

Abstract
The increase in the growth of the elderly population in the past 2 decades has been paralleled by an increase in the number of active elderly drivers. Consequentially, this growth has been accompanied by a rise in fatal road-related accidents. Due to age-related fragility, elderly drivers are more susceptible to injuries and death following a road-related accident. The increased risk of accidents has become a growing public health issue and has led to certain guidelines and restrictions for elderly drivers. Moreover, the cognitive and physiological decline that exacerbates with age has encouraged preventative measures aimed at optimizing their ability to operate motor vehicles. Some of these include yearly vision, cognitive, motor, and mental assessment tests. Results obtained from these tests may help suggest when an elderly driver becomes unsuitable to drive.
Keywords: geriatric medicine, geriatric trauma, fragility fractures, systems of care, dementia
Introduction
In the past 2 decades, the geriatric population has experienced a growth increase that has outpaced that of any other group, and experts project that approximately 20% of the population will be considered elderly by 2030.1 It is estimated that more than 40 million individuals in the United States are at least 65 years of age, representing the fastest growing group in the country.1,2 This growth in the elderly population corresponds with the increase in the number of elderly drivers, with an estimated 36 million who currently hold an active drivers’ license.3 These drivers are more likely to require medical attention, use medical facilities, and are at a higher risk for sustaining motor vehicle injuries.4 Compared to individuals in their 40s, those between ages 65 and 69 and over the age of 85 are 1.29 and 3.74 times more likely to be involved in fatal car accidents, respectively.4,5 This increased likelihood of death following a vehicular accident is attributed to progressive age-related fragility. Other statistics also highlight road-related hazards such as the increased risk of injuries and mortality for other drivers and vehicle occupants.6 Moreover, studies have shown a rise in accidents (178%) and fatalities (158%) involving elderly individuals, and have projected a 40% increase in motor vehicle accidents and 50% increase in mortality over the next few years.7 Taken together, these projections emphasize a major public health concern regarding elderly drivers.
Recommendations made by health professionals have led to the placement of certain restrictions on elderly drivers to foster a safer driving environment for drivers and passengers alike. They include visual acuity screening, cognitive and mental health assessments, and muscle evaluations.8 Some limitations can include area (ie, no freeway driving), distance, time, and placement of special mechanical equipment to aid driving. No single assessment can reveal when elderly patients should stop driving.
Risks and Assessments for Elderly Drivers
Although the majority of motor vehicle accidents involve teenage drivers, road-related fatalities are highest among the elderly population.9 Furthermore, the fatality rates for elderly drivers over 85 years are 5 times more than teenagers.9 Age-related fragility greatly contributes to the increased risk and susceptibility to sustain fatal injuries. The most common injuries sustained from accidents involve regions of the head and neck, chest, pelvic area, and extremities.4,9 The most prevalent chest injuries include the pleura, lungs, and rib fractures.4,9 Although some sustained injuries are not immediately fatal, the associated complications typically have poor prognoses.9,10
Age-related physiological and mental decline has led to medical guidelines to assess the ability of elderly drivers to operate motor vehicles. Suboptimal results may lead to temporary or permanent revocation of the driver’s license. Annual vision screenings are also recommended. The most prevalent causes of visual deterioration and blindness for the elderly population include cataracts, glaucoma, and macular degeneration.11,12 More than 1 million elderly individuals are considered blind, whereas another 2.4 million have poor vision.12 The Snellen test is widely used to assess visual acuity13 (Figure 1). Individuals are asked to stand within a set distance (usually 20 ft) and identify letters arranged in rows. Normal vision is reported as 20/20, and an individual is considered blind with a score of 20/200. Vision beyond 20/50 (ie, 20/60, 20/80) is considered impaired,13 possibly justifying suspension of driving until visual defects are corrected.
Figure 1.
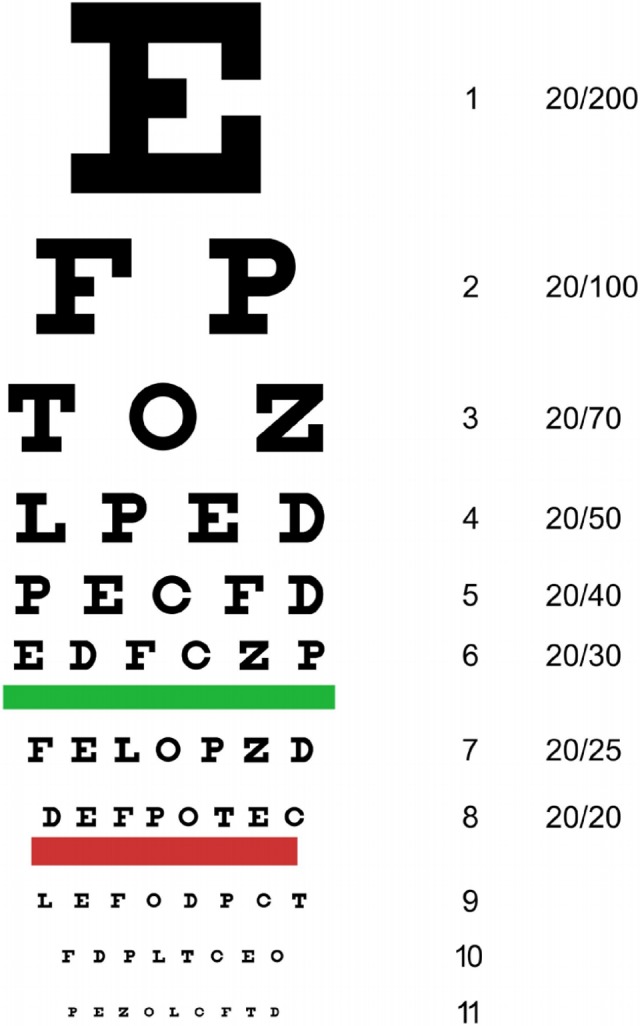
Snellen chart (visual acuity test).
Cognitive impairments can increase reaction times and compromise judgment. These impairments are often characteristic of aging and may result from dementia, seizures, and strokes.14,15 Since 2011, all Medicare beneficiaries under the Affordable Care Act are recommended to attend the Medicare Annual Wellness where their cognitive abilities can be assessed as well.16 This includes assessments by both the patient and their family members. For the patient, typical cognitive assessments include the General Practitioner Assessment of Cognition, Mini-Cog, and Memory Impairment Screen.16 For family members, the short Informant Questionnaire on Cognitive Decline in the Elderly is administered.16 No single tool can best assess cognitive function, therefore, a combination of several tests is typically used. Failed assessments prompt further evaluation by a specialist to definitively diagnose cognitive decline.
Physical weakness and fatigue are among the top complaints of the elderly patients.17 Muscle weakness is a possible cause due to the age-related decrease in muscle mass and function. Wrist and hand movements are important to perform steering maneuvers among other manual functions. Also, foot maneuvers such as plantar flexion and dorsiflexion are important for successful accelerating and braking. Muscle testing is an important aspect of the annual physical checkup and is commonly performed using manual muscle testing techniques—methods found to be reliable for testing age-related muscle weakness.18 In this series of tests, individual hands, arms, legs, and feet are tested separately against gravity and resistance for strength and durability.
Health-Care Costs and Associated Challenges
Costs surrounding elderly drivers are substantial primarily due to their rate of hospitalization.4,19 More than any other group, the elderly population are more likely to become hospitalized and have traumatic and deliberating injuries associated with vehicular collisions.4,19 Despite only comprising 13% of the nation’s population, they account for nearly 36% of all health-care expenditures.19 The number of procedures performed on the elderly population exceeds that of any other group. Regarding litigation, they are more often found to be at fault in vehicular accidents.20
The elderly population also face challenges beyond the potential physical harm and financial constraints suffered from vehicular accidents. The loss of independence and autonomy when forced to give up driving (for health or other reasons) is a commonly reported challenge.21,22 Moreover, it leads to an overall decrease in quality of life and increased dependency on others. Drivers who have strokes or seizures are temporarily suspended from driving until their symptoms improve, which can take up to a year before clearance to resume driving. To circumvent this problem, some elderly drivers elect to avoid screening tests and exams in fear of losing their ability to drive.22 To combat this, Foley et al recommended updating license renewal guidelines for elderly drivers.23 Currently, elderly drivers are required to renew their license generally every 5 years in some states, and the proposal to reduce this number remains an area of debate.
Another challenge involves restricting the driving area. For example, elderly drivers are recommended to avoid freeways, winter driving, nighttime driving, and are advised to drive shorter distances. Some drivers proactively limit themselves from driving under certain conditions.
The Decision-Making Process and Beyond
When subpar results are obtained from the physical and mental assessments, physicians and other health-care professionals should discuss these results with family members to explore available courses of action. Likewise, relatives of elderly individuals should inform their health-care providers regarding any observed mental or physical changes that may impair driving abilities. Programs aimed at rehabilitative efforts to help older drivers can be recommended. For example, the “Mature Driver Program” from the American Automobile Association (AAA)24 and the “Driver Safety Program” by the American Association for Retired Persons (AARP)25 are both designed to safely keep elderly drivers on the road. Another program by the AAA, the “Flexibility Fitness Program” uses occupation therapist to work with elderly drivers to improve physical fitness and motion to reduce the risk of injuries.26 Physicians can also refer patients directly to occupational or physical therapists for evaluation, rehabilitation, and to create individualized plans. Less formal programs such as personalized fitness training or fitness classes are also available and can be beneficial to elderly individuals. There are no objective data outlining physiological parameters that make the greatest difference in safe driving. However, criteria for driving evaluation used by the New York State’s Department of Motor Vehicle (DMV) include visual, hearing, reaction abilities, perception of speed and distance.27 Following participation in these programs, the patients are reevaluated and results are sent to the DMV, which can either lead to extension, suspension, or revocation of driver’s license.27
Conclusion
The incidence of accidents caused by, or involving, elderly drivers continues to rise. In response, steps have been taken to ensure that driving capacity is maintained with age. The increase in age generally correlates with decrease in functionality, and elderly drivers commonly experience physiological and mental changes that may deem them unsuitable for driving and hazardous to other drivers. The substantial cost of care associated with caring for geriatric patients also necessitates preventative measures that include visual, cognitive, and mental health screenings. Physicians, physical therapist, and occupational therapists can recommend both established and less formal programs and work together with patients to find appropriate solutions that are beneficial for them.
Footnotes
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Braver ER, Trempel RE. Are older drivers actually at higher risk of involvement in collisions resulting in deaths or non-fatal injuries among their passengers and other road users? Inj Prev. 2004;10(1):27–32. doi:10.1136/ip.2003.002923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Hutchins L. Cynthia. Opening a Vital Dialogue with Aging Family Members. Financial Gerontology Series: Part 1; 2014:1–4. [Google Scholar]
- 3. Department of Transportation (US), Federal Highway Administration. Highway Statistics 2012. Washington, DC: FHWA; 2015. [Google Scholar]
- 4. Yee WY, Cameron PA, Bailey MJ. Road traffic injuries in the elderly. Emerg Med J. 2006;23(1):42–46. doi:10.1136/emj.2005.023754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Preusser DF, Williams AF, Ferguson SA, Ulmer RG, Weinstein HB. Fatal crash risk for older drivers at intersections. Accid Anal Prev. 1998;30(2):151–159. doi:10.1016/S0001-4575(97)00090-0. [DOI] [PubMed] [Google Scholar]
- 6. Tefft BC. Risks older drivers pose to themselves and to other road users. J Safety Res. 2008;39(6):577–582. doi:10.1016/j.jsr.2008.10.002. [DOI] [PubMed] [Google Scholar]
- 7. Lyman S, Ferguson S, Braver ER, Williams F. Older driver involvements in police reported crashes and fatal crashes: trends and projections. Inj Prev. 2002;8(2):116–120. doi:10.1136/ip.8.2.116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. McCarthy DP, Mann WC. Process and Outcomes Evaluation of Older Driver Screening Programs: The Assessment of Driving-Related Skills (ADReS) Older-Driver Screening Tool. Washington, DC: NHTSA; 2009:28. [Google Scholar]
- 9. Augenstein J. Differences in Clinical Response between the Young and the Elderly. Proceedings of the Ageing and Driving Symposium; Southfield, MI. 2001. Des Plaines, IL: Association for the Advancement of Automotive Medicine; 2001. [Google Scholar]
- 10. Wang SC. An Aging Population: Fragile, Handle with Care. Washington, DC: National Highway Traffic Safety Administration; 2001. Web site http://www.nhtsa.dot.gov/departments/nrd-50/ciren/umfragile.html. Updated March 2016. Accessed January 2016. [Google Scholar]
- 11. Desapriya E, Wijeratne H, Subzwari S, et al. Vision screening of older drivers for preventing road traffic injuries and fatalities. Cochrane Database Syst Rev. 2014;21(3):cd006252 doi:10.1002/14651858.CD006252.pub2. [DOI] [PubMed] [Google Scholar]
- 12. Congdon N, O’Colmain B, Klaver CC, et al. Causes and prevalence of visual impairment among adults in the United States. Arch Ophthalmol. 2004;122(4):477–485. doi:10.1001/archopht.122.4.477. [DOI] [PubMed] [Google Scholar]
- 13. Visual Standards. Vision Requirements for Driving Safety with Emphasis on Individual Assessment. London, United Kingdom: International Council of Ophthalmology; 2006. [Google Scholar]
- 14. Deary IJ, Corley J, Gow AJ, et al. Age-associated cognitive decline. Br Med Bull. 2009;92(1):135–152. doi:10.1093/bmb/ldp033. [DOI] [PubMed] [Google Scholar]
- 15. Holsinger T, Deveau J, Boustani M, Williams JW., Jr Does this patient have dementia? JAMA. 2007;297(21):2391–2404. Web site www.ncbi.nlm.nih.gov/pubmed/17551132. Updated June 2007. Accessed January 2016. [DOI] [PubMed] [Google Scholar]
- 16. Centers for Medicare & Medicaid Services. MLN Matters Number: MM 7079. 2013:1–6.
- 17. Espinoza S, Walston JD. Frailty in older adults: insights and interventions. Cleve Clin J Med. 2005;72(12):1105–1112. [DOI] [PubMed] [Google Scholar]
- 18. Conable KM, Rosner AL. A narrative review of manual muscle testing and implications for muscle testing research. J Chiropr Med. 2011;10(3):157–165. doi:10.1016/j.jcm.2011.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Mark W, Stanton M. The High Concentration of U.S. Health Care Expenditures. Agency Healthc Res Qual. 2006;6(19):1–11. [Google Scholar]
- 20. Stutts J, Martell C, Staplin L. Identifying Behaviors and Situations Associated With Increased Crash Risk for Older Drivers. National Highway Traffic Safety Administration. 2009. Web site http://trid.trb.org/view.aspx?id=897748. Updated June 2009. Accessed January 2016.
- 21. Burkhardt JE, Berger AM, McGavock AT. The mobility consequences of the reduction or cessation of driving by older women. In: Proceedings from the Second National Conference on Women’s Travel Issues; October 23-26, 1996; Baltimore, MD doi:10.1037/e736202011-024. [Google Scholar]
- 22. Shipp MD, Penchansky R. Vision testing and the elderly driver: is there a problem meriting policy change? J Am Optom Assoc. 1995;66(6):343–351. [PubMed] [Google Scholar]
- 23. Foley DJ, Heimovitz HK, Guralnik JM, Brock DB. Driving life expectancy of persons aged 70 years and older in the United States. Am J Public Health. 2002;92(8):1284–1289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. American Automobile Association Mature Driving Program. Web site http://seniordriving.aaa.com/. Published and updated April 2012. Accessed February 2016.
- 25. American Association for Retired Persons Driver Safety Program. Web site http://www.aarpdriversafety.org/. Published and updated April 2012. Accessed February 2016.
- 26. American Automobile Association Fitness Driver Program. Web site https://www.aaafoundation.org/sites/default/files/flexibility_brochure.pdf. Published and updated 2007. Accessed February 2016.
- 27. New York State Department of Motor Vehicle: Re-evaluation Program. Web site http://dmv.ny.gov/driver-license/dmv-driver-re-evaluation. Published 2008. Updated January 2016. Accessed February 2016.