

Abstract
Objective
Dermoid and epidermoid cysts are rare cysts of the head and neck region, which should be considered in differential diagnosis of sublingual mass, constituting 0.01 % of all oral cavity cysts. There are suspected theories regarding the basis of the pathology.
Case Report
30-year-old male referred to our clinic with a chief complaint of sublingual mass which had been present for many years but the lesion enlarged over the past 3 years. MRI examination revealed a giant cystic mass which was 3.6 × 3.9 mm in diameter and medially located at sublingual region.
Treatment and Prognosis
Intraoral approach was preferred for surgery and no recurrence or complaints were detected during follow-up period.
Conclusion
When a cystic mass is detected on the floor of oral cavity, we must consider dermoid cysts for differential diagnosis. Surgery is the only treatment. If possible, intraoral approach should be preferred because of its perfect cosmetic results.
Keywords: Dermoid, Epidermoid cysts, Sublingual, Intraoral approach, Giant
Introduction
Dermoid and epidermoid cysts are benign lesions that can be seen all over the body. They constitute 7 % of all cysts in the head–neck region. Of those, only 1.6 % are located in the oral cavity [1–5]. The exact pathogenesis of the cyst is not known but dysontogenic and thyroglossal anomaly theories are accused [6]. The difference between dermoid and epidermoid cysts is that epidermoid cysts are lined with epithelium but dermoid cysts have skin appendages such as gland and hair. Clinically most of the dermoid cysts are presented by slowly and progressively growing masses. If congenital, they are detected in the 2nd and 3rd decades of life. Depending on the size of the mass, dermoid cysts cause swallowing, speaking and respiratory problems.
The main treatment modality is surgery via extraoral or intraoral approach according to the size and location of the mass. Dermoid cysts are classified according to their location as submental, sublingual and submandibular. Intraoral approach is chosen in the literature usually for small and sublingual dermoid cysts. Extraoral approach is preferred for large and submandibular cysts.
We present a giant (larger than 6 cm) dermoid cyst located in sublingual region which was surgically excised by intraoral approach.
Case Report
A 30-year-old male patient was admitted to our department with a mass on the sublingual region. The lesion had been present for many years but the lesion enlarged over the past 3 years. The patient had no complaints except the mass. There was no history of trauma and surgery at head and neck region. Physical examination of the patient revealed a palpable, well-demarcated swelling at the sublingual region, which was 4 cm in diameter (Fig. 1). The sublingual cystic lesion was visible in the oral cavity. The tongue movements were intact. T2-weighted images of the neck revealed a hyperintense, medially located, cystic mass, which was 36 × 39 mm in diameter (Fig. 2).
Fig. 1.

Anteroposterior and lateral views of the patient preoperatively
Fig. 2.

MRI examination shows of the huge dermoid cyst located in sublingual region
After obtaining informed consent, intraoral approach was preferred for the excision of the dermoid cyst. Following nasotracheal intubation under general anesthesia, the Wharton ducts were identified and protected. Approximately 8 cm oral incision was used and the cyst cavity was detected submucosally. The cyst was then carefully dissected sharply and bluntly from the surrounding tissue. Finally the cyst was separated from mylohyoid and geniohyoid muscles and specimen was sent for pathology. The skin incision was closed in layers (Fig. 3).
Fig. 3.

Intraorally excised en-bloc surgical specimen compared to the tongue and lips
Macroscopically, surgical specimen was 12 × 5 × 4 cm in size (Fig. 4). Histopathologically, cystic structure lined with squamous epithelium and its lumen containing keratinous material was noted. Sebaceous gland connected with squamous epithelium was seen in one area (Fig. 5). The patient did well postoperatively and no recurrence was noticed during 6-months follow-up period (Fig. 6).
Fig. 4.

A giant surgical specimen and its contents
Fig. 5.
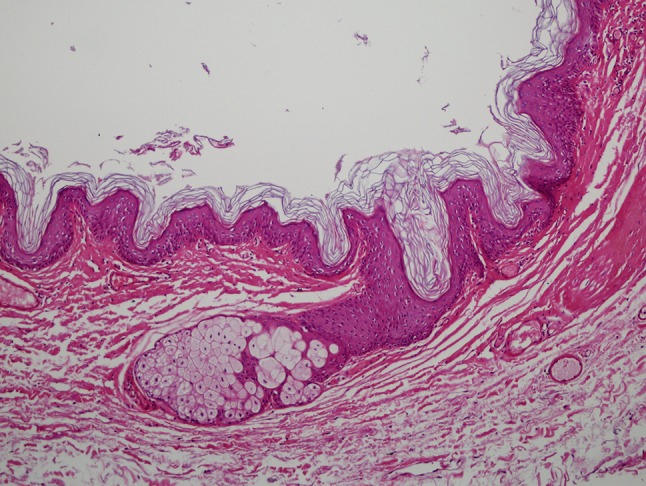
Cystic structure lined with squamous epithelium and its lumen containing keratinous material. Sebaceous gland connected with squamous epithelium in one area (HE × 100)
Fig. 6.

Anteroposterior and lateral views of the patient postoperatively
Discussion
Dermoid and epidermoid cysts of the oral cavity are rare lesions that consist of less than 0.01 % of the oral cavity cysts [1–6]. Epidermoid cysts are merely lined with epithelium; on the other hand, dermoid cysts have the skin adventia [7]. Dermoid cysts of the oral cavity floor are dysembryonic lesions that are formed by growth and entrapment of epithelial cells during fusion between first and second branchial arches in the 3rd and 4th embryonic week [7]. Also dermoid cysts might be caused by iatrogenic or traumatic route through inclusion of the epithelium and skin appendages [6, 7]. Dermoid cysts are mostly diagnosed by the 2nd and 3rd decades of life. Patients can be presented by dysphagia, dysphonia and speaking problems according to the size and location of the mass.
Anatomically the cysts can be divided into three regions as sublingual, submental and lateral. Lateral eyebrow is the most common site for dermoid cysts located on the head and neck region. Second zone is the floor of the oral cavity. Differential diagnosis includes infections, ranula, lymphadenopathies, duplication foregut cysts [1–6].
Imaging procedures such as MRI help us to identify the cyst and its relationship between geniohyoid and mylohyoid muscles. Also this information clarifies the surgical approach. Fine needle aspiration biopsy is beneficial for the diagnosis. Treatment of the cysts is surgical via extraoral or intraoral approach. Some authors claim that lesions that are less than 6 cm in diameter and above the mylohoid muscle are suitable for intraoral excision. Also they claim that dermoid cysts larger than 6 cm in diameter and located sublingually should be excised by extraoral approach [8].
In our case the dermoid cyst was larger than 6 cm in diameter. According to the literature, our case was one of the biggest lesions that was excised by intraoral approach. Although the lesion was very large, we had chosen the intraoral approach. We believe that sufficient traction and counter traction, and precise dissection of the anatomically sensitive regions allowed successful results for intraoral approach. We must keep in mind that intraoral approach provides excellent cosmetic results. If the surgeon is tolerant and evaluation of the patient is sufficient enough, intraoral approach can be chosen for all sizes of the oral cavity dermoid cysts.
Conclusion
Dermoid and epidermoid cysts are benign lesions that can be seen on the floor of the oral cavity. When a cystic mass is detected on the floor of oral cavity, we must consider dermoid cysts for differential diagnosis. Surgery is the only treatment. If possible, intraoral approach should be preferred because of its perfect cosmetic results.
Compliance with Ethical Standards
Conflict of interest
All the authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from participant included in the study.
References
- 1.Kim IK, Kwak HJ, Choi J, Han JY, Park SW. Coexisting sublingual and submental dermoid cysts in an infant. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. 2006;102:778–781. doi: 10.1016/j.tripleo.2005.09.016. [DOI] [PubMed] [Google Scholar]
- 2.Longo F, Maremonti P, Mangone GM, De Maria G. Midline (dermoid) cysts of the floor of the mouth: report of 16 cases and review of surgical techniques. Plast Reconstr Surg. 2003;112:1560–1565. doi: 10.1097/01.PRS.0000086735.56187.22. [DOI] [PubMed] [Google Scholar]
- 3.MacNeil SD, Moxham JP. Review of floor of mouth dysontogenic cysts. Ann Otol Rhinol Laryngol. 2010;119:165–173. doi: 10.1177/000348941011900304. [DOI] [PubMed] [Google Scholar]
- 4.Turetschek K, Hospodka H, Steiner E. Case report: epidermoid cyst of the floor of the mouth: diagnostic imaging by sonography, computed tomography and magnetic resonance imaging. Br J Radiol. 1995;68:205–207. doi: 10.1259/0007-1285-68-806-205. [DOI] [PubMed] [Google Scholar]
- 5.De Ponte FS, Brunelli A, Marchetti E, Bottini DJ. Sublingual epidermoid cyst. J Craniofac Surg. 2002;13:308–310. doi: 10.1097/00001665-200203000-00024. [DOI] [PubMed] [Google Scholar]
- 6.Kandogan T, Koc M, Vardar E, Sezgin O, Selek E. Sublingual epidermoid cyst: a case report. J Med Case Rep. 2007;1:87. doi: 10.1186/1752-1947-1-87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Meyer I. Dermoid cysts (dermoids) of the floor of the mouth. Oral Surg Oral Med Oral Pathol. 1955;8:1149–1164. doi: 10.1016/0030-4220(55)90380-7. [DOI] [PubMed] [Google Scholar]
- 8.El-Hakim IE, Alyamani A. Alternative surgical approaches for excision of dermoid cyst of the floor of mouth. Int J Oral Maxillofac Surg. 2008;37:497–499. doi: 10.1016/j.ijom.2007.12.004. [DOI] [PubMed] [Google Scholar]