

Abstract
Objective
The aim of this study was to investigate whether the level of serum microRNA-199a/b-3p (miR-199a/b-3p) can serve as a predictor of treatment response to transarterial chemoembolization (TACE) in patients with hepatocellular carcinoma (HCC).
Methods
Serum miR-199a/b-3p expression level was measured in 132 patients with HCC before TACE (t1) and 3–5 days after TACE (t2). Additionally, 126 patients of these 132 patients had levels measured 4 weeks after TACE (t3) and 3–5 days after second TACE (t4). Serum miR-199a/b-3p expression levels were compared with those of 50 healthy controls. Correlations between miR-199a/b-3p expression levels and clinicopathologic factors and tumor responsiveness were analyzed. The modified Response Evaluation Criteria in Solid Tumors assessment was conducted at t3.
Results
A lower mean baseline miR-199a/b-3p expression level was observed in patients with HCC compared with healthy controls (0.68±0.81 vs 2.50±2.16, P<0.001). A negative correlation between baseline miR-199a/b-3p expression levels and tumor size (P<0.001) was observed. The nonresponder group had significantly lower miR-199a/b-3p expression levels than the responder group at t1 (0.77±1.09 vs 1.96±1.32, P<0.001). In addition, the decrease in miR-199a/b-3p at t2 was greater in the responder group than in the nonresponder group (P=0.011). A higher proportion of the responder group achieved a >25% decrease in serum miR-199a/b-3p expression levels compared with the nonresponder group (64% vs 39%).
Conclusion
Serum miR-199a/b-3p may represent a novel biomarker for predicting efficacy of TACE in patients with HCC.
Keywords: biomarker, hepatocellular carcinoma, microRNA, microRNA-199a/b-3p, transarterial chemoembolization
Introduction
An estimated 782,500 new liver cancer cases and 745,500 cancer deaths occurred worldwide during the year 2012. Half of these cases and deaths were estimated to occur in the People’s Republic of China.1 Hepatocellular carcinoma (HCC), the most common primary liver cancer, is the fifth most frequent cancer and the third cause of cancer-related mortality worldwide.2 Most patients with HCC are diagnosed at the intermediate to advanced stages, so that only 30% of patients with HCC are eligible to receive surgery. When surgical options are precluded, transarterial chemoembolization (TACE) is one of the options that can be used to treat locally advanced tumors in the liver. In this procedure, an intraarterial injection of anticancer compounds (usually lipiodol, doxorubicin, and/or cisplatin) is administered immediately prior to embolization.3 Assessment of response within the first 4 weeks after commencement of TACE treatment is vital for making therapeutic decisions and adjustments.4 However, clinical outcomes vary significantly and are difficult to predict. There are few studies on the identification of biomarkers for the prediction of outcomes for patients with HCC and their prognosis after TACE treatment.
MicroRNAs (miRs) are a class of small, endogenous, phylogenetically conserved RNAs, which are responsible for the posttranscriptional regulation of mRNA translation and mRNA stability.5,6 During the regulation process, miRs can pair to complementary binding sites within the 3′-untranslated region of any of hundreds of target mRNAs, and as a result, they participate in nearly all biological processes.7 Previous studies have reported important roles for miRs during HCC development and progression. Most previous studies on miR expression have been performed on tissue samples. However, recent findings have demonstrated that human serum and plasma contain a large number of stable miRs, and that the expression profile of these miRs holds great promise as a novel noninvasive biomarker, because tumor-derived miRs can be present and can exist stably in blood.8,9
Hou et al10 found that the third most strongly expressed miR-199a/b-3p (miR-199a-3p/miR-199b-3p) was consistently decreased in HCC tissue, and its decrement significantly correlated with poor survival of patients with HCC. Moreover, miR-199a/b-3p could target the tumor-promoting protein kinase PAK4 to suppress HCC growth through inhibiting the PAK4/Raf/MEK/ERK pathway, both in vitro and in vivo. Moreover, microarray analysis showed that miR-199a/b-3p was downregulated in HCC tissue compared with normal controls’ tissue,11 and other studies have indicated that miR-199 can act as a tumor suppressor by regulating various pathways.12–14 The mature sequence of miR-199a-3p is the same as that of miR-199b-3p.15
In this study, we aimed to compare the expression levels of serum miR-199a/b-3p between patient with HCC and healthy controls, between patients before and after TACE treatment, and between patients with different stages of HCC. We attempted to find out whether serum miR-199a/b-3p expression levels could be used to predict the treatment response of patients with HCC receiving TACE treatment and, therefore, act as a biomarker for early and accurate identification of patients with a high risk of treatment failure. For such high-risk patients, modified therapy or adjuvant therapy could potentially be applied to improve their survival.
Methods
Patients with HCC
In total, 132 patients with unresectable HCC who underwent TACE for the first time at the Nanfang Hospital, Southern Medical University, between March 2014 and October 2014, were enrolled into the current study. Criteria for patient selection were according to the HCC guidelines formulated by the Ministry of Health of the People’s Republic of China.16 Inclusion and exclusion criteria are presented in Figure 1. Serum levels of α-fetoprotein (AFP; ≥400 ng/mL) were elevated in 48%. Most patients had a Child–Pugh A classification (77%) and multiple liver tumor lesions (66%). According to the Barcelona Clinic Liver Cancer (BCLC) staging system, 36 patients (27%) had stage A, 60 (45%) had stage B, and 36 (27%) had stage C tumors. None of the patients received chemotherapy/radiation or surgical therapy toward the tumor.
Figure 1.

Flowchart of inclusion and exclusion criteria.
Notes: All the BCLC early-stage patients with HCC preferred TACE treatment, refusing surgery or chemotherapy/radiation therapy.
Abbreviations: BCLC, Barcelona Clinic Liver Cancer; HCC, hepatocellular carcinoma; TACE, transarterial chemoembolization.
The study was approved by the Ethics Committee of Nanfang Hospital, and written informed consent was obtained from all study participants.
TACE treatment, follow-up, and assessment of treatment response
Selective angiography was performed to identify the major arterial supply to the HCC tumor. TACE was conducted using a mixture of adriamycin, lipiodol, and contrast agent. The dose of adriamycin and lipiodol was dependent on tumor size and vascularity, with 20–50 mg of adriamycin and 5–20 mL lipiodol used per session. Subsequently, embolization was performed using polyvinyl alcohol particles, and occlusion of target vessels and absence of additional tumor blood supply were confirmed.
All patients had follow-up evaluations 4 weeks after first TACE treatment, with routine monitoring by contrast-enhanced computed tomography, liver function tests, and measurement of serum AFP levels. Computed tomography was performed at baseline and 4 weeks after the first TACE treatment for the evaluation of tumor response, and repeat TACE was performed 4 weeks after the first TACE treatment. The modified Response Evaluation Criteria in Solid Tumors (mRECIST) was used to monitor patient response to TACE treatment.17 Tumor measurements were performed by two qualified radiologists. Complete response (CR) was defined as disappearance of any intratumoral arterial enhancement in all target lesions. Partial response (PR) was defined as at least a 30% decrease in the sum of the diameters of viable (enhancement in the arterial phase) target lesions, compared with the baseline sum of the diameters of these target lesions. The remaining patients were categorized as having stable disease (SD) or progressive disease (PD). Patients with CR and PR were defined as responders, and patients with SD or PD were defined as nonresponders.
Serum collection and detection of miR-199a/b-3p by quantitative real-time polymerase chain reaction
Serum samples were obtained from patients at four different time points: before TACE (t1), 3–5 days after TACE (t2), 4 weeks after first TACE (t3), and 3–5 days after second TACE (t4). Samples were centrifuged at 1,500× g for 10 minutes at 4°C within 2 hours after venous blood was collected, and serum supernatant was transferred to a new microcentrifuge tube and recentrifuged at 16,000× g for 10 minutes at 4°C. The serum supernatants were stored at −80°C until further processing.
Total RNA was extracted from 200 µL of serum using the miRNeasy Serum/Plasma Kit (Qiagen NV, Venlo, the Netherlands) following the manufacturer’s protocol. The yield of RNA was determined using a NanoDrop 2000 spectrophotometer (Thermo Fisher Scientific, Waltham, MA, USA). Quantification was performed with a two-step reaction process consisting of reverse transcription (RT) and polymerase chain reaction (PCR). Complementary DNA (cDNA) was synthesized from total RNA using miScript® RT Kit (Qiagen NV) and following the manufacturer’s protocol. Reactions were performed in a T100 Thermal Cycler (Bio-Rad Laboratories Inc., Hercules, CA, USA) for 60 minutes at 37°C, followed by heat inactivation of RT for 5 minutes at 95°C. The 10 µL RT reaction mixture was then diluted ×10 in nuclease-free water and held at −20°C. Quantitative real-time PCR was performed using miScript® SYBR PCR Kit (Qiagen NV) in a StrataGene Mx3005P (Agilent Technologies, Santa Clara, CA, USA) with 10 µL PCR reaction mixture consisting of 1 µL cDNA, 1 µL miR-specific primer, 1 µL universal primer (Qiagen NV), 2 µL nuclease-free water, and 5 µL QuantiTect SYBR Green PCR Master Mix. Reactions were incubated in a 96-well optical plate at 95°C for 15 minutes, followed by 40 cycles of 94°C for 15 seconds, 55°C for 30 seconds, and 70°C for 30 seconds. Each sample was run in triplicate for analysis. At the end of the PCR cycles, melting curve analysis was performed to validate the specific generation of the expected PCR product. miR-199a/b-3p primers were 5′-GTCACAGTAGTCTGCACAT-3′. The relative expression level (fold change) of miR-199a/b-3p was normalized to RNU6B (5′-ACGCAAATTCGTGAAGCGTT-3′) and calculated using the 2−ΔΔCt method (Livak and Schmittgen, 2001). ΔCtpatients/controls = CtmiR-199a/b-3p − CtU6 and ΔΔCt = ΔCtpatients − ΔCtcontrols. In addition, the relative change in serum miR-199a/b-3p from baseline (t1) to 3–5 days after first TACE treatment (t2) was defined as:
| (1) |
Statistical analysis
All data for continuous variables were expressed as mean ± standard deviation and analyzed using Student’s t-test. Categorical variables were presented as number and percentages. The χ2 test, Wilcoxon rank sum test, and Fisher’s exact tests were used, as appropriate, to test the association of miR-199a/b-3p with each of the clinicopathological parameters. The results were analyzed using GraphPad Prism software (GraphPad Software, Inc., La Jolla, CA, USA). All statistical tests were two sided, and P<0.05 was considered significant.
Results
Serum miR-199a/b-3p baseline expression level was decreased in patients with HCC
Baseline expression of serum miR-199a/b-3p in patients (including six patients who missed follow-up) with HCC before TACE (t1) was significantly lower than that of the healthy controls (0.68±0.81 vs 2.50±2.16, P<0.001; Figure 2).
Figure 2.
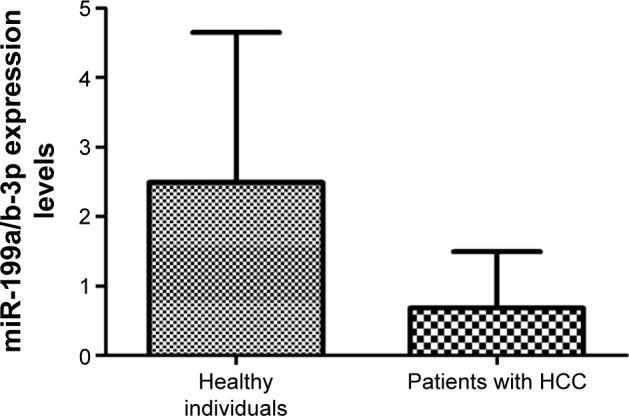
Baseline expression of serum miR-199a/b-3p in patients with HCC before first TACE (t1) was significantly lower compared with healthy controls (0.68±0.81 vs 2.50±2.16, P<0.001; N=132).
Abbreviations: HCC, hepatocellular carcinoma; miR-199a/b-3p, microRNA-199a/b-3p; TACE, transarterial chemoembolization.
The TACE nonresponder group had lower baseline serum miR-199a/b-3p than the responder group
Tumor response was evaluated according to the mRECIST at 4 weeks after TACE treatment. CR was observed in 15 patients, PR in 35, SD in 62, and PD in 14. Thus, 50 patients (CR + PR) were classified as the responder group and 76 (SD + PD) as the nonresponder group.
The nonresponder group had significantly lower miR-199a/b-3p expression levels than the responder group at t1 (0.77±1.09 vs 1.96±1.32, P<0.001; Figure 3).
Figure 3.
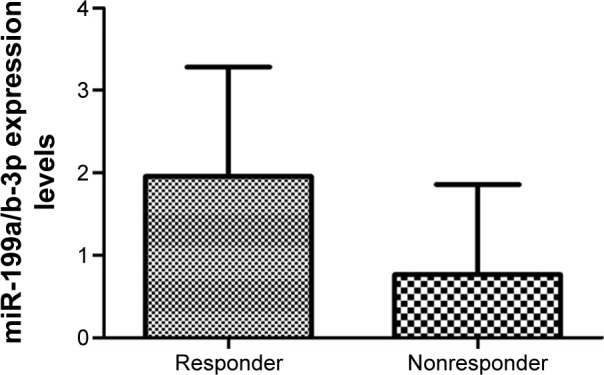
The nonresponder group had significantly lower miR-199a/b-3p expression levels than the responder group at t1 (0.77±1.09 vs 1.96±1.32, P<0.001; N=126).
Note: t1, before first TACE.
Abbreviations: miR-199a/b-3p, microRNA-199a/b-3p; TACE, transarterial chemoembolization.
miR-199a/b-3pt1-t2 expression change correlated with tumor responsiveness
The relationship between tumor responsiveness and changes in levels of serum miR-199a/b-3p at t1, t2, and t3 was analyzed. The decrease in miR-199a/b-3pt1-t2 was greater in responder group than in the nonresponder group (P=0.011; Table 1). A higher proportion of the responder group achieved a >25% decrease in serum miR-199a/b-3p levels compared with the nonresponder group (64% vs 39%). Serum miR-199a/b-3p decreased at t2 and t3 (Figure 4). There was no significant difference in the decrease in miR-199a/b-3pt1-t3 between the responder and the nonresponder groups (P=0.132).
Table 1.
Change in serum miR-199a/b-3p levels at t2 and association with tumor responsiveness
| Change in miR-199a/b-3p | Tumor response, n (%)
|
Total, n (%) | P-value | |
|---|---|---|---|---|
| Responder | Nonresponder | |||
| Decreased >25% | 32 (25) | 30 (24) | 62 (49) | – |
| Decreased ≤25% or increased | 18 (14) | 46 (37) | 64 (51) | – |
| Total | 50 | 76 | 126 | 0.011 |
Note: t2, 3–5 days after TACE.
Abbreviations: miR-199a/b-3p, microRNA-199a/b-3p; TACE, transarterial chemoembolization; –, not available.
Figure 4.
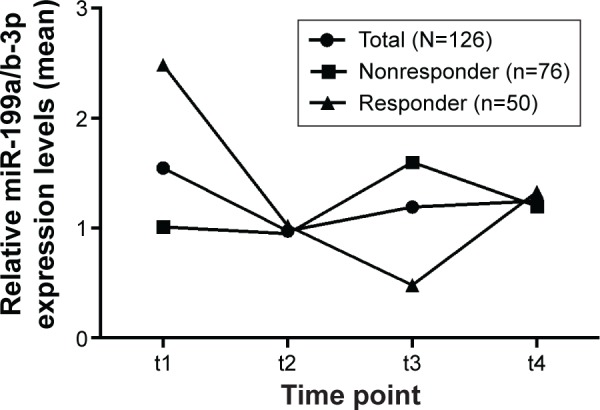
Relative miR-199a/b-3p expression levels at second TACE.
Notes: Relative serum miR-199a/b-3p expression levels were measured in the TACE responder group, the TACE nonresponder group, and the total patient group before TACE (t1), 4 days after TACE (t2), 4 weeks after first TACE (t3), and 4 days after second TACE (t4). The miR-199a/b-3p levels of patients in the responder group had a relatively sharp decrease at t2 and t3 compared with the nonresponder group.
Abbreviations: miR-199a/b-3p, microRNA-199a/b-3p; TACE, transarterial chemoembolization.
miR-199a/b-3p expression levels correlated with tumor size and BCLC stage
To understand whether there is a correlation between serum miR-199a/b-3p expression levels and clinicopathologic characteristics of patients with HCC, we divided the 132 patients into two groups: a lower expression group and a higher expression group. We found that lower levels of serum miR-199a/b-3p correlated with larger tumor size (P<0.001; Table 2). Expression levels of serum miR-199a/b-3p were significantly different between patients with HCC (staged as BCLC grades A, B, or C) and healthy controls (A vs B vs C vs healthy controls: 0.70±0.64 vs 1.07±1.42 vs 1.31±1.14 vs 2.50±2.16, P<0.001; Figure 5), but they were not significantly different with the χ2 test (Table 2). Expression levels did not correlate with hepatitis B surface antigen status, presence of vascular invasion or cirrhosis, Child–Pugh classification, or level of AFP (Table 3).
Table 2.
Correlations between clinicopathologic characteristics and miR-199a/b-3p serum levels in patients with HCC before TACE
| Variables | Lower expression group (n=66) | Higher expression group (n=66) | P-value |
|---|---|---|---|
| Sex (male/female) | 49/17 | 41/25 | 0.191 |
| Age (≥55 years/<55 years) | 38/28 | 49/17 | 0.066 |
| HBsAg (positive/negative) | 50/16 | 54/12 | 0.524 |
| Liver cirrhosis (presence/absence) | 52/14 | 49/17 | 0.682 |
| Child–Pugh classification (class A/class B) | 47/19 | 55/11 | 0.145 |
| Tumor size (≤5 cm/>5 cm) | 25/41 | 45/21 | <0.001 |
| AFP (≤400 ng/mL/>400 ng/mL) | 39/27 | 30/36 | 0.163 |
| Number of tumors (1/≥2) | 26/40 | 19/47 | 0.271 |
| Vascular invasion (presence/absence) | 15/51 | 24/42 | 0.126 |
| BCLC stage (A/B/C) | 19/34/13 | 17/26/23 | 0.138 |
Abbreviations: AFP, α-fetoprotein; BCLC, Barcelona Clinic Liver Cancer; HBsAg, hepatitis B surface antigen; HCC, hepatocellular carcinoma; miR-199a/b-3p, microRNA-199a/b-3p; TACE, transarterial chemoembolization.
Figure 5.
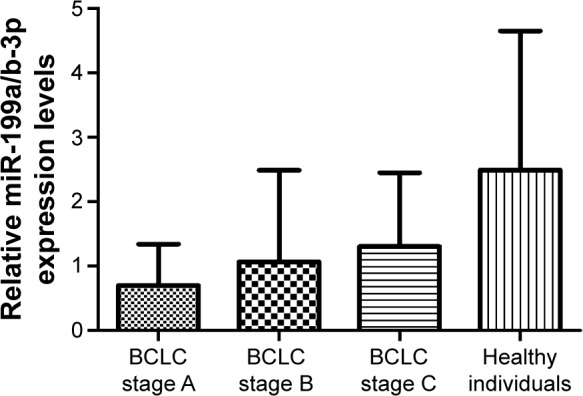
Expression levels of serum miR-199a/b-3p in patients with HCC staged as BCLC A, B, or C, and healthy individuals were significantly different (0.70±0.64 vs 1.07±1.42 vs 1.31±1.14 vs 2.50±2.16, P<0.001).
Notes: Higher serum miR-199a/b-3p expression level correlated with advanced BCLC stage. The results were analyzed with unpaired t-test.
Abbreviations: BCLC, Barcelona Clinic Liver Cancer; HCC, hepatocellular carcinoma; miR-199a/b-3p, microRNA-199a/b-3p.
Table 3.
Clinicopathologic factors associated with mRECIST responder and nonresponder groups
| Clinicopathologic factors | Overall | Responder (n=50) | Nonresponder (n=76) | P-value |
|---|---|---|---|---|
| Sex | ||||
| Male | 90 | 34 | 56 | 0.548 |
| Female | 36 | 16 | 20 | |
| Age (years) | ||||
| ≥55 | 87 | 39 | 48 | 0.115 |
| <55 | 39 | 11 | 28 | |
| HBsAg | ||||
| Positive | 100 | 38 | 62 | 0.503 |
| Negative | 26 | 12 | 14 | |
| Liver cirrhosis | ||||
| Presence | 98 | 35 | 63 | 0.125 |
| Absence | 28 | 15 | 13 | |
| Child–Pugh classification | ||||
| Class A | 97 | 35 | 62 | 0.533 |
| Class B | 29 | 15 | 14 | |
| Tumor size (cm) | ||||
| ≤5 | 67 | 41 | 18 | <0.001 |
| >5 | 59 | 9 | 58 | |
| AFP (ng/mL) | ||||
| ≤400 | 60 | 29 | 31 | 0.070 |
| >400 | 66 | 21 | 45 | |
| Number of tumors | ||||
| 1 | 43 | 13 | 30 | 0.129 |
| ≥2 | 83 | 37 | 46 | |
| Vascular invasion | ||||
| Presence | 37 | 10 | 27 | 0.073 |
| Absence | 89 | 40 | 49 | |
| BCLC stage | ||||
| A | 33 | 20 | 13 | 0.006 |
| B | 58 | 22 | 36 | |
| C | 35 | 8 | 27 |
Abbreviations: AFP, α-fetoprotein; BCLC, Barcelona Clinic Liver Cancer; HBsAg, hepatitis B surface antigen; mRECIST, modified response evaluation criteria.
Discussion
The current study showed that patients with HCC had significantly lower baseline serum miR-199a/b-3p levels compared with healthy controls. A significant correlation between baseline serum miR-199a/b-3p levels and tumor size was observed, and there was a tendency for serum miR-199a/b-3p expression levels to increase with the progression of BCLC stage (stage C > B > A). No other significant correlations between serum miR-199a/b-3p levels and patient characteristics, such as sex, age, vascular invasion, AFP, number of tumors, Child–Pugh classification, hepatitis B surface antigen, and liver cirrhosis or BCLC stage, were found. In accordance with our data, Hou et al reported that miR-199a/b-3p was consistently decreased in HCC tissue compared with healthy tissue from both patients and healthy controls. Yin et al18 in their study reported that serum miR-199a-3p expression level was significantly downregulated in patients with HCC compared with healthy controls and appeared to be potentially useful biomarkers for HCC detection. Our study results support an important and a specific role of miR-199a/b-3p in HCC tumorigenesis and tumor progression. Moreover, the downregulation of miR-199a/b-3p has been observed in several other cancers.
In papillary renal cell carcinoma, miR-199a-3p overexpression significantly decreased cell proliferation through regulating the expression of genes linked to the focal adhesion and extracellular matrix pathways, such as caveolin 2, integrin beta 8, MET proto-oncogene, and mammalian target of rapamycin (mTOR).19 Catecholamines were shown to induce mTOR activation through the inhibition of miR-199a/b-3p in breast cancer.20 In addition, miR-199a-3p was found to have an effect on mTOR through different signaling pathways in glioma, papillary thyroid carcinoma, and endometrial endometrioid adenocarcinoma,21–23 while miR-199a-3p inhibited hepatocyte growth factor/c-Met signaling to suppress renal cancer carcinoma.24 miR-199a/b-3p was shown to be overexpressed in head and neck adenoid cystic carcinoma compared with squamous cell carcinoma, indicating that lower miR-199a/b-3p expression levels indicated a more aggressive and malignant tumor phenotype.25 miR-199a-3p was expressed at low levels in ovarian cancer, and miR-199a-3p drastically inhibited ovarian cancer progression through the downregulation of c-Met expression.26 Similarly, miR-199a-3p was expressed at lower levels in osteosarcoma and played an important role in the development of apoptosis, metastasis, recurrence, and drug resistance via different pathways, such as the cluster of differentiation 44 (CD44), p53, and Akt.27–29 miR-199a-3p was downregulated in cancerous tissues compared with normal prostate tissues, with the expression pattern inversely correlated with that of Aurora kinase A.30 A previous study suggested that NLK was an identified miR-199a-3p target gene and functioned as a tumor suppressor gene in colorectal cancer.31 In addition, miR-199a-3p was downregulated in bladder and gastric cancer.32,33 The findings from the current study were consistent with these results, and our nonresponder group had significantly lower miR-199a/b-3p expression levels at t1 than the responder group, demonstrating that miR-199a/b-3p may be an important regulator in the process of HCC.
The potential of circulating miRs to be used as cancer biomarkers is based on their high stability and their capacity to reflect tumor status and predict therapy response.34 Circulating miRs in blood are resistant to degradation by RNase enzymes and remain stable.9 An increase in miR-199a/b-3p expression levels would be expected after TACE treatment, because healthy controls had a higher expression of miR-199a/b-3p in both tissue and serum compared with patients with HCC, indicating miR-199a/b-3p as a tumor suppressor. However, interestingly, our results showed that there was actually a great decrease in miR-199a/b-3pt1-t2 in the responder group compared with the nonresponder group, and a higher proportion of the responder group achieved a >25% decrease in serum miR-199a/b-3p expression levels compared with the nonresponder group. One possible explanation may be that miR-199a/b-3p was downregulated under the hypoxia induced by TACE treatment. Kinose et al26 screened miRs to identify those that displayed altered expression patterns under hypoxic conditions and then analyzed their functional roles in ovarian cancer progression. Their miR PCR arrays, performed on cells from two ovarian cancer cell lines (CaOV3 and RMUG-S), revealed that miR-199a-3p was downregulated under hypoxia. The upregulation of hypoxia-inducible factor-1α (HIF-1α) that occurs under hypoxic conditions suppresses miR-199a-5p expression levels and promotes glycolysis, whereas reintroduction of miR-199a-5p interferes with HK2 expression, abrogating hypoxia-enhanced glycolysis.35 As tumors grow, it becomes increasingly difficult for the inner cancer cells to get sufficient oxygen supply from the blood, and hypoxia occurs in the majority of solid tumors, including HCC. Consequently, HIF-1α is upregulated in a number of human cancers. Moreover, killing the cells in the tumor lesions may decrease the stimulation to secrete miR-199a/b-3p. This would partly explain why serum miR-199a/b-3p was downregulated rather than upregulated in our patients after the first TACE treatment. Serum miR-199a/b-3p expression levels stabilized or increased after TACE treatment, indicating that the tumor lesions did not have a good response to TACE therapy. Therefore, this study shows, for the first time to our knowledge, a link between serum miR-199a/b-3p expression levels and efficacy of TACE in patients with HCC.
miR-199a/b-3p was downregulated in HCC compared with control tissue samples, and in addition, a significantly higher expression of miR-199a/b-3p was observed in cirrhotic tissue compared with noncirrhotic liver tissue, not only in HCC tissue but also in control tissue samples. In a previous study, HCC tissue was shown to have a sharp decrease in miR-199a/b-3p expression levels.15 However, in our study, serum miR-199a/b-3p expression levels were not significantly different between cirrhotic and noncirrhotic tissue in either patients with HCC (Table 2; P=0.682) or healthy controls (P=0.572). Yeligar et al observed that liver sinusoidal endothelial cells derived from ethanol-fed rats showed several fold increases in the mRNA expression of endothelin-1 (ET-1), HIF-1α, and inflammatory cytochemokines compared with control rat liver sinusoidal endothelial cells. In addition, miR-199 attenuated HIF-1α and ET-1 expression, whereas anti-miR-199 reversed these effects, suggesting that ethanol-induced miR-199 downregulation may contribute to augmented HIF-1α and ET-1 expression. Moreover, the presence of the same complementary binding sites for miRs in 3′-untranslated regions of both HIF-1α and ET-1 mRNA showed that miR-199 was a common mediator of HIF-1α and ET-1 mRNA expression.36 It therefore seems that miR-199a/b-3p plays an important role in the entire process from normal liver to liver cirrhosis, and finally to HCC. This possibility warrants further study.
In the current study, mRECIST response was identified as a predictor of overall survival in patients with HCC undergoing TACE treatment. It is generally accepted that the assessment of objective response is crucial in the evaluation of the effect of antitumor treatment.37 Lencioni and Llovet17 demonstrated that mRECIST assessment with the addition of the concept of viable enhancing lesions was clearly different from the traditional RECIST assessment. The only drawback in the newer scale is that response assessment by mRECIST is performed 4 weeks after TACE treatment. Our results showed that the change in the expression of serum miR-199a/b-3pt1-t2 could be a potential biomarker to reliably predict TACE treatment response and thereby be an alternative method to guide therapeutic decision making ahead of time.
The current study has some limitations. Because of the retrospective nature of the study, the serum samples of some patients were in storage for long periods of time and might have been subject to degradation. Another limitation of this study is the limited number of patients and controls. Finally, we measured the relative level rather than the absolute concentration of miR-199a/b-3p.
Conclusion
Our present study provides new insight on serum miR-199-a/b-3p that may represent a novel biomarker for predicting efficacy of TACE for patients with HCC.
Acknowledgments
This work was supported by the Science and Technology Planning Project of Guangdong Province, People’s Republic of China (grant no 2012B010200027) and the Key Technologies R&D Program of Guangzhou, People’s Republic of China (no 201300000199). The authors thank Xihe Qin and Zhou Wu for their technical assistance.
Footnotes
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. doi: 10.3322/caac.21262. [DOI] [PubMed] [Google Scholar]
- 2.Yang JD, Roberts LR. Epidemiology and management of hepatocellular carcinoma. Infect Dis Clin North Am. 2010;24(4):899–919. viii. doi: 10.1016/j.idc.2010.07.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mabed M, Esmaeel M, El-Khodary T, Awad M, Amer T. A randomized controlled trial of transcatheter arterial chemoembolization with lipiodol, doxorubicin and cisplatin versus intravenous doxorubicin for patients with unresectable hepatocellular carcinoma. Eur J Cancer Care. 2009;18(5):492–499. doi: 10.1111/j.1365-2354.2008.00984.x. [DOI] [PubMed] [Google Scholar]
- 4.Golfieri R, Renzulli M, Mosconi C, et al. Bologna Liver Oncology Group (BLOG) Hepatocellular carcinoma responding to superselective transarterial chemoembolization: an issue of nodule dimension? J Vasc Interv Radiol. 2013;24(4):509–517. doi: 10.1016/j.jvir.2012.12.013. [DOI] [PubMed] [Google Scholar]
- 5.Gottesman S. Small RNAs shed some light. Cell. 2004;118(1):1–2. doi: 10.1016/j.cell.2004.06.024. [DOI] [PubMed] [Google Scholar]
- 6.Caldas C, Brenton JD. Sizing up miRNAs as cancer genes. Nat Med. 2005;11(7):712–714. doi: 10.1038/nm0705-712. [DOI] [PubMed] [Google Scholar]
- 7.Krol J, Loedige I, Filipowicz W. The widespread regulation of microRNA biogenesis, function and decay. Nat Rev Genet. 2010;11(9):597–610. doi: 10.1038/nrg2843. [DOI] [PubMed] [Google Scholar]
- 8.Chen X, Ba Y, Ma L, et al. Characterization of microRNAs in serum: a novel class of biomarkers for diagnosis of cancer and other diseases. Cell Res. 2008;18(10):997–1006. doi: 10.1038/cr.2008.282. [DOI] [PubMed] [Google Scholar]
- 9.Mitchell PS, Parkin RK, Kroh EM, et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proc Natl Acad Sci U S A. 2008;105(30):10513–10518. doi: 10.1073/pnas.0804549105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hou J, Lin L, Zhou W, et al. Identification of miRNomes in human liver and hepatocellular carcinoma reveals miR-199a/b-3p as therapeutic target for hepatocellular carcinoma. Cancer Cell. 2011;19(2):232–243. doi: 10.1016/j.ccr.2011.01.001. [DOI] [PubMed] [Google Scholar]
- 11.Lin L, Lin Y, Jin Y, Zheng C. Microarray analysis of microRNA expression in liver cancer tissues and normal control. Gene. 2013;523(2):158–160. doi: 10.1016/j.gene.2013.02.055. [DOI] [PubMed] [Google Scholar]
- 12.Mudduluru G, Ceppi P, Kumarswamy R, Scagliotti GV, Papotti M, Allgayer H. Regulation of Axl receptor tyrosine kinase expression by miR-34a and miR-199a/b in solid cancer. Oncogene. 2011;30(25):2888–2899. doi: 10.1038/onc.2011.13. [DOI] [PubMed] [Google Scholar]
- 13.Fornari F, Milazzo M, Chieco P, et al. MiR-199a-3p regulates mTOR and c-Met to influence the doxorubicin sensitivity of human hepato-carcinoma cells. Cancer Res. 2010;70(12):5184–5193. doi: 10.1158/0008-5472.CAN-10-0145. [DOI] [PubMed] [Google Scholar]
- 14.Kim S, Lee UJ, Kim MN, et al. MicroRNA miR-199a* regulates the MET proto-oncogene and the downstream extracellular signal-regulated kinase 2 (ERK2) J Biol Chem. 2008;283(26):18158–18166. doi: 10.1074/jbc.M800186200. [DOI] [PubMed] [Google Scholar]
- 15.Wojcicka A, Swierniak M, Kornasiewicz O, et al. Next generation sequencing reveals microRNA isoforms in liver cirrhosis and hepatocellular carcinoma. Int J Biochem Cell Biol. 2014;53:208–217. doi: 10.1016/j.biocel.2014.05.020. [DOI] [PubMed] [Google Scholar]
- 16.Qin S, Primary Liver Cancer Diagnosis and Treatment Expert Panel of the Chinese Ministry of Health Guidelines on the diagnosis and treatment of primary liver cancer (2011 edition) Chin Clin Oncol. 2012;1(1):10. doi: 10.3978/j.issn.2304-3865.2012.07.01. [DOI] [PubMed] [Google Scholar]
- 17.Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30(1):52–60. doi: 10.1055/s-0030-1247132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Yin J, Hou P, Wu Z, Wang T, Nie Y. Circulating miR-375 and miR-199a-3p as potential biomarkers for the diagnosis of hepatocellular carcinoma. Tumour Biol. 2015;36(6):4501–4507. doi: 10.1007/s13277-015-3092-0. [DOI] [PubMed] [Google Scholar]
- 19.Wala SJ, Karamchandani JR, Saleeb R, et al. An integrated genomic analysis of papillary renal cell carcinoma type 1 uncovers the role of focal adhesion and extracellular matrix pathways. Mol Oncol. 2015;9(8):1667–1677. doi: 10.1016/j.molonc.2015.04.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Liu D, Yang Z, Wang T, et al. β2-AR signaling controls trastuzumab resistance-dependent pathway. Oncogene. 2015;35(1):47–58. doi: 10.1038/onc.2015.58. [DOI] [PubMed] [Google Scholar]
- 21.Shen L, Sun C, Li Y, et al. MicroRNA-199a-3p suppresses glioma cell proliferation by regulating the AKT/mTOR signaling pathway. Tumour Biol. 2015;36(9):6929–6938. doi: 10.1007/s13277-015-3409-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Minna E, Romeo P, De Cecco L, et al. miR-199a-3p displays tumor suppressor functions in papillary thyroid carcinoma. Oncotarget. 2014;5(9):2513–2528. doi: 10.18632/oncotarget.1830. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wu D, Huang HJ, He CN, Wang KY. MicroRNA-199a-3p regulates endometrial cancer cell proliferation by targeting mammalian target of rapamycin (mTOR) Int J Gynecol Cancer. 2013;23(7):1191–1197. doi: 10.1097/IGC.0b013e31829ea779. [DOI] [PubMed] [Google Scholar]
- 24.Huang J, Dong B, Zhang J, et al. miR-199a-3p inhibits hepatocyte growth factor/c-Met signaling in renal cancer carcinoma. Tumour Biol. 2014;35(6):5833–5843. doi: 10.1007/s13277-014-1774-7. [DOI] [PubMed] [Google Scholar]
- 25.Veit JA, Scheckenbach K, Schuler PJ, et al. MicroRNA expression in differentially metastasizing tumors of the head and neck: adenoid cystic versus squamous cell carcinoma. Anticancer Res. 2015;35(3):1271–1277. [PubMed] [Google Scholar]
- 26.Kinose Y, Sawada K, Nakamura K, et al. The hypoxia-related microRNA miR-199a-3p displays tumor suppressor functions in ovarian carcinoma. Oncotarget. 2015;6(13):11342–11356. doi: 10.18632/oncotarget.3604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Gao Y, Feng Y, Shen JK, et al. CD44 is a direct target of miR-199a-3p and contributes to aggressive progression in osteosarcoma. Sci Rep. 2015;5:11365. doi: 10.1038/srep11365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Tian Y, Zhang YZ, Chen W. MicroRNA-199a-3p and microRNA-34a regulate apoptosis in human osteosarcoma cells. Biosci Rep. 2014;34(4):e00132. doi: 10.1042/BSR20140084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Tian R, Xie X, Han J, et al. miR-199a-3p negatively regulates the progression of osteosarcoma through targeting AXL. Am J Cancer Res. 2014;4(6):738–750. [PMC free article] [PubMed] [Google Scholar]
- 30.Qu Y, Huang X, Li Z, et al. miR-199a-3p inhibits aurora kinase A and attenuates prostate cancer growth: new avenue for prostate cancer treatment. Am J Pathol. 2014;184(5):1541–1549. doi: 10.1016/j.ajpath.2014.01.017. [DOI] [PubMed] [Google Scholar]
- 31.Han Y, Kuang Y, Xue X, et al. NLK, a novel target of miR-199a-3p, functions as a tumor suppressor in colorectal cancer. Biomed Pharmacother. 2014;68(5):497–505. doi: 10.1016/j.biopha.2014.05.003. [DOI] [PubMed] [Google Scholar]
- 32.Ratert N, Meyer HA, Jung M, et al. miRNA profiling identifies candidate miRNAs for bladder cancer diagnosis and clinical outcome. J Mol Diagn. 2013;15(5):695–705. doi: 10.1016/j.jmoldx.2013.05.008. [DOI] [PubMed] [Google Scholar]
- 33.Peng W, Chen ZY, Wang L, Wang Z, Li J. MicroRNA-199a-3p is downregulated in gastric carcinomas and modulates cell proliferation. Genet Mol Res. 2013;12(3):3038–3047. doi: 10.4238/2013.August.20.5. [DOI] [PubMed] [Google Scholar]
- 34.Cortez MA, Welsh JW, Calin GA. Circulating microRNAs as noninvasive biomarkers in breast cancer. Recent Results Cancer Res. 2012;195:151–161. doi: 10.1007/978-3-642-28160-0_13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Guo W, Qiu Z, Wang Z, et al. MiR-199a-5p is negatively associated with the malignancies and regulates glycolysis and lactate production by targeting hexokinase 2 in liver cancer. Hepatology. 2015;62(4):1132–1144. doi: 10.1002/hep.27929. [DOI] [PubMed] [Google Scholar]
- 36.Yeligar S, Tsukamoto H, Kalra VK. Ethanol-induced expression of ET-1 and ET-BR in liver sinusoidal endothelial cells and human endothelial cells involves hypoxia-inducible factor-1alpha and microrNA-199. J Immunol. 2009;183(8):5232–5243. doi: 10.4049/jimmunol.0901084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Jung ES, Kim JH, Yoon EL, et al. Comparison of the methods for tumor response assessment in patients with hepatocellular carcinoma undergoing transarterial chemoembolization. J Hepatol. 2013;58(6):1181–1187. doi: 10.1016/j.jhep.2013.01.039. [DOI] [PubMed] [Google Scholar]