

Abstract
Objectives
While early onset of puberty among girls has been related to substance use involvement and other adverse outcomes, less research has examined pubertal development and outcomes in boys. Further, research on puberty has not been conducted in the context of other risk factors for substance use involvement such as impulsivity. To address these gaps, this study characterized boys' pubertal development from preadolescence to mid-adolescence and related it to substance use risk and behavioral impulsivity.
Methods
A sample of 153 boys completed the Pubertal Development Scale to assess perception of their pubertal development relative to same age peers from ages 10 to 16 years, at 6-month intervals. Group-based trajectory modeling identified three distinct patterns of pubertal development: boys with more slowly developing boys with either earlier (n = 54) or later (n = 43) pubertal timing, and boys with faster tempo of pubertal development (n = 56). The groups were compared on demographic and substance use risk characteristics, as well as behavioral measures of impulsivity.
Results
Boys who had the accelerated progression through puberty had the highest proportion of family histories of substance use disorder and perform more impulsively on reward choice measures.
Conclusions
Outcomes are consistent within the Maturation Compression Hypothesis and social neuroscience models of adolescent developmental risk.
Keywords: puberty, maturation compression, adolescence, impulsivity, family history of substance use disorder
Introduction
Individual differences in the timing of pubertal maturation have been linked to delinquent and externalizing behaviors including substance use involvement. However, the precise nature of this association remains unclear. There is evidence suggesting adverse outcomes are associated with at least two types of variation from typical pubertal maturation: (1) the timing of puberty onset; or (2) the tempo of puberty changes over time. Of these two domains, pubertal timing has received much more attention. The Developmental Stage Termination hypothesis suggests that early onset of pubertal development increases risk for adverse outcomes like problem substance use (Petersen and Taylor, 1980). According to this theory, early pubertal timing is problematic because physical changes precede psychological development that is necessary for adjusting to changes that come with puberty. As a result, those who mature early may be ill-prepared to cope with changes to their social environment and expectations of others, leading to participation in delinquency and/or substance use involvement (Brooks-Gunn et al., 1985; Caspi and Moffitt, 1991; Peterson and Taylor, 1980). Alternatively, the Maturation Compression Hypothesis holds that unusually rapid transition through puberty, rather than earlier onset, is what accounts for disruption of social emotional adjustment, thereby increasing propensity to externalizing behavior (Mendle et al., 2010). While each of these theories focuses on different aspects of variation in pubertal timing, they are similar in positing that that atypical pubertal development (either early or rapidly changing) results in disruption of one's social environment, stress, and problem behaviors.
While there is a large literature on puberty and its relationship to adverse outcomes, this research has generally focused on early puberty onset among girls and been conducted using cross-sectional methods (Mendle et al., 2010). There are reasons to expect gender differences; given that the criteria used to rate girls' and boys' puberty are different and girls are about 1.5 years ahead of boys in pubertal development (Petersen et al., 1988). While cross-sectional methods are faster and less costly than prospective designs, they may lead to different outcomes than might be observed longitudinally. For instance, cross-sectional approaches are capable of identifying early puberty onset for tests of the Developmental Stage Termination, but not as effective in reliably quantifying change in pubertal development across time for testing the Maturation Compression Hypothesis. This focus on cross-sectional methods may be biasing our understanding of the relationships of puberty with adverse outcomes, such as substance use risk, because of the potential for interacting with sex differences. For example, one recent report (Marceau et al., in press) suggests that, had only early onset of puberty been considered, it would appear that there is a less consistent relationship between puberty and changes in parent-child conflict and closeness for boys than for girls. However, significant relationships were observed for boys when the tempo of changes in pubertal development across time was considered (Marceau et al., in press). Building on this approach, the current study examined change in pubertal development among boys and in relation to risk factors for substance use involvement.
Many of the negative outcomes associated with altered pubertal timing and tempo occur in mid- to late-adolescence, but risk factors for these problems are evident even in preadolescence prior to any substance use. Impulsivity is one of the risk factors for subsequent substance use involvement that is measurable early in puberty prior to initiation of use. Impulsivity has been defined as “a predisposition toward rapid, unplanned reactions to internal or external stimuli without regard to the negative consequences of these reactions to the impulsive individual or to others” (Moeller et al., 2001, p. 1784). Since 2000, there has been an exponential increase in the number of publications examining the role of impulsive behaviors in various aspects of substance misuse. For instance, behavioral impulsivity is not only increased among populations with long-term, chronic patterns of substance dependence (Bjork et al., 2004; Duka et al., 2003; Moeller et al., 2004; Rubio et al., 2008), but also following short-term, regular use (Dougherty et al., 2013), acutely during intoxication (Dougherty et al., 2008; Fillmore et al., 2001; Reynolds et al., 2006), and even prior to substance use initiation, among those at increased risk due to family histories of substance use disorder (Acheson et al., 2011; Dougherty et al., 2014). Within this literature there are distinctions between reward choice and rapid decision impulsivity (Dougherty et al., 2005a; Dougherty et al., 2009). Of these distinct classes of measures, there have generally been more consistent relationships of reward choice impulsivity with substance use outcomes and risks. While there is broad support identifying relationships of substance use and substance use risk with increased impulsivity, these relationships have not been tested in the context the individual differences in pubertal maturation described by Developmental Stage Termination model or the Maturation Compression Hypothesis. The research on puberty and behavioral impulsivity are separate literatures and there is a lack of data on how they relate to one another.
The purpose of this study was to characterize boys' impulsive behavior and substance use risk within the context of prospective pubertal development. Puberty, substance use risk, and impulsivity were measured at an initial assessment occurring between ages 10-12 years and repeated at 6-month intervals prospectively. Pubertal development was characterized using group-based trajectory modeling of boys' responses on the Pubertal Development Scale (Petersen et al., 1988) and behavioral impulsivity was tested with reward choice and rapid decision measures among boys at high risk for substance use involvement due to family history of substance use disorder and healthy controls. This study extends the literature by: testing whether there is evidence for a compressed pubertal maturation subgroup during this age range for boys; and comparing substance use risk and behavioral impulsivity by pubertal developmental trajectories. We were interested in determining: (1) whether a compressed pubertal trajectory could be differentiated from early pubertal maturation; and (2) if there were distinct trajectories of earlier and compressed maturing boys, do these two patterns of pubertal maturation differ on reward choice and/or rapid decision impulsive behavior and/or risk of substance use involvement.
Materials and Methods
Participants
Participants were 153 boys recruited as part of a broader study of prospective development of substance use involvement. These boys were a mixed group from families with (n = 121) or without (n = 32) history of substance use disorder in their parents and grandparents who were recruited to participate in the larger study using online and radio advertisements. Boys with both types of family histories were included to have a broad range of risk and prospective patterns of substance use. The current study's participants selected from the larger cohort (187 boys described in Ryan et al., in press) if they had at least three pubertal development assessments so that their pubertal trajectory could be estimated. There were no significant differences between boys who were (n = 153) selected or not selected (n = 34) on demographic characteristics of age (p = .78), verbal IQ (p = .92), ethnicity (p = .26), race (p = .56), or initial pubertal score (p = .73).
Procedure
Each boy and a parent/guardian were first screened for eligibility; measures of puberty, impulsive behavior, and substance use were then obtained prospectively at approximately 6-month intervals (median number of visits = 6; maximum = 8 visits). All study procedures were reviewed and approved by our Institutional Review Board and all participants provided written informed consent. Boys were compensated $75 for the screening, which took approximately 5 hours to complete, and then $120 for baseline and subsequent follow-up visits.
Screening
Inclusion criteria were: children ages 10-12 years, physically healthy (medical history and exam by a physician or physician's assistant), and having at least a father with a substance use disorder for the boys with family history of substance use disorder. Exclusionary criteria included: youth who had already initiated regular substance use at study entry (≥1 per month for six consecutive months; Clark et al., 2005), low intelligence (IQ < 70; Wechsler Abbreviated Intelligence Scale; the Psychological Corporation, 1999), and psychiatric disorders other than Oppositional Defiant Disorder, Conduct Disorder, Attention Deficit Hyperactivity Disorder (ADHD), Dysthymia, or Anxiety Disorders (Kiddie and Young Adult Schizophrenia and Affective Disorders Schedule, Present State and Lifetime: Kaufman et al., 1997). These disorders were not exclusionary because previous research (e.g., Iacono et al., 2008) has demonstrated that they frequently co-occur with substance misuse.
Pubertal Development
Pubertal status and change in puberty over time was measured using the Pubertal Development Scale (PDS; Petersen et al., 1988). Boys completed this 5-item questionnaire that queries about changes in body hair, facial hair, voice, skin, and growth spurt. Each item is rated on a 4-point scale describing each pubertal process as: 1 = not yet started, 2 = barely started, 3 = definitely underway, or 4 = completed. Scores from the 5 items are summed to yield a total score, which is the dependent variable used in this study. Puberty categories were also computed based on the Carskadon & Acebo (1993) methodology (i.e. categories of Prepubertal, Early Pubertal, Midpubertal, Late Pubertal, and Postpubertal). Previous research has reported that the PDS has established reliability (median Cronbach's α = .77) and validity (e.g., median correlation .70 with pubertal interviewer ratings; Petersen et al., 1988).
Besides direct measurement of puberty, height and weight was also assessed as a measure of physical development. A physician assistant measured height and weight of boys at each visit (Detecto Weigh Beam Eye-Level scale; Detecto, Webb City, MO). From these measures, pediatric Body Mass Index (BMI) was calculated [weight lbs/(Height in)2)*703] (Centers for Disease Control and Prevention, 2014). These observed height and weight were compared to age-adjusted national norms (i.e., CDC Growth Charts for the United States; National Center for Health Statistics, 2000).
Substance Use
A range of substance use characteristics were assessed. Family history of substance use disorder was assessed using the Family History Assessment Module (Rice et al., 1995). This instrument was also used to collect information to calculate the number of biological parents and grandparents meeting criteria for substance use disorders (i.e. Family Density). In addition to the family histories of substance use, the boys own substance use was assessed using interview of the child (Drug History Questionnaire; Dougherty et al., 2013). This information was coupled with a breath alcohol test (AlcoTest® 7110 MKIII C device; Draeger Safety Inc., Durango, CO) and urine-drug test (Panel/Dip Drugs of Abuse Testing Device; Redwood Biotech, Santa Rosa, CA) in determining recent use.
Impulsive Performance
Because impulsivity is a complex set of process, requiring multiple modes of assessment (de Wit, 2009; Evenden, 1999; Winstanley et al., 2006), this study examined performance across three measures: consequence sensitivity, response initiation, and response inhibition. Consequence sensitivity is a reward choice measure that describes showing relatively greater preference for smaller rewards that are available sooner rather than larger rewards later. Response initiation is a rapid response measure that reflects rash, inaccurate responding to environment stimuli prior to completion of information processing. Finally, response inhibition is a rapid response measure that describes the failure to withhold responding based on feedback from the environment. These three processes have been described together in a model of impulsivity (Dougherty et al., 2005a; Dougherty et al., 2009). While this model has been applied for studying risk for substance use involvement (e.g. Acheson et al., 2011; Dougherty et al., 2014), but it has not been tested in the context of variation in pubertal maturation.
Two Choice Impulsivity Paradigm (TCIP)
The TCIP is a measure of consequence sensitivity and requires 50 discrete choices between smaller-more-immediate rewards and larger-more-delayed rewards (Dougherty et al., 2005b). In this computerized task, boys made choices between circles associated with a 5 cent reward that could be earned after a delay of 5 seconds and squares associated with a 15 cent reward after a 15 second delay. The dependent variable for this task was the proportion of responses for the smaller-more-immediate rewards (i.e., TCIP Proportion Short; Dougherty et al., 2005b).
Immediate Memory Task (IMT)
The IMT is a measure of response initiation by assessing ability to withhold responding to rapidly presented 5-digit stimuli that are very similar to target stimuli (Dougherty et al., 2002). In this computerized task, boys were instructed respond to target cues (consecutive matching numbers) and avoid responding to non-targets. Some of the non-target stimuli are very similar to the target, matching on 4 of 5 digits. The proportion of responses to these similar non-targets relative to target responding is referred to as the IMT Ratio and is the primary dependent measure of impulsivity for this instrument.
GoStop Impulsivity Paradigm (GoStop)
The GoStop (Dougherty et al., 2005b) is a measure of response inhibition by assessing the failure to inhibit an already initiated response. In this computerized task, the boys were instructed to respond to targeted “go” (black consecutive matching numbers), but withhold responding to “stop” cues (consecutive matching number that turns from black to red) that are rapidly displayed on a computer monitor. The proportion of responses to the trials with a stop cue relative to the go cue is referred to as the GoStop Ratio and is the primary dependent measure of impulsivity for this instrument (e.g., Dougherty et al., 2008).
Data Analysis
First, to identify distinct patterns of pubertal development, a specialized form of finite mixture modeling called group-based trajectory modeling (Nagin and Odgers, 2010) was used to examine patterns of PDS Total scores across time. Because the PDS Total scores ranged from 5 to 20, the censored normal distribution was used for modeling the data. Various trajectory models with 2, 3, or 4 groups and up to a 5th order polynomial function of age (in month) were fitted. The 3-group model was selected because it optimized simplicity and minimized model fit indices including Bayesian Information Criteria (BIC; Raftery, 1995, Schwartz, 1978), Akaike Information Criterion (AIC; Akaike, 1998), and entropy (Nagin & Odgers, 2010). Based on the outcomes of the 3-group model, each of the boys was assigned a nominal code representing the one of three possible pubertal trajectories they fit (1 = Earlier, 2 = Compressed, and 3 =Later) using the posterior probabilities and the maximum probability group assignment rule. The diagnostic performance of the selected 3-group model was tested as recommend (Nagin 2005, Nagin & Odgers, 2010). Specifically, the average of the posterior probability of group membership for boys assigned to each group was 0.88; the odds of correct classification for each group was greater than 9 for all groups; observing reasonably right confidences intervals around estimated group membership probabilities; as well as the correspondence between the model predicted class membership proportions (28.6%, 35.2%, and 36.2%) and the actual sample class membership proportions based on highest posterior probability assignment (28.1%, 35.3%, and 36.6%) was adequately close. Subsequent group-based comparisons were conducted based on this pubertal trajectory coding.
Once pubertal trajectory groups were identified, they were compared on several additional measures of puberty and body size to corroborate that the groups indeed differed on indicators of pubertal status. PDS Total at study entry, height, weight, and BMI were separately compared using univariate analyses of covariance (ANCOVA) with age at study entry as a covariate and group as the dependent variable. Pubertal Stage and self-perceived pubertal timing was compared using chi-square analyses. Following these additional comparisons of puberty, the three pubertal trajectory groups were compared on tests of demographic characteristics using chi-square analyses for categorical variables and ANOVA for continuous variables.
Differences in behavioral impulsivity performance across the three pubertal trajectory groups were examined in two ways: cross-sectionally from tests conducted at study entry, and longitudinally from tests collected at each prospective visit. The cross-sectional analyses were conducted using ANCOVA. Separate ANCOVAs were tested for the TCIP, IMT, and GoStop with each impulsivity measure as the dependent variable. Both pubertal trajectory group and family history of substance use disorder were included as the independent variables. Because the three pubertal trajectory groups differed in Verbal IQ at study entry, this variable was included as the covariate.
Finally, behavioral impulsivity was compared longitudinally. For each of the three types of impulsivity, separate mixed-effects models with both a random intercept and a random slope were used to examine the effect of pubertal trajectory groups on the longitudinal trajectory of change in impulsivity for each participant. The fully adjusted model included age at study entry, Verbal IQ, time of measurement, and pubertal group as the explanatory variables and continuous impulsivity scores as the response variables. The interaction between pubertal groups and time of measurement was also examined but was not significant, therefore not included in the final model.
Pubertal characteristics, demographic characteristics, substance use characteristics, and impulsive performance measured at study entry were conducted using SPSS version 21 (IBM Corp. Armonk, NY). Group-based trajectory modeling was conducted using Stata (version 13, StataCorp; College Station, TX). Mixed-effect modeling was conducted using SAS (version 9.3, SAS Institute Inc., Cary, NC).
Results
Group-Based Trajectory Modeling of Puberty
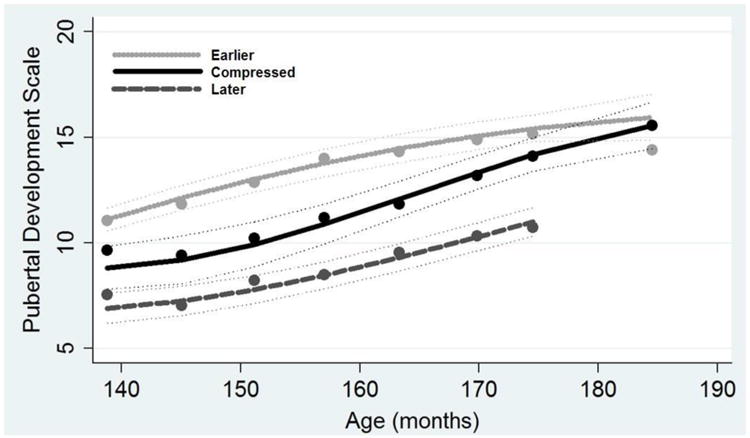
The trajectory modeling resulted in identification of 3 distinct groups of boys differing in their pubertal development over time: Earlier, Compressed, and Later (see Figure 1 for PDS Total scores by group). The Earlier group (n = 54; 35.3% of the sample) had the highest overall Pubertal Development Scale (PDS)scores both at study entry and prospectively, which was indicative of pubertal development starting at a younger age than the other groups. The Later group (n = 43; 28.1% of the sample) had the overall lowest scores on the PDS, and these low PDS scores gradually increased at a tempo similar to the Earlier group. Finally, the Compressed group (n = 56; 36.6% of the sample) started the study with PDS scores between the Earlier and Later groups, but had the largest increases in puberty over time (82% increase compared to 45% for Earlier and 43% for Later groups). This more rapid pattern change in PDS Total scores over time among the Compressed group is consistent with risky pattern described by the Maturation Compression Hypothesis (Mendle et al., 2010).
Figure 1. Group-Based Trajectory Modeling of Pubertal Development Scale Scores over Time.
Comparisons of Pubertal Development across Trajectory Groups
Further analyses were conducted to confirm that the 3 pubertal trajectory groups derived from our analyses were in fact distinct in their pubertal development. In other words, these tests were conducted to verify the effectiveness of the group-based trajectory modeling in identifying distinct types of pubertal development.
First, PDS Total score was examined at study entry. There was a significant difference between all three groups in terms of PDS score (Earlier> Compressed> Later;ANCOVA F2,149 = 27.482, p< .001; see top panel, Table 1). Next, groups were compared in terms of PDS Pubertal Stages (bottom panel, Table 1). The three groups were significantly different in Pubertal Stage at study entry (χ2 = 36.828, p< .001; see bottom panel, Table 1). The Earlier group was more likely to enter the study at the Midpubertal stage than the Compressed (p< .001) and Late (p< .001) groups. There was a trend for the Later group to be more likely to start at the Prepubertal stage than the Compressed group (p = .067). There were also significant group differences in the boys' perception of their pubertal development relative to their peers (χ2 = 17.135, p = .002). The Earlier group was significantly more likely to rate their own development as occurring earlier than their peers when compared to ratings of boys in the Later (Fishers Exact p = .003) and Compressed (Fishers Exact p< .001) groups, which did not differ from each other (p = .695).
Table 1. Pubertal Characteristics.
| Characteristics | Pubertal Maturation Groups | p | Contrast | |||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Earlier E n = 54 |
Compressed C n = 56 |
Later L n = 43 |
||||||
|
|
|
|
||||||
| Mean | (SD) | Mean | (SD) | Mean | (SD) | |||
| Puberty, PDS Total | 11.11 | (2.6) | 9.51 | (2.5) | 7.61 | (1.9) | < .001 | E>C>L |
| Weight, lbs | 111.17 | (39.6) | 99.30 | (24.1) | 89.76 | (31.0) | .004 | E>C,L |
| Weight, % Expected | 35.96 | (47.4) | 21.36 | (29.2) | 8.38 | (32.5) | .002 | E>C,L |
| Height, in | 59.56 | (4.1) | 57.28 | (3.3) | 56.10 | (3.9) | < .001 | E>C>L |
| Height, % Expected | 4.14 | (5.6) | 0.00 | (4.5) | -2.30 | (5.7) | < .001 | E>C>L |
| BMI | 21.83 | (6.6) | 21.16 | (4.3) | 19.62 | (4.4) | .120 | |
| BMI, % Expected | 24.43 | (38.3) | 20.78 | (25.1) | 11.91 | (23.7) | .121 | |
| Number | (%) | Number | (%) | Number | (%) | p | ||
|
| ||||||||
| Pubertal Stage | < .001 | a L>C>E | ||||||
| Prepubertal | 5 | (9.3) | 7 | (12.5) | 15 | (34.9) | ||
| Early Pubertal | 7 | (12.9) | 24 | (42.8) | 19 | (44.2) | ||
| Midpubertal | 37 | (68.5) | 22 | (39.3) | 9 | (20.9) | ||
| Late Pubertal | 5 | (9.3) | 3 | (5.4) | 0 | (0.0) | ||
| Perceived Pubertal Timing | ||||||||
| Earlier | 22 | (40.7) | 10 | (17.8) | 8 | (18.6) | .002 | b E>C,L |
| On-Time | 27 | (50.0) | 24 | (42.9) | 21 | (48.8) | ||
| Later | 5 | (9.3) | 22 | (39.3) | 14 | (32.6) | ||
% Expected = percent difference from age-adjusted 50 percentile expected size for boys based on National Center for Health Statistics, 2000; BMI = body mass index; in = inches; lbs = pounds; PDS = Pubertal Development Scale.
Group comparison ranked by proportion of sample in each Pubertal Stage (i.e. the Earlier group has significantly higher proportion of the sample in the Midpubertal stage than Early or Compressed groups).
Group comparison ranked by proportion of the sample that perceive their puberty is occurring earlier than their peers (i.e. Group 2 has significantly higher proportion of the sample rating earlier onsets than peers).
The three groups also differed in body size, which is associated with pubertal changes (see top panel, Table 1). On average, boys in the Earlier group were heavier and taller than boys in both the Compressed and Later groups. The Compressed boys were taller, but not heavier than the Later group. This same pattern of group differences was observed for comparisons based on percent difference between observed and expected height and weight (based on national norms).
The pattern of outcomes, tested from this variety of different perspectives, supports the interpretation that three distinct puberty trajectories were identified by the modeling procedure.
Demographic Characteristics of Trajectory Groups
Besides pubertal characteristics, the three groups were also compared on general demographic characteristics (see Table 2). The purpose of this comparison was to identify any demographic characteristics that systematically differed by pubertal trajectory group, which may explain any group differences in impulsive performance. On average across all participants, boys were about 11.44 years of age at study entry, of average intelligence (M = 97.05, SD = 12.2), and predominantly Hispanic ethnicity and White race. The three pubertal trajectory groups differed in Verbal IQ. Although average IQ for the three groups was within the average range (i.e., 90-109, The Psychological Corporation, 1999), boys in the Earlier group had significantly higher Verbal IQ than those in the Later and Compressed groups, who were not different than one another. There were no group differences in terms of age at study entry, Performance IQ, ethnicity, race, or prevalence of psychiatric diagnoses.
Table 2. Demographic Characteristics.
| Characteristics | Pubertal Maturation Groups | p | Contrast | |||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Earlier E
n = 54 |
Compressed C n = 56 |
Later L n = 43 |
||||||
|
|
|
|
||||||
| Mean | (SD) | Mean | (SD) | Mean | (SD) | |||
| Age at Study Entry | 11.51 | (0.9) | 11.42 | (0.8) | 11.37 | (0.9) | .711 | |
| Verbal IQ | 100.20 | (12.8) | 93.30 | (11.6) | 92.51 | (15.3) | .006 | E>C,L |
| Performance IQ | 100.91 | (12.1) | 95.05 | (10.6) | 94.79 | (13.3) | .252 | |
| Family SUD Density | 1.85 | (1.7) | 2.36 | (1.4) | 1.95 | (1.6) | .196 | |
| Age of First Substance Use | 14.03 | (0.9) | 13.47 | (1.2) | 13.73 | (1.8) | .508 | |
| Number | (%) | Number | (%) | Number | (%) | p | ||
|
| ||||||||
| Family History of SUD | 37 | (68.5) | 50 | (89.3) | 34 | (79.1) | .028 | C>L |
| Substance Use, any | 13 | (24.1) | 14 | (25.0) | 9 | (20.9) | .888 | |
| Ethnicity, Hispanic | 28 | (65.1) | 43 | (79.6) | 46 | (82.1) | .112 | |
| Race, White | 34 | (79.1) | 49 | (90.7) | 58 | (85.7) | .266 | |
| Psychiatric Diagnosis | ||||||||
| ADHD | 16 | (37.2) | 13 | (24.1) | 17 | (30.4) | .374 | |
| Anxiety | 5 | (11.6) | 4 | (7.4) | 8 | (14.3) | .513 | |
| Depression | 1 | (2.3) | 3 | (5.5) | 1 | (1.7) | .496 | |
| ODD | 5 | (11.6) | 1 | (1.8) | 8 | (14.3) | .062 | |
ADHD = Attention Deficit Hyperactivity Disorder; ODD = Oppositional Defiant Disorder; SUD = Substance Use Disorder
There were significant differences by pubertal group on some of the substance histories. For instance, there was a significant group difference in the proportion of boys with family histories of substance use disorder (χ2 = 7.168, p = .028); there was a relatively higher proportion of boys in the Compressed group with a family history of substance use disorder than in the Earlier group (p = .007). The proportion with family histories was not significantly different between the Compressed and Later groups (p = .160). In examining the substance use among the boys themselves, the groups did not differ in the proportion of boys who had tried substances, although they differed on the number of substances they had used. A majority of the boys in the Later group with substance use reported using only a single type of substance (n = 7 of 9), while most of Earlier (n = 10 of 14; Fisher's Exact p = .036) and Compressed (n = 12 of 16; Fisher's Exact p = .011) users reported more than one type of substance used. Marijuana was the most prevalent of the substances used (n = 29), followed by alcohol (n = 25), and tobacco (n = 19). Finally, there was no significant between group difference in age at first substance use.
Impulsive Performance
Cross Sectional Assessment at Study Entry
There were significant group differences in impulsive performance and this effect was specific to the measure of reward choice (i.e., TCIP: see Figure 2; left column). Specifically, there was a significant puberty group difference in consequence sensitivity impulsivity (TCIP proportion short; ANCOVA F2,148 = 6.745, p = .002). The Compressed group showed significantly greater preference for the impulsive, smaller-sooner choices than Earlier or Later groups (p values = .001 and .012, respectively). This pubertal group difference in consequence sensitivity was further tested in the context of demographic characteristics: there was no significant interaction or main effect of family history of substance use disorder, boys' substance use, or boys' psychiatric comorbidity.
Figure 2. Baseline and Prospective Comparisons of Impulsive Performance among Youth from three Pubertal Trajectory Class Groups.
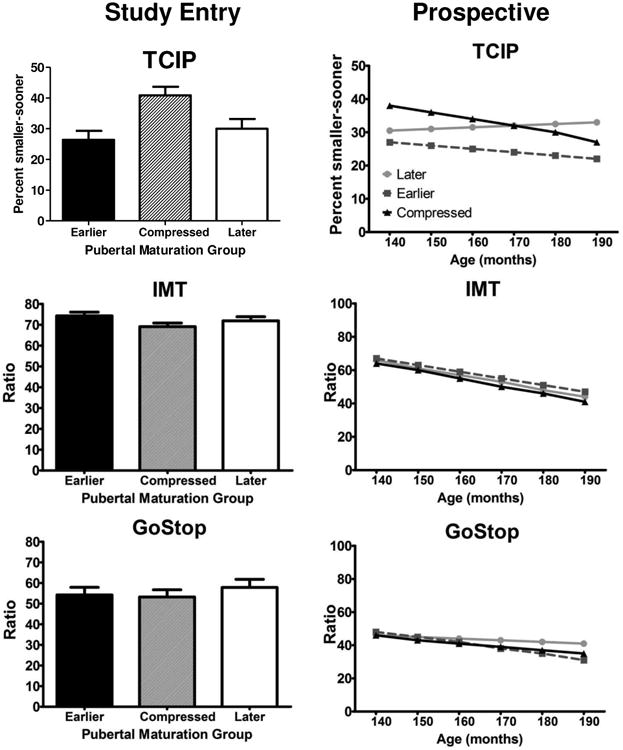
There were no significant differences between puberty and/or family history groups in terms of performance on the rapid decision measures of response initiation impulsivity (IMT Ratio; ANCOVA F2,145 = 2.135, p = .122) or response inhibition (GoStop Ratio: ANCOVA F2,144 = 0.109, p = .665).
Prospective Comparisons
Not only did the Compressed group have a greater preference for TCIP smaller-sooner choices at study entry, these group differences persisted prospectively (see Figure 2; right column). There were significant group differences in the proportion of smaller-sooner choices on the TCIP over time (p = .038). On average, the Compressed group had significantly more impulsive responses than the Earlier group (25% difference; p = .013), but this difference was only at trend levels when compared to performance of Later group (17.6% difference; p = .094). Exploratory analyses failed to reveal any significant pubertal trajectory group difference in consequence sensitivity at study entry that interacted with family history of substance use disorder (p = .420) or boys' substance use (p = 0.706). Finally, there was no significant puberty or family history group effects for prospective comparisons of rapid response measures of the IMT Ratio or GoStop Ratio.
Discussion
This study identified three distinct patterns of pubertal development among boys between the ages of 10 and 16 years of age: Earlier, Compressed, and Later maturing. The Developmental Stage Termination would predict that those maturing early would be more likely to have difficulties; however, in this study it was the faster maturing group that had more substance use risk (i.e., family history of substances use disorder) and reward choice impulsivity. Identification of significant relationships with faster maturing puberty is consistent with the Maturation Compression Hypothesis and extends this literature by examining its relationship with behavioral impulsivity.
Puberty group differences in impulsivity were not constant across the three types of impulsivity measures. The Compressed group performed significantly more impulsively than the Earlier group on the reward choice measure of consequence sensitivity impulsivity but not on rapid response measures of response initiation or inhibition. The selective nature of performance differences, apparent on some tasks but not others, is consistent with conceptualization of impulsive performance in general. Previous research and theory has identified how consequence sensitivity represents a distinct process from response initiation or inhibition (Dougherty et al., 2003; Dougherty et al., 2005a; Lane et al., 2003). Not only is performance across these different measurement approaches not highly correlated, but they are differentially related to outcomes. Rapid response impulsivity tasks have shown larger effects in differentiating performance between individuals with psychiatric conditions like childhood disruptive behavior disorders from healthy controls (e.g., Dougherty et al., 2003), while reward choice impulsivity tasks have demonstrated larger effects in relationship to substance use and substance use risk (Hamilton et al., 2015). For example, previous research has demonstrated relatively larger effects of consequence sensitivity than response initiation and/or inhibition when comparing performance of healthy controls with adolescents who frequently use marijuana (Dougherty et al., 2013), adults who have binge drinking patterns of alcohol use (Sanchez-Roige et al., 2014), and following acute alcohol consumption among young adults who drink and drive (McCarthy et al., 2012). Not only are individual differences in reward choice impulsivity systematically related to substance use, but this study found them to be associated with variation in pubertal maturation as well.
There is a biological basis for the observed relationship between puberty and consequence sensitivity. Social neuroscience theory describes pubertal development and changes in different aspects of impulsive behavior through childhood and adolescence. From this perspective, impulse choice for reward processes, like those measured with the Two Choice Impulsivity Paradigm, are expected to be more strongly associated with puberty than rapid response measures and this relationship is attributed to changes in dopamine activity that occur with puberty (Smith et al., 2013; Steinberg, 2008). Alternatively, impulse control on processes like response initiation and inhibition more gradually develops later in adolescence and appears associated with age rather than pubertal timing (Steinberg, 2008). The asynchrony of these reward-seeking and impulse control processes is what accounts for the heightened risk for engaging in appetitive behavior that that also carries with it the potential for negative, maladaptive consequences (Geier, 2013). The current findings of pubertal group differences in consequence sensitivity during early adolescence are consistent with this social neuroscience conceptualization.
Identification of differences between the Earlier and Compressed trajectories of pubertal timing supports the need to account not just for timing of puberty onset but also tempo of change in puberty over time. Much of the puberty literature has only focused on early onset of puberty among girls as related to adverse outcomes, because the majority of this literature is based on cross-sectional study design. Although this approach allows for identification of early variation in pubertal timing, it is not reliable in quantifying the tempo of changes in puberty over time. When studies have used repeated puberty assessments prospectively, they have found that onset (i.e., timing) and change in puberty (i.e., tempo) over time: (1) are not strongly correlated; (2) are the result of distinct etiology; and (3) are differentially related to substance use involvement by mid- to late- adolescence (Castellanos-Ryan et al., 2013). The current study extended the approach of Mendle and colleagues (2010) by using statistical analyses of prospective assessments of puberty to identify distinct patterns of early timing and faster tempo of puberty in relation to impulsive behavior. By evaluating tempo of puberty changes, a group of boys was identified with relatively faster (i.e., compressed) pubertal development. While the Compressed group was similar to the Earlier group's PDS Total at the conclusion of the study, they were significantly lower in puberty scores than the Earlier group at study entry. This outcome highlights the challenges of cross sectional assay of puberty. Had puberty been only assessed at the end of the study, both Compressed and Earlier groups would appear to be a single group, even though through repeated assessment we know them to have different rates of pubertal development over the course of early to mid-adolescence. The identification of both Earlier and Compressed pubertal groups allows for interpretations and contrasts to be drawn about impulsive performance and substance use risk from perspectives of both Developmental Stage Termination and Maturation Compression Hypotheses.
Although this study represents a novel application of behavioral impulsivity testing, there have been a few studies examining personality dimensions of impulsiveness and related personality traits (i.e., sensation seeking). A large (N =871; Castellanos-Ryan et al., 2013) study of boys in Montreal found that self-reported sensation seeking, but not impulsiveness, was weakly (r < .2) but significantly related with timing of puberty onset at 11-13 years of age. The tempo of puberty changes was not related to impulsiveness or sensation seeking. Further, sensation-seeking mediated the relationship of pubertal status at age 12 and substance use outcomes at ages 15-16 (relationships with puberty tempo were not significant). In the current study with a younger group of boys, there was no significant interaction of puberty with behavioral impulsivity in relationship to family history of substance use.
While this study provides a novel test of pubertal development, behavioral impulsivity, and substance use risk, its outcomes must be interpreted in context of its limitations. The logistical and time constraints introduced by inclusion of the prospective laboratory-based impulsivity assessment resulted in more modest sample size than epidemiological studies of puberty. Additionally, the sample was intentionally limited to boys because they typically have been under-represented in this area of the literature and differences in pubertal assessment between boys and girls make direct comparison between them difficult. Finally, the puberty assessment relied exclusively on self-report and where not confirmed by clinical evaluation (e.g., Marshall and Tanner, 1970) or other endocrine assay. The instrument used for assessing puberty (i.e., PDS) was designed to assess somatic pubertal changes rather than underlying endocrine changes, which may have different relationships with outcomes and risk factors (Petersen et al., 1988). Adding this biological component will be important for future research in advancing understanding of pubertal timing and tempo relationships with behavioral impulsivity. Finally, we did not include a reference group that would allow identification of normative pubertal changes and were not able to identify age-based norms on the PDS in prior literature. Therefore, we cannot be sure how our Earlier, Compressed, and Later designations compare to average or “typical” pubertal development in this age range.
Conclusions
This study builds on literature examining relationships of age of onset and tempo of pubertal development in relation to outcomes by testing for differences in impulsive performance as a potential mechanism of substance use risk. Consistent with the Maturation Compression Hypothesis those who had the accelerated progression through puberty had the highest proportion of family histories of substance use disorder and highest consequence sensitivity impulsivity. The systematic relationship of pubertal changes during this age range is consistent with the social neuroscience conceptualization with development and reward seeking behaviors.
Acknowledgments
Research reported in this publication was supported by the National Institutes of Health under award numbers R01 DA026868; R01 DA033997; R01 MH081181; and T32 DA031115. The content is solely the view of the authors and does not necessarily represent the official view of the National Institutes of Health. Dr. Donald M. Dougherty also gratefully acknowledges support from a research endowment, the William and Marguerite Wurzbach Distinguished Professor.
We gratefully acknowledge the technical contributions of Philip Brink, Cynthia Cornejo, Allison Ford, Martin Goros, David Hernandez, Amanda Paley, and Marika Vela-Gude.
References
- Acheson A, Richard DM, Mathias CW, Dougherty DM. Adults with a family history of alcohol related problems are more impulsive on measures of response initiation and response inhibition. Drug Alcohol Depend. 2011;117:198–203. doi: 10.1016/j.drugalcdep.2011.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Akaike H. Information theory and an extension of the maximum likelihood principle. In: Parzen E, Tanabe K, Kitagawa G, editors. Selected papers of Hirotugu Akaike. New York: Springer; 1998. pp. 199–213. [Google Scholar]
- Bjork JM, Hommer DW, Grant SJ, Danube C. Impulsivity in abstinent alcohol-dependent patients: relation to control subjects and type 1–/type 2–like traits. Alcohol. 2004;34:133–150. doi: 10.1016/j.alcohol.2004.06.012. [DOI] [PubMed] [Google Scholar]
- Brooks-Gunn J, Petersen AC, Eichorn D. The study of maturational timing effects in adolescence. J Youth Adolesc. 1985;14:149–161. doi: 10.1007/BF02090316. [DOI] [PubMed] [Google Scholar]
- Carskadon MA, Acebo C. A self-administered rating scale for pubertal development. J Adolesc Heath. 1993;14:190–195. doi: 10.1016/1054-139x(93)90004-9. [DOI] [PubMed] [Google Scholar]
- Caspi A, Moffitt TE. Individual differences are accentuated during periods of social change: The sample case of girls at puberty. J Pers Soc Psychol. 1991;61:157–168. doi: 10.1037//0022-3514.61.1.157. [DOI] [PubMed] [Google Scholar]
- Castellanos-Ryan N, Parent S, et al. Pubertal development, personality, and substance use: a 10-year longitudinal study from childhood to adolescence. J Abnorm Psychol. 2013;122:782–792. doi: 10.1037/a0033133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clark DB, Cornelius JR, Kirisci L, Tarter RE. Childhood risk categories for adolescent substance involvement: a general liability typology. Drug Alcohol Depend. 2005;77:13–21. doi: 10.1016/j.drugalcdep.2004.06.008. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. [Accessed June 30, 2015];About BMI for Children and Teens. 2014 Available from http://www.cdc.gov/healthyweight/assessing/bmi/childrens_bmi/childrens_bmi_formula.html.
- de Wit H. Impulsivity as a determinant and consequence of drug use: a review of underlying processes. Addict Biol. 2009;14:22–31. doi: 10.1111/j.1369-1600.2008.00129.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dougherty DM, Bjork JM, Harper RA, et al. Behavioral impulsivity paradigms: A comparison in hospitalized adolescents with disruptive behavior disorders. J Child Psychol Psychiatry. 2003;44:1145–1157. doi: 10.1111/1469-7610.00197. [DOI] [PubMed] [Google Scholar]
- Dougherty DM, Charles NE, Mathias CW, et al. Delay discounting differentiates pre-adolescents at high and low risk for substance use disorders based on family history. Drug Alcohol Depend. 2014;143:105–111. doi: 10.1016/j.drugalcdep.2014.07.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dougherty DM, Marsh DM, Mathias CW. Immediate and Delayed Memory Tasks: A computerized measure of memory, attention, and impulsivity. Behav Res Methods Instrum Comput. 2002;34:391–398. doi: 10.3758/bf03195467. [DOI] [PubMed] [Google Scholar]
- Dougherty DM, Marsh DM, Mathias CW, Swann AC. Bipolar disorder and substance abuse: The conceptualization and role of impulsivity. Psychiatr Times. 2005a;22:32–35. [Google Scholar]
- Dougherty DM, Marsh-Richard DM, Hatzis ES, et al. A test of alcohol dose effects on multiple behavioral measures of impulsivity. Drug Alcohol Depend. 2008;96:111–120. doi: 10.1016/j.drugalcdep.2008.02.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dougherty DM, Mathias CW, Dawes MA, et al. Impulsivity, attention, memory, and decision-making among adolescent marijuana users. Psychopharmacology. 2013;226:307–319. doi: 10.1007/s00213-012-2908-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dougherty DM, Mathias CW, Marsh DM, Jagar AA. Laboratory behavioral measures of impulsivity. Behav Res Methods Instrum Computers. 2005b;37:82–90. doi: 10.3758/bf03206401. [DOI] [PubMed] [Google Scholar]
- Dougherty DM, Mathias CW, Marsh-Richard DM, et al. Distinctions in behavioral impulsivity: Implications for substance abuse research. Addict Disord Treat. 2009;8:61–73. doi: 10.1097/ADT.0b013e318172e488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duka T, Townshend JM, Collier K, et al. Impairment in cognitive functions after multiple detoxifications in alcoholic inpatients. Alcohol Clin Exp Res. 2003;27:1563–1572. doi: 10.1097/01.ALC.0000090142.11260.D7. [DOI] [PubMed] [Google Scholar]
- Evenden JL. Impulsivity: a discussion of clinical and experimental findings. J Psychopharmacol. 1999;3:180–192. doi: 10.1177/026988119901300211. [DOI] [PubMed] [Google Scholar]
- Fillmore MT, Rush CR, Kelly TH, Hays L. Triazolam impairs inhibitory control of behavior in humans. Exp Clin Psychopharm. 2001;9:363–371. doi: 10.1037//1064-1297.9.4.363. [DOI] [PubMed] [Google Scholar]
- Geier CF. Adolescent cognitive control and reward processing: Implications for risk taking and substance use. Horm Behav. 2013;64:333–342. doi: 10.1016/j.yhbeh.2013.02.008. [DOI] [PubMed] [Google Scholar]
- Hamilton KR, Mitchell MR, Wing VC, et al. Choice impulsivity: Definitions, measurement issues, and clinical implications. Personal Disord Theory Res Treat. 2015;6:182–198. doi: 10.1037/per0000099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iacono WG, Malone SM, McGue M. Behavioral disinhibition and the development of early-onset addiction: common and specific influences. Annu Rev Clin Psychol. 2008;4:325–348. doi: 10.1146/annurev.clinpsy.4.022007.141157. [DOI] [PubMed] [Google Scholar]
- Kaufman J, Birmaher B, Brent D, et al. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Psychiatry. 1997;36:980–988. doi: 10.1097/00004583-199707000-00021. [DOI] [PubMed] [Google Scholar]
- Lane SD, Cherek DR, Rhoades HM, et al. Relationships among laboratory and psychometric measures of impulsivity: Implications in Substance Abuse and Dependence. Addict Disord Treat. 2003;2:33–40. [Google Scholar]
- Marceau K, Ram N, Susman EJ. Development and lability in the parent-child relationships during adolescence: Associations with pubertal timing and tempo. J Res Adolescence. doi: 10.1111/jora.12139. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshall WA, Tanner JM. Variations in the pattern of pubertal changes in boys. Arch Dis Child. 1970;45:13–23. doi: 10.1136/adc.45.239.13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCarthy DM, Niculete ME, Treloar HR, et al. Acute alcohol effects on impulsivity: Associations with drinking and driving behavior. Addiction. 2012;107:2109–2114. doi: 10.1111/j.1360-0443.2012.03974.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mendle J, Harden KP, Brooks-Gunn J, Graber JA. Development's tortoise and hare: pubertal timing, pubertal tempo, and depressive symptoms in boys and girls. Dev Psychol. 2010;46:1341–1353. doi: 10.1037/a0020205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moeller FG, Barratt ES, Dougherty DM, et al. Psychiatric aspects of impulsivity. Am J Psychiatry. 2001;158:1783–1793. doi: 10.1176/appi.ajp.158.11.1783. [DOI] [PubMed] [Google Scholar]
- Moeller FG, Barratt ES, Fischer CJ, et al. P300 event related potential amplitude and impulsivity in cocaine dependent subjects. Neuropsychobiology. 2004;50:167–173. doi: 10.1159/000079110. [DOI] [PubMed] [Google Scholar]
- Nagin DS. Group-based Modeling of Development. Cambridge, MA: Harvard University Press; 2005. [Google Scholar]
- Nagin DS, Odgers CL. Group-based trajectory modeling in clinical research. Annu Rev Clin Psychol. 2010;6:109–138. doi: 10.1146/annurev.clinpsy.121208.131413. [DOI] [PubMed] [Google Scholar]
- National Center for Health Statistics. 2000 CDC growth charts for the United States: Methods and development. [Accessed 09/01/2014];2000 Series 11, No. 246, 39. at http://www.cdc.gov/growthcharts/2000growthchart-us.pdf. [PubMed]
- Petersen AC, Crockett LJ. Pubertal timing and grade effects on adjustment. J Youth Adolesc. 1985;14:191–206. doi: 10.1007/BF02090318. [DOI] [PubMed] [Google Scholar]
- Petersen AC, Crockett L, Richards M, Boxer A. A self-report measure of pubertal status: Reliability, validity, and initial norms. J Youth Adolesc. 1988;17:117–133. doi: 10.1007/BF01537962. [DOI] [PubMed] [Google Scholar]
- Petersen AC, Taylor B. The biological approach to adolescence. In: Adelson J, editor. Handbook of Adolescent Psychology. New York: Wiley; 1980. pp. 115–155. [Google Scholar]
- Psychological Corporation. WASI: Wechsler Abbreviated Scale of Intelligence®. San Antonio, TX: Harcourt Brace and Company; 1999. [Google Scholar]
- Raftery AE. Bayesian model selection in social research. In: Marsden P, editor. Sociological Methodology. Cambridge, MA: Blackwell Sci; 1995. pp. 111–163. [Google Scholar]
- Reynolds B, Richards JB, de Wit H. Acute-alcohol effects on the Experiential Discounting Task (EDT) and a question-based measure of delay discounting. Pharmacol Biochem Behav. 2006;83:194–202. doi: 10.1016/j.pbb.2006.01.007. [DOI] [PubMed] [Google Scholar]
- Rice JP, Reich T, Bucholz KK, et al. Comparison of direct interview and family history diagnoses of alcohol dependence. Alcohol Clin Exp Res. 1995;19:1018–1023. doi: 10.1111/j.1530-0277.1995.tb00983.x. [DOI] [PubMed] [Google Scholar]
- Rubio G, Jimenez M, Rodriguez-Jimenez R, et al. The role of behavioral impulsivity in the development of alcohol dependence:a 4-year follow-up study. Alcohol Clin Exp Res. 2008;32:1681–1687. doi: 10.1111/j.1530-0277.2008.00746.x. [DOI] [PubMed] [Google Scholar]
- Ryan SR, Acheson A, Charles NE, et al. Clinical and social/environmental characteristics in a community sample of children with and without family histories of Substance Use Disorder in the San Antonio area: A descriptive study. J Child Adolesc Subst Abuse. doi: 10.1080/1067828X.2014.999202. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sanchez-Roige S, Baro V, Trick L, et al. Exaggerated waiting impulsivity associated with human binge drinking, and high alcohol consumption in mice. Neuropsychopharmacology. 2014;39:2919–2927. doi: 10.1038/npp.2014.151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz G. Estimating the dimension of a model. Ann Stat. 1978;6:61–464. [Google Scholar]
- Smith AR, Chein J, Steinberg L. Impact of socio-emotional context, brain development, and pubertal maturation on adolescent risk-taking. Horm Behav. 2013;64:323–332. doi: 10.1016/j.yhbeh.2013.03.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steinberg L. A social neuroscience perspective on adolescent risk-taking. Dev Rev. 2008;28:78–106. doi: 10.1016/j.dr.2007.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Winstanley CA, Eagle DM, Robbins TW. Behavioral models of impulsivity in relation to ADHD: translation between clinical and preclinical studies. Clin Psychol Rev. 2006;26:379–395. doi: 10.1016/j.cpr.2006.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]