

Abstract
We present the case of a 70-year-old man with a giant right-sided retroperitoneal pseudocyst, confirmed histologically after resection to be benign with appearances dissimilar to pancreatic and adrenal tissue. The cyst was noted incidentally on table at the time of laparoscopic surgery. Retroperitoneal pseudocysts most commonly arise from the pancreas and adrenal glands occurring as a result of an inflammatory process. Primary retroperitoneal pseudocysts are a rare entity. This case highlights the importance of examining the patient thoroughly and not focusing on the obvious. The mass was not palpated on initial review prior to listing for surgery, and the patient was asymptomatic from the mass.
Introduction
We report the unusual case of a 70-year-old Caucasian man who presented with a nonspecific symptom and was noted to have a giant retroperitoneal pseudocyst.
A pseudocyst is defined as a fluid-filled cavity that is not lined by an epithelial surface. Most pseudocysts arise from retroperitoneal structures like the pancreas and the adrenal glands. In this case report, we discuss the incidental finding of a primary retroperitoneal pseudocyst [1–4].
Case Report
A 70-year-old patient was referred to the general surgical clinic complaining of bilateral reducible groin swellings. The right-sided swelling was slightly larger than the left and was also, at times, uncomfortable. There were no obstructive symptoms of note. His medical history included shingles and a hiatus hernia. The patient was a non-smoker who occasionally drank alcohol. He was fit and well otherwise aside from a slightly elevated BMI (28 kg/m2). Bilateral inguinal hernias were diagnosed and the patient was listed to undergo an elective laparoscopic bilateral inguinal hernia repair.
Electively the procedure was carried out through a totally extra-peritoneal approach. The procedure was uneventful aside from the incidental finding of a large right-sided cystic mass below the liver edge. This was noted clinically when the patient was on table and was confirmed laparoscopically. The patient was later discharged as a day case and an urgent outpatient computed tomography (CT) of abdomen and pelvis was organized.
The CT (Figs 1–3) was performed identifying a unilocular, cystic lesion arising from within the right side of the abdomen. This lesion was distinct and not found to be related to any of the intra-abdominal organs. The radiological dimensions of the lesion were 22 × 20 × 19 cm. There were no radiological features to suggest acute or chronic pancreatitis. The findings were explained to the patient, and he was booked for laparotomy and excision of the cyst.
Figure 2:

Coronal section of the retroperitoneal pseudocyst.
Figure 1:
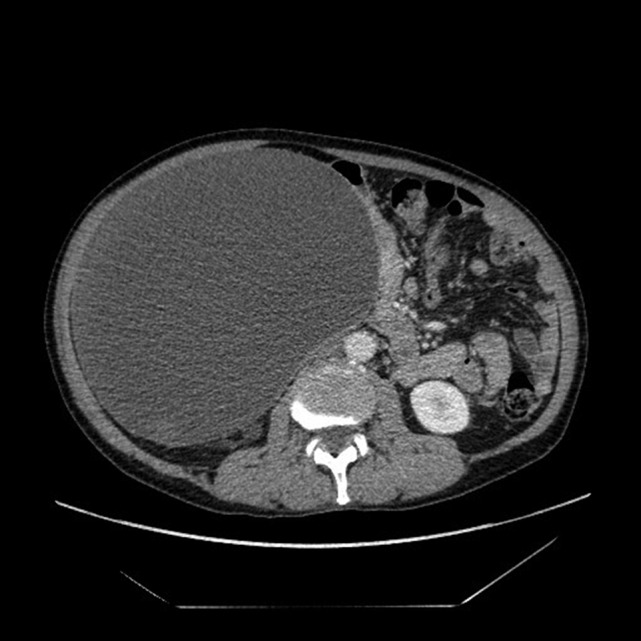
Axial slice from the CT imaging identifying the retroperitoneal pseudocyst.
Figure 3:

Sagittal view of the retroperitoneal pseudocyst.
Intra-operatively, a midline approach was used. A large cyst was identified and found to be occupying most of the right retroperitoneal cavity. Medially, the cyst was attached to the small bowel mesentery and extended from immediately below the liver to the pelvic brim. The cyst was mobilized free and retrieved intact using both blunt and sharp dissection. Intra-operatively, the procedure progressed uneventfully. Figures 4 and 5 show operative retrieval of the pseudocyst and the macroscopic appearances of the specimen.
Figure 4:
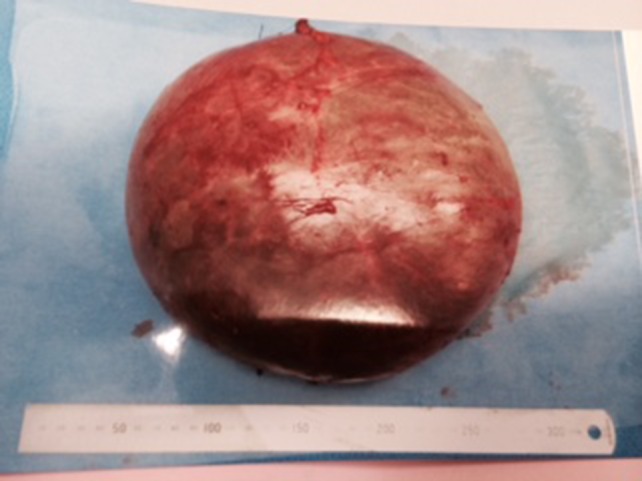
The intact excised pseudocyst.
Figure 5:
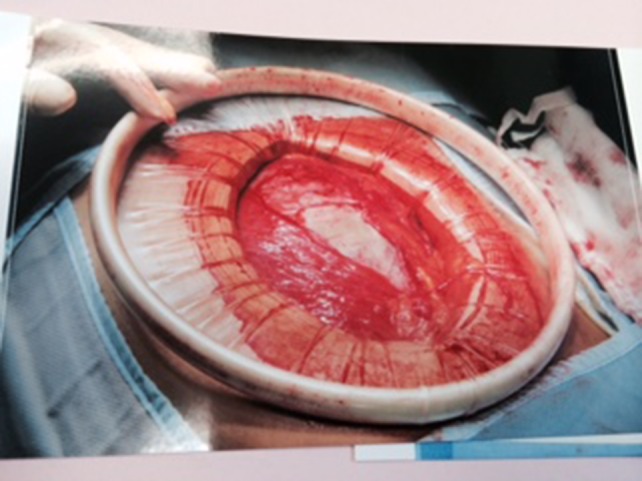
A large Alexis wound retractor was utilized. In the image, centrally, the pseudocyst can be identified prior to retrieval.
Macroscopic histology showed an intact retroperitoneal cyst measuring 24 × 21 × 13 cm containing turbid fluid and weighing 4035 g. Microscopically the cyst wall was lined by foamy macrophages and fibrin, with some chronic inflammation noted in the wall as well. An epithelial or mesothelial lining was absent in all of the multiple sections taken. It was identified as a benign pseudocyst with no evidence of malignancy. The appearances were dissimilar to pancreatic and adrenal tissues.
Discussion
Primary retroperitoneal pseudocysts are a rare entity and arise predominately from the mesentery and omentum without any significant communication with adjacent structures [1]. They are characteristically unilocular or multilocular in appearance with abundant debris on abdominal ultrasound scan and an enhancing wall on CT imaging [2]. Cystic lesions in the retroperitoneum are rare with a reported incidence of between 0.0004 and 0.02% per annum, with even a smaller percentage being ‘pseudo’ in origin [5]. Pseudocysts consist of serous fluid and due to their non-pancreatic etiology contain significantly low levels of amylase and lipases. Histopathological assessment usually demonstrates a fluid-filled cavity devoid of epithelium that is not histologically similar to either pancreatic or adrenal tissue. In chronic cases, the surrounding fibrous capsule undergoes calcification and has been described as ‘resembling an eggshell’ [3].
Non-pancreatic retroperitoneal pseudocysts generally grow at a slow, steady rate and only become symptomatic if they become large enough to compress adjacent anatomical structures. Primary retroperitoneal pseudocysts can become both necrotic and infected [4, 5].
Surgical excision is the mainstay of treatment and has the best outcome in the literature reviewed. An open approach is preferable if the patient is symptomatic, the mass is >6 cm or the possibility of malignancy is present. Laparoscopic surgery is indicated for small pseudocysts [4, 5].
This case highlights the importance of a thorough clinical history/examination during a busy general surgical clinic. The patient initially presented with bilateral reducible groin swellings and was asymptomatic with regard to gastrointestinal/general symptoms. The pseudocyst was incidentally discovered on table laparoscopically. Pseudocysts are a rare entity and can grow to large sizes without causing any specific symptoms. This combined with the minimal literature and scientific evidence available, we as clinicians are at risk of identifying and treating these patients at a later stage resulting in higher mortality and morbidity. The benefits of laparoscopic surgery have been highlighted in identifying incidental intra-abdominal pathologies when history and examination have failed. This report aims to add to the literature with regard to presentation, pathophysiology and management so that these patients are identified and treated at an earlier stage.
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Author Contributions
L.K. performed literature review, devised first and subsequent drafts; D.L. performed literature review, devised first and subsequent drafts; M.S. conceived study, participated in design and coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
Conflict of Interest Statement
None declared.
References
- 1.Prabhu R, Rodrigues G, Sarma YS, Benakatti R.. Non-pancreatic retroperitoneal pseudocyst: a benign disease with non-specific symptoms. BMJ Case Rep doi:10.1136/bcr-2013-200184. http://casereports.bmj.com/content/2013/bcr-2013-200184.abstract [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Yang DM, Jung DH, Kim H, Kang JH, Kim SH, Kim JH, et al. Retroperitoneal cystic masses: CT, clinical, and pathologic findings and literature review. Radiographics 2004;24:1353–65. http://www.ncbi.nlm.nih.gov/pubmed/15371613 [DOI] [PubMed] [Google Scholar]
- 3.Li ZL, Li HL, Chen HW, Gan WM.. An eggshell-like retroperitoneal pseudocyst. Urology 2011;78:561–2. http://www.ncbi.nlm.nih.gov/pubmed/21333331 [DOI] [PubMed] [Google Scholar]
- 4.Palanivelu C, Rangarajan M, Senthilkumar R, Madhankumar MV, Annapoorni S.. Laparoscopic excision of an infected ‘egg-shelled’ retroperitoneal pseudocyst. J Gastrointest Liver Dis 2008;17:465–8. http://www.jgld.ro/2008/4/17.pdf [PubMed] [Google Scholar]
- 5.Nam SH, Kim DY, Kim SC, Kim IK. The surgical experience for retroperitoneal, mesenteric and omental cyst in children. J Korean Surg Soc 2012;83:102–6. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3412181/ [DOI] [PMC free article] [PubMed] [Google Scholar]