

Abstract
Objective
To chart emergency department (ED) attendance and acute admission following a devastating earthquake in 2011 which lead to Canterbury's rapidly accelerated integrated health system transformations.
Design
Interrupted time series analysis, modelling using Bayesian change-point methods, of ED attendance and acute admission rates over the 2008–2014 period.
Setting
ED department within the Canterbury District Health Board; with comparison to two other district health boards unaffected by the earthquake within New Zealand.
Participants
Canterbury's health system services ∼500 000 people, with around 85 000 ED attendances and 37 000 acute admissions per annum.
Main outcome measures
De-seasoned standardised population ED attendance and acute admission rates overall, and stratified by age and sex, compared before and after the earthquake.
Results
Analyses revealed five global patterns: (1) postearthquake, there was a sudden and persisting decrease in the proportion of the population attending the ED; (2) the growth rate of ED attendances per head of population did not change between the pre-earthquake and postearthquake periods; (3) postearthquake, there was a sudden and persisting decrease in the proportion of the population admitted to hospital; (4) the growth rate of hospital admissions per head of the population declined between pre-earthquake and postearthquake periods and (5) the most dramatic reduction in hospital admissions growth after the earthquake occurred among those aged 65+ years. Extrapolating from the projected and fitted deseasoned rates for December 2014, ∼676 (16.8%) of 4035 projected hospital admissions were avoided.
Conclusions
While both necessarily and opportunistically accelerated, Canterbury's integrated health systems transformations have resulted in a dramatic and sustained reduction in ED attendances and acute hospital admissions. This natural intervention experiment, triggered by an earthquake, demonstrated that integrated health systems with high quality out-of-hospital care models are likely to successfully curb growth in acute hospital demand, nationally and internationally.
Keywords: integrated health system, hospital attendances and admissions, epidemiological investigation, Bayesian statistical methods
Strengths and limitations of this study.
This is the first general population study that sought to provide a longitudinal assessment of emergency department attendance and acute admission rate changes following a rapid healthcare system reorientation.
Novel interrupted time series analyses, modelled using Bayesian change-point methods, were employed to investigate sudden and long-term changes in attendance and admission rates prior to and following a devastating earthquake.
By itself, a limitation of this natural intervention experiment analysis is the potential difficulty in separating effect attribution due to the earthquake, the system reorientation or other drivers.
The geographically localised perimeter of this study, together with its focus on only two key variables, may fail to capture the full scope of population health seeking behaviour changes resulting from the integrated health system reorientation and may limit its generalisability to other jurisdictions.
Introduction
Acute admissions from emergency departments (EDs) are costly and often preventable, yet they have been rapidly growing in many countries.1–3 A continuing unabated increase in acute admissions potentially threatens the safe delivery of national public health services.1 4 5 In the UK, a series of publications concerned about the effect of rising hospital admissions have characterised hospitals as being ‘on the edge’,6 that admissions are ‘out of control’,7 and that an urgent ‘call to action’8 is needed. While these publications are perhaps provocative, ‘business as usual’ models of healthcare delivery will not be viable in the future. Similar sustainability concerns have been raised in New Zealand,5 9 and a reorientation of the country's healthcare systems called for—although it is recognised that there is no one panacea.10 Disease prevention is seen as a key solution, as is harnessing technological, social and other innovations.8 Proactive management of people with long-term conditions, together with multiple coordinated strategies underpinned by an integrated information system have also been mooted as among the key strategies to reduce ED demand.11 12 However, there is mounting recognition and consensus that integrated, cross-sector solutions are fundamental in redressing the sustainability issues plaguing our health systems,5 8 10 11 13 although their direct effects on hospital admission rates is not yet understood.14
The Canterbury District Health Board (CDHB)—the organisation charged with planning, managing, providing and purchasing health services to meet the needs of the population within the greater Christchurch region—in 2008 began implementing a significant transformation to integrated services.5 Among the primary motivations for this rescoping was to decrease fragmentation of services, dismantle professional silos, reduce escalating and unsustainable clinical and resource pressures on the Canterbury health system, ensure services were arranged more effectively and efficiently, and ultimately, to improve the health of its population.5 The vision for the integrated health system centred around enabling people to stay in their own homes, with an interconnected structure supporting them to live well and take greater responsibility for their own health; figure 1. It focused on integrating primary healthcare and other community sectors in managing patients.5 13 This whole-system approach was supported by several key service model enablers, including the Acute Demand Management Service (ADMS, a hospital avoidance programme) and the Community Rehabilitation Enhancement Support Team (CREST, a wrap-around, home-based rehabilitation programme), and system enablers, including ‘HealthPathways’ and the Canterbury Initiative (primary care doctors and hospital-based specialists developing and agreeing to primary care management and referral pathways).5 15 ADMS is founded on primary care doctors managing patients in their own homes and communities where it is safe to do so.5 13 Primary care teams, supported by mobile acute nursing services, community observation beds and rapid diagnostic services, are enabled to ‘do whatever it takes’.15 16 ‘HealthPathways’ provides guidance to primary care teams and includes system-wide agreed ambulance diversion protocols for patients to be managed in primary care practice or urgent care centres including a 24 h surgery where appropriate.
Figure 1.

Canterbury integrated health system vision. (Reproduced from Gullery and Hamilton,5 copyright 2015 Royal College of Physicians. Reproduced with permission.)
On Tuesday, 22 February 2011, at 1251 h New Zealand Standard Time, a shallow violent 6.3 Mw earthquake with epicentre 10 km southeast of Christchurch struck.17 18 Damage and destruction was extensive;17 19 a state of national emergency declared,20 and 185 deaths and over 6500 injuries resulted.18 21 Immediately after the earthquake there was considerable burden placed on Christchurch's seven hospitals. However, Christchurch Hospital is the only acute hospital within the region that has an ED, an intensive care unit, and a full range of tertiary hospital surgical and medical services.22 It was partially compromised by earthquake damage, and several non-acute hospitals temporarily provided emergency care.18 Damage to roads, bridges and other infrastructure isolated the east of the city from Christchurch Hospital, leaving primary care practitioners in these suburbs to manage many casualties.18 Earthquake damage resulted in the loss of 106 acute hospital beds, 635 aged residential care beds, 19 community pharmacies, five primary care practices, and displaced many small non-governmental organisations from the central city. Owing to the infrastructure damage and medical demands in the ensuing weeks and months following the earthquake, it was both necessary and an opportunity for the CDHB to accelerate transformational changes and implement new initiatives. One major strategy included the escalation of ADMS, with a deliberate intent in reducing ED attendances and hospital admissions.5 23
This descriptive epidemiological study assessed the impact of an integrated health system on ED attendances and acute admissions at Christchurch Hospital, New Zealand, before and after a major earthquake.
Methods
Using routinely collected data between 2008 and 2014, we compared acute admission rates following Christchurch Hospital's ED attendances before and after the earthquake with data from Waitemata DHB (WDHB) and Auckland DHB (ADHB) that serve the population of greater Auckland. WDHB and ADHB are in the North Island of New Zealand and were geologically unaffected by the earthquake. The WDHB was selected because it has a demographically similar population to that of the CDHB, but it does not have a tertiary hospital. ADHB was chosen because it does have such a hospital.
Design
An interrupted time series design, modelling using Bayesian change-point methods, of ED attendance and acute admission rates over the 2008–2014 period.
Target population
All patient ED attendances and acute admissions within the CDHB; with comparison to patients within the WDHB and ADHB jurisdictions.
Procedure
Monthly aggregated and anonymised ED attendance and admission volume data were provided from CDHB, WDHB and ADHB regions over the 2008–2014 period. These data were stratified by sex (male, female) and age groupings (each spanning 5 years). Similarly, stratified annual population projections were obtained from Statistics New Zealand for these DHBs.24 Following the 2013 Census, the 2013 and 2014 annual population projections were amended, accounting for evacuations and movement.
Patient involvement
No patients were involved in setting the research question or the outcome measures, nor were they involved in the design and implementation of the study. There are no plans to involve patients in dissemination.
Statistical analyses
Utilising the annualised population projections, standardised monthly attendance and admission rates (per 1000 people) were calculated. Scatter plots and superimposed lowess curves (non-parametric mean estimate function) were used to ascertain patterns. Time series analysis of the CDHB data employed Bayesian methods, in which series were partitioned into constant, trend and seasonal components; together with allowing for a disconnected change-point mechanism to account for any significant interruption caused by the earthquake.25 Seasonal adjustment was modelled by assigning a categorical indicator variable for each month. A disconnected change-point model allows for a piecewise mean and slope shift within the time series to be statistically detected and assigned. Separate models were run for attendance and admission rate series (where the change point was estimated from the data and compared to the actual earthquake date), and for these data partitioned by sex and age groups (where the change point was set to the earthquake date). Here, monthly data were assigned an integer value from 1 (January 2008) to 84 (December 2014). Standardised rates were assumed to be normally distributed. Non-informative priors were employed and Markov chain Monte Carlo methods utilised two parallel chains, each with simulation size n=100 000 after a burn-in period of 5000 iterations. The Gelman-Rubin statistic and visual plots were used to assess model convergence and stability; and residual distribution and autocorrelation checks were conducted. In comparing rates, posterior probabilities (pp) were employed. Estimated pp<0.025 and pp>0.975 were deemed to be statistically significant, and 95% credible regions (CRs) were derived by using the 2.5 and 97.5 centiles of the posterior distribution. A pp>0.975 implies that the pre-earthquake rate was importantly higher than the postearthquake rate; pp<0.025 implies that the pre-earthquake rate was importantly lower than the postearthquake rate; and 0.025≤pp≤0.975 implies that there was no important change in rates between periods. All statistical analyses were conducted in WinBUGS V.1.4.3,26 and graphs were drawn in Stata V.14.1 (StataCorp, College Station, USA).
Results
Demographics
Over the study period, the estimated CDHB population increased by 19 100 (3.9%) people; substantially less than that estimated for the WDHB and ADHB jurisdictions of 41 730 (8.0%) and 31 450 (7.2%) people, respectively (table 1). The annual ED attendance numbers for the CDHB, WDHB and ADHBs also increased by 15 885 (20.8%), 31 825 (40.3%) and 18 851 (22.5%) people, respectively; as did acute admission numbers by 4346 (12.5%), 16 758 (35.3%) and 7932 (14.8%) people, respectively. Annual CDHB population projections by sex and age groups appear in table 2. Within the CDHB region, small but important demographic shifts in the distribution of sex and age distributions was discernible over time—with relatively more male residents and adults aged 65+ years, and relatively fewer children aged 0–14 years.
Table 1.
Total population projections for CDHB, WDHB, and ADHB regions estimated by Statistics New Zealand and total ED attendances and hospital admissions from 2008 to 2014
| CDHB |
WDHB |
ADHB |
|||||||
|---|---|---|---|---|---|---|---|---|---|
| Year | Popn | Attendances | Admissions | Popn | Attendances | Admissions | Popn | Attendances | Admissions |
| 2008 | 495 940 | 76 550 | 34 834 | 520 950 | 79 010 | 47 512 | 438 130 | 83 704 | 53 769 |
| 2009 | 502 040 | 81 178 | 35 784 | 528 720 | 77 589 | 47 547 | 444 190 | 87 925 | 56 162 |
| 2010 | 508 250 | 86 938 | 39 443 | 537 480 | 88 415 | 52 051 | 450 290 | 85 075 | 53 520 |
| 2011 | 502 780 | 78 900 | 35 875 | 546 200 | 98 567 | 56 285 | 456 640 | 92 539 | 54 694 |
| 2012 | 503 460 | 82 784 | 36 316 | 553 080 | 102 540 | 59 186 | 461 230 | 95 534 | 56 984 |
| 2013* | 504 220 | 88 031 | 38 315 | 552 770 | 105 769 | 60 862 | 460 450 | 98 300 | 60 720 |
| 2014* | 515 040 | 92 435 | 39 180 | 562 680 | 110 835 | 64 270 | 469 580 | 102 555 | 61 701 |
*Updated population estimates, derived from the 2013 New Zealand Census.
ADHB, Auckland District Health Board; CDHB, Canterbury District Health Board; ED, emergency department; WDHB, Waitemata District Health Board.
Table 2.
Population projections by sex and age categories for the CDHB region estimated by Statistics New Zealand from 2008 to 2014
| Year | Sex |
Age (years) |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Females |
Males |
0–14 |
15–34 |
35–64 |
65+ |
|||||||
| Popn | (%) | Popn | (%) | Popn | (%) | Popn | (%) | Popn | (%) | Popn | (%) | |
| 2008 | 252 450 | (50.9) | 243 490 | (49.1) | 94 030 | (19.0) | 133 860 | (27.0) | 200 290 | (40.4) | 67 760 | (13.7) |
| 2009 | 255 150 | (50.8) | 246 890 | (49.2) | 94 230 | (18.8) | 134 800 | (26.9) | 203 360 | (40.5) | 69 650 | (13.9) |
| 2010 | 257 960 | (50.8) | 250 290 | (49.2) | 94 690 | (18.6) | 135 720 | (26.7) | 206 020 | (40.5) | 71 820 | (14.1) |
| 2011 | 254 840 | (50.7) | 247 940 | (49.3) | 92 700 | (18.4) | 133 780 | (26.6) | 203 450 | (40.5) | 72 850 | (14.5) |
| 2012 | 254 900 | (50.6) | 248 560 | (49.4) | 91 810 | (18.2) | 133 380 | (26.5) | 202 640 | (40.2) | 75 630 | (15.0) |
| 2013* | 253 570 | (50.3) | 250 650 | (49.7) | 94 930 | (18.8) | 132 830 | (26.3) | 202 510 | (40.2) | 73 950 | (14.7) |
| 2014* | 258 850 | (50.3) | 256 190 | (49.7) | 95 520 | (18.5) | 137 950 | (26.8) | 204 520 | (39.7) | 77 050 | (15.0) |
*Updated estimates, derived from the 2013 New Zealand Census.
CDHB, Canterbury District Health Board.
Figure 2 presents scatter plots of observed standardised monthly ED attendance rates and acute admission rates per 1000 people, together with superimposed lowess curves for the three DHBs. Unlike that observed within the WDHB and ADHB jurisdictions, a clear interrupted pattern change is visible in the scatterplot distribution and superimposed lowess curves before and after the 22 February 2011 earthquake (denoted by the vertical line) for ED attendance and acute admission rates within the CDHB.
Figure 2.

Scatter plots of observed standardised monthly ED attendance rates and acute hospital admissions rates per 1000 people, together with superimposed lowess curves (non-parametric mean estimate function) for the CDHB, WDHB and ADHB between 2008 and 2014. The vertical line denotes the time of the 22 February 2011 earthquake. ADHB, Auckland District Health Board; CDHB, Canterbury District Health Board; WDHB, Waitemata District Health Board.
ED attendance rates
Analysis of the observed CDHB standardised monthly ED attendance rates revealed significant intercept, trend and monthly seasonal components (figure 3). A change point was detected at study period month 38.4 (95% CR 37.2–39.0). This CR includes the value 38.8 which corresponds to 22 February 2011—the date of the earthquake. At the detected change point, the estimated deseasoned ED monthly attendance rate fell from 14.7/1000 people to 12.7, a decrease that was significant (pp>0.999) and dramatic (table 3). Also notable in table 3 is the lack of change in the deseasoned growth rate in ED attendances between the pre-earthquake and postearthquake periods (pp=0.36). These patterns, together with expected postearthquake ED attendance rates extrapolated from pre-earthquake estimates, are also illustrated in figure 3. Residual analyses revealed one outlying observation (February 2011), a unimodal but skewed distribution (Shapiro-Wilk's test, p=0.003), and evidence of positive autocorrelation (Durbin-Watson d-statistic=1.12). No other issues were noted.
Figure 3.
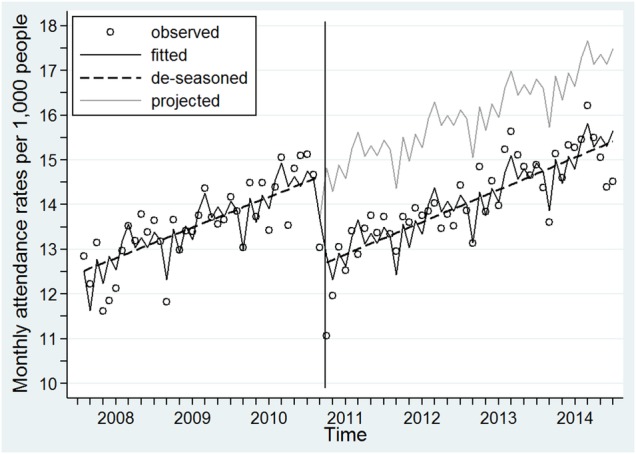
Scatter plots of observed CDHB standardised monthly ED attendance rates per 1000 people (hollow circles), together with a superimposed fitted lined from the full time-series model (solid line), the estimated deseasoned trend line (heavy dashed straight line) and the extrapolated projected line (grey line). The vertical line denotes the time of the 22 February 2011 earthquake. CDHB, Canterbury District Health Board.
Table 3.
Estimated deseasoned ED attendance rates per 1000 people prior to and post the change point, together with the estimated monthly increase in deseasoned ED attendance rates per 1000 people in the periods prior to and post the change point for the CDHB population in total and stratified by sex and age groups over the 2008–2014 period
| Deseasoned ED attendance rates at change point |
Monthly increase in deseasoned ED attendance rates |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Prior |
Post |
Posterior | Prior to change point |
Post change point |
Posterior | |||||
| Estimate | (95% CR) | Estimate | (95% CR) | Probability | Estimate | (95% CR) | Estimate | (95% CR) | Probability | |
| All | 14.7 | (14.3–15.0) | 12.7 | (12.4–13.0) | >0.999 | 0.057 | (0.042–0.072) | 0.060 | (0.049–0.071) | 0.36 |
| Sex | ||||||||||
| Female | 14.0 | (13.7–14.3) | 12.0 | (11.7–12.3) | >0.999 | 0.063 | (0.049–0.077) | 0.063 | (0.053–0.074) | 0.48 |
| Male | 15.3 | (15.0–15.6) | 13.4 | (13.0–13.7) | >0.999 | 0.050 | (0.034–0.066) | 0.057 | (0.045–0.069) | 0.22 |
| Age (years) | ||||||||||
| 0–14 | 13.7 | (13.0–14.4) | 11.8 | (11.2–12.4) | >0.999 | 0.067 | (0.036–0.097) | 0.032 | (0.009–0.054) | 0.967 |
| 15–34 | 15.3 | (14.8–15.8) | 12.9 | (12.4–13.4) | >0.999 | 0.065 | (0.041–0.089) | 0.110 | (0.092–0.128) | 0.002 |
| 35–64 | 10.9 | (10.7–11.2) | 9.8 | (9.6–10.0) | >0.999 | 0.036 | (0.025–0.048) | 0.044 | (0.036–0.053) | 0.13 |
| 65+ | 25.2 | (24.6–25.8) | 21.2 | (20.7–21.8) | >0.999 | 0.070 | (0.042–0.098) | 0.043 | (0.022–0.064) | 0.941 |
CDHB, Canterbury District Health Board; CR, credible region; ED, emergency department.
Fixing the change point to 38.8 and partitioning the data by sex, the Bayesian model yielded estimates of deseasoned rates of ED attendances at the change point that significantly decreased for females and males (table 3). However, there was no significant difference in the monthly increase in deseasoned attendance rates between pre-earthquake and postearthquake periods for either sex. When comparing males and females at the change point, males had significantly higher rates of ED attendance than females pre-earthquake (pp>0.999) and postearthquake (pp>0.999). However, the monthly increase in attendance rates was not significantly different between females and males either in the period before (pp=0.89) or after (pp=0.78) the February earthquake. Repeating the Bayesian analyses on ED attendance data partitioned by age groups yielded generally similar findings. Significant decreases in the deseasoned ED attendances rates were seen across all age groups at the time of the earthquake (all pp>0.999). Deseasoned monthly increases in ED attendance rates for the 0–14, 35–64 and 65+ years age groups did not significantly change between pre-earthquake and postearthquake periods. However, for the 15–34 years age group, a significant rise in this rate was observed in the postearthquake period compared with the pre-earthquake period (table 3).
Hospital admissions rates
Significant intercept, trend and monthly seasonal components were also evident in the analysis of the observed CDHB standardised monthly acute hospital admissions rates (figure 4). For this series, a change point was detected at study period month 38.2 (95% CR 37.1–39.0), with the CR again overlapping with the earthquake date. At this detected change point, the estimated deseasoned monthly acute admissions rate significantly fell from 6.59/1000 people to 5.83, pp>0.999. However, unlike that seen for ED attendances, an apparent change in deseasoned rates of change in hospital admissions between the pre-earthquake and postearthquake periods was also observed (see figure 4). Prior to the change point, the deseasoned rates of acute admissions increased by an estimated 0.026/1000 people per month, whereas after the change point the estimated increase was estimated at 0.014, pp=0.998 (table 4). Residual analyses found evidence for positive autocorrelation (Durbin-Watson d-statistic=1.18). No other issues were noted.
Figure 4.
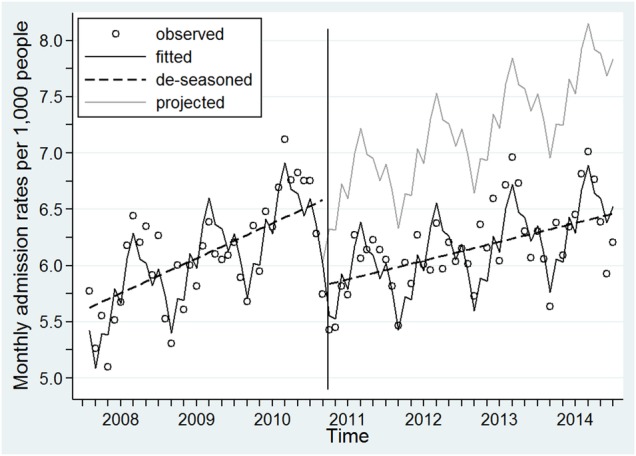
Scatter plots of observed CDHB standardised monthly acute hospital admission rates per 1000 people (hollow circles), together with a superimposed fitted lined from the full time series model (solid line), the estimated deseasoned trend line (heavy dashed straight line) and the extrapolated projected line (grey line). The vertical line denotes the time of the 22 February 2011 earthquake. CDHB, Canterbury District Health Board.
Table 4.
Estimated deseasoned hospital admissions rates per 1000 people prior to and post the change point, together with the estimated monthly increase in deseasoned hospital admission rates per 1000 people in the periods prior to and post the change point for the CDHB population in total and stratified by sex and age groups over the 2008–2014 period
| Deseasoned admission rates at change point |
Monthly increase in deseasoned admission rates |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Prior |
Post |
Posterior | Prior to change point |
Post change point |
Posterior | |||||
| Estimate | (95% CR) | Estimate | (95% CR) | Probability | Estimate | (95% CR) | Estimate | (95% CR) | Probility | |
| All | 6.59 | (6.45–6.73) | 5.83 | (5.70–5.95) | >0.999 | 0.026 | (0.020–0.032) | 0.014 | (0.009–0.019) | 0.998 |
| Sex | ||||||||||
| Female | 6.42 | (6.27–6.58) | 5.63 | (5.49–5.78) | >0.999 | 0.025 | (0.018–0.032) | 0.017 | (0.012–0.022) | 0.959 |
| Male | 6.75 | (6.59–6.90) | 6.01 | (5.86–6.15) | >0.999 | 0.026 | (0.019–0.033) | 0.011 | (0.006–0.016) | >0.999 |
| Age (years) | ||||||||||
| 0–14 | 5.65 | (5.31–5.98) | 5.29 | (4.98–5.60) | 0.938 | 0.030 | (0.015–0.045) | 0.014 | (0.003–0.026) | 0.948 |
| 15–34 | 3.75 | (3.58–3.92) | 3.36 | (3.21–3.52) | >0.999 | 0.020 | (0.012–0.028) | 0.016 | (0.010–0.022) | 0.78 |
| 35–64 | 4.63 | (4.50–4.76) | 4.20 | (4.08–4.32) | >0.999 | 0.012 | (0.006–0.018) | 0.009 | (0.004–0.013) | 0.83 |
| 65+ | 18.6 | (18.2–19.1) | 15.4 | (15.0–15.9) | >0.999 | 0.049 | (0.029–0.070) | 0.018 | (0.003–0.033) | 0.992 |
CDHB, Canterbury District Health Board; CR, credible region.
Again, assigning the change point to 38.8 and partitioning by sex, estimates of the deseasoned rate of hospital admissions at the change point significantly fell for females and males (table 4). Between pre-earthquake and postearthquake periods, there was a non-significant fall in the monthly increase in deseasoned admission rate estimate for females (pp=0.959) but a significant fall for males (pp>0.999)—with estimated increases less than half that after the earthquake than in the period before. When comparing males and females at the change point, males had significantly higher rates of hospital admission than females prior to the earthquake (pp=0.992) and after the earthquake (pp>0.999). However, the monthly increase in admission rates was not significantly different between females and males before (pp=0.42) or after (pp=0.940) the earthquake. Table 4 also presents results stratified by age groups. A notable feature of these results is a significant decrease in the deseasoned admission rates at the change point (pp>0.999) and the monthly increase in rates before and after the change point (pp=0.992) of those aged 65+ years. For the 15–34 years and 35–64 years age groups, there was a significant decrease in the deseasoned rate of admissions at the change point (both pp>0.999), but no significant change in monthly increases of deseasoned admission rates between pre-earthquake and postearthquake periods (pp=0.78 and 0.83, respectively). Finally, for the 0–14 years age group, no significant change was noted; although the estimated monthly increase in deseasoned admission rates for the postearthquake period was less than half that in the pre-earthquake period.
Discussion
Our interpreted time series analysis demonstrated that the rapidly accelerated integrated Canterbury health system transformation strategy after the earthquake significantly lowered the level and the growth rate of acute admissions. These important shifts have significant resource implications. Looking at hospital admissions for December 2014 alone, the difference between projected and fitted rates per 1000 people is 1.31. Upscaling, this equates to ∼676 (16.8%) admissions avoided from 4035 projected for that month. Prior to the earthquake, the community ADMS received ∼14 000 referrals per annum. However, the infrastructure damage and constraints imposed by the earthquake resulted in a rapid escalation of this service, which now receives around 30 000 referrals per annum.
The most dramatic reduction in acute admissions growth after the earthquake occurred among those aged 65+ years. Accelerated population ageing, coupled with the resultant increase in age-related chronic diseases, has been opined as being among the most pressing challenges of all modern health systems worldwide,8 12 including New Zealand.10 27 As such, Canterbury's integrated health system model, which embodies community inventions including ADMS, CREST, the Medication Management Service (engaging community pharmacists to actively review medications) and the Community Falls Prevention programme, targeted older adults.5 Unlike hospital avoidance programmes elsewhere,28 this targeting has been successful. For example, among those aged 75+ years, the Community Falls Prevention programme has been attributed with 1076 fewer ED attendances due to falls, 386 fewer femoral neck fracture operations, 86 fewer deaths 180 days postdischarge, and 25 fewer people in hospital each day as a result of a fracture since February 2012. Should these decreased levels persist, and be generalisable to other health jurisdictions, then the case for the integrated health system model is further enhanced.5 13
ED attendance rates were also significantly influenced by the Canterbury health system's whole-system community-focused approach. While the overall ED attendance growth rate did not change between pre-earthquake and postearthquake periods, this represents a positive and important finding. If a ‘business as usual’ approach was adopted, growth in the postearthquake period could have been expected to accelerate, compensating for the sudden drop. But this did not happen. The sustained rate fall, together with the unchanged monthly postearthquake growth rate, represents a significant resource saving relative to pre-earthquake expectations. However, a significant increase in ED attendances growth was observed in one subgroup, those aged 15–34 years; a likely consequence of worker immigration, arriving for the Christchurch rebuilding programme.24 It will be of interest to observe this pattern in the future, once the rebuild programme wanes.
Strengths and limitations of this study
While this study has salient strengths, including the analysis of comprehensive, contemporaneous and accurate hospital data using apposite Bayesian methods, it also has its limitations. In terms of the statistical models, positive autocorrelation was observed between residuals, and some evidence was found to question the normal distribution assumption of ED attendance rates. Such assumption violations may introduce biases into mean and variance estimates; although in this case, such biases are likely to be relatively modest. Sensitivity analysis that removed the most extreme outlying ED attendance rate observation found little change in parameter estimates, and high overlap of respective 95% CRs (data not show). Population estimates are produced annually by Statistics New Zealand to inform population-based funding for the country's 20 DHBs. However, these estimates lag behind rapid population changes, such as that associated with the Christchurch rebuild workforce, potentially significantly undercounting population or subpopulation numbers. Such undercounting results in rate inflation and may serve to underestimate the true rate reductions observed in the postearthquake period. ED attendances and acute admissions are but two related indicators of Canterbury's whole-system approach, and a fuller suite of indicators should be appraised before more substantial claims of the success of the approach can be made. The sustained decrease in ED attendances and the reduced hospital admission growth rate points to a successful admission avoidance/acute demand management effort, rather than an unmeasured population effect. However, unmeasured population effects cannot be entirely dismissed. Indeed, the acute admission rates for the ADHB flattened over the 2009–2012 period (figure 2). Although this is likely to have resulted from new and improved ED facilities in neighbouring WDHB,29 the northern DHBs working more closely together,29 and ADHB's drive to reduce admissions.30 Moreover, the baseline acute admission rate was significantly higher in Auckland than Canterbury, although differing data definitions and coding approaches between the DHBs exist, making direct comparisons difficult. The fact that hospitals admission rates decreased most for the target group of older adults further reduces the likelihood of an unmeasured population effect. The possibility that improved pathways could have resulted in increasing direct admissions to the ward without an ED stay was explored, however, little difference was found. Furthermore, it might be opined that the observed attendance and admission decrease may be, at least partially, a lingering consequence of the earthquake rather than the integrated health service changes. Analysis of data from an extended study period, together with further studies directly capturing staff and patient perceptions and behaviour changes would be required to disentangle these effects. Finally, the analyses are defined for the 2008–2014 period, and the findings should not be extrapolated outside this range.
Conclusions
‘Are hospital admissions out of control?’7 There are many reasons why they might be and, if left uncurbed, will only get worse.4 Integrated healthcare systems with high quality out-of-hospital care could be part of the solution;1 2 4 13 a view championed and implemented within the Canterbury health system.5 Using a methodologically novel approach and a rapidly transformed health system, initiated by a devastating earthquake, our findings unequivocally support this position.
Acknowledgments
The authors thank many people, including members of the public, emergency services, healthcare professionals, police and urban search and rescue personnel who helped the injured people of Canterbury; and the participating DHBs for making available their data.
Footnotes
Contributors: PJS conceived the study. All authors finalised the study and contributed to its design. GJH facilitated retrieval of hospital data. PJS conducted the statistical analysis. All authors contributed to data interpretation. PJS and JMD led the manuscript writing with contributions from GJH and MWA. All authors approved the final version. PJS is the guarantor.
Funding: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: All authors have completed the Unified Competing Interests form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author). GJH is an employee of the CDHB and is a member of the Canterbury Clinical Network's Urgent Care Service Level Alliance. JMD received funding from the Emergency Co-ordination Teams and Emergency Care Foundation for medical writing. MWA is an employee of the CDHB, chair of the RHISE Group (Researching the Health Implications of Seismic Events) and is a trustee of the Emergency Care Foundation. Apart for the salaried positions of GJH and MWA, there were no financial relationships with any organisation that might have an interest in this study; no other relationships or activities that could appear to have influences this work.
Ethics approval: The study complied with the ethical standards for human experimentation as established by the Helsinki Declaration 1995 (as revised in Edinburgh 2000) and New Zealand's Health and Disability Ethics Committee (HDEC). HDEC defined this study as minimal risk observational research, and it did not require ethics committee review.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data sharing statement: Other researchers can apply for our data through the CDHB, ADHB and WDHB Planning and Funding Divisions. New Zealand Census data are freely available from Statistics New Zealand. See: http://www.stats.govt.nz/Census/2013-census/data-tables/dhb-tables.aspx.
References
- 1.Blunt I, Bardsley M, Dixon J. Trends in emergency admissions in England 2004–2009. London: Nuffield Trust, 2010. [Google Scholar]
- 2.Lappegard Ø, Hjortdahl P. Acute admissions to a community hospital—health consequences: a randomized controlled trial in Hallingdal, Norway. BMC Fam Pract 2014;15:198 10.1186/s12875-014-0198-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hider P, O'Hagan J, Bidwell S et al. The rise in acute medical admissions. Aust N Z J Med 2000;30:252–60. 10.1111/j.1445-5994.2000.tb00816.x [DOI] [PubMed] [Google Scholar]
- 4.Gillam S. Rising hospital admissions. BMJ 2010;340:c636 10.1136/bmj.c636 [DOI] [PubMed] [Google Scholar]
- 5.Gullery C, Hamilton G. Towards integrated person-centred healthcare—the Canterbury journey. Future Hosp J 2015;2:111–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Royal College of Physicians. Hospitals on the edge? The time for action. London: Royal College of Physicians, 2012. [Google Scholar]
- 7.Robinson P. Are hospital admissions out of control? Alcester: CHKS, 2010. [Google Scholar]
- 8.NHS England. The NHS belongs to the people: a call to action. London: NHS England, 2013. [Google Scholar]
- 9.Sandiford P, Zhou L, Salvetto M et al. Measuring unexplained variation in acute hospital use by patients enrolled with northern New Zealand general practices. J Prim Health Care 2014;6:93–100. [PubMed] [Google Scholar]
- 10.Mays N. Reorienting the New Zealand health care system to meet the challenge of long-term conditions in a fiscally constrained environment. http://www.victoria.ac.nz/sacl/about/cpf/publications/pdfs/Nick-Mays-Revised-Conference-Paper-Jan-2013-website-version.pdf (accessed 7 Sep 2015). [Google Scholar]
- 11.Ham C, Imison C, Jennings M. Avoiding hospital admissions: lessons from evidence and experience. London: The King's Fund, 2010. [Google Scholar]
- 12.Bayliss EA, Ellis JL, Shoup JA et al. Effect of continuity of care on hospital utilization for seniors with multiple medical conditions in an integrated health care system. Ann Fam Med 2015;13:123–9. 10.1370/afm.1739 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Timmins N, Ham C. The quest for integrated health and social care: a case study in Canterbury, New Zealand. London: The King's Fund, 2013. [Google Scholar]
- 14.Steventon A, Bardsley M, Billings J et al. An evaluation of the impact of community based interventions on hospital use: a case study of eight Partnership for Older People Projects (POPP). London: Nuffield Trust, 2011. [Google Scholar]
- 15.McGeoch G, Anderson I, Gibson J et al. Consensus pathways: evidence into practice. N Z Med J 2015;128:86–96. [PubMed] [Google Scholar]
- 16.McGeoch G, McGeoch P, Shand B. Is HealthPathways effective? An online survey of hospital clinicians, general practitioners and practice nurses. N Z Med J 2015;128:36–46. [PubMed] [Google Scholar]
- 17.Johnston D, Standring S, Ronan KR et al. The 2010/2011 Canterbury earthquakes: context and cause of injury. Nat Hazards 2014;73:627–37. 10.1007/s11069-014-1094-7 [DOI] [Google Scholar]
- 18.Ardagh MW, Richardson SK, Robinson V et al. The initial health-system response to the earthquake in Christchurch, New Zealand, in February, 2011. Lancet 2012;379:2109–15. 10.1016/S0140-6736(12)60313-4 [DOI] [PubMed] [Google Scholar]
- 19.Stevenson JR, Kachali H, Whitman Z et al. Preliminary observations of the impacts the 22 February Christchurch earthquake had on organisations and the economy: a report from the field. Bull N Z S Earthquake Eng 2011;44:65–76. [Google Scholar]
- 20.Carter J. Minister of Civil Defence statement to Parliament that state of national emergency declared. http://www.beehive.govt.nz/speech/minister-civil-defence-statement-parliament-state-national-emergency-declared (accessed 6 Jan 2015).
- 21.Morgan J, Begg A, Beaven S et al. Monitoring wellbeing during recovery from the 2010–2011 Canterbury earthquakes: the CERA Wellbeing Survey. Int J Disaster Risk Reduction 2015;14(Pt 1):96–103. 10.1016/j.ijdrr.2015.01.012 [DOI] [Google Scholar]
- 22.Canterbury District Health Board. Christchurch Hospital. http://www.cdhb.govt.nz/chc/ (accessed 6 Jan 2015).
- 23.Canterbury District Health Board. Earthquake update thirteen—Canterbury DHB 26 February. http://www.nzdoctor.co.nz/un-doctored/2011/february-2011/27/earthquake-update-thirteen-%E2%80%93-canterbury-dhb-26-february.aspx (accessed 6 Jan 2015).
- 24.Statistics New Zealand. Population statistics. Dataset: subnational population estimates (Territoral Authority, Area Unit), by age and sex, at 30 June 2006–14 (2013 boundaries). Wellington: Statistics New Zealand, 2015. [Google Scholar]
- 25.Carlin BP, Gelfand AE, Smith AFM. Hierarchical Bayesian analysis of changepoint problems. Appl Stat 1992;41:389–405. 10.2307/2347570 [DOI] [Google Scholar]
- 26.Lunn DJ, Thomas A, Best N et al. WinBUGS—a Bayesian modelling framework: concepts, structure, and extensibility. Stat Comput 2000;10:325–37. 10.1023/A:1008929526011 [DOI] [Google Scholar]
- 27.Ministerial Review Group. Meeting the challenge: enhancing sustainability and the patient and consumer experience within the current legislative framework for health and disability service in New Zealand. Wellington: The New Zealand Government, 2009. [Google Scholar]
- 28.Steventon A, Bardsley M, Billings J et al. The role of matched controls in building an evidence base for hospital-avoidance schemes: a retrospective evaluation. Health Serv Res 2012;47:1679–98. 10.1111/j.1475-6773.2011.01367.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Waitemata District Health Board. Annual plan 2010/11. Waitemata: WDHB, 2010. [Google Scholar]
- 30.Auckland District Health Board. District annual plan 2010–2011. Auckland: ADHB, 2010. [Google Scholar]