

Abstract
Toxoplasma gondii is an important opportunistic pathogen that causes toxoplasmosis, which has very few therapeutic treatment options. The most effective therapy is a combination of pyrimethamine and sulfadiazine; however, their utility is limited because of drug toxicity and serious side effects. For these reasons, new drugs with lower toxicity are urgently needed. In this study, the compound, (Z)-1-[(5-nitrofuran-2-yl)methyleneamino]-imidazolidine-2,4-dione (nitrofurantoin), showed anti-T. gondii effects in vitro and in vivo. In HeLa cells, the selectivity of nitrofurantoin was 2.3, which was greater than that of pyrimethamine (0.9). In T. gondii-infected female ICR mice, the inhibition rate of T. gondii growth in the peritoneal cavity was 44.7% compared to the negative control group after 4-day treatment with 100 mg/kg of nitrofurantoin. In addition, hematology indicators showed that T. gondii infection-induced serum alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels, biochemical parameters involved in liver injury, were reduced by nitrofurantoin significantly. Moreover, nitrofurantoin exerted significant effects on the index of antioxidant status, i.e., malondialdehyde (MDA) and glutathione (GSH). The nitrofurantoin-treated group inhibited the T. gondii-induced MDA levels while alleviating the decrease in GSH levels. Thus, nitrofurantoin is a potential anti-T. gondii candidate for clinical application.
Keywords: Toxoplasma gondii, nitrofurantoin, selectivity, therapeutic efficacy, mouse, HeLa cell
INTRUDUCTION
Toxoplasma gondii is the causative agent of toxoplasmosis, one of the most severe infectious diseases worldwide, and infects members of the Felidae family and a wide range of intermediate hosts, including warm-blooded animals and humans [1]. Toxoplasmosis can lead to a congenital disease and abortion in humans and domestic animals. In humans, the infection is usually subclinical; however, cervical lymphadenopathy or ocular disease can be present in some patients. Typical clinical symptoms of congenital toxoplasmosis, as proposed by Sabin in 1942 [2], include hydrocephalus or microcephalus, intracerebral calcification, and chorioretinitis. In addition, acquired toxoplasmosis can manifest itself in a variety of places, such as on lymph nodes, liver, heart, lungs, and skeleton [3].
After Sabin and Warren [4] reported the effectiveness of sulfonamides against murine toxoplasmosis, Eyles and Coleman [5] discovered the synergistic effect of combined therapy with sulfonamides and pyrimethamine, which has since been a standard treatment for toxoplasmosis in humans. Since 1958, when it was shown that spiramycin has anti-Toxoplasma activity in mice [6], it has been a recommended treatment for pregnant women, to reduce transmission of the parasite from mother to fetus [7]. In addition, clindamycin showed anti-Toxoplasma activity in conjunction with other drugs, especially in patients allergic to sulfonamides [8,9]. However, adverse effects of sulfadiazine plus pyrimethamine, or clindamycin plus pyrimethamine, such as skin rash, fever, and bone marrow suppression, are frequently observed [10-12]. Therefore, the development of alternative therapies with fewer allergic and adverse effects to treat toxoplasmosis is necessary.
Nitrofurantoin, (Z)-1-[(5-nitrofuran-2-yl)methyleneamino]-imidazolidine-2,4-dione (Fig. 1), is a newly synthesized derivative of imidazolidine-2,4-dione. Although it had been reported that imidazolidine-2,4-dione derivatives have biological activities in vitro and in vivo, their effects against T. gondii have not been investigated. Therefore, in the present study, nitrofurantoin was investigated for anti-T. gondii effects in vitro and in vivo.
Fig. 1.
The chemical structure of nitrofurantoin.
MATERIALS AND METHODS
Drugs and reagents
Nitrofurantoin and pyrimethamine were purchased from Sigma-Aldrich Chemical Co. (St. Louis, Missouri, USA). The CellTiter 96 AQueous One Solution Cell Proliferation Assay kit was purchased from Promega Corporation (Madison, Wisconsin, USA). All the sera, antibiotics, and RPMI 1640 for cell culture were obtained from Invitrogen (Grand Island, New York, USA). All the chemicals were of reagent grade.
Cell culture and T. gondii maintenance
HeLa cells were cultured in RPMI 1640 medium supplemented with 10% heat-inactivated fetal bovine serum, 100 units/ml penicillin, and 100 μl/ml streptomycin with 5% CO2 at 37˚C. T. gondii (RH strain) was maintained in female ICR mice (Koatech, Pyeongtaek, South Korea), and tachyzoites were obtained from peritoneal fluid.
Cell proliferation assay
A 3-(4,5-dimethylthiazol-zyl)-5-(3-carboxymethoxyphenyl)-2-(4-sulfophenyl)-2H-tetrazolium, inner salt (MTS) assay was used to determine cell proliferation by the CellTiter 96 AQueous One Solution Cell Proliferation Assay kit. HeLa cells were grown and infected with T. gondii for 24 hr in a 96-well microplate, and then treated with drugs. After 24 hr, 20 μl of MTS solution was added directly into culture wells, followed by incubating for 1.5 hr at 37˚C and measuring the absorbance at 490 nm in a microplate reader. Cell viability was expressed as a percentage of the control value.
Drug selectivity
Drug selectivity and individual effective concentrations (EC50) were determined as previously described [13]. For nitrofurantoin, the selectivity was calculated by the formula:
Selectivity=HeLa cell EC50/T. gondii EC50.
Animal treatment
Female ICR mice (6-week-old, 5 mice/group) were injected with 1×105 tachyzoites in the abdominal cavity. Mice were separated into 4 groups: normal (no T. gondii), negative control (T. gondii and water), positive control (T. gondii and pyrimethamine), and drug treated (T. gondii and nitrofurantoin). After infection for 2 hr, negative control, positive control, and drug-treated groups were administered 300 μl of water, pyrimethamine, or nitrofurantoin, respectively, once/day for 4 days. Animals were sacrificed 4 days post infection. Ascites fluid was drawn for determining tachyzoite proliferation. Spleens and livers were weighed and then lipid peroxidation (LPO) and glutathione (GSH) levels were measured in the livers.
LPO assay
LPO activity was measured by determining malondialdehyde (MDA) levels using thiobarbituric acid as described previously [14]. Liver homogenate was added to 0.2 ml of SDS (8.1%), 1.5 ml of thiobarbituric acid (0.67%), 1.5 ml of acetic acid (pH 3.5), and 0.6 ml of water. After incubation at 95˚C for 1 hr, it was cooled to room temperature. After adding 5 mk of n-butanol, the samples were centrifuged at 4,000 rpm for 10 min, and the absorbance of the organic layer was measured at 532 nm. Tetraethoxypropane was used in place of the liver homogenate for the standard.
GSH assay
Liver GSH was measured using an enzymatic recycling method [15]. The liver was pulverized in 8 ml of buffer (1 M HClO4 and 2 mM EDTA) using a Polytron homogenizer. The homogenate was centrifuged at 5,000 rpm for 5 min, and the supernatant was transferred to a semi-micro cuvette. Phosphate buffer (0.125 M phosphate, 6.3 mM EDTA, pH 7.5), NADPH (0.3 mM, 0.7 ml), and 5,5ʹ-dithio-bis-(2-nitrobenzoic acid) (6 mM, 0.1 ml) were then added to the supernatant, followed by mixing and incubating at room temperature for 4 min. Finally, glutathione reductase (50 units/ml) was added, and the absorbance was measured at 412 nm.
Alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels
Serum levels of AST and ALT were measured as previously described [16]. Briefly, ALT or AST substrate was incubated with serum at 37˚C for 30 min or 60 min, followed by the addition of 2,4-dinitrophenylhydrazine at room temperature for 20 min. NaOH was then added and the mixture incubated for 30 min followed by measuring the absorbance at 520 nm.
Statistical analysis
Statistical analysis was performed by the Student’s t-test. Differences were considered to be significant at P<0.05.
RESULTS
Selectivity of nitrofurantoin in vitro
In our study, the system for T. gondii drug screening has been used in vitro, which involved cell viability methods to calculate nitrofurantoin selectivity [13]. The selectivity reflects the efficacy of the test compound against T. gondii and toxicity for host cells. The selectivity of nitrofurantoin and pyrimethamine was measured in HeLa cells and was determined to be 2.3 and 0.9, respectively (Table 1). The effect of nitrofurantoin on cell proliferation after infection with T. gondii is shown in Fig. 2. Nitrofurantoin showed dose-dependent inhibition of T. gondii infection; concentrations of 5, 10, 20, and 40 μM resulted in 17, 30, 58, and 80% inhibition, respectively, compared to the negative-control group. In addition, the EC50 of nitrofurantoin against T. gondii was calculated to be 14.7 μM, and that for HeLa cells was 33.1 μM (data not shown). Nitrofurantoin had a higher selectivity than pyrimethamine, and showed good efficacy as an anti-T. gondii compound in vitro.
Table 1.
Selectivity of nitrofurantoin in HeLa cells
| EC50 in HeLa cells (μM) | EC50 in T. gondii (μM) | Selectivity | |
|---|---|---|---|
| Nitrofurantoin | 33.1 | 14.7 | 2.3 |
| Pyrimethamine | 760 | 850 | 0.9 |
Fig. 2.
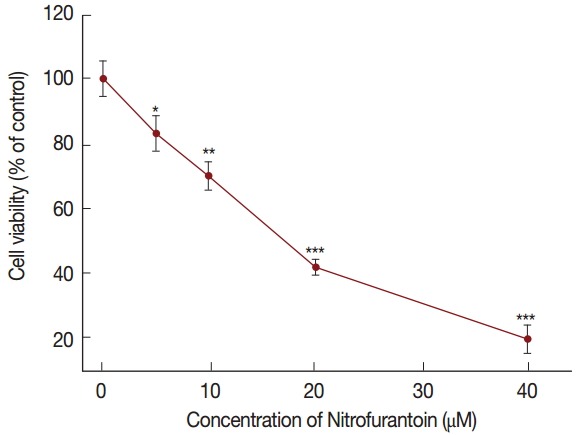
The effect of nitrofurantoin on cell proliferation after infection with T. gondii by MTS assay in HeLa cells. The data are presented as means±SD. The experiments were performed in triplicate. Statistical analysis was performed using the Student’s t-test. *P<0.05, **P<0.01, and ***P<0.001 were considered significant relative to the negative control.
Effect of nitrofurantoin on liver and spleen weights
The relative liver weight of all groups did not change significantly compared with the normal group, but that of the spleen was changed. Compared with the normal group, the relative spleen weight of the T. gondii-negative, nitrofurantoin, and pyrimethamine groups was significantly increased to 215, 147, and 214%, respectively. When the nitrofurantoin group was compared to the T. gondii-negative group, these increases were reduced to 43%, whereas pyrimethamine did not show this effect.
Therapeutic efficacy of nitrofurantoin against T. gondii in vivo
Our in vivo model used 6-week-old mice; however, 4-week-old mice were used in our previous study [17], and we therefore repeated the determination of the optimal dose of the positive-control compound, pyrimethamine, for this study. We found 20 mg/kg pyrimethamine to be an optimally effective and safe dose (data not shown). Mice were sacrificed 4 days post infection, and ascites fluid was used to determine tachyzoite proliferation. The dose-dependent effects of nitrofurantoin (orally 20, 50, and 100 mg/kg) in mice were first examined. The lower concentrations, 20 and 50 mg/kg, of nitrofurantoin did not show any anti-T. gondii effect in the peritoneal cavity, whereas 100 mg/kg dose significantly reduced the tachyzoite number in the peritoneal cavity (Fig. 3). Based on these results, 20 mg/kg pyrimethamine and 100 mg/kg nitrofurantoin were used in our in vivo experiment, even though the nitrofurantoin concentration was higher than that of pyrimethamine. The numbers of tachyzoites in the peritoneal cavity of T. gondii-negative group, pyrimethamine-treated positive group, and nitrofurantoin-treated group were 105.7, 22.9, 104.8, 94.5, and 58.5 (×106), respectively. The inhibition rate of T. gondii growth in the peritoneal cavity was significantly different (44.7%) compared to the negative group after treatment with 100 mg/kg nitrofurantoin. However, this inhibition was not significantly better than that of the group with 20 mg/kg pyrimethamine treatment (78.3%). These results suggested that nitrofurantoin produced a good anti-T. gondii effect in mouse peritoneal cavities.
Fig. 3.
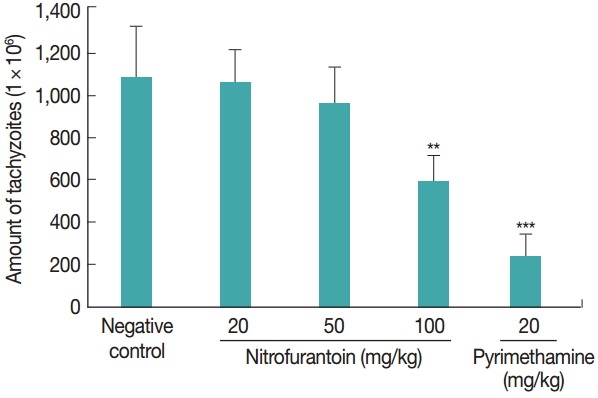
Number of tachyzoites in the mouse peritoneal cavity. After mice were infected with T. gondii (105/mouse) for 2 hr, the negative-control, positive-control, and nitrofurantoin-treated groups were treated orally by gavage once per day for 4 days with water, 20 mg/kg pyrimethamine, or nitrofurantoin (20, 50, and 100 mg/kg), respectively. All mice were sacrificed 4 days post infection, and tachyzoites were harvested from peritoneal cavities (5 mice/group). **P<0.01 and ***P<0.001 were considered significant compared to the negative control.
Effect of nitrofurantoin on ALT and AST levels in T. gondii-infected mice
During natural infections, T. gondii initially crosses the intestinal epithelium, disseminates into deep tissues, and enters the circulation, which leads to hepatotoxicity and increase in serum AST and ALT levels. The serum ALT and AST levels, which indicate hepatotoxicity, are shown in Fig. 4. AST and ALT levels were elevated in the negative group and nitrofurantoin-treated group, as compared with the normal group (Fig. 4). The AST (53%) and ALT (51%) levels were reduced significantly after nitrofurantoin was administered to the negative group, although their levels were not significantly less than those in the pyrimethamine group.
Fig. 4.
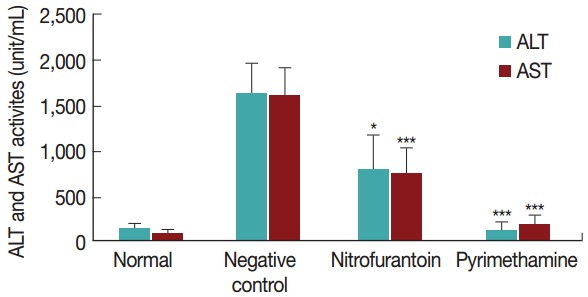
Serum alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels in ICR mice after treatment with T. gondii, nitrofurantoin, and pyrimethamine. Mice received an abdominal cavity injection with tachyzoites. After infection for 2 hr, negative-control, positive-control, and drug-treated groups were orally administered 300 μl water, pyrimethamine, and nitrofurantoin, respectively, once per day for 4 days. The serum levels of AST and ALT were determined by a colorimetric assay. The values are means±SD (n=5), and the data were analyzed by Student’s t-test. *P<0.05 and ***P<0.001 were considered significant relative to the negative-control group.
Effect of nitrofurantoin on MDA levels in T. gondii-infected livers
To observe the effects of nitrofurantoin on cell damage, malondialdehyde (MDA), which is a product of LPO and an index of oxidative damage, was assayed by using thiobarbituric acid. The MDA level was significantly decreased to 52% compared with the negative group when treated with 100 mg/kg nitrofurantoin (Fig. 5), which is similar to that observed in the pyrimethamine group.
Fig. 5.
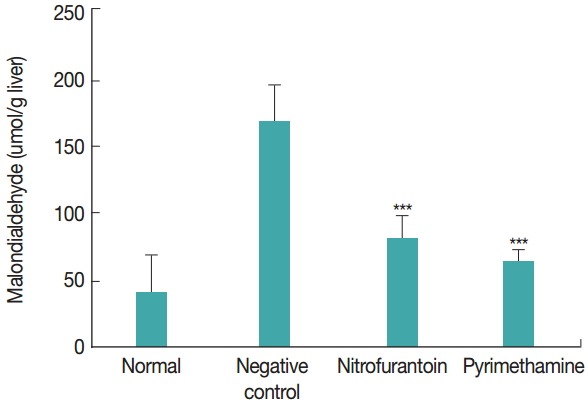
Effects of nitrofurantoin on malondialdehyde levels in livers of female ICR mice. The malondialdehyde content of the liver was determined after 4 days of treatment. The values are means±SD (n=5), and the data were analyzed by Student’s t-test. ***P<0.001 was considered significant relative to the negative-control group.
Effect of nitrofurantoin on GSH levels in T. gondii-infected livers
We also measured the level of GSH, one of the most important antioxidant molecules in the liver. The normal GSH level was usually maintained at about 6.61±1.23 μmol/g, but the infected group showed a 65% decrease to about 4.32±1.55 μmol/g, compared to the normal group. However, the GSH level of the nitrofurantoin-treated group significantly increased by 30% compared to that of the negative group (Fig. 6).
Fig. 6.
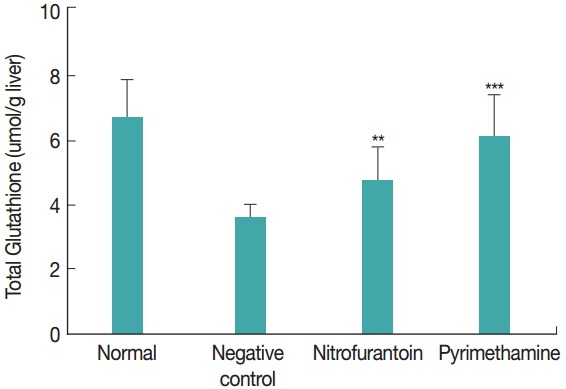
Effects of nitrofurantoin on glutathione levels in the livers of female ICR mice. The total glutathione content of the liver was determined after 4 days of treatment. The values are means±SD (n=5), and the data were analyzed by Student’s t-test. **P<0.01 and ***P<0.001 were considered significant compared with the negative-control group.
DISCUSSION
It is well known that standard treatment of toxoplasmosis is usually accompanied with severe side effects; thus, identification of alternative therapeutic compounds is urgently needed. In the present study we evaluated the efficacy and toxicity of a new synthetic imidazolidine-2,4-dione derivative, nitrofurantoin, in vitro and in vivo. It had been reported that many imidazolidine-2,4-dione derivatives have biological activities in vitro and in vivo. Some investigators have found that imidazolidine-2,4-dione derivatives exhibit potential antidepressant activity with a mechanism different from that of the tricyclic antidepressants and monoamine oxidase inhibitors[18], and exert an inhibitory effect against the central nervous system, including anxiety-relieving, anticonvulsant, and anti-depressive effects [19]. In addition, some of these derivatives have shown antiarrhythmic activity in chloroform-, barium chloride-, or adrenaline-induced arrhythmia [20]. Moreover, these derivatives have been shown to selectively inhibit human heart chymase [21], and some were identified as fatty acid amide hydrolase inhibitor templates [22], as novel antitumor agents [23], and as potent radiosensitizing agents [24]. However, there have been no studies of nitrofurantoin, especially concerning its anti-T. gondii activities.
In our study, we have developed a simple high-throughput assay for in vitro drug screening [13], which is fast, simple, and effective, compared with other reported methods. The inhibition of the in vitro infection rate of host cells (EC50) was determined by the MTS assay to calculate drug selectivity. These measurements reflected the efficacy of nitrofurantoin against T. gondii and toxicity for host cells.
In the current study, nitrofurantoin displayed higher selectivity than pyrimethamine in vitro. In contrast, the pyrimethamine inhibition rate was higher than that of nitrofurantoin in vivo. This discrepancy may be because the clinical parameters of pyrimethamine for use against T. gondii have been optimized, such as its concentration and side effects.
Pyrimethamine is known to have antimalarial activities and is used clinically in the therapy of toxoplasmosis and human immunodeficiency virus-associated pneumonia. For adults, pyrimethamine is administered at 25 mg per day for 3-4 weeks, whereas children are administered 2 mg/kg/day for 3 days, and then 1 mg/kg/day (maximum 25 mg/day) for 4 weeks. In animal models, one study reported using a combination of dapsone and pyrimethamine in which pyrimethamine was administered at 18.5 mg/kg/day [25]; however, this dosage was previously reported to be non-curative against T. gondii infection [26]. It has been reported that 12.5 mg/kg of pyrimethamine inhibited the growth of tachyzoites by about 55.5% in 4 days [17]. This result is consistent with the present study in that 20 mg/kg of pyrimethamine inhibited the growth of tachyzoites by 78.3%.
Toxoplasmosis causes liver pathologies [27], and the significant agreement of serologically positive cases with elevated plasma AST and ALT has been reported [28]. A decrease in GSH activity was detected, while an increase of MDA was observed in T. gondii-infected patients [29]. Therefore, we assessed the plasma activities of ALT, AST, GSH, and MDA in T. gondi-iinfected liver homogenates to compare the efficacy of nitrofurantoin to that of pyrimethamine. Previously, we found that 6-trifluoromethyl-2-thiouracil, a potent anti-T.gondii compound, could recover ALT, AST, and MDA to normal level in T. gondii-infected mice but it could not increase the T. gondii- reduced GSH level [30].
In summary, nitrofurantoin showed good anti-toxoplasmosis effects in T. gondii-infected mice. Furthermore, it showed effective protection against T. gondii-induced damage in the liver, similar to that of pyrimethamine. Thus, nitrofurantoin is a potentially useful anti-T. gondii candidate drug that could have a therapeutic value for the treatment of toxoplasmosis. Additional studies are needed to determine the pharmacological indices of nitrofurantoin, such as the side effects and chronic toxicity.
Acknowledgments
This research was supported by Priority Research Centers Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, (NRF-2015 R1A6A1A03032236).
Footnotes
We have no conflict of interest related to this work.
REFERENCES
- 1.Tenter AM. Toxoplasma gondii in animals used for human consumption. Mem Inst Oswaldo Cruz. 2009;104:364–369. doi: 10.1590/s0074-02762009000200033. [DOI] [PubMed] [Google Scholar]
- 2.Sabin AB, Feldman HA. Chorioretinopathy associated with other evidence of cerebral damage in childhood; a syndrome of unknown etiology separable from congenital toxoplasmosis. J Pediatr. 1949;35:296–309. doi: 10.1016/s0022-3476(49)80002-3. [DOI] [PubMed] [Google Scholar]
- 3.Dubey JP, Zarnke R, Thomas NJ, Wong SK, Van Bonn W, Briggs M, Davis JW, Ewing R, Mense M, Kwok OC, Romand S, Thulliez P. Toxoplasma gondii, Neospora caninum, Sarcocystis neurona, and Sarcocystis canis-like infections in marine mammals. Vet Parasitol. 2003;116:275–296. doi: 10.1016/s0304-4017(03)00263-2. [DOI] [PubMed] [Google Scholar]
- 4.Sabin AB, Warren J. Therapeutic effectiveness of certain sulfonamide on infection by an intracellular protozoon (Toxoplasma) Proc Soc Exp Biol Med. 1942;51:19–23. [Google Scholar]
- 5.Eyles DE, Coleman N. The effect of metabolites on the antitoxoplasmic action of pyrimethamine and sulfadiazine. Am J Trop Med Hyg. 1960;9:277–283. doi: 10.4269/ajtmh.1960.9.277. [DOI] [PubMed] [Google Scholar]
- 6.Garin JP, Eyles DE. Le traitement de la toxoplasmose experimentale de la souris par la spiramycine. Presse Medicale. 1958;66:957–958. [PubMed] [Google Scholar]
- 7.Desmonts G, Couvreur J. Toxoplasmosis in pregnancy and its transmission to the fetus. Bull N Y Acad Med. 1974;50:146–159. [PMC free article] [PubMed] [Google Scholar]
- 8.Dubey JP, Velmurugan GV, Ulrich V, Gill J, Carstensen M, Sundar N, Kwok OC, Thulliez P, Majumdar D, Su C. Transplacental toxoplasmosis in naturally-infected white-tailed deer: isolation and genetic characterisation of Toxoplasma gondii from foetuses of different gestational ages. Int J Parasitol. 2008;38:1057–1063. doi: 10.1016/j.ijpara.2007.11.010. [DOI] [PubMed] [Google Scholar]
- 9.Araujo FG, Remington JS. Effect of clindamycin on acute and chronic toxoplasmosis in mice. Antimicrob Agents Chemother. 1974;5:647–651. doi: 10.1128/aac.5.6.647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Dannemann B, McCutchan JA, Israelski D, Antoniskis D, Leport C, Luft B, Nussbaum J, Clumeck N, Morlat P, Chiu J, Vilde JL, Orellana M, Feigal D, Bartok A, Heseltine P, Leedom J, Remington J. Treatment of toxoplasmic encephalitis in patients with AIDS. A randomized trial comparing pyrimethamine plus clindamycin to pyrimethamine plus sulfadiazine. Ann Intern Med. 1992;116:33–43. doi: 10.7326/0003-4819-116-1-33. [DOI] [PubMed] [Google Scholar]
- 11.Georgiev VS. Management of toxoplasmosis. Drugs. 1994;48:179–188. doi: 10.2165/00003495-199448020-00005. [DOI] [PubMed] [Google Scholar]
- 12.Luft BJ, Remington JS. Toxoplasmic encephalitis in AIDS. Clin Infect Dis. 1992;15:211–222. doi: 10.1093/clinids/15.2.211. [DOI] [PubMed] [Google Scholar]
- 13.Jin C, Kaewintajuk K, Jiang J, Jeong W, Kamata M, Kim HS, Wataya Y, Park H. Toxoplasma gondii: a simple high-throughput assay for drug screening in vitro. Exp Parasitol. 2009;121:132–136. doi: 10.1016/j.exppara.2008.10.006. [DOI] [PubMed] [Google Scholar]
- 14.Ohkawa H, Ohishi N, Yagi K. Assay for lipid peroxides in animal tissues by thiobarbituric acid reaction. Anal Biochem. 1979;95:351–358. doi: 10.1016/0003-2697(79)90738-3. [DOI] [PubMed] [Google Scholar]
- 15.Griffith OW. Determination of glutathione and glutathione disulfide using glutathione reductase and 2-vinylpyridine. Anal Biochem. 1980;106:207–212. doi: 10.1016/0003-2697(80)90139-6. [DOI] [PubMed] [Google Scholar]
- 16.Reitman S, Frankel S. A colorimetric method for the determination of serum glutamic oxalacetic and glutamic pyruvic transaminases. Am J Clin Pathol. 1957;28:56–63. doi: 10.1093/ajcp/28.1.56. [DOI] [PubMed] [Google Scholar]
- 17.Jiang JH, Jin CM, Kim YC, Kim HS, Park WC, Park H. Anti-toxoplasmosis effects of oleuropein isolated from Fraxinus rhychophylla. Biol Pharm Bull. 2008;31:2273–2276. doi: 10.1248/bpb.31.2273. [DOI] [PubMed] [Google Scholar]
- 18.Wessels FL, Schwan TJ, Pong SF. Synthesis and antidepressant activity of 5-(4-dimethylaminobenzyl)imidazolidine-2,4-dione. J Pharm Sci. 1980;69:1102–1104. doi: 10.1002/jps.2600690933. [DOI] [PubMed] [Google Scholar]
- 19.Zejc A, Kiec-Kononowicz K, Chlon G, Kleinrok Z, Kolasa K, Pietrasiewicz T, Czechowska G. Synthesis and pharmacological properties of diphenylimidazolidine acetic and propionic acids derivatives. Pol J Pharmacol Pharm. 1989;41:483–493. [PubMed] [Google Scholar]
- 20.Kiec-Kononowicz K, Byrtus H, Zejc A, Filipek B, Chevallet P. Synthesis and antiarrhythmic properties of basic amide derivatives of imidazolidine-2,4-dione and pyrrolidine-2,5-dione II. Farmaco. 1995;50:355–360. [PubMed] [Google Scholar]
- 21.Niwata S, Fukami H, Sumida M, Ito A, Kakutani S, Saitoh M, Suzuki K, Imoto M, Shibata H, Imajo S, Kiso Y, Tanaka T, Nakazato H, Ishihara T, Takai S, Yamamoto D, Shiota N, Miyazaki M, Okunishi H, Kinoshita A, Urata H, Arakawa K. Substituted 3-(phenylsulfonyl)-1-phenylimidazolidine-2,4-dione derivatives as novel nonpeptide inhibitors of human heart chymase. J Med Chem. 1997;40:2156–2163. doi: 10.1021/jm960793t. [DOI] [PubMed] [Google Scholar]
- 22.Muccioli GG, Fazio N, Scriba GK, Poppitz W, Cannata F, Poupaert JH, Wouters J, Lambert DM. Substituted 2-thioxoimidazolidin-4-ones and imidazolidine-2,4-diones as fatty acid amide hydrolase inhibitors templates. J Med Chem. 2006;49:417–425. doi: 10.1021/jm050977k. [DOI] [PubMed] [Google Scholar]
- 23.Mukherjee A, Dutta S, Chashoo G, Bhagat M, Saxena AK, Sanyal U. Evaluation of fluoren-NU as a novel antitumor agent. Oncol Res. 2009;17:387–396. doi: 10.3727/096504009788912516. [DOI] [PubMed] [Google Scholar]
- 24.Reddy YT, Sekhar KR, Sasi N, Reddy PN, Freeman ML, Crooks PA. Novel substituted (Z)-5-((N-benzyl-1H-indol-3-yl)methylene)imidazolidine-2,4-diones and 5-((N-benzyl-1H-indol-3-yl) methylene)pyrimidine-2,4,6(1H,3H,5H)-triones as potent radio-sensitizing agents. Bioorg Med Chem Lett. 2010;20:600–602. doi: 10.1016/j.bmcl.2009.11.082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Derouin F, Piketty C, Chastang C, Chau F, Rouveix B, Pocidalo JJ. Anti-Toxoplasma effects of dapsone alone and combined with pyrimethamine. Antimicrob Agents Chemother. 1991;35:252–255. doi: 10.1128/aac.35.2.252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Piketty C, Derouin F, Rouveix B, Pocidalo JJ. In vivo assessment of antimicrobial agents against Toxoplasma gondii by quantification of parasites in the blood, lungs, and brain of infected mice. Antimicrob Agents Chemother. 1990;34:1467–1472. doi: 10.1128/aac.34.8.1467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Roca B, Calabuig C, Arenas M. Toxoplasmosis and hepatitis. Med Clin (Barc) 1992;99:595–596. (in Spanish) [PubMed] [Google Scholar]
- 28.Yarim GF, Nisbet C, Oncel T, Cenesiz S, Ciftci G. Serum protein alterations in dogs naturally infected with Toxoplasma gondii. Parasitol Res. 2007;101:1197–1202. doi: 10.1007/s00436-007-0601-0. [DOI] [PubMed] [Google Scholar]
- 29.Karaman U, Celik T, Kiran TR, Colak C, Daldal NU. Malondialdehyde, glutathione, and nitric oxide levels in Toxoplasma gondii seropositive patients. Korean J Parasitol. 2008;46:293–295. doi: 10.3347/kjp.2008.46.4.293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Choi HJ, Yu ST, Lee KI, Choi JK, Chang BY, Kim SY, Ko MH, Song HO, Park H. 6-trifluoromethyl-2-thiouracil possesses anti-Toxoplasma gondii effect in vitro and in vivo with low hepatotoxicity. Exp Parasitol. 2014;143:24–29. doi: 10.1016/j.exppara.2014.05.002. [DOI] [PubMed] [Google Scholar]