

Summary
Background
Myxomatous mitral valve with prolapse are classically seen with abnormal leaflet apposition during contraction of the heart. Hemodynamic disorders can result from eccentric mitral regurgitation usually caused by chordae tendinae rupture or papillary muscle dysfunction. Echocardiography is the gold standard for evaluation of leaflet flail and prolapse due to high sensitivity and specificity. Though most mitral valve prolapse are asymptomatic those that cause severe regurgitation need emergent surgical intervention to prevent disease progression.
Case Report
We report a 54 year old Hispanic male who presented with progressively worsening dyspnea and palpitations. Initial evaluation was significant for atrial fibrillation on electrocardiogram with subsequent echocardiography revealing myxomatous mitral valve with prolapse. Following surgical repair of the mitral valve, the dyspnea and palpitations resolved.
Conclusions
Mitral valve prolapse is a common valvular abnormality but the pathogenic cause of myxomatous valves has not been elucidated. Several theories describe multiple superfamilies of proteins to be involved in the process. Proper identification of these severe mitral regurgitation due to these disease valves will help relieve symptomatic mitral valve prolapse patients.
MeSH Keywords: Mitral Valve Annuloplasty, Mitral Valve Insufficiency, Mitral Valve Prolapse
Background
Myxomatous mitral valve (accumulation of elastin and collagen) is the most common cause of mitral valve prolapse (MVP). MVP is defined by echocardiographic imaging showing a single or dual prolapse of >2 mm beyond the annular plane. Complications such as chordae tendinae rupture, severe mitral regurgitation, LV systolic dysfunction, endocarditis and neurological sequelae can occur with myxomatous degeneration. Here, we present a case of a 54-year-old Hispanic male who presented with bi-leaflet prolapse and flail P2 scallop with severe eccentric type II mitral regurgitation.
Case Report
A 54-year-old Hispanic male admitted with complains of progressive dyspnea and palpitations. On physical examination he was tachycardic with irregular rhythm, had elevated jugular venous distention, bilateral rales on lung examination and grade 3/6 systolic ejection murmur at the apex. His 12-lead ECG showed atrial fibrillation and on transthoracic and transesophageal echocardiogram he was found to have myxomatous mitral valve with prolapse of both the anterior and posterior leaflets and severe LV systolic dysfunction. In addition, there was a flail P2 scallop of the posterior mitral leaflet with anteriorly directed eccentric jet of severe mitral regurgitation as seen in Figures 1–3 which show this anteriorly directed mitral regurgitation in 0°, 30° and 120° views. His coronary angiogram showed angiographically normal coronaries. After his heart failure was managed and the rapid ventricular rate due to atrial fibrillation was controlled, he underwent a successful repair of the P2 scallop, which eliminated his mitral regurgitation.
Figure 1.

Transesophageal 0° mid esophageal view with color Doppler showing myxomatous bileaflet prolapse with flail P2 scallop and anteriorly directed eccentric MR jet.
Figure 2.

Transesophageal 30° mid esophageal view with color Doppler showing myxomatous bileaflet prolapse with flail P2 scallop and anteriorly directed eccentric MR jet.
Figure 3.

Transesophageal 120° mid esophageal view with color Doppler showing myxomatous bileaflet prolapse with flail P2 scallop and anteriorly directed eccentric MR jet.
Discussion and Conclusions
Mitral valve prolapse is a common valvular abnormality in the general population affecting approximately 5% of the population with no sex discrimination [1]. Myxomatous mitral valve has an underlying pathological mechanism which is the result of poorly organized proteoglycan deposition, this patient has a 4 and 3 chamber view of the bileaflet myxomatous deposition in Figures 4 and 5 [2]. This layered deposition on the mitral valve results in thickened leaflets leading to inefficient opening and closing of valves causing mitral regurgitation [2]. Recent research shows that TGF-β superfamily proteins, bone morphogenic proteins (BMP), proteoglycans and ADAMTs, oxidative stress, muscle structural proteins and serotonin signaling all play a role in the remodeling process for myxomatous mitral valve prolapse. However, the mechanism has not been elucidated thus far [2–4].
Figure 4.
Apical 4-chamber view showing myxomatous bileaflet prolapse with flail leaflet and anteriorly directed eccentric MR jet.
Figure 5.

Apical 3-chamber view showing myxomatous bileaflet prolapse with flail leaflet and anteriorly directed eccentric MR jet.
The most common causes of flail leaflets include chord rupture, myxomatous degeneration, and a combination of both mechanisms [5]. Most cases of flail P2 scalloping, in the context of myxomatous mitral valve prolapse, will be treated with surgical intervention [6,7]. The general surgical approach to repair mitral valve prolapse include an anuloplasty ring and resection of flail portion of the affected leaflets [8]. If particularly severe, surgeons may require placement of an artificial prosthetic chordae and shorten or transplant chordae from other leaflets [8]. Mitral clip by itself is also an option among high-risk patients. However, the recurrence rate of mitral regurgitation is higher with this approach [9]. The incidence of independent flail P2 scalloping was ~55% in a recent study conducted in 100 patients with an increased incidence of flail associated with posterior leaflet and middle scallop [5].
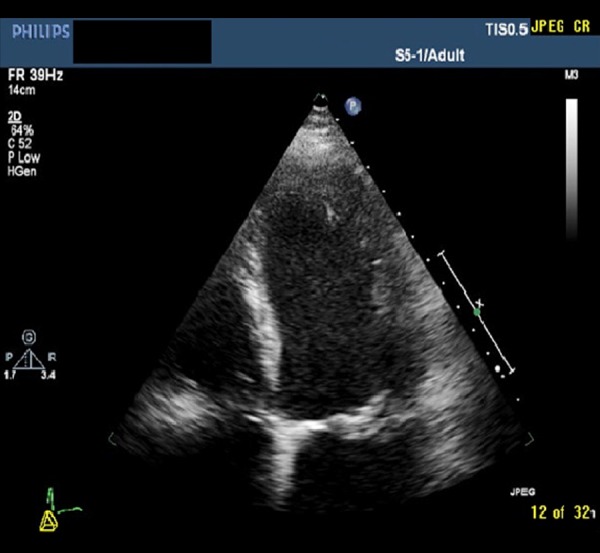
As a general rule, visualizing mitral valve prolapse on a four-chamber view will be less specific than apical two-chamber or parasternal long-axis views, as seen in Figure 6 this patient’s echocardiogram was performed using a more specific method in parasternal long-axis view [8].
Figure 6.

Transthoracic 2 D and color Doppler images in parasternal long.
References
- 1.Savage D, Garrison R, Devereux R, et al. Mitral valve prolapse in the general population. 1. Epidemiologic features: The Framingham Study. Am Heart J. 1983;106:571–76. doi: 10.1016/0002-8703(83)90704-4. [DOI] [PubMed] [Google Scholar]
- 2.Hulin A, Deroanne C, Lambert C, et al. Emerging pathogenic mechanisms in human myxomatous mitral valve: lessons from past and novel data. Cardiovasc Pathol. 2013;22:245–50. doi: 10.1016/j.carpath.2012.11.001. [DOI] [PubMed] [Google Scholar]
- 3.Sainger R, Grau J, Branchetti E, et al. Human myxomatous mitral valve prolapse: Role of bone morphogenetic protein 4 in valvular interstitial cell activation. J Cell Physiol. 2012;227:2595–604. doi: 10.1002/jcp.22999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hayek E, Gring C, Griffin B. Mitral valve prolapse. Lancet. 2005;365:507–18. doi: 10.1016/S0140-6736(05)17869-6. [DOI] [PubMed] [Google Scholar]
- 5.Yuan S. Clinical significance of mitral leaflet flail. Cardiol J. 2009;16:151–56. [PubMed] [Google Scholar]
- 6.Calafiore A, Mauro M, Actis-Dato G, et al. Longitudinal plication of the posterior leaflet in myxomatous disease of the mitral valve. Ann Thorac Surg. 2006;81:1909–10. doi: 10.1016/j.athoracsur.2005.02.067. [DOI] [PubMed] [Google Scholar]
- 7.Carpentier A. Cardiac valve surgery: The French correction. J Thorac Cardiovasc Surg. 1983;86:323–37. [PubMed] [Google Scholar]
- 8.Feigenbaum H, Armstrong W, Ryan T, et al. Feigenbaum’s echocardiography. 6Pth ed. Philadelphia (PA): Lippincott Williams and Wilkins; 2005. [Google Scholar]
- 9.Fedak P, McCarthy P, Bonow R. Evolving concepts and technologies in mitral valve repair. Circulation. 2008;117:963–74. doi: 10.1161/CIRCULATIONAHA.107.702035. [DOI] [PubMed] [Google Scholar]