

Abstract
The aim here was to report a case of a young adult patient who evolved with tumor formation in the left thigh, 14 years after revision surgery on hip arthroplasty. Davies in 2005 made the first description of this disease in patients undergoing metal-on-metal hip arthroplasty. Over the last decade, however, pseudotumors around metal-on-polyethylene surfaces have become more prevalent. Our patient presented with increased volume of the left thigh 8 years after hip arthroplasty revision surgery. Two years before the arising of the tumor in the thigh, a nodule in the inguinal region was investigated to rule out a malignant neoplastic process, but the results were inconclusive. The main preoperative complaints were pain, functional limitation and marked reduction in the range of motion of the left hip. Plain radiographs showed loosening of acetabular and femoral, and a large mass between the muscle planes was revealed through magnetic resonance imaging of the left thigh. The surgical procedure consisted of resection of the lesion and removal of the components through lateral approach. In respect of total hip arthroplasty, pseudotumors are benign neoplasms in which the bearing surface consists of metal-on-metal, but they can also occur in different tribological pairs, as presented in this case.
Keywords: Granuloma of plasma cells, Hip arthroplasty, Orthopedics
Resumo
Relatar o caso de um paciente adulto jovem que evoluiu com tumoração na coxa esquerda após 14 anos de uma cirurgia de revisão de artroplastia do quadril. Davies em 2005 descreveu esta afecção em pacientes submetidos a artroplastia de quadril com par tribológico metal–metal, mas na última década é possível achar relatos de pseudotumores em superfície metal–polietileno. O paciente iniciou queixa de aumento de volume da coxa esquerda após oito anos da cirurgia de revisão da artroplastia do quadril. Dois anos antes do aparecimento da tumoração da coxa, a investigação para descartar um processo neoplásico maligno de um nódulo em região inguinal foi inconclusiva. Suas principais queixas pré-operatórias eram dor, limitação funcional e marcada redução da amplitude de movimento do quadril esquerdo. As radiografias do membro acometido evidenciavam soltura dos componentes acetabular e femoral, e uma grande massa entre os planos musculares se revelou à ressonância magnética da coxa esquerda. A abordagem cirúrgica consistiu de ressecção intralesional da coxa esquerda, seguida da retirada dos componentes pela via lateral direta. No âmbito da cirurgia de artroplastia de quadril, os pseudotumores são neoplasias benignas cujo par tribológico consiste em metal -metal, mas podem também ocorrer em diferentes pares tribológicos, como neste caso.
Palavras-chave: Granuloma de células plasmáticas, Artroplastia de quadril, Ortopédica
Introduction
Total hip replacement is an established procedure in the context of orthopedic surgery. However, as in any surgical procedure, it is not free of complications. An uncommon complication is the appearance of pseudotumors, as cited by Panditt in 2008, which consists in the formation of structures (solid masses, cysts, nodules) in the peri-prosthetic tissues without infection or malignancy characteristics. This entity was originally associated with the metal–metal interface,1, 2, 3 but the appearance of pseudotumors has also been described in the case of metal–polyethylene4, 5, 6, 7, 8 and metal–ceramic9 interfaces. This is a very undesirable complication for both the surgeon and the patient, as it can cause severe pain, restricting the range of motion and eventually compressing neurovascular structures. In addition, it also represents a major concern in relation to the hypothesis of a possible neoplasia.
Case report
Male patient, 45 years old, former smoker with no other comorbidities, was treated by the Hip Group and the Orthopedic Oncology Group. He reported pain and progressive bulging in the medial region of the left thigh since approximately 2 years ago. At 14 years of age, the patient had a fracture of the left femoral neck and was treated with osteosynthesis and cannulated screws in another service. Four years after the surgery, at age 18, he was admitted to another hospital for the treatment of posttraumatic osteonecrosis of left femoral head. On that occasion he underwent a left total hip arthroplasty (THA), of which tribological pair consisted of a metal head and polyethylene insert, with uncemented femoral stem and uncemented acetabulum. Thirteen years after the THA, the patient suffered an automobile accident and had a periprosthetic fracture, which was treated with revision of the primary arthroplasty. An anatomical, uncemented femoral component was used, with porous coating (PCA Howmedica®), metal head and polyethylene insert. Five years after this surgery, the patient developed a nodule in the left groin area. A biopsy of the lesion had inconclusive results. Two years later, he started to feel left leg weakness and pain worsening in the inguinal region, mainly when he remained in the sitting position for more than 30 min. He also had difficulty driving because of the pain he felt when using the car clutch. The patient developed progressive hardening and increased volume of the left thigh. Venous Doppler ultrasound of the lower limbs diagnosed venous thrombosis of the left thigh. The patient was treated with full anticoagulation for 6 months, with thrombosis resolution, but the nodule in the groin persisted, which gradually increased in volume.
On physical examination, the patient was having difficulty walking, but did not need to use an orthosis. While in the supine position, the external rotation of the left leg, thigh volume increase and tumor with cystic consistency and not painful on palpation were demonstrated (Fig. 1). Upon inspection, there were no signs of inflammation, such as hyperemia and local heat or floating points on palpation. Imaging tests were performed for diagnosis clarification and treatment planning. Plain radiography of the hip and pelvis showed loosening of the acetabular and femoral components. The magnetic resonance imaging (MRI) examination of the left thigh disclosed soft tissue lesion amid the musculature of the medial thigh compartment, measuring 10 cm × 17 cm × 14 cm, with cystic areas and marked hypointense signal in all sequences (Fig. 2). The arteriography showed that the tumor was located medially to the neurovascular bundle. This, in turn, was anterolaterally displaced at the magnetic resonance imaging. Surgical treatment of the lesion was chosen, which consisted in the intralesional resection of the pseudotumor, collecting the material for infectious and anatomopathological analysis and removal of the prosthetic implant. Surgical access was initially carried out through medial access of 4 cm in length at the apex of the lesion, from anterosuperior to posteroinferior direction. Due to the presence of tumor mass that was deeper and more distal to the cystic lesion, additionally a posteroinferior and medial access measuring 5 cm performed to facilitate the emptying of the fluid material (Fig. 3).
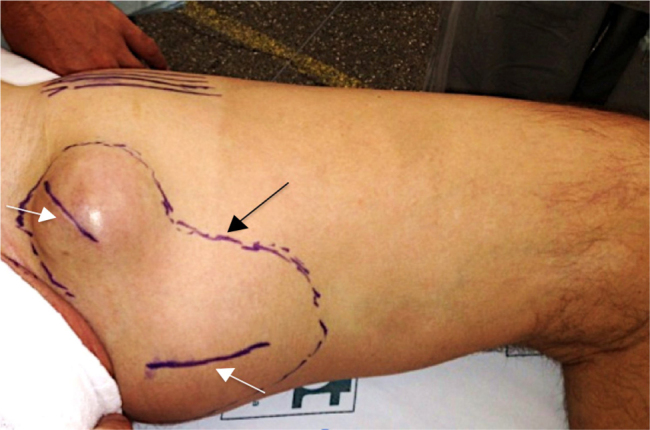
Fig. 1.

Clinical image of the left thigh anteromedial and proximal regions. Black arrow, neurovascular bundle. White arrow, tumor of cystic consistency next to the region of the left groin, with 9 cm of diameter × 5 cm height.
Fig. 2.
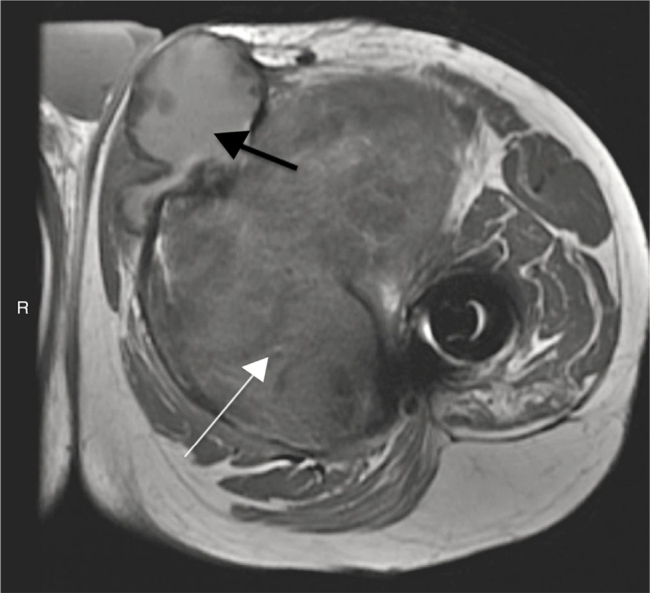
MRI axial view of the proximal region of the left thigh weighted in T1. White arrow, hyposignal and expansive formation in muscle planes in the anteromedial region of the left thigh. Black arrow, adjacent cyst with presence of fluid collection and thick content and debris inside.
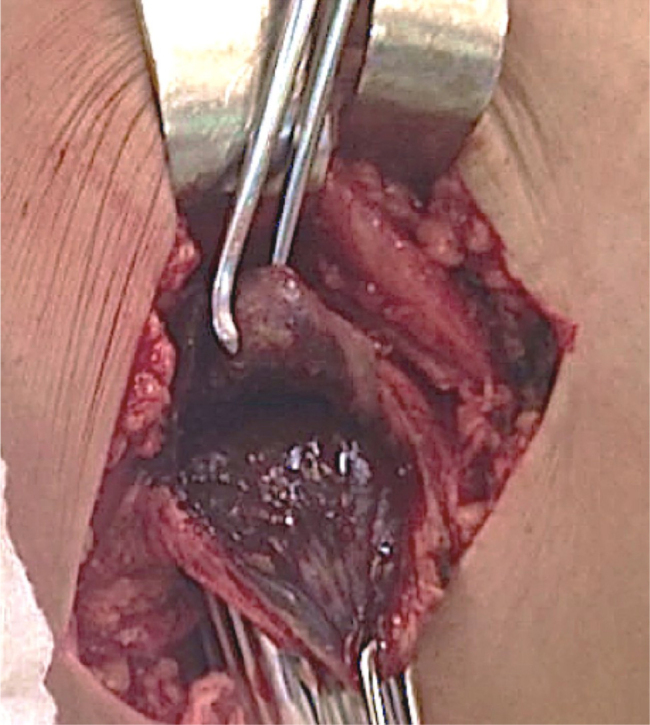
Fig. 3.
Clinical picture of the medial region of the left thigh. Black arrow, outlining of the tumor mass in the proximal region of the left thigh. White arrows, surgical planning through two medial access routes.
The patient was placed in the supine position with the aid of a cushion on the back of the left thigh. Through the two medial access routes, it was possible to achieve the emptying of a large amount of dark yellowish-green secretion, without distinctive odor or purulent aspect, with organized lumps (Fig. 4). After the emptying of the cystic contents, it was possible to identify the pseudotumor capsule with more precision (Fig. 5). This structure was preserved and its closure was carried out by approximation with spaced stitches and Mononylon 4.0™. Then, with the patient still in the supine position, the implant was removed using Hardinge's lateral approach. It was observed that the polyethylene insert was intact. Serum levels of chromium and cobalt were measured with the help of Instituto de Química da Universidade de São Paulo (Chemistry Institute of the University of São Paulo), using the graphite furnace atomic absorption spectrometry (GFAAS) technique. The cobalt level was not identified and the chrome level was 0.7 μg Cr/L (micrograms per liter), which is within the normal range. The measurement of chrome level in urine was performed at Instituto Adolfo Lutz. In the first sample, collected 1 week after implant removal, the absolute value found was 14.1 g/L. The second sample was collected 3 months after surgery, which also measured the metal ratio with urinary creatinine. The absolute value was 13.9 μg/L and the relative value of 6.7 μg Cr/g of creatinine, a slightly increased level. The patient was also submitted to the Harris Hip Score questionnaire before and after surgery, which showed an increase of nine points 2 weeks after surgery (54–63); the patient is currently asymptomatic and the surgical wound has a good aspect. The leukocyte count, ESR and CRP values are within the normal range (Fig. 4, Fig. 5).
Fig. 4.

(a) Emptying of the pseudotumor showing large amounts of dark green fluid; (b) presence of lumps of the same color without characteristic odor and (c) approximated image of lumps and liquid contents in the syringe that was sent for laboratory analysis.
Fig. 5.
Intraoperative image of pseudotumor capsule after emptying of the fluid contents. The dark aspect of its inner wall can be observed.
Discussion
Pseudotumors that occur after a total hip arthroplasty usually affect the population aged >50 years old3, 4, 5, 6, 7, 8, 9, 10, 11 and this can be partly explained by the fact that arthroplasty is performed more often in elderly individuals. In the study by Davies,12 samples of tissue around the implant were collected in patients undergoing THA revision, and this surgery is usually performed in older patients. However, pseudotumors may also occur in younger patients.13, 14
Usually, the clinical picture reported by patients consists of pain in the affected hip, particularly when walking, which shows progressive worsening and makes ambulation difficult.5, 9, 10 In some cases, symptoms can occur in more remote locations of the hip joint, which requires greater attention of the orthopedist in relation to the differential diagnosis.6, 11 A palpable mass is not always present and, in this sense, the imaging examinations are of utmost importance for the diagnosis. Hip plain radiography usually does not show signs of acetabular and femoral loosening.5, 9, 11, 15 Computed tomography of the pelvis, in turn, allows the identification of signs of pelvic osteolysis14 and cystic mass adjacent to the implant.2, 6, 11, 14 In cases where the previous tests are normal, the MRI of the operated hip can be useful.10
Laboratory analysis usually characterizes a non-infectious process with normal inflammatory markers.4, 5, 6, 9, 10, 15, 16 In case of elevated inflammatory markers,5, 11, 13 the investigation of rheumatic diseases should be considered.8 The eosinophil increase is also described, but only as a finding in the leukogram.5, 10 Lymphohistiocytic infiltrate, multinucleated giant cells and necrotic fibrous-connective tissue are common findings at the histological analysis of pseudotumor after THA.4, 6, 7, 13 The understanding of delayed hypersensitivity reactions to metal is necessary, as they characterize the immunology of these patients and can occur in several types of contact surface. Aseptic Lymphocytic Vasculitis-Associated Lesions (ALVAL) and perivascular lymphocytic infiltration (PVLI) may be histologically associated and present in arthroplasty surgeries.15, 17
When the pseudotumor is diagnosed in patients undergoing THA, there is doubt about the real need for surgical intervention. From the functional recovery point of view, assessed through questionnaires such as the Harris Hip Score and Merle D’Aubigne Postel scale, the surgical indication is beneficial.9, 14 Additionally, some pseudotumors may recur after drainage and more aggressive methods may be necessary, with no guarantee of good results.16 Conversely, the refusal to accept a revision arthroplasty of the hip due to the presence of a pseudotumor should also be considered. A decrease in volume and even the complete disappearance of the tumor mass can justify the conservative treatment.7
Conflicts of interest
The authors declare no conflicts of interest.
Footnotes
Study carried out at Instituto de Ortopedia e Traumatologia, Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo (USP), São Paulo, SP, Brazil.
References
- 1.Pandit H., Glyn-Jones S., McLardy-Smith P., Gundle R., Whitwell D., Gibbons C.L. Pseudotumours associated with metal-on-metal hip resurfacings. J Bone Joint Surg Br. 2008;90(7):847–851. doi: 10.1302/0301-620X.90B7.20213. [DOI] [PubMed] [Google Scholar]
- 2.Bisschop R., Boomsma M.F., Van Raay J.J., Tiebosch A.T., Maas M., Gerritsma C.L. High prevalence of pseudotumors in patients with a Birmingham hip resurfacing prosthesis: a prospective cohort study of one hundred and twenty-nine patients. J Bone Joint Surg Am. 2013;95(17):1554–1560. doi: 10.2106/JBJS.L.00716. [DOI] [PubMed] [Google Scholar]
- 3.Kwon Y.M., Ostlere S.J., McLardy-Smith P., Athanasou N.A., Gill H.S., Murray D.W. Asymptomatic pseudotumors after metal-on-metal hip resurfacing arthroplasty: prevalence and metal ion study. J Arthroplasty. 2011;26(4):511–518. doi: 10.1016/j.arth.2010.05.030. [DOI] [PubMed] [Google Scholar]
- 4.Lin K.H., Lo N.N. Failure of polyethylene in total hip arthroplasty presenting as a pelvic mass. J Arthroplasty. 2009;24(7):1144.e13–1144.e15. doi: 10.1016/j.arth.2008.06.029. [DOI] [PubMed] [Google Scholar]
- 5.Walsh A.J., Nikolaou V.S., Antoniou J. Inflammatory pseudotumor complicating metal-on-highly cross-linked polyethylene total hip arthroplasty. J Arthroplasty. 2012;27(2):324.e5–324.e8. doi: 10.1016/j.arth.2011.03.013. [DOI] [PubMed] [Google Scholar]
- 6.Murgatroyd S.E. Pseudotumor presenting as a pelvic mass: a complication of eccentric wear of a metal on polyethylene hip arthroplasty. J Arthroplasty. 2012;27(5):820.e1–820.e4. doi: 10.1016/j.arth.2011.09.008. [DOI] [PubMed] [Google Scholar]
- 7.Almousa S.A., Greidanus N.V., Masri B.A., Duncan C.P., Garbuz D.S. The natural history of inflammatory pseudotumors in asymptomatic patients after metal-on-metal hip arthroplasty. Clin Orthop Relat Res. 2013;471(12):3814–3821. doi: 10.1007/s11999-013-2944-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bisseling P., Tan T., Lu Z., Campbell P.A., Susante J.L. The absence of a metal-on-metal bearing does not preclude the formation of a destructive pseudotumor in the hip – a case report. Acta Orthop. 2013;84(4):437–441. doi: 10.3109/17453674.2013.823590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hsu A.R., Gross C.E., Levine B.R. Pseudotumor from modular neck corrosion after ceramic-on-polyethylene total hip arthroplasty. Am J Orthop (Belle Mead NJ) 2012;41(9):422–426. [PubMed] [Google Scholar]
- 10.Scully W.F., Teeny S.M. Pseudotumor associated with metal-on-polyethylene total hip arthroplasty. Orthopedics. 2013;36(5):e666–e670. doi: 10.3928/01477447-20130426-33. [DOI] [PubMed] [Google Scholar]
- 11.Leigh W., O’Grady P., Lawson E.M., Hung N.A., Theis J.C., Matheson J. Pelvic pseudotumor: an unusual presentation of an extra-articular granuloma in a well-fixed total hip arthroplasty. J Arthroplasty. 2008;23(6):934–938. doi: 10.1016/j.arth.2007.08.003. [DOI] [PubMed] [Google Scholar]
- 12.Davies A.P., Willert H.G., Campbell P.A., Learmonth I.D., Case C.P. An unusual lymphocytic perivascular infiltration in tissues around contemporary metal-on-metal joint replacements. J Bone Joint Surg Am. 2005;87(1):18–27. doi: 10.2106/JBJS.C.00949. [DOI] [PubMed] [Google Scholar]
- 13.Shahrdar C. Pseudotumor in large-diameter metal-on-metal total hip articulation. J Arthroplasty. 2011;26(4):665.e21–665.e23. doi: 10.1016/j.arth.2010.05.022. [DOI] [PubMed] [Google Scholar]
- 14.Bourghli A., Fabre T., Tramond P., Durandeau A. Total hip replacement pseudotumoral osteolysis. Orthop Traumatol Surg Res. 2010;96(3):319–322. doi: 10.1016/j.otsr.2009.11.013. [DOI] [PubMed] [Google Scholar]
- 15.Mao X., Tay G.H., Godbolt D.B., Crawford R.W. Pseudotumor in a well-fixed metal-on-polyethylene uncemented hip arthroplasty. J Arthroplasty. 2012;27(3):493.e13–493.e17. doi: 10.1016/j.arth.2011.07.015. [DOI] [PubMed] [Google Scholar]
- 16.Lee J.H., Le V.H., Steinhoff A., Hoang B.H. Vascular tumor in metal-on-polyethylene THA requiring hemipelvectomy. Orthopedics. 2013;36(7):e974–e977. doi: 10.3928/01477447-20130624-32. [DOI] [PubMed] [Google Scholar]
- 17.Ng V.Y., Lombardi A.V., Jr., Berend K.R., Skeels M.D., Adams J.B. Perivascular lymphocytic infiltration is not limited to metal-on-metal bearings. Clin Orthop Relat Res. 2011;469(2):523–529. doi: 10.1007/s11999-010-1570-7. [DOI] [PMC free article] [PubMed] [Google Scholar]