

Abstract
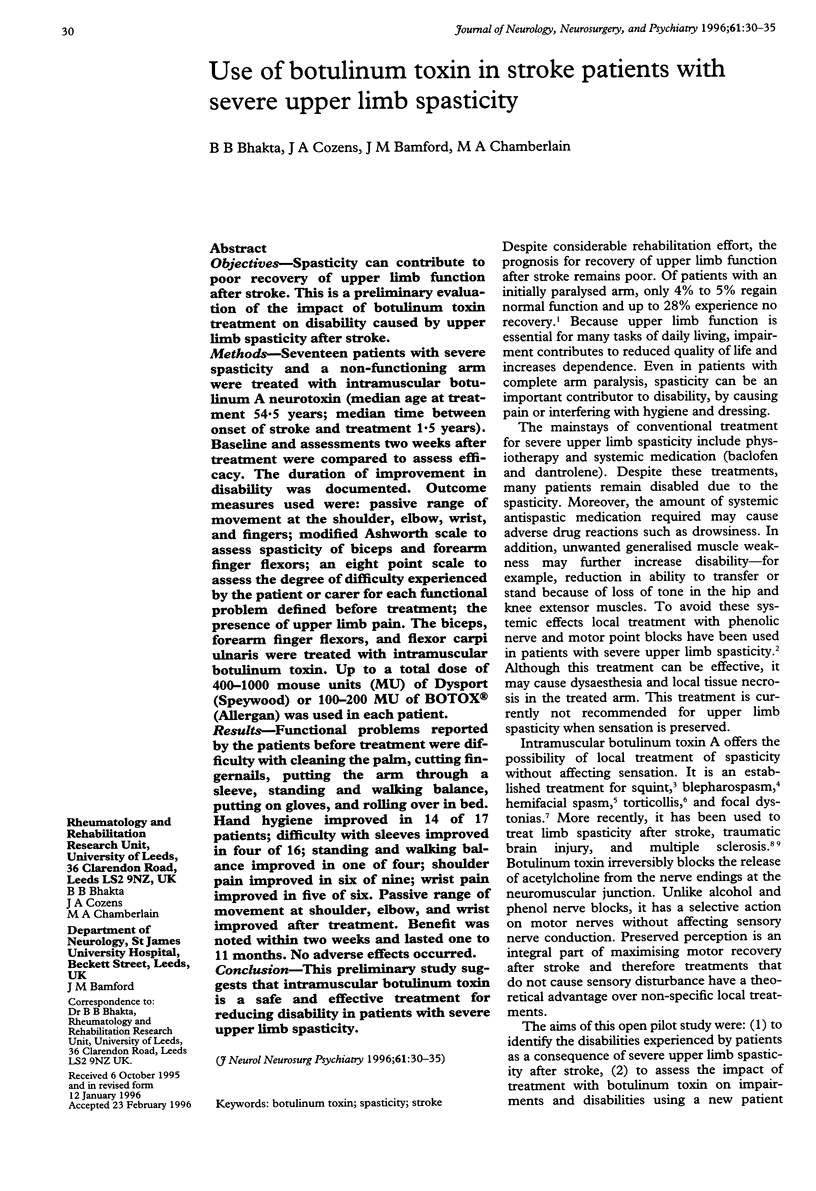
OBJECTIVES--Spasticity can contribute to poor recovery of upper limb function after stroke. This is a preliminary evaluation of the impact of botulinum toxin treatment on disability caused by upper limb spasticity after stroke. METHODS--Seventeen patients with severe spasticity and a non-functioning arm were treated with intramuscular botulinum A neurotoxin (median age at treatment 54.5 years; median time between onset of stroke and treatment 1.5 years). Baseline and assessments two weeks after treatment were compared to assess efficacy. The duration of improvement in disability was documented. Outcome measures used were; passive range of movement at the shoulder, elbow, wrist, and fingers; modified Ashworth scale to assess spasticity of biceps and forearm finger flexors; an eight point scale to assess the degree of difficulty experienced by the patient or carer for each functional problem defined before treatment; the presence of upper limb pain. The biceps, forearm finger flexors, and flexor carpiulnaris were treated with intramuscular botulinum toxin. Up to a total dose of 400-1000 mouse units (MU) of Dysport (Speywood) or 100-200 MU of BOTOX (Allergan) was used in each patient. RESULTS--Functional problems reported by the patients before treatment were difficulty with cleaning the palm, cutting fingernails, putting the arm through a sleeve, standing and walking balance, putting on gloves, and rolling over in bed. Hand hygiene improved in 14 of 17 patients; difficulty with sleeves improved in four of 16; standing and walking balance improved in one of four; shoulder pain improved in six of nine; wrist pain improved in five of six. Passive range of movement at shoulder, elbow, and wrist improved after treatment. Benefit was noted within two weeks and lasted one to 11 months. No adverse effects occurred. CONCLUSION--This preliminary study suggests that intramuscular botulinum toxin is a safe and effective treatment for reducing disability in patients with severe upper limb spasticity.
Full text
PDF



Images in this article



Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Anderson T. J., Rivest J., Stell R., Steiger M. J., Cohen H., Thompson P. D., Marsden C. D. Botulinum toxin treatment of spasmodic torticollis. J R Soc Med. 1992 Sep;85(9):524–529. [PMC free article] [PubMed] [Google Scholar]
- Bohannon R. W., Smith M. B. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther. 1987 Feb;67(2):206–207. doi: 10.1093/ptj/67.2.206. [DOI] [PubMed] [Google Scholar]
- Borodic G. E., Joseph M., Fay L., Cozzolino D., Ferrante R. J. Botulinum A toxin for the treatment of spasmodic torticollis: dysphagia and regional toxin spread. Head Neck. 1990 Sep-Oct;12(5):392–399. doi: 10.1002/hed.2880120504. [DOI] [PubMed] [Google Scholar]
- Das T. K., Park D. M. Effect of treatment with botulinum toxin on spasticity. Postgrad Med J. 1989 Apr;65(762):208–210. doi: 10.1136/pgmj.65.762.208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flanders M., Chin D., Boghen D. Botulinum toxin: preferred treatment for hemifacial spasm. Eur Neurol. 1993;33(4):316–319. doi: 10.1159/000116961. [DOI] [PubMed] [Google Scholar]
- Pearce L. B., First E. R., Borodic G. E. Botulinum toxin potency: a mystery resolved by the median paralysis. J R Soc Med. 1994 Sep;87(9):571–572. [PMC free article] [PubMed] [Google Scholar]
- Scott A. B. Botulinum toxin injection of eye muscles to correct strabismus. Trans Am Ophthalmol Soc. 1981;79:734–770. [PMC free article] [PubMed] [Google Scholar]
- Scott A. B., Kennedy R. A., Stubbs H. A. Botulinum A toxin injection as a treatment for blepharospasm. Arch Ophthalmol. 1985 Mar;103(3):347–350. doi: 10.1001/archopht.1985.01050030043017. [DOI] [PubMed] [Google Scholar]
- Snow B. J., Tsui J. K., Bhatt M. H., Varelas M., Hashimoto S. A., Calne D. B. Treatment of spasticity with botulinum toxin: a double-blind study. Ann Neurol. 1990 Oct;28(4):512–515. doi: 10.1002/ana.410280407. [DOI] [PubMed] [Google Scholar]
- Tugwell P., Bombardier C., Buchanan W. W., Goldsmith C. H., Grace E., Hanna B. The MACTAR Patient Preference Disability Questionnaire--an individualized functional priority approach for assessing improvement in physical disability in clinical trials in rheumatoid arthritis. J Rheumatol. 1987 Jun;14(3):446–451. [PubMed] [Google Scholar]
- Wiegand H., Erdmann G., Wellhöner H. H. 125I-labelled botulinum A neurotoxin: pharmacokinetics in cats after intramuscular injection. Naunyn Schmiedebergs Arch Pharmacol. 1976;292(2):161–165. doi: 10.1007/BF00498587. [DOI] [PubMed] [Google Scholar]