

Abstract
If the atrial appendages lie adjacent to each other on same side of the great arteries, instead of encircling their roots, they are referred as juxtaposed. Right juxtaposition of atrial appendages is less common than left juxtaposition. The images demonstrate the classical radiological, echocardiographic, and surgical images of juxtaposed atrial appendages. Their clinical incidence, associations, and relevance during interventional and surgical procedures are discussed.
Keywords: Atrial appendages, juxtaposition, imaging
INTRODUCTION
Juxtaposed atrial appendages defined as the two atrial appendages lying adjacent to each other on the same side of the great arteries instead of encircling their roots is reported in 0.28-1.1% of different pathological series.[1,2,3] The initial classification of juxtaposition proposed by Dixon is based on its position in relation to the great arteries. If both appendages are positioned on the left side of the great arteries, then they are called as left juxtaposition. This entity is six times commoner than right juxtaposition, where both atrial appendages lie on the right side of great arteries.[4,5] Dixon's classification is primarily based on the anatomical position of the two atrial appendages only and does not consider the morphology of atrial appendages. The classification proposed by VanPraagh is based on the morphology of the appendages.[1,2] Whenever the morphological right atrial appendage, which is broad, triangular, and more trabeculated, is abnormally positioned above the thin slender fingerlike left atrial appendage, VanPraagh's classification will name this anomaly as juxtaposition of the right atrial appendage.[2] This is commonly associated with significant cardiac anomalies in the heart, most commonly with transposition of great arteries. The other variant, namely juxtaposition of the left atrial appendages, is very rare and may be seen in structurally normal heart or with minor cardiac anomalies also.[1] The morphological definition proposed by Van Praagh has the advantage over Dixon classification when it is applied to situs inversus and in heterotaxy syndromes.[6] The images in this report demonstrate classical features of right and left juxtapositions and discuss their clinical relevance.
FIRST PATIENT
A one year old boy diagnosed with large ventricular septal defect and severe hyperkinetic pulmonary arterial hypertension had situs solitus with levocardia, D-looped ventricles, and normally related great arteries. He had right juxtaposition of the morphological left atrial appendage. The juxtaposed left atrial appendage was lying superior to the right atrial appendage, which was cannulated for cardiopulmonary bypass [Figure 1]. The chest x-ray [Figure 2], echocardiography [Figure 3, Movie 1], and intraoperative transesophageal echocardiogram [Figure 4, Movie 2] showed the classical findings. The patient underwent uneventful surgical correction.
Figure 1.
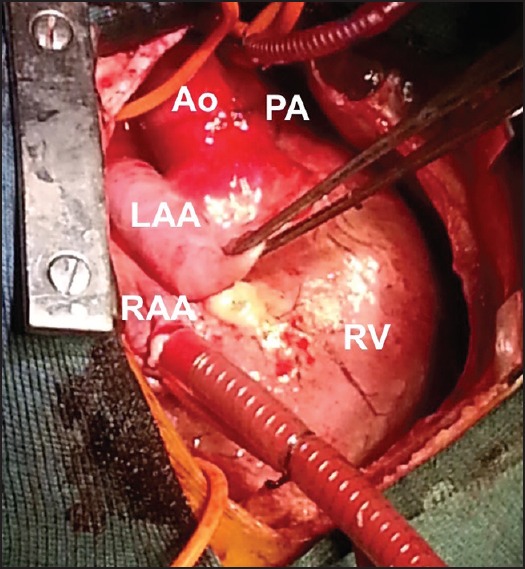
Surgical image of right juxtaposition of left atrial appendage (LAA) held with forceps, lying superior to the normally positioned right atrial appendage (RAA) that has been cannulated. Both appendages appear on the right side of the great arteries, aorta (Ao), and pulmonary artery (PA). RV: Right ventricle
Figure 2.
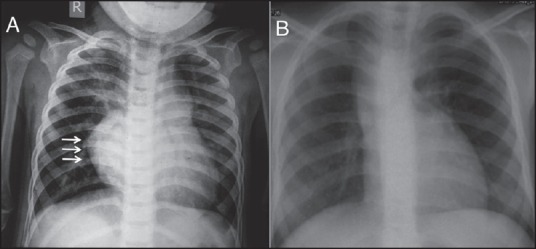
Right atrial border on anteroposterior view of chest X-ray is very prominent and convex shown by arrows (a) In right juxtaposition of atrial appendages and concave (b) In left juxtaposition
Figure 3.
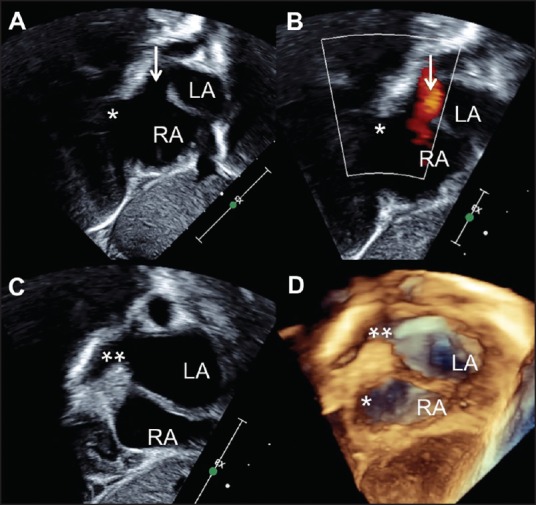
Subxiphoid short axis echocardiogram (A) with color flows (B) showing right atrial appendage* appearing below the entry of the right superior vena cava (shown as arrow). On a further rightward sweep (C) from this view, left atrial appendage** is seen juxtaposed superior to the right atrial appendage. Three-dimensional echocardiogram (D) with a larger volume of data demonstrates both the left atrial and right atrial appendages, the former above the latter. LA - Left atrium, RA - right atrium (Movie 1)
Figure 4.
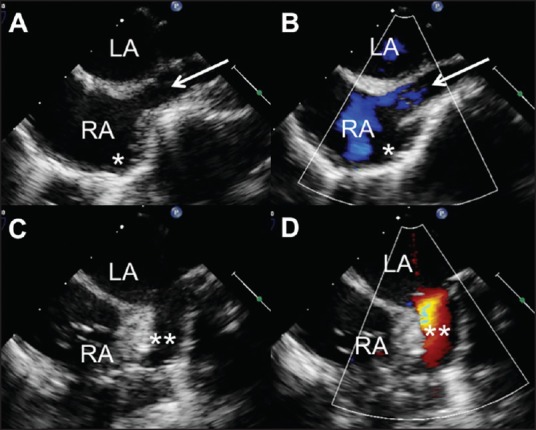
Transesophageal echocardiogram in bi-caval view shows right superior vena cava (arrow) entering the right atrium (RA) with morphological right atrial appendage* projecting anteriorly. On a leftward sweep, the right juxtaposed morphological left atrial appendage** is seen projecting superior to the other appendage (Movie 2)
SECOND PATIENT
A 3-year-old patient diagnosed to have situs solitus, tricuspid atresia, transposed great arteries, large nonrestrictive atrial and ventricular septal defects, and pulmonary stenosis underwent bidirectional Glenn shunt. His chest X-ray [Figure 2], echocardiogram [Figure 5, Movie 3], and angiogram [Figure 6, Movie 4] showed classical findings of left juxtaposition of morphological right atrial appendage.
Figure 5.
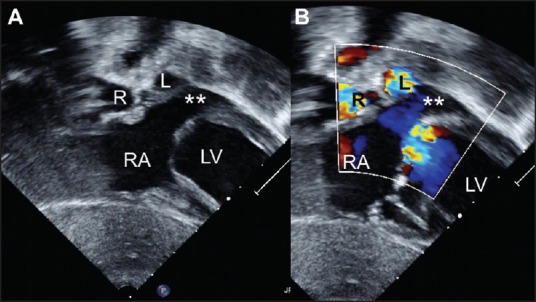
Subxiphoid coronal view echocardiogram (A) with color flows (B) showing left juxtaposition of the morphological right atrial appendage** which projects on the left border of the heart. RA - right atrium, LV- left ventricle, R-right pulmonary artery, L-left pulmonary artery (Movie 3)
Figure 6.
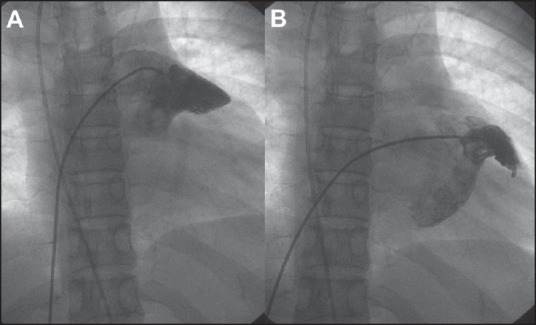
Angiogram with end-hole injection in anteroposterior projection into both the appendages show a broad triangular juxtaposed morphological right atrial appendage (a) Appearing superior to the native morphological finger like left atrial appendage (b) (Movie 4)
DISCUSSION
The left-sided juxtaposition where appendages lie to the left of the great vessels outnumbers the right-sided juxtaposition by a ratio of about 6:1.[4,5,6] Developmentally, left-sided juxtaposition is caused by underdevelopment of torsion of the primitive cardiac tube in the setting of situs solitus and D-ventricular loop. On the contrary, the less common right-sided juxtaposition in situ s solitus is due to the overdevelopment of torsion of primitive cardiac tube.[4] Both anomalies are commonly associated with significant congenital heart disease. Unlike the left juxtaposition of right atrial appendage that is frequently associated with transposition of the great vessels and tricuspid atresia, right juxtaposition of left atrial appendage may be associated with left atrial outlet obstruction, left ventricular hypoplasia, and aortic outflow tract obstruction.[1,2,3] Sometimes the latter is associated with relatively simpler lesions as our second patient or rarely with a structurally normal heart. In rare instances, the atrial appendage on one of the sides may be bifid, with one component in normal position and other component juxtaposed. These rare variants are called “partial juxtaposition.”[6]
The prominent convex right atrial border in right juxtaposition and concave right atrial border in left juxtaposition on the chest X-ray offers the first clues to this anomaly[7] [Figure 2]. Prior identification has implications during cardiac catheterizations and surgery.[8] In all hearts with atrial appendage juxtapositions, the juxtaposed atrial appendage always lies above the native atrial appendage. In the commoner left juxtaposition, the native left atrial appendage lies below the juxtaposed right atrial appendage. On the contrary, in right juxtaposition, the left atrial appendage lies above the right. If this is not recognized during cardiac surgery, the orifice of the juxtaposed atrial appendage may be mistaken for an atrial septal defect and it may be closed with a patch.[8]
In the echocardiographic images of patients with juxtaposition of atrial appendages, the plane of atrial septum in the anterior part is parallel to the anterior chest wall; but in the posterior part it is normally oriented.[8] This horizontal orientation of the anterior atrial septum is the most diagnostic echocardiographic observation in this anomaly. Since the plane of the interatrial septum is different in these patients, occluder devices used to close secundum atrial septal defects that are located in the anterior portion of the atrial septum may have a different device orientation on echocardiography and fluoroscopy.[9]
Catheter entry into pulmonary veins by maneuvering a catheter through the atrial septal defect or patent foramen ovale will not be possible if the catheter or guidewire tip is positioned in the left juxtaposed right atrial appendage instead of the left atrium.[6] Failure to identify position of an inflated septostomy catheter in the left juxtaposed right atrial appendage may lead to trauma to the base of the appendage during the balloon atrial septostomy for the transposition of great arteries, which is the commonest association of this anomaly.[10] In this same anomaly, Blalock Hanlon septectomy is extremely difficult in the setting of juxtaposition due to anatomical smaller size of the right atrium.[11] Mustard operation may also be technically challenging in this anomaly.[12]
Cannulations and venting during cardiopulmonary bypass and performance of surgeries such as senning surgery or lateral tunnel Fontan surgery can be planned well without on-table surprises with prior recognition of these juxtapositions.[13] Even though right atrial to pulmonary artery Fontan surgeries are almost never performed nowadays, this anomaly used to pose significant difficulties in the past. In such instances, direct anastomosis was achieved from the juxtaposed morphological right atrial appendage to the left pulmonary artery.[14]
Videos available on www.annalspc.com
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Van Praagh S, O’Sullivan J, Brili S, Van Praagh R. Juxtaposition of the morphologically left atrial appendage in solitus and inversus atria: A study of 18 postmortem cases. Am Heart J. 1996;132:391–402. doi: 10.1016/s0002-8703(96)90438-x. [DOI] [PubMed] [Google Scholar]
- 2.Van Praagh S, O’Sullivan J, Brili S, Van Praagh R. Juxtaposition of the morphologically right atrial appendage in solitus and inversus atria: A study of 35 postmortem cases. Am Heart J. 1996;132:382–90. doi: 10.1016/s0002-8703(96)90437-8. [DOI] [PubMed] [Google Scholar]
- 3.Lai WW, Ravishankar C, Gross RP, Kamenir SA, Lopez L, Nguyen KH, et al. Juxtaposition of the atrial appendages: A clinical series of 22 patients. Pediatr Cardiol. 2001;22:121–7. doi: 10.1007/s002460010174. [DOI] [PubMed] [Google Scholar]
- 4.Dixon AS. Juxtaposition of the atrial appendages: Two cases of an unusual congenital cardiac deformity. Br Heart J. 1954;16:153–64. doi: 10.1136/hrt.16.2.153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Becker AE, Becker MJ. Juxtaposition of atrial appendages associated with normally oriented ventricles and great arteries. Circulation. 1970;41:685–8. doi: 10.1161/01.cir.41.4.685. [DOI] [PubMed] [Google Scholar]
- 6.Frescura C, Thiene G. Juxtaposition of the atrial appendages. Cardiovasc Pathol. 2012;21:169–79. doi: 10.1016/j.carpath.2011.02.002. [DOI] [PubMed] [Google Scholar]
- 7.Bream PR, Elliott LP, Bargeron LM., Jr Plain film findings of anatomically corrected malposition: Its association with juxtaposition of the atrial appendages and right aortic arch. Radiology. 1978;126:589–95. doi: 10.1148/126.3.589. [DOI] [PubMed] [Google Scholar]
- 8.Rice MJ, Seward JB, Hagler DJ, Edwards WD, Julsrud PR, Tajk AJ. Left juxtaposed atrial appendages: Diagnostic two-dimensional echocardiographic features. J Am Coll Cardiol. 1983;1:1330–6. doi: 10.1016/s0735-1097(83)80148-x. [DOI] [PubMed] [Google Scholar]
- 9.Sivakumar K. Catheter closure of an atrial septal defect in anatomically corrected malposition with left juxtaposition of atrial appendages. Cardiol Young. 2009;19:534–6. doi: 10.1017/S1047951109990849. [DOI] [PubMed] [Google Scholar]
- 10.Tyrell MJ, Moes CA. Congenital levoposition of the right atrial appendage. Its relevance to balloon septostomy. Am J Dis Child. 1971;121:508–10. doi: 10.1001/archpedi.1971.02100170090013. [DOI] [PubMed] [Google Scholar]
- 11.Rosenquist GC, Stark J, Taylor JF. Anatomical relationships in transposition of the great arteries: Juxtaposition of the atrial appendages. Ann Thorac Surg. 1974;18:456–61. doi: 10.1016/s0003-4975(10)64386-x. [DOI] [PubMed] [Google Scholar]
- 12.Vidne BA, Subramanian S. Complete correction of transposition of the great arteries with left juxtaposition of the atrial appendages. Thorax. 1976;31:178–80. doi: 10.1136/thx.31.2.178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Deutsch V, Shem-Tov A, Yahini JH, Neufeld HN. Juxtaposition of atrial appendages: Angiocardiographic observations. Am J Cardiol. 1974;34:240–4. doi: 10.1016/0002-9149(74)90204-5. [DOI] [PubMed] [Google Scholar]
- 14.Kidani M, Noto T, Okamura H. Surgical repair of tricuspid atresia with juxtaposition of the atrial appendages, direct anastomosis of right atrial appendage to the pulmonary artery (author's transl) Kyobu Geka. 1979;32:630–3. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.