal orientation were found to be significant positive and negative predictors of psychosocial beliefs [7].
Meaning in life: Australian psychology students reported, with the exception of amotivation, all positive and similar associations between autonomous and controlled forms of motivation and presence of meaning in life [26]. In the same study, with the exception of intrinsic motivation to know, all autonomous and controlled motivation variables and amotivation showed positive and significant correlations with search for meaning in life. These results do not follow the theoretical continuum of SDT, and one reason might be due to the association of a contextual variable (academic motivation) with a general variable (meaning in life, as not being meaning in academic life).
Affective outcomes
Academic self-concept: A pattern consistent with SDT was found for dental students’ motivation and academic self-concept [18]. Identified regulation and the three intrinsic motivation subtypes showed the strongest positive and significant correlations (from r=0.18 to 0.24), introjected regulation showed a weaker but still positive and significant association (r=0.10), external regulation score was very weak and non-significant (r=0.05), while amotivation showed a negative and significant correlation (r=-0.15,)
Adaptation to University: Amongst Australian psychology students, intrinsic motivation to know and to experience stimulation were positive and significantly associated with measures of adaptation to university such as academic adjustment and institutional attachment, whereas introjected regulation showed a negative significant correlation with personal adjustment, as well as amotivation that showed a negative significant association with social adjustment and with all the aforementioned variables [26]. Furthermore, similar results were reported for British psychology students’ suggesting that, as students’ self-determination decreases, so does their adaptation to university [27].
Burnout: British psychology students’ autonomous and controlled motivation showed, respectively, significant negative and positive associations with exhaustion, cynicism and inefficacy, which characterise the burnout syndrome [28]. These results were mirrored by Dutch medical students’ reports on autonomous/controlled motivation and exhaustion [16].
Depression and anxiety: Amotivation showed a positive and significant correlation with Australian psychology students’ depression (r=0.44) and anxiety levels (r=0.36) [26]. All other motivation types were non-significant, with the exception of introjected regulation, which showed a positive correlation with anxiety (r=0.16). This is of special interest, as students endorsing this type of controlled motivation depend on success and achievements to alleviate internal pressure and avoid feelings of guilt, shame, and self-derogation, explaining the significant levels of anxiety in order to maintain their self-esteem, ego, and sense of pride. In line with these findings, Korean medical students’ self-determined motivation was found to predict lower levels of depression [19].
Harmonious passion: Autonomous motivation of psychology students had a positive and significant correlation with harmonious academic passion (r=0.44), which corresponds when individuals incorporate an activity freely into their self-identity, without incorporating any behavioural contingencies or rewards [28].
Satisfaction with life: Intrinsic motivation to know and amotivation showed significant positive and negative associations respectively with psychology students’ satisfaction with life [26].
Positive and negative emotions: Self-determined motivation has also been associated with positive and negative emotions experienced in university. Increasingly stronger positive correlations from controlled to autonomous forms of motivation and negative correlations of amotivation with positive emotions have been reported by dental students [18]. Similar results were reported for psychology students, who additionally showed a positive association between amotivation and both negative emotions [26] and psychological distress [27].
Stress: Perceived levels of stress towards university were studied to assess the amount of stress students experience during medical school, focusing on areas such as the school curriculum, the educational environment, and personal competence/endurance amongst others. Korean medical and British psychology students’ stress levels towards university showed positive correlations with amotivation, which then turned increasingly negative when correlated with controlled and autonomous motivation [19,27].
Behavioural outcomes
Academic engagement: Psychology students’ vigour, dedication, and absorption, all of which are indicators of academic engagement, showed positive and negative associations with autonomous and controlled motivation, respectively [28].
Enthusiastic attendance to class: When attending a 20-week course on patient interviewing skills, second year medical students endorsing autonomous reasons for studying showed a significant positive correlation with enthusiastic attendance, both on the first and second 10-week block [7].
Intention to continue studies: Self-determined motivation has also been associated with intentions to continue studying medicine, showing a positive and negative correlation with autonomous motivation and amotivation, respectively [15]. The latter was also supported by the fact that the only 3 students who dropped out of the medical programme, while the study took place, showed a high amotivation profile.
Support of patients’ autonomy: Medical students’ autonomous orientation at the end of a patient-interviewing course was positively correlated, six months later, with the autonomy-supportiveness towards standardized patients on cardiovascular risk and smoking cessation counselling [7].
Peer tutoring: Motivational patterns of medical students’ choices of cross-year peer tutoring activity showed autonomous motivation as having a significant positive correlation with number of courses tutored within a four-semester timeframe [15].
Academic performance: For Australian psychology students [26], and for Dutch [16,17], Korean [19], and Brazilian [15] medical students, autonomous motivation was positive and significantly associated with high performance, and as motivation became more controlled, the correlation became weaker and non-significant, which in turn became negative and significant when associated with amotivation. On the other hand, two studies reported inconsistent findings in psychology and dental students [18,27], however authors recommended cautious interpretation of their findings, as these came from cumulative instead of concurrent grade point average.
Learning orientation: Students’ reasons for studying showed significant correlations to the way students approached their learning process. Four studies reported [15, 16, 17, 18] that when medical and dental students’ autonomous forms of motivation increased, so did their deep study strategies and meaning orientation to learning. On the other hand, as controlled forms of motivation increased, deep study strategies decreased and surface study strategies and reproductive orientations to learning increased. This suggests that stronger autonomous motivation goes together with enhanced self-regulation of learning.
Discussion
The study of motivation in health professions education from the SDT perspective has been investigated in different cultural educational settings, however, the health-profession-context in which it has been explored is quite narrow, being mostly dedicated to medical education with few exceptions in psychology and dental education. The latter represents an important challenge for health education researchers, mainly because of the differences between health professions’ education and general education, and amongst the diverse health professions. These being different in several aspects, such as in the intensity of study, the timing and responsibility of patient contact, the requirement to carry out clinical work along with study, and the needs to follow a highly specifically defined path to being able to qualify to practice as a health professional. Indeed, several authors have highlighted the needs to continue expanding this research to other health areas [23,26], and similarly in medicine, authors have claimed that literature exists on students’ motivation to enter medical school yet very little is known about what happens afterwards [15,20].
SDT argues that its principles are independent of the individuals’ origin [2]. This is consistent with the findings from the reviewed articles, in which studies coming from different locations showed similar results. Future investigations should continue expanding cultural aspects such as gender and ethnic differences, as they provide important evidence about the external validity of SDT.
Studying students’ types of motivation should be an important feature for teachers, administrators, and curriculum developers when aiding to identify different determinants that impact students’ self-determination, which in turn may impact on educational outcomes and wellbeing [1]. The findings reported indicate that motivation is predicted by both the educational environment and students’ personal characteristics (Fig. 3). Of these, some can be manipulated and some cannot, implying that motivation can vary depending on its predictors [8].
Regardless of being unlikely to be manipulated, intrapersonal characteristics play an important role in students’ self-determination. Concerning gender, for instance, women appear to have a more autonomous profile than men, which is in line with research on SDT coming from other domains [29]. Indeed, in medical education women have been clustered into an interest-motivated group (i.e., higher autonomous motivation), whereas men have been clustered into a status-motivated profile (i.e., higher controlled motivation) [16]. Therefore, intrapersonal determinants should not be overlooked, as they might provide teachers with different insights on how to mentor or give advice to students [14].
On the other hand, interpersonal determinants were mostly related to the educational environment and represent a group of variables in which great attention should be paid, as they represent the ‘day-by-day’ influences over motivation in which educators may intervene. The learning climate, this being controlling or autonomy supportive, is suggested to influence students’ reasons for engaging in academic activities [1]. The relevance of creating an autonomy supportive learning climate in clinical education has been recently stressed by several authors [1,3,30], in which encouraging self-initiation, volitional activities, the use of constructive feedback, and providing rationale is pointed as crucial. The impact of learning in such environment has been suggested as beneficial for both students and patients, as students engaging in activities based on autonomous reasons are more likely to interact and support their patients’ autonomy towards their healthcare [7]. Moreover, the emerging development of curricula based on entrusted professional activities [31], has common grounds with SDT by highlighting the importance of developing students’ autonomy and competence over time. Since several academic conditions were related to students’ self-determination, these variables may well be used for developing interventions for lowering the incidence of and/or increasing the recovery from low self-determined forms of motivation and prevent future academic failure [6,21]
Despite the inconclusive findings with regards to year of curriculum and motivation, it is interesting to note that motivation fluctuates along the curriculum. This was shown for dental students, in which amotivation reached the highest score in the fourth year (when transitioning from pre-clinical to clinical courses) and then decreasing towards the final sixth year, with the opposite pattern being shown for intrinsic motivation. As such, it seems possible that this is due to the experience students have when transitioning through different learning cycles (i.e., basic sciences and preclinical and clinical activities). It has been suggested that an early patient contact and vertical integration might increase students autonomous motivation and decrease the amotivation when experiencing an abrupt transition [1,18]. However, further research needs to be undertaken before the association between clinical transition and motivation is more clearly understood.
One unanticipated finding was that no study tested the mediating role of students’ basic psychological needs satisfaction between interpersonal determinants and motivation. This mediating effect has been tested with success in other domains [32]. So far, there is useful evidence on how motivation is directly influenced by different determinants; nevertheless there is no evidence showing the effect of mediating variables. As to what impacts motivation is how students perceive these determinants to affect their basic psychological needs and not their original intended effect [2], many questions are still unanswered leaving abundant room for further research.
When students were experiencing autonomous reasons to attend university and for engaging in academic activities, positive cognitive, affective, and behavioural outcomes were reported. As to how students processed information, cognitive outcomes such as reflection were higher as motivation became more autonomous. Reflection in- and on-action has been related to an increased lifelong learning experience [33] and as students become more autonomous, so might their future self-regulation of learning. Additionally, in recent years there has been an increased emphasis on the technical-biological and pharmacological aspects of healthcare, which is believed to carry a dehumanisation of patient care [7]. Instead, as students’ self-determination increased, so did their psychosocial beliefs towards a more humanistic approach to medical care.
The findings regarding students’ affective outcomes are consistent with data obtained in research with primary and secondary school students and in other areas of higher education, in which autonomous motivation has been related to better psychological adjustment [34]. Moreover, these findings are also in line with those of James et al. [35] who suggested that amotivation is associated with an increased risk of students discontinuing university.
In terms of students’ actions, as motivation orientations became more self-determined, behavioural outcomes became more positive. These findings seem to be consistent with research in other domains of higher education, where autonomous motivation has been related to sustained student involvement and with higher academic performance [36], and where controlled motivation/amotivation was shown to correlate with cheating [37] and plagiarism [38].
In general, students reported a mix of autonomous and controlled reasons for studying, thus supporting the idea that internal and external sources of motivation play an important role in the context of demanding undergraduate programmes. Nevertheless, internal and external reasons are associated with positive and negative outcomes respectively. Therefore, efforts should point at encouraging students to engage in activities out of interest and enjoyment. It is unrealistic, however, to think that students will participate out of intrinsic motivation all the time. This highlights the relevance of fostering the internalisation process of motivation, from external to internal reasons, in which students need clear rationale and autonomy-support to bridge the importance that learning activities will have for their professional practice and to engage from autonomous forms of motivation.
This review has applied robust methods and has led to relevant findings; nevertheless, there are a series of limitations that should be taken into account. First, we limited our analysis to English-, Spanish-, and French-language articles, which might have excluded relevant literature from other languages. Second, we searched the literature through multiple sources, however the review is inherently limited to these and some relevant publications might have been excluded. Third, the findings reported might be somewhat limited by the number of small-sized but still meaningful correlations and should be interpreted within the context of each study. Finally, the downside of bringing together research conducted in different health-related disciplines is that it involves a variety of educational contexts, study designs, and participants, where results found in one context might not be generalised to others. Nonetheless, details have been provided of the methods and results of the included studies, so that readers can judge the transferability of findings to different health professions education settings.
In conclusion, this study has found that generally, motivation could be enhanced by changes in the educational environment and by an early detection of students’ characteristics. Doing so, may support future health practitioners’ self-determined forms of motivation and positively influence how they process information and their emotions and how they approach their learning activities, which may ultimately contribute to the fundamental purpose of health professions education: the improvement of healthcare practice, patient care, and patients outcomes.
Footnotes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Supplementary material
Audio recording of the abstract.
References
- 1.Ten Cate TJ, Kusurkar RA, Williams GC. How self-determination theory can assist our understanding of the teaching and learning processes in medical education. AMEE guide No. 59. Med Teach. 2011;33:961–973. doi: 10.3109/0142159X.2011.595435. http://dx.doi.org/10.3109/0142159X.2011.595435. [DOI] [PubMed] [Google Scholar]
- 2.Deci EL, Ryan RM. Self-determination theory: a macrotheory of human motivation, development, and health. Can Psychol. 2008;49:182–185. http://dx.org/10.1037/a0012801. [Google Scholar]
- 3.Orsini C, Evans P, Jerez O. How to encourage intrinsic motivation in the clinical teaching environment?: a systematic review from the self-determination theory. J Educ Eval Health Prof. 2015;12:8. doi: 10.3352/jeehp.2015.12.8. http://dx.org/10.3352/jeehp.2015.12.8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ryan RM, Deci EL. Intrinsic and extrinsic motivations: classic definitions and new directions. Contemp Educ Psychol. 2000;25:54–67. doi: 10.1006/ceps.1999.1020. http://dx.org/10.1006/ceps.1999.1020. [DOI] [PubMed] [Google Scholar]
- 5.Deci EL, Ryan RM. Facilitating optimal motivation and psychological well-being across life’s domains. Can Psychol. 2008;49:14–23. http://dx.org/10.1037/0708-5591.49.1.14. [Google Scholar]
- 6.Hulsman RL, Oort FJ, Michels RP, Casteelen G, Griffioen FM. Effectiveness of selection in medical school admissions: evaluation of the outcomes among freshmen. Med Educ. 2007;41:369–377. doi: 10.1111/j.1365-2929.2007.02708.x. http://dx.org/10.1111/j.1365-2929.2007.02708.x. [DOI] [PubMed] [Google Scholar]
- 7.Williams GC, Deci EL. Internalization of biopsychosocial values by medical students: a test of self-determination theory. J Pers Soc Psychol. 1996;70:767–779. doi: 10.1037//0022-3514.70.4.767. http://dx.org/10.1037/0022-3514.70.4.767. [DOI] [PubMed] [Google Scholar]
- 8.Kusurkar RA, Ten Cate TJ, van Asperen M, Croiset G. Motivation as an independent and a dependent variable in medical education: a review of the literature. Med Teach. 2011;33:e242–e262. doi: 10.3109/0142159X.2011.558539. http://dx.org/10.3109/0142159X.2011.558539. [DOI] [PubMed] [Google Scholar]
- 9.Gordon M, Gibbs T. STORIES statement: publication standards for healthcare education evidence synthesis. BMC Med. 2014;12:143. doi: 10.1186/s12916-014-0143-0. http://dx.org/10.1186/s12916-014-0143-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Moher D, Liberati A, Tetzlaff J. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:19. doi: 10.1371/journal.pmed.1000097. http://dx.org/10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Harden RM, Grant J, Buckley G, Hart IR. BEME guide no. 1: best evidence medical education. Med Teach. 1999;21:553–562. doi: 10.1080/01421599978960. http://dx.doi.org/10.1080/01421599978960. [DOI] [PubMed] [Google Scholar]
- 12.Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8:45. doi: 10.1186/1471-2288-8-45. http://dx.org/10.1186/1471-2288-8-45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Tanaka M, Mizuno K, Fukuda S, Tajima S, Watanabe Y. Personality traits associated with intrinsic academic motivation in medical students. Med Educ. 2009;43:384–387. doi: 10.1111/j.1365-2923.2008.03279.x. http://dx.org/10.1111/j.1365-2923.2008.03279.x. [DOI] [PubMed] [Google Scholar]
- 14.Kusurkar R, Croiset G, ten Cate O. Implications of gender differences in motivation among medical students. Med Teach. 2013;35:173–174. doi: 10.3109/0142159X.2012.737056. http://dx.org/10.3109/0142159X.2012.737056. [DOI] [PubMed] [Google Scholar]
- 15.Sobral DT. What kind of motivation drives medical students’ learning quests? Med Educ. 2004;38:950–957. doi: 10.1111/j.1365-2929.2004.01913.x. http://dx.doi.org/10.1111/j.1365-2929.2004.01913.x. [DOI] [PubMed] [Google Scholar]
- 16.Kusurkar RA, Croiset G, Galindo-Garre F, Ten Cate O. Motivational profiles of medical students: association with study effort, academic performance and exhaustion. BMC Med Educ. 2013;13:87. doi: 10.1186/1472-6920-13-87. http://dx.org/10.1186/1472-6920-13-87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kusurkar RA, Ten Cate TJ, Vos CM, Westers P, Croiset G. How motivation affects academic performance: a structural equation modelling analysis. Adv Health Sci Educ Theory Pract. 2013;18:57–69. doi: 10.1007/s10459-012-9354-3. http://dx.org/10.1007/s10459-012-9354-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Orsini C, Binnie V, Evans P, Ledezma P, Fuentes F, Villegas MJ. Psychometric validation of the academic motivation scale in a dental student sample. J Dent Educ. 2015;79:971–981. [PubMed] [Google Scholar]
- 19.Park J, Chung S, An H, Park S, Lee C, Kim SY, Lee JD, Kim KS. A structural model of stress, motivation, and academic performance in medical students. Psychiatry Investig. 2012;9:143–149. doi: 10.4306/pi.2012.9.2.143. http://dx.org/10.4306/pi.2012.9.2.143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kusurkar R, Croiset G, Kruitwagen C, ten Cate O. Validity evidence for the measurement of the strength of motivation for medical school. Adv Health Sci Educ Theory Pract. 2011;16:183–195. doi: 10.1007/s10459-010-9253-4. http://dx.org/10.1007/s10459-010-9253-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Tanaka M, Watanabea Y. Academic and family conditions associated with intrinsic academic motivation in Japanese medical students: a pilot study. Health Educ J. 2011;71:358–364. http://dx.org/10.1177/0017896911401004. [Google Scholar]
- 22.Wouters A, Bakker AH, van Wijk IJ, Croiset G, Kusurkar RA. A qualitative analysis of statements on motivation of applicants for medical school. BMC Med Educ. 2014;14:200. doi: 10.1186/1472-6920-14-200. http://dx.org/10.1186/1472-6920-14-200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Orsini C, Evans P, Binnie V, Ledezma P, Fuentes F. Encouraging intrinsic motivation in the clinical setting: teachers’ perspectives from the self-determination theory. Eur J Dent Educ. 2016;20:102–111. doi: 10.1111/eje.12147. http://dx.org/10.1111/eje.12147. [DOI] [PubMed] [Google Scholar]
- 24.Williams GC, Saizow R, Ross L, Deci EL. Motivation underlying career choice for internal medicine and surgery. Soc Sci Med. 1997;45:1705–1713. doi: 10.1016/s0277-9536(97)00103-2. http://dx.org/10.1016/S0277-9536(97)00103-2. [DOI] [PubMed] [Google Scholar]
- 25.Williams GC, Wiener MW, Markakis KM, Reeve J, Deci EL. Medical students’ motivation for internal medicine. J Gen Intern Med. 1994;9:327–333. doi: 10.1007/BF02599180. http://dx.org/10.1007/BF02599180. [DOI] [PubMed] [Google Scholar]
- 26.Bailey TH, Phillips LJ. The influence of motivation and adaptation on students’ subjective well-being, meaning in life and academic performance. High Educ Res Dev. 2016;35:201–216. http://dx.org/10.1080/07294360.2015.1087474. [Google Scholar]
- 27.Baker SR. Intrinsic, extrinsic, and amotivational orientations: their role in university adjustment, stress, well-being, and subsequent academic performance. Curr Psychol. 2004;23:189–202. http://dx.org/10.1007/s12144-004-1019-9. [Google Scholar]
- 28.Stoeber J, Childs JH, Hayward JA, Feast AR. Passion and motivation for studying: predicting academic engagement and burnout in university students. Educ Psychol. 2011;31:513–528. http://dx.org/10.1080/01443410.2011.570251. [Google Scholar]
- 29.Vansteenkiste M, Sierens E, Soenens B, Luyckx K, Lens W. Motivational profiles from a self-determination perspective: the quality of motivation matters. J Educ Psychol. 2009;101:671–688. http://dx.org/10.1037/a0015083. [Google Scholar]
- 30.Kusurkar RA, Croiset G, Ten Cate TJ. Twelve tips to stimulate intrinsic motivation in students through autonomy-supportive classroom teaching derived from self-determination theory. Med Teach. 2011;33:978–982. doi: 10.3109/0142159X.2011.599896. http://dx.org/10.3109/0142159X.2011.599896. [DOI] [PubMed] [Google Scholar]
- 31.Ten Cate O, Chen HC, Hoff RG, Peters H, Bok H. Curriculum development for the workplace using entrustable professional activities (EPAs): AMEE guide no. 99. Med Teach. 2015;37:983–1002. doi: 10.3109/0142159X.2015.1060308. http://dx.doi.org/10.3109/0142159X.2015.1060308. [DOI] [PubMed] [Google Scholar]
- 32.Chen B, Vansteenkiste M, Beyers W, Boone L, Deci EL, Duriez B, Lens W, Matos L, Mouratidis A. Basic psychological need satisfaction, need frustration, and need strength across four cultures. Motiv Emot. 2014;39:216–236. http://dx.org/10.1007/s11031-014-9450-1. [Google Scholar]
- 33.Kaufman DM, Mann KV. Teaching and learning in medical education: how theory can inform practice. In: Swanwick T, editor. Understanding medical education: evidence, theory and practice. Oxford: John Wiley & Sons; 2010. pp. 16–36. http://dx.doi.org/10.1002/9781118472361.ch2. [Google Scholar]
- 34.Deci EL, Ryan RM, Williams GC. Need satisfaction and the self-regulation of learning. Learn Individ Differ. 1996;8:165–183. http://dx.org/10.1016/S1041-6080(96)90013-8. [Google Scholar]
- 35.James R, Krause KD, Jennings C, Centre for the Study of Higher Education, University of Melbourne . The first-year experience in Australian universities: findings from 1994 to 2009. Melbourne: Centre for the Study of Higher Education, University of Melbourne; 2010. [Google Scholar]
- 36.Vansteenkiste M, Zhou M, Lens W, Soenens B. Experiences of autonomy and control among chinese learners: vitalizing or immobilizing? J Educ Psychol. 2005;97:468–483. http://dx.doi.org/10.1037/0022-0663.97.3.468. [Google Scholar]
- 37.Davy JA, Kincaid JF, Smith KJ, Trawick MA. An examination of the role of attitudinal characteristics and motivation on the cheating behavior of business students. Ethics Behav. 2007;17:281–302. http://dx.org/10.1080/10508420701519304. [Google Scholar]
- 38.Angell LR. The relationship of impulsiveness, personal efficacy, and academic motivation to college cheating. Coll Stud J. 2006;40:118–131. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Audio recording of the abstract.