

Abstract
[Purpose] This study aimed to clarify the immediate effects of a combined transcutaneous electrical nerve stimulation and stretching protocol. [Subjects] Fifteen healthy young males volunteered to participate in this study. The inclusion criterion was a straight leg raising range of motion of less than 70 degrees. [Methods] Subjects performed two protocols: 1) stretching (S group) of the medial hamstrings, and 2) tanscutaneous electrical nerve stimulation (100 Hz) with stretching (TS group). The TS group included a 20-minute electrical stimulation period followed by 10 minutes of stretching. The S group performed 10 minutes of stretching. Muscle hardness, pressure pain threshold, and straight leg raising range of motion were analyzed to evaluate the effects. The data were collected before transcutaneous electrical nerve stimulation (T1), before stretching (T2), immediately after stretching (T3), and 10 minutes after stretching (T4). [Results] Combined transcutaneous electrical nerve stimulation and stretching had significantly beneficial effects on muscle hardness, pressure pain threshold, and straight leg raising range of motion at T2, T3, and T4 compared with T1. [Conclusion] These results support the belief that transcutaneous electrical nerve stimulation combined with stretching is effective in reducing pain and decreasing muscle hardness, thus increasing range of motion.
Key words: TENS, Muscle hardness, Stretching
INTRODUCTION
One of the major purposes of physical therapy is improvement of muscle flexibility and consequently increase of the range of motion (ROM) of the affected joint. From the suite of manual skills available, joint range of motion exercises and stretching are more commonly selected. From the available selection of physical agents, thermal therapy and electrical stimulation therapy have been actively used to improve tightened soft tissue, alleviate pain, and reduce the muscle spasms that limit ROM. The aims of applying a physical agent and stretching are similar to each other, such as to decrease pain and aid relaxation; therefore, they are often used in combination with each other in order to be complementary and with the expectation of synergistic effects. Currently the main combination is thermotherapy and therapeutic exercises, such as hot packs or therapeutic ultrasound with stretching. Thermotherapy modalities, when applied before therapeutic exercises, promote improvement in connective tissue (such as collagen fiber) extensibility; this improvement is thought to enhance the effect of stretching. When the pain is the primary complaint recorded and thus restricted ROM is present, transcutaneous electrical nerve stimulation (TENS) is initially applied to relieve the pain before the application of ROM exercises and stretching in the clinical setting.
In our previous study1), we clarified that TENS, when applied to the medial hamstrings in young healthy subjects, led to an increased pressure pain threshold (PPT), which resulted in decreased muscle hardness (MH) and an increased straight leg raising (SLR) range of motion(ROM). This is consistent with the findings of Espejo2), who applied interferential current through bipolar application with a frequency of 4 kHz and a frequency modulation amplitude of 100 Hz. They reported that their electrical stimulation group and stretching group had greater effects on improvement of knee extension range when compared with their control group.
When deep connective tissues, such as the skeletal muscle and the joint capsule, are injured, excitement of the nociceptor is induced, and this leads to hyperactivity in the muscle spindle and lowering of the muscle spindle threshold. This condition of increased muscle tone is called muscular guarding. With regards to circulatory dynamics, persistent muscle contraction induces a state of ischemia in the muscle, which produces algesic substances, such as inflammatory mediators, and induces excitation of the nociceptor3). Kubo4) stated that improvement in the ROM as caused by stretching accompanied changes in muscle-tendon unit viscoelasticity and increased pain tolerance at the end of the stretching range. When passively stretching muscles, increased pain would be a factor limiting ROM in addition to shortening of the muscle and soft tissue. Given the above, we hypothesized that TENS could enhance the stretching effect in a synergistic manner by decreasing MH and increasing both muscle flexibility and the pain threshold. The purpose of this study was to clarify the immediate effects of TENS in combination with stretching on MH, PPT, and the ROM in SLR in healthy individuals.
SUBJECTS AND METHODS
Fifteen healthy young males (age, 18–26 years; height, 168.8 ± 4.7 cm; body weight, 67.8 ± 13.7 kg) volunteered to participate in this study. The inclusion criteria were as follows: 1) no history of neuromuscular disease or musculoskeletal injury involving the lower extremities and 2) less than 70 degrees ROM in SLR. All subjects were notified of the procedures and purpose of this study, and informed written consent was obtained from all of the volunteers before initiation of the study. The protocol was approved by the Koriyama Tohto Academy Educational Foundation Ethics Committee (approval number: R-1401).
Subjects performed two protocols, which were 1) stretching alone (S group) and 2) TENS and stretching (TS group). The TS group received a 20-minute TENS application and immediately afterwards performed 10 minutes of stretching, while the S group completed only 10 minutes of stretching. Both protocols included 10-minute rest, periods with the subjects in the supine position before and after the protocols. Static stretching (i.e., stretching) was used as the stretching method in our study. Stretching was done at 90% of the maximum SLR ROM for 30 seconds followed by a 30-second rest a total of 10 times over 10 minutes.
Electrical stimulation was generated via a TENS unit (EU-940, ITO Co., Ltd., Tokyo, Japan). The TENS parameters were s symmetrical biphasic pulse current waveform, 100 Hz frequency, and 200 μs pulse duration. TENS lasted for 20 minutes. The stimulation intensity was set at 80% of the sense of pain threshold and in which a muscular contraction was also produced. TENS was delivered through two self-adhesive carbon rubber electrodes (5 cm × 9 cm) positioned over the medial hamstrings and attached to the middle portion between the ischial tuberosity and the popliteal region, and they were located 20 cm apart.
Three parameters were used for the experiment: PPT, soft tissue hardness as expressed by MH, and SLR ROM. The data were collected before TENS (T1), before stretching (T2, immediately after the end of TENS application for the TS group), immediately after stretching (T3), and 10 minutes after stretching was concluded (T4).
A digital clinometer was used to measure the SLR ROM. The clinometer was placed on the patellar ligament and adjusted to zero at the starting point of the SLR ROM, and then the maximum SLR ROM was measured manually. The knee and hip joints of the contralateral leg were maintained in full extension. For the measurements of MH and PPT, an Outcome Evaluation System (OE-220, ITO Co., Ltd., Tokyo, Japan) was used5), and MH and PPT were measured on the medial hamstrings at an angle of 90% of the maximum SLR ROM. In order to maintain this angle, the distal part of the lower leg was suspended in a sling, and the sling was fixed at the position in which the traction force was applied perpendicular to the lower leg through a pulley (Fig. 1). MH and PPT were measured three times, and the mean values were calculated. The experimental room was controlled at a temperature of 25 °C and a humidity of 50%. The two protocols were performed on two separate occasions at least one day apart but no more than seven days apart. The order of testing was randomized.
Fig. 1.
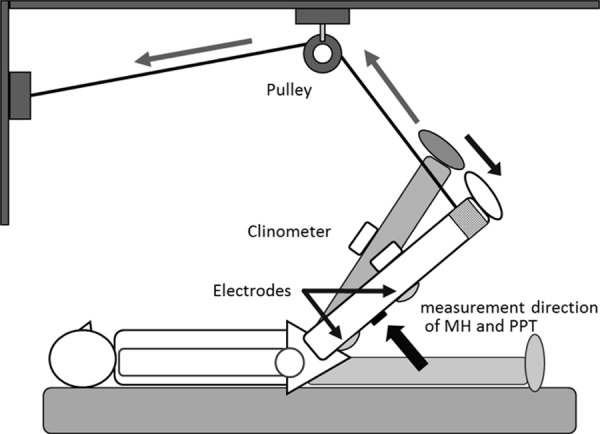
Block diagram of the experimental setup
In the position of 90% SLR ROM, the muscle hardness (MH) and pressure pain threshold (PPT) were measured on the medial hamstrings, and the measurement sensors were attached to the lower leg.
Statistical analysis with a paired t-test was used to compare the differences in values at T1 in the TS group and at T2 in the S group. Additionally, a one-way repeated measures analysis of variance (ANOVA) was performed to determine the time-dependent changes (between T1, T2, T3, and T4) in each group, and a Bonferroni’s test was undertaken at the point at which a significant main effect was observed. The difference values were calculated based on T2 in the S group and T1 in the TS group. Difference value 1 (D1) indicates the difference between T2 and T3 in the S group or between T1 and T3 in the TS group, while difference value 2 (D2) indicates the difference between T2 and T4 in the S group or between T1 and T4 in the TS group. These differences can be expressed as D1=T3−T2 and D2=T4−T2 for the S group and as D1=T3−T2 and D2=T4−T2 for the TS group. Following calculation of the difference values, a paired t-test was performed to detect significant differences between the S and TS groups. IBM SPSS Statistics for Windows, version 22.0 (IBM Japan, Ltd., Tokyo, Japan), was used, and statistical significance was accepted for values of p < 0.05 in all analyses.
RESULTS
The changes in MH, PPT, and SLR ROM (mean ± SD) in the S and TS groups are shown in Table 1, 2, and 3. There was no significant difference between T2 in the S group and T1 in the TS group. Therefore, the starting values were relatively similar between the S group and the TS group for all three parameters.
Table 1. Changes in MH of each group and comparison between groups Mean±SD (N) n=15.
| T1 | T2 | T3 | T4 | D1 | D2 | |
|---|---|---|---|---|---|---|
| S group | 3.6±0.5 | 3.4±0.4 | 3.5±0.4 | −0.2±0.2 | 0.1±0.1 | |
| TS group | 3.6±0.5 | 3.1±0.5 | 3.1±0.5 | 3.4±0.5 | −0.5±0.2** | −0.3±0.2** |
S group: stretching alone; TS group: TENS and stretching. **D1&D2: S group vs. TS group (p<0.01)
Table 2. Changes in PPT of each group and comparison between groups Mean±SD (N) n=15.
| T1 | T2 | T3 | T4 | D1 | D2 | |
|---|---|---|---|---|---|---|
| S group | 15.1±1.3 | 15.6±1.3 | 15.2±1.3 | 0.6±1.2 | 0.1±1.0 | |
| TS group | 14.7±1.9 | 21.9±1.9 | 20.6±2.3 | 17.3±1.1 | 5.9±2.0** | 2.6±1.4** |
S group: stretching alone; TS group: TENS and stretching. **D1&D2: S group vs. TS group (p<0.01)
Table 3. Changes in SLR ROM of each group and comparison between groups Mean±SD (degrees) n=15.
| T1 | T2 | T3 | T4 | D1 | D2 | |
|---|---|---|---|---|---|---|
| S group | 65.3±2.4 | 70.7±3.0 | 69.8±2.8 | 5.4±2.0 | 4.5±2.2 | |
| TS group | 64.8±1.8 | 73.2±3.2 | 76.9±4.1 | 73.1±0.4 | 12.2±2.8** | 8.3±1.9** |
S group: stretching alone; TS group: TENS and stretching. **D1&D2: S group vs. TS group (p<0.01)
In the S group, one-way repeated measures ANOVA revealed significant main effects in MH and SLR ROM (MH, F = 11.07, p < 0.01; PPT, F = 2.07, p = 0.146; SLR, F = 66.50, p < 0.01). Multiple comparison revealed significant differences in T3 compared with T2 in MH (p < 0.01) and in T3 and T4 compared with T2 in SLR ROM (p < 0.01). On the other hand, there were significant main effects in MH, PPT, and SLR ROM in the TS group (MH, F = 65.54, p < 0.01; PPT, F = 107.56, p < 0.01; SLR, F= 162.40, p < 0.01). Multiple comparison showed significant differences in T2, T3, and T4 compared with T1 in all parameters (p < 0.01 except p < 0.05 at T4 in MH).
With regards to the results of MH, D1 in the S group was −0.2 ± 0.2 N, and D1 in the TS group was −0.5 ± 0.2 N; thus, there was a significant difference between the groups (p < 0.01). Similarly, D2 in the S group was −0.1 ± 0.1 N, and D2 in the TS group was −0.3 ± 0.2 N; thus, there was a significant difference between the groups (p < 0.01).
Secondly, the changes in PPT were as follows: D1 in the S group was 0.6 ± 1.2 N, and D1 in the TS group was 5.9 ± 2.0 N; there was a significant difference between the groups (p < 0.01). Similar results were shown for D2. D2 in the S group was 0.1 ± 1.0 N, and D2 in the TS group was 2.6 ± 1.4 N; there was a significant difference between the groups (p < 0.01).
In terms of SLR ROM, D1 in the S group was 5.4 ± 2.0°, and D1 in the S group was 12.2 ± 2.8°; there was a significant difference between the groups (p < 0.01). Similarly, D2 in the S group was 4.5 ± 2.2°, and D2 in the TS group was 8.3 ± 1.9°; there was a significant difference between the groups (p < 0.01).
DISCUSSION
We examined the influence of TENS on muscle hardness and pressure pain threshold in a previous study1). As a new initiative, this study aimed to clarify the immediate effects of the combination of TENS, which is widely known to have a pain inhibitory effect, and stretching by using the three parameters of muscle hardness, pressure pain threshold, and SLR ROM. The main findings in this study show that the combination of TENS and stretching is more effective than stretching alone, since the results for all three parameters, muscle hardness, pressure pain threshold, and SLR ROM, in the TS group showed significantly beneficial changes compared with the S group.
A large number of studies have reported the pain inhibitory effect of TENS6,7,8,9,10,11,12,13,14). Previous studies10, 15, 16) have shown that the TENS parameter used in this study has a high hypoalgesic effect. As in these studies, the present study also revealed significantly increased values for pressure pain threshold in the TS group, although the S group did not show such a significant change. Calculation of the percentage (the rate of change) of D1 based on T1 in the TS group (based on T2 in the S group) revealed that the TS group had a 41.0 ± 15.9% difference and that the S group had a 3.8 ± 7.9% difference in pressure pain threshold. From the above, the pain inhibitory effect of TENS and stretching when used in combination was readily recognized, and the results indicated that stretching might not achieve the same amount of inhibitory effect when performed solely.
There are several earlier reports that examined the method and time parameters and conditions of stretching17,18,19,20,21,22,23). Akagi17) reported that 2 minutes of stretching of the gastrocnemius significantly increased ROM and decreased muscle-tendon unit stiffness; however, it did not change the joint torque. Nakamura18) assessed passive torque as an index of muscle-tendon unit resistance and myotendinous junction displacement as an index of muscle extensibility using ultrasonography and a dynamometer during 5 minutes of stretching. Their results suggested that stretching for more than 2 minutes effectively increased muscle extensibility, which in turn decreased muscle-tendon unit resistance. Matsuo19) and Umegaki20) also reported that 5 minutes of stretching, the protocol for which comprised of 5 repeated 1-minute stretching periods with a 30-second rest period between each stretching period, decreased the stiffness of the hamstring’ muscle-tendon unit. Additionally, Magnusson21) also reported the effectiveness of 5 minutes of stretching in improving the flexibility of the hamstrings. Based on the above studies, the time set for stretching in this study (a total of 5 minutes of stretching over an allocated 10-minute period) seemed to be adequate to obtain a sufficient effect.
With regards to the actual method of stretching for the hamstrings, Umegaki24) studied the use of ultrasonic shear wave elastography and reported that adding hip rotation to the stretching position for the hamstrings (i.e., internal rotation for the medial hamstrings and external rotation for the lateral hamstrings) may not have a significant effect on muscle elongation of each hamstring. Given the above, we stretched the medial hamstrings at the intermediate position between internal and external rotation in the present study.
Regarding the application of a combined physical agent and stretching protocol, there are many studies that have reported on the combination of thermal therapy, such as hot packs, and stretching. A meta-analysis completed by Nakano25) reviewed 12 randomized clinical trials involving 352 healthy participants and concluded that treatments combining thermal therapy and stretching improved ROM when compared with stretching alone. Additionally, they stated that this is due to increased collagen extensibility and reduced connective tissue viscosity and viscoelasticity of muscle fiber at higher temperatures as caused by the thermal therapy.
As for the combined usage of TENS and stretching, general clinical recommendations are as follows: stretching is applied after reducing pain by TENS in orthopedic disorders, and stretching is applied during or after electrically stimulating the antagonist of muscles displaying high levels of spasticity in central nervous system disorders26, 27). However, the mechanisms of their effects have not been fully clarified.
Hou et al.6) reported on the combination of physical agents and therapeutic exercises and stated that some combinations were effective for easing cervical myofascial pain and increasing cervical ROM. They compared five therapeutic combinations of ischemic compression, TENS, stretching, interferential current or the myofascial release technique combined with hot packs and active ROM exercise. The results showed that a combination of a hot pack plus active ROM exercise coupled with TENS or interferential current was more effective for pain relief and that a combination of a hot pack plus active ROM exercise coupled with stretching or the myofascial release technique was more effective in increasing cervical ROM than other combinations. These results partially support our findings, particularly regarding the results indicating a pain inhibitory effect caused by the combined usage of TENS and the therapeutic exercise. However, the precise influence of TENS on muscle hardness and ROM is not clear.
As for the effect of TENS on muscle hardness, our previous study15) showed that TENS significantly reduced muscle hardness values, although at 10 minutes after application, the reduction level was not as much as that immediately after application. In the present study, we could maintain the TENS effect for 10 minutes after application by adding stretching after TENS. The results show that the change rate of D1 for muscle hardness was −14.1 ± 4.7% in the TS group and −6.3 ± 5.0% in the S group; the TS group had a significant decrease in the muscle hardness compared with the S group.
Regarding the SLR ROM, the change rates of D1 were 18.7 ± 4.0% and 8.0 ± 3.0% in the TS and S groups; thus there was almost a 19% increase in SLR ROM in the TS group. Espejo2) reported that interferential current and stretching both had significant effects on improvement of ROM in the knee joint compared with the control group, although there was almost no difference between the two interventions. The reason why a significant difference was not seen between the two interventions is likely due to the length of the interferential current application and stretching. In the study, the length of the stretching procedure was 80 seconds, which included 2 sets of 30-seconds of stretching and 10 seconds of rest. The length of electrotherapy also matched the procedure for stretching, i.e., a total of 80 seconds, which included 2 sets of 30-seconds of stimulation with 10 seconds of rest. In our experiment, we applied TENS for 20 minutes; therefore, this could have led to a significant effect compared with the previous study. Furthermore, the combined application in our study was found to be more effective for increasing hamstrings extensibility than a single solely applied protocol.
Passive ROM has been recognized as a less reliable index in assessment of improvement in muscle flexibility and the effects of stretching. This is because it tends to be affected by psychological factors, such as increased tolerance of pain and repeated extension stimulation28). Because of this, several measurement methods, such as measuring passive torque when moving a joint passively and measuring the amount of displacement of the muscle-tendon junction, have been developed recently as new tools for evaluating muscle flexibility and the effects of stretching. However, these methods require expensive devices, such as an isometric dynamometer and ultrasonography; additionally, passive torque is generally used only as a parameter of limited joint movement. Nakamura29) reported that significant positive correlations were observed between muscle hardness and passive torque or displacement of the myotendinous junction and suggested that muscle hardness when measured by a muscle hardness meter is both an accurate index and an easy-to-use method. In our study, a muscle hardness meter was used to assess the changes in muscle hardness while maintaining the same SLR ROM before and after the intervention. Since a significant decrease in muscle hardness was shown post intervention, it could be deduced that the intervention significantly increased muscle tissue flexibility.
In our previous study1), an increased pressure pain threshold was observed after applying TENS. Based on this finding, the mechanism of the decrease in muscle hardness might be explained as follows: firstly, decreased input from the sensory system caused by the pain inhibitory effect of TENS led to a decline in γ-motor neuron activity and thus a decline in muscle spindle sensitivity. Therefore, the overactivity of muscle tone was controlled, and this resulted in decreased muscular viscoelasticity and an increase in ROM.
In addition to the above mechanism, further increased muscle flexibility resulting from stretching could be the reason for the significant increase in the SLR ROM. Increased muscle flexibility caused by stretching has been indicated to be due to an increase in the flexibility and movement of the aponeurosis and the connective tissue, such as the endomysium, perimysium, and epimysium, and not to be due to lengthening of muscle fiber30, 31).
There are several limitations in this study. Firstly, we did not investigate how the physical stimulation of TENS had influenced the connective tissue, including the perimysium and the epimysium, because of the parameters used in this study. Secondly, since the intensity of the electrical stimulation used in this study was set at a level that induced muscle contraction, electrical stimulation might have additionally produced local muscle fatigue. Thus, electrical stimulation might also influence the changes in muscle hardness. Furthermore, this study targeted healthy young males as subjects, and so further clinical study is required to clarify the effects of combined usage of TENS and stretching on elderly people and people with pain and muscle tone abnormalities.
We investigated the immediate outcomes caused by combined application of TENS and stretching on muscle hardness, pressure pain threshold, and SLR ROM. The findings in this study revealed that combined usage led to a significant decrease in muscle hardness, a significant increase in the pressure pain threshold, and a significant increase in SLR ROM when compared with stretching alone. Therefore, it is suggested that a combination of TENS and stretching is an effective method of increasing muscle flexibility.
REFERENCES
- 1.Ogihara H, Karasuno H, Morishita K, et al. : Influence of transcutaneous electrical nerve stimulation (TENS) on muscular viscoelasticity: chang in muscular hardness at straight leg raising (SLR). J J Electro Agents, 2015, 22: 22–29. [Google Scholar]
- 2.Espejo-Antunez L, Lopez-Minarro PA, Albornoz-Cabello M, et al. : Acute effect of electrical muscle elongation and static stretching in hamstring muscle extensibility. Sci Sports, 2015, 15: 1–7. [DOI] [PubMed] [Google Scholar]
- 3.Muraoka Y, Masakado Y, Tomita Y, et al. : Disynaptic reciprocal inhibition in stroke patients before and after therapeutic electrical stimulation. Jpn J Rehabil Med, 2000, 37: 453–458. [Google Scholar]
- 4.Kubo K: Viscoelastic change of muscle tendon unit by application of therapeutic stretching. Rigaku Ryoho, 2010, 27: 967–972 (in Japanese). [Google Scholar]
- 5.Morozumi K, Fujiwara T, Karasuno H, et al. : A new tissue hardness meter and algometer; a new meter incorporating the functions of a tissue hardness meter and an algometer. J Phys Ther Sci, 2010, 22: 239–245. [Google Scholar]
- 6.Hou CR, Tsai LC, Cheng KF, et al. : Immediate effects of various physical therapeutic modalities on cervical myofascial pain and trigger-point sensitivity. Arch Phys Med Rehabil, 2002, 83: 1406–1414. [DOI] [PubMed] [Google Scholar]
- 7.Han JS, Terenius L: Neurochemical basis of acupuncture analgesia. Annu Rev Pharmacol Toxicol, 1982, 22: 193–220. [DOI] [PubMed] [Google Scholar]
- 8.Han JS, Chen XH, Sun SL, et al. : Effect of low- and high-frequency TENS on Met-enkephalin-Arg-Phe and dynorphin A immunoreactivity in human lumbar CSF. Pain, 1991, 47: 295–298. [DOI] [PubMed] [Google Scholar]
- 9.Tong KC, Lo SK, Cheing GL: Alternating frequencies of transcutaneous electric nerve stimulation: does it produce greater analgesic effects on mechanical and thermal pain thresholds? Arch Phys Med Rehabil, 2007, 88: 1344–1349. [DOI] [PubMed] [Google Scholar]
- 10.Chesterton LS, Foster NE, Wright CC, et al. : Effects of TENS frequency, intensity and stimulation site parameter manipulation on pressure pain thresholds in healthy human subjects. Pain, 2003, 106: 73–80. [DOI] [PubMed] [Google Scholar]
- 11.Chen CC, Johnson MI: An investigation into the hypoalgesic effects of high- and low-frequency transcutaneous electrical nerve stimulation (TENS) on experimentally-induced blunt pressure pain in healthy human participants. J Pain, 2010, 11: 53–61. [DOI] [PubMed] [Google Scholar]
- 12.Dailey DL, Rakel BA, Vance CG, et al. : Transcutaneous electrical nerve stimulation reduces pain, fatigue and hyperalgesia while restoring central inhibition in primary fibromyalgia. Pain, 2013, 154: 2554–2562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Levin MF, Hui-Chan CW: Conventional and acupuncture-like transcutaneous electrical nerve stimulation excite similar afferent fibers. Arch Phys Med Rehabil, 1993, 74: 54–60. [PubMed] [Google Scholar]
- 14.Bi X, Lv H, Chen BL, et al. : Effects of transcutaneous electrical nerve stimulation on pain in patients with spinal cord injury: a randomized controlled trial. J Phys Ther Sci, 2015, 27: 23–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ogihara H, Karasuno H, Morishita K, et al. : The influence of Transcutaneous Electrical Nerve Stimulation (TENS), utilizing different stimulus parameters, on the pain control mechanism—changes in pressure pain threshold before and after TENS application—. JABM, 2014, 5: 39–45. [Google Scholar]
- 16.Tanaka K, Ikeuchi M, Izumi M, et al. : Effects of two different intensities of transcutaneous electrical nerve stimulation on pain thresholds of contralateral muscles in healthy subjects. J Phys Ther Sci, 2015, 27: 2771–2774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Akagi R, Takahashi H: Acute effect of static stretching on hardness of the gastrocnemius muscle. Med Sci Sports Exerc, 2013, 45: 1348–1354. [DOI] [PubMed] [Google Scholar]
- 18.Nakamura M, Ikezoe T, Takeno Y, et al. : Time course of changes in passive properties of the gastrocnemius muscle-tendon unit during 5 min of static stretching. Man Ther, 2013, 18: 211–215. [DOI] [PubMed] [Google Scholar]
- 19.Matsuo S, Suzuki S, Iwata M, et al. : Acute effects of different stretching durations on passive torque, mobility, and isometric muscle force. J Strength Cond Res, 2013, 27: 3367–3376. [DOI] [PubMed] [Google Scholar]
- 20.Umegaki H, Ikezoe T, Nakamura M, et al. : Acute effects of static stretching on the hamstrings using shear elastic modulus determined by ultrasound shear wave elastography: differences in flexibility between hamstring muscle components. Man Ther, 2015, 20: 610–613. [DOI] [PubMed] [Google Scholar]
- 21.Magnusson SP, Simonsen EB, Aagaard P, et al. : Biomechanical responses to repeated stretches in human hamstring muscle in vivo. Am J Sports Med, 1996, 24: 622–628. [DOI] [PubMed] [Google Scholar]
- 22.Nishikawa Y, Aizawa J, Kanemura N, et al. : Immediate effect of passive and active stretching on hamstrings flexibility: a single-blinded randomized control trial. J Phys Ther Sci, 2015, 27: 3167–3170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kimura A: The effects of hamstring stretching on leg rotation during knee extension. J Phys Ther Sci, 2013, 25: 697–703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Umegaki H, Ikezoe T, Nakamura M, et al. : The effect of hip rotation on shear elastic modulus of the medial and lateral hamstrings during stretching. Man Ther, 2015, 20: 134–137. [DOI] [PubMed] [Google Scholar]
- 25.Nakano J, Yamabayashi C, Scott A, et al. : The effect of heat applied with stretch to increase range of motion: a systematic review. Phys Ther Sport, 2012, 13: 180–188. [DOI] [PubMed] [Google Scholar]
- 26.Karakoyun A, Boyraz İ, Gunduz R, et al. : Electrophysiological and clinical evaluation of the effects of transcutaneous electrical nerve stimulation on the spasticity in the hemiplegic stroke patients. J Phys Ther Sci, 2015, 27: 3407–3411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Cho HY, Kim EH, Kim B, et al. : Effects of repetitive high frequency transcutaneous electrical nerve stimulation (HF-TENS) on spasticity and motor function following spinal cord injury in rats. J Phys Ther Sci, 2012, 24: 133–137. [Google Scholar]
- 28.McHugh MP, Kremenic IJ, Fox MB, et al. : The role of mechanical and neural restraints to joint range of motion during passive stretch. Med Sci Sports Exerc, 1998, 30: 928–932. [DOI] [PubMed] [Google Scholar]
- 29.Nakamura M, Ikezoe T, Takeno Y, et al. : Relationship between muscle stiffness measured by the muscle hardness meter and passive torque or myotendinous junction displacement. Rigaku Ryohogku, 2013, 40: 193–199. [Google Scholar]
- 30.Morse CI, Degens H, Seynnes OR, et al. : The acute effect of stretching on the passive stiffness of the human gastrocnemius muscle tendon unit. J Physiol, 2008, 586: 97–106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Nakamura M, Ikezoe T, Takeno Y, et al. : Acute and prolonged effect of static stretching on the passive stiffness of the human gastrocnemius muscle tendon unit in vivo. J Orthop Res, 2011, 29: 1759–1763. [DOI] [PubMed] [Google Scholar]