

Abstract
Introduction:
Type 2 diabetes mellitus is a significant health problem and imposes great physical, financial and psychological burden among the affected population. Among people with diabetes, fatigue is a pervasive and distressing complaint, which is further accentuated by presence of depression.
Objective:
To assess the prevalence of fatigue and depression and associated clinical and socio demographic correlates in type 2diabetes.
Materials and Methods:
This cross sectional study included 100 patients of diabetes type 2 and equal number of healthy controls between the ages of 18 to 70 years. A detailed evaluation of socio demographic and clinical parameters was made. Participants were also assessed for presence of depression and fatigue using PHQ-9 and Fatigue Severity Scale(FSS)respectively.
Results:
Fatigue and depression was found in 68 % and 53 % of diabetic participants. Diabetic patients were 10.37 times and 4.80 times more likely to suffer from fatigue and depression respectively. Both fatigue and depression were found to be significantly associated with duration of illness, fasting and post prandial blood glucose level, diabetic complications and Body Mass Index (BMI). Fatigue was also strongly correlated with depression in study sample.
Conclusions:
Fatigue and depression are reasonably correlated with type 2 diabetes. Various clinical parameters of diabetes are strongly associated with both fatigue and depression. Fatigue itself has significant correlation with depression in type 2 diabetes. Regular monitoring of biochemical parameters are paramount to predict the development of fatigue and depression in type 2 diabetes.
Keywords: Depression, diabetes mellitus, fatigue
The prevalence of diabetes mellitus has attained an epidemic level across the globe as indicated in reports from the International Diabetes Federation.[1] Among people with diabetes, fatigue is a pervasive and distressing complaint.[2]
It is difficult to define fatigue due to great discrepancy among causes and indicators. In general, it may be defined as a complex phenomenon including physiological, psychological, and situational components.[3] The prevalence of fatigue in diabetes has been found as high as 61% in an epidemiological study of type 2 diabetes patients.[4]
Fatigue can result from various physiological factors associated with diabetes, such as hypo- and hyperglycemia, and the wide swings between the two.[5] Numerous complications have also been found contributing to the development or exacerbation of fatigue in this population. Various lifestyle issues such as physical activities or high body mass index (BMI) may also give rise to fatigue in type 2 diabetes.[6] Psychological factors such as depression and anxiety may also result in fatigue. It has been suggested that psychological disorders are more predictive of fatigue than the physical illnesses. Association between diabetes and depression has also been well established. A study[7] in recent past has reported the prevalence of depression in patients with diabetes as high as 71.8%. Despite high frequency and impact of fatigue in patients with diabetes and its association with depression, only a few studies have explored this issue. Hence, this study was designed to investigate the prevalence of fatigue and depression in type 2diabetes. This study also explores the correlation of sociodemographic and clinical parameters of diabetes type 2 with fatigue and depression.
METHODOLOGY
This cross-sectional study was conducted in collaboration between Department of Psychiatry and Diabetes Clinic of Department of Medicine in a secondary care referral hospital. The hospital is a multispecialty treatment facility center catering to the health needs of a defined group of the population from the entire province. Diabetes patients are evaluated in detail in routine clinical practice, and all relevant biochemical tests are performed. The nature and purpose of the study were explained to all the participants, and informed consent was obtained before their inclusion in the study sample.
The study sample comprised 100 patients of diabetes between the ages of 18–70 years attending the outpatient department (OPD) of diabetes clinic. Equal number of healthy controls was also enrolled to make a comparison group. Utmost care was taken to ensure the homogeneity of the sample population by recruiting the close relatives or friends of the patients as a control group. The purpose of the study was revealed to the participants and consent was obtained.
Diabetes was defined as either requiring oral or injectable antidiabetic medication or having random blood glucose level above 200 mg/dl.
The participants were excluded from the study if they were known. (1) To have current substance use disorder using Diagnostic and Statistical Manual, Fourth edition (DSM-IV) criteria. (2) To have current or past psychosis or mania or any other mental disorder using DSM-IV criteria except existing major depressive disorder (MDD). (3) To have major medical or surgical problem before the diagnosis of diabetes.
Measures
A detailed evaluation of sociodemographic and clinical profile was made on specially designed semi-structured instrument by interviewing the participants and from the medical records. This included duration of illness, duration of treatment, type of treatment, BMI, complications due to diabetes, fasting, and postprandial blood glucose levels. Participants were also be assessed for the presence of depression and fatigability by applying the Patient Health Questionnaire-9 (PHQ-9) and fatigue severity scale (FSS), respectively. Participants who scored 10 or above on PHQ-9 were further evaluated by psychiatrist.
PHQ-9, a self-report version of PRIME-MD11, which assesses the presence of MDD using modified DSM-IV criteria.[8] There is a good agreement reported between the PHQ diagnosis and those of independent psychiatry health professionals (for the diagnosis of any one or more PHQ disorder, κ = 0.65; overall accuracy, 85%; sensitivity, 75%; specificity, 90%). In this study, Hindi version of PHQ-9 was used. It has been validated in Indian population and is considered to be reliable tool for diagnosis of depression.
The PHQ-9 is a dual instrument that is used to establish a provisional depressive disorder as well as it provides a symptoms severity score. For the diagnosis of depression, we defined clinical significant depression as: A PHQ-9 score of 10 or above.
FSS is the most commonly used fatigue specific questionnaire.[9] The FSS emphasizes the impact of fatigue on daily life in terms of accumulation of functional fatigue effects, which appears suitable for detecting the presence and severity of fatigue.
FSS is designed to differentiate fatigue from clinical depression, since they have some common symptoms. The FSS test different domains including motivation, exercise, and interference with work, family, or social life. It is 9 item questionnaires, and scoring is done by adding up the response (numbers) and dividing by 9. A score of <4 is considered as having no fatigue, score of 4–4.9 are considered as having moderate fatigue, and scores of 5 or more are considered as having severe fatigue. FSS has shown good reliability with a Cronbach's α = 0.89 and also a strong construct validity.
Data analysis
All data collected were entered into Microsoft Excel 2007 worksheet in the form of a master chart. These data were classified and analyzed as per the aims and objectives. The data on sample characteristics were described in the form of tables. Inferential statistics such as Chi-square test was used to find out the association of fatigue and depression with various factors and odds ratio (OR) was used to quantify the association of depression with diabetes. The “Microsoft Excel” and “Primer” software version 6 (developed by McGraw-Hill Global Education Holdings, LLC) were used for analysis of the data.
RESULTS
The study included 100 subjects with diabetes type 2 attending medical OPD. Equal number of age- and sex-matched healthy control was enrolled to serve as a comparison group for assessment of the prevalence of depression and fatigue in cases and controls. The study sample of diabetes patients comprised equal number of females (50%) and males (50%). The mean age of study subjects was 55.08 years (standard deviation [SD] = 11.76) with mean duration of illness being 7.15 years (SD = 5.73). Most of the patients (80%) had been receiving treatment for more than 12 months. Seventy percent (n = 70) had been taking oral medication as compared to 30% of those receiving injectables (n = 30). Fasting and postprandial blood sugar level were raised above normal in 64% (n = 64) and 89% (n = 89) of the study subjects, respectively. The average fasting and postpostprandial blood glucose level of the study subjects were 153.06 mg% (SD = 59.25) and 235.65 mg% (SD = 78.98), respectively. Forty-six percent (n = 46) of the cases were without any diabetic complications. However, 41% (n = 41) had cardiovascular complications including coronary artery disease and hypertension (CAD and HT) and 13% (n = 13) had retinopathy. Almost half (47%) of the subjects had optimal BMI, followed by 34% and 15% being overweight and obese, respectively. Four percent (n = 4) of the patients were underweight.
In this study, fatigue and depression were found in 68% and 53% of diabetes patients as compared to 17% and 19% of nondiabetic participants (OR for fatigue 10.37, 95% confidence interval [CI]: 5.3–20.27; OR for depression 2.8, 95% CI: 2.54–9.07) [Table 1].
Table 1.
Prevalence of fatigue and depression in diabetic cases and controls

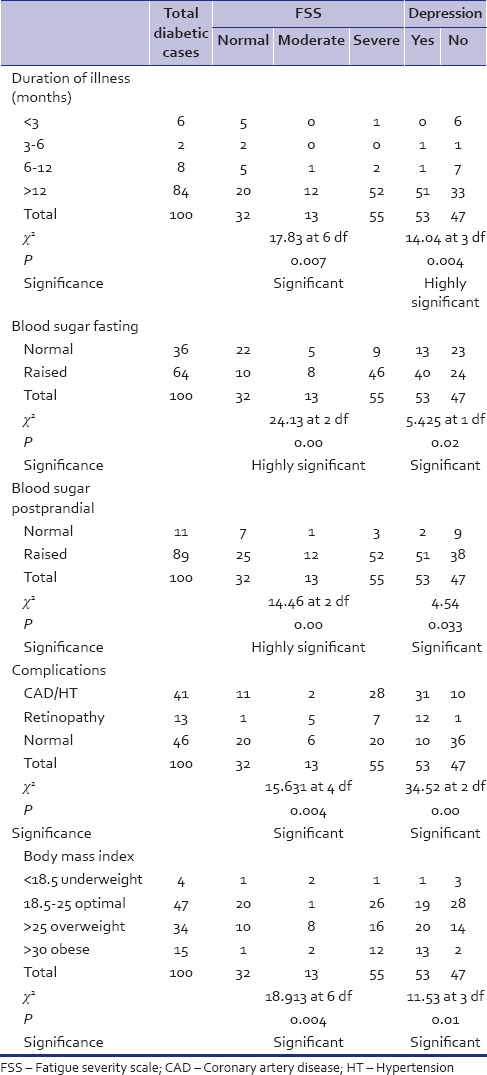
Fatigue and depression both were found to be significantly associated with duration of illness, blood glucose level fasting as well as postprandial, with complications of diabetes and BMI among patients with diabetes. However, there was no significant association of fatigue and depression with sex, age, income, and type and duration of treatment [Tables 2 and 3].
Table 2.
Association of sociodemographic factors with fatigue and depression in diabetic cases
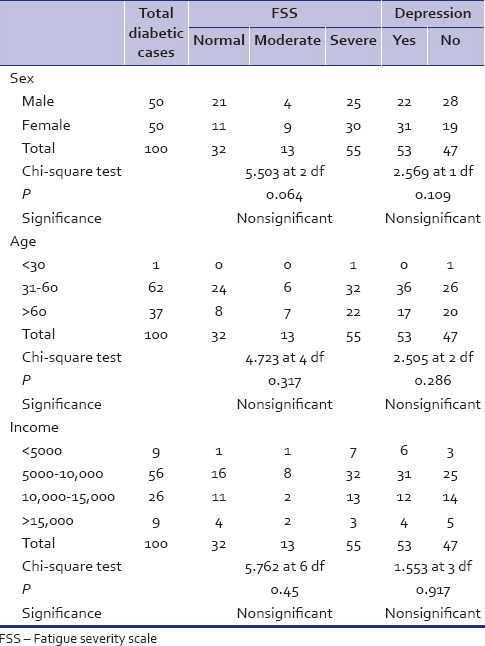
Table 3.
Correlation of clinical parameters with fatigue and depression in diabetic cases
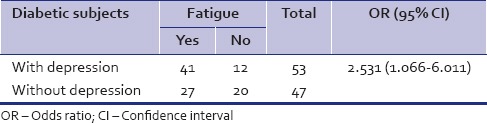
There were 2.53 times more chances of fatigue in diabetic subjects with depression as compared to those without depression [Table 4].
Table 4.
Association of fatigue with depression in diabetic patients
DISCUSSION
Patients of diabetes were almost five times more likely to develop depression than the healthy control group. Similarly, Khamseh et al.[7] reported the prevalence of depression being as high as 71.8% in a sample of 206 Iranian patients with type 1 and type 2 diabetes corroborating finding of this study.
Two major hypotheses are currently proposed to explain the causal pathway between diabetes and depression. One hypothesis suggests that depression precedes type 2 diabetes. The increased risk of type 2 diabetes in individual with depression has been attributed to increased counter-regulatory hormone release and action, alteration in glucose transport function, and increased immune inflammatory activation.[10] These physiological alterations in turn lead to insulin resistance and beta islet cell dysfunction leading to the development of type 2 diabetes. Another hypothesis assumes that chronic psychological stressors associated with chronic medical conditions such as diabetes may result in depression.[11]
Prevalence of fatigue was assessed using FSS, which tests the fatigue severity in terms of both mental and physical domain. Further analysis of distribution curve has revealed that the FSS was normally distributed even in small sample which may indicate that FSS is the most appropriate test to use in this population.
In this study, odds of fatigue were almost 10 times more in diabetes patients in comparison to healthy controls. Our result in this regard is identical to previous studies. Epidemiological studies comprising 1137 subjects with type 2 diabetes has reported prevalence of fatigue as high as 61% which is almost in comparison to this study.[4] The preponderance of fatigue in diabetes can result from various factors incorporating physiological changes such as altered blood glucose levels, diabetic complications, psychological phenomenon, diabetes-related emotional distress, or lifestyle factors such as being overweight or physically inactive.
Significant association of various clinical parameters of diabetes was established with fatigue and depression. This included duration of illness, blood glucose level both fasting and postprandial, BMI, and diabetic complications including CAD, HT, and retinopathy.
Correlation between duration of diabetes and high prevalence of depression has been established in other studies as well.[12] However, Balhara et al.[13] reported no such association between duration of diabetes and depression. The chronicity of illness is likely to impose several negative impacts including cost of treatment, poor drug compliance, diabetic complications, and increased fatigue which may cumulatively contribute to develop depression in these patients.
Duration of diabetes in this study has also been found associated with fatigue. Similar correlation has been established by Calrelti-Weder et al.[14] who evaluated fatigue in a placebo-controlled double blind study of interleukin 1 beta (IL-1 β) antagonism with monoclonal anti IL-1 β antibody in 30 patients of type 2 diabetes.
Blood glucose levels both fasting and postprandial were associated with depression and fatigue. Fatigue was found significantly associated with fasting plasma glucose levels in an epidemiological study of 1137 newly diagnosed type 2 diabetes.[3] The probable reason for fatigue in diabetes may be alteration in blood glucose level. Altered blood glucose metabolism may result in hypo- or hyperglycemia. Fatigue may get affected by these alterations separately or in tandem.
There is ample of evidence that establishes association between comorbid depression with poor glycemic control in diabetes. Lustman et al.[15] in his meta-analysis of 24 studies have found that depression was significantly associated with poor glycemic control in individuals with type 1 and type 2 diabetes. Comorbid depression exerts negative impact among individuals with diabetes. This includes less physical activities, unhealthy and irregular diet, and lower adherence to oral medications.
Significant association of BMI with depression and fatigue was observed in this study. Similar observations have been made by another study in India by Balhara et al.[13] who have reported that BMI has been associated with increased prevalence of depression and anxiety in type 2 diabetes. Obesity often leads to low self-esteem associated with economical, social, and psychological problems. This might contribute to negative affective state in these patients. Fritschi et al.[16] studied 83 women with type 2 diabetes to assess risk factors for fatigue. Higher BMI was one of the strongest explanatory factors for fatigue. It is proposed that the fatigue itself may interfere with physical activity, hence interrupts in weight reduction. Thus, fatigue tends to generate a vicious cycle with self-exacerbating condition.
Diabetic complications were also associated with depression and fatigue in this study. Earlier studies have reported similar kind of association. Clouse et al.[17] found that onset and prevalence of coronary heart disease were affected in depressed diabetic women. Depression in these patients may negatively influence the drug compliance, physical activity, and diet intake leading to development of complications which itself may further contribute to development or exacerbation mood symptoms thus ensue a vicious cycle.
Like our study, fatigue was found significantly associated with a number of diabetic complications in a cross-sectional study designed to examine the presence of fatigue in type 2 diabetes.[18] Complications are likely to result in fatigue as it makes an individual more incapacitating and fragile. Presence of depression further accentuates the fatigue.
Correlation between depression and fatigue was also established in this study as patients with depression had almost 2½ times more odds to experience fatigue symptoms than those without depression. It is known that depression may predisposes individuals to develop subsequent fatigue. There is evidence to suggest that depression and fatigue may predict and influence each other in time.[19] It has also been proposed that chronic fatigue is merely a form of depression considering the overlap in symptoms and occurrence. However, fatigue seems to have genetic and environmental risk factors that are independent of psychiatric symptoms as reported in twin studies.[20] It has been argued that different definitions of fatigue in different studies may have led to this overlapping between depression and fatigue. Nevertheless, empirical evidence suggests that the association between depression and fatigue becomes even larger when narrower and more exclusive definition of fatigue are used.[21]
Feeling of both mental and physical fatigue is one of the common symptoms of depression, and the association between the two may well be explained by this common sharing of symptoms as well as some common risk factors such as diabetes responsible for the occurrence of both depression and fatigue as evident in this study.
CONCLUSION
Fatigue and depression are reasonably correlated with type 2 diabetes. Various clinical parameters of diabetes including duration of illness, alteration in blood glucose level, BMI, and diabetic complication are strongly associated with fatigue and depression both. Fatigue itself has a significant correlation with depression in type 2 diabetes. Presence of fatigue and depression in these patients may adversely affect the prognosis and impose additional cost of treatment, morbidity and mortality. Regular monitoring of biochemical parameters such as blood glucose level and BMI are paramount to predict the development of fatigue and depression in type 2 diabetes.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.4th ed. Brussels: International Diabetes Federation; 2009. International Diabetes Federation. Diabetes Atlas. [PubMed] [Google Scholar]
- 2.Fritschi C, Quinn L. Fatigue in patients with diabetes: A review. J Psychosom Res. 2010;69:33–41. doi: 10.1016/j.jpsychores.2010.01.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Aaronson LS, Teel CS, Cassmeyer V, Neuberger GB, Pallikkathayil L, Pierce J, et al. Defining and measuring fatigue. Image J Nurs Sch. 1999;31:45–50. doi: 10.1111/j.1547-5069.1999.tb00420.x. [DOI] [PubMed] [Google Scholar]
- 4.Drivsholm T, de Fine Olivarius N, Nielsen AB, Siersma V. Symptoms, signs and complications in newly diagnosed type 2 diabetic patients, and their relationship to glycaemia, blood pressure and weight. Diabetologia. 2005;48:210–4. doi: 10.1007/s00125-004-1625-y. [DOI] [PubMed] [Google Scholar]
- 5.Weijman I, Kant I, Swaen GM, Ros WJ, Rutten GE, Schaufeli WB, et al. Diabetes, employment and fatigue-related complaints: A comparison between diabetic employees, “healthy” employees, and employees with other chronic diseases. J Occup Environ Med. 2004;46:828–36. doi: 10.1097/01.jom.0000135605.62330.ca. [DOI] [PubMed] [Google Scholar]
- 6.Telford RD. Low physical activity and obesity: Causes of chronic disease or simply predictors? Med Sci Sports Exerc. 2007;39:1233–40. doi: 10.1249/mss.0b013e31806215b7. [DOI] [PubMed] [Google Scholar]
- 7.Khamseh ME, Baradaran HR, Rajabali H. Depression and diabetes in Iranian patients: A comparative study. Int J Psychiatry Med. 2007;37:81–6. doi: 10.2190/FP64-82V3-1741-842V. [DOI] [PubMed] [Google Scholar]
- 8.Kroenke K, Spitzer RL, Williams JB. The PHQ-9: Validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch Neurol. 1989;46:1121–3. doi: 10.1001/archneur.1989.00520460115022. [DOI] [PubMed] [Google Scholar]
- 10.Musselman DL, Betan E, Larsen H, Phillips LS. Relationship of depression to diabetes types 1 and 2: Epidemiology, biology, and treatment. Biol Psychiatry. 2003;54:317–29. doi: 10.1016/s0006-3223(03)00569-9. [DOI] [PubMed] [Google Scholar]
- 11.Talbot F, Nouwen A. A review of the relationship between depression and diabetes in adults: Is there a link? Diabetes Care. 2000;23:1556–62. doi: 10.2337/diacare.23.10.1556. [DOI] [PubMed] [Google Scholar]
- 12.Perveen S, Otho MS, Siddiqi MN, Hatcher J, Rafique G. Association of depression with newly diagnosed type 2 diabetes among adults aged between 25 to 60 years in Karachi, Pakistan. Diabetol Metab Syndr. 2010;2:17. doi: 10.1186/1758-5996-2-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Balhara YP, Sagar R. Correlates of anxiety and depression among patients with type 2 diabetes mellitus. Indian J Endocrinol Metab. 2011;15(Suppl 1):S50–4. doi: 10.4103/2230-8210.83057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cavelti-Weder C, Furrer R, Keller C, Babians-Brunner A, Solinger AM, Gast H, et al. Inhibition of IL-1beta improves fatigue in type 2 diabetes. Diabetes Care. 2011;34:e158. doi: 10.2337/dc11-1196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lustman PJ, Anderson RJ, Freedland KE, de Groot M, Carney RM, Clouse RE. Depression and poor glycemic control: A meta-analytic review of the literature. Diabetes Care. 2000;23:934–42. doi: 10.2337/diacare.23.7.934. [DOI] [PubMed] [Google Scholar]
- 16.Fritschi C, Quinn L, Hacker ED, Penckofer SM, Wang E, Foreman M, et al. Fatigue in women with type 2 diabetes. Diabetes Educ. 2012;38:662–72. doi: 10.1177/0145721712450925. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Clouse RE, Lustman PJ, Freedland KE, Griffith LS, McGill JB, Carney RM. Depression and coronary heart disease in women with diabetes. Psychosom Med. 2003;65:376–83. doi: 10.1097/01.psy.0000041624.96580.1f. [DOI] [PubMed] [Google Scholar]
- 18.Singh R, Kluding PM. Fatigue and related factors in people with type 2 diabetes. Diabetes Educ. 2013;39:320–6. doi: 10.1177/0145721713479144. [DOI] [PubMed] [Google Scholar]
- 19.Huibers MJ, Leone SS, van Amelsvoort LG, Kant I, Knottnerus JA. Associations of fatigue and depression among fatigued employees over time: A 4-year follow-up study. J Psychosom Res. 2007;63:137–42. doi: 10.1016/j.jpsychores.2007.02.014. [DOI] [PubMed] [Google Scholar]
- 20.Hickie I, Kirk K, Martin N. Unique genetic and environmental determinants of prolonged fatigue: A twin study. Psychol Med. 1999;29:259–68. doi: 10.1017/s0033291798007934. [DOI] [PubMed] [Google Scholar]
- 21.Skapinakis P, Lewis G, Mavreas V. Unexplained fatigue syndromes in a multinational primary care sample: Specificity of definition and prevalence and distinctiveness from depression and generalized anxiety. Am J Psychiatry. 2003;160:785–7. doi: 10.1176/appi.ajp.160.4.785. [DOI] [PubMed] [Google Scholar]