

Summary:
Breast surgery is one of the most frequently performed surgeries in hospitals and can be associated with significant postoperative pain. We report a novel technique of intraoperative lateral pectoral nerve block under direct vision for analgesia post subpectoral implant placement for breast reconstruction.
We report a novel technique of intraoperative lateral pectoral nerve block under direct vision for analgesia after subpectoral implant placement for breast reconstruction. Breast surgery is one of the most frequently performed surgeries in hospitals, and even minor breast surgery can be associated with significant postoperative pain.1
Blanco et al2 describe the “pecs block” of the lateral pectoral nerve under ultrasound guidance, which was found to be particularly useful for patients who have had breast expanders and implants. Similarly, Semenza3 reported a case of successful ultrasound-guided blockade of the lateral pectoral nerve to improve postoperative analgesia after submuscular breast augmentation. Leiman et al4 report blockade of the medial and lateral pectoral nerves under ultrasound guidance that results in complete relaxation of the pectoralis major and reduction in postoperative pain.
The paravertebral approach providing multilevel intercostal nerve block is another technique providing a similar level of analgesia that we have used for such breast cases. It also provides excellent analgesia, similar to that seen with skin infiltration plus lateral pectoral nerve block but accessing the paravertebral or intercostal space always carries a small risk of accidental pneumothorax.5 Although thoracic intercostal nerves provide sensory innervation to the breast, significant pain afferents from the muscle are carried by the lateral pectoral nerve after submuscular prosthesis placement.3
The pectoralis major muscle is principally supplied by the lateral pectoral nerve via spinal segments C5, C6, and C7 and the medial pectoral nerve (C8, T1). The lateral pectoral nerve is readily visualized emerging from the clavipectoral fascia along with the pectoral branch of the thoracoacromial artery during elevation of the pectoralis major muscle; the medial pectoral nerve (C8, T1) pierces pectoralis minor to run on the undersurface of pectoralis major and supplies the lower costal fibers.6 Submuscular implant placement, therefore, provides an opportune time to block the lateral pectoral nerve (and communicating fibers from medial pectoral nerve) intraoperatively.
During surgery, for postmastectomy breast reconstruction or cosmetic subpectoral implants, the pectoralis major muscle is elevated from its inferolateral aspect. Once the muscle is dissected off its costal attachments, blunt dissection is carried out until the lateral pectoral nerve is visualized emerging from the clavipectoral fascia. Using a blunt tip cannula, 10 mL of 0.75% ropivacaine is infiltrated around the lateral pectoral nerve under direct visualization. Blockade of the nerve is conducted just before implant placement (Fig. 1).
Fig. 1.
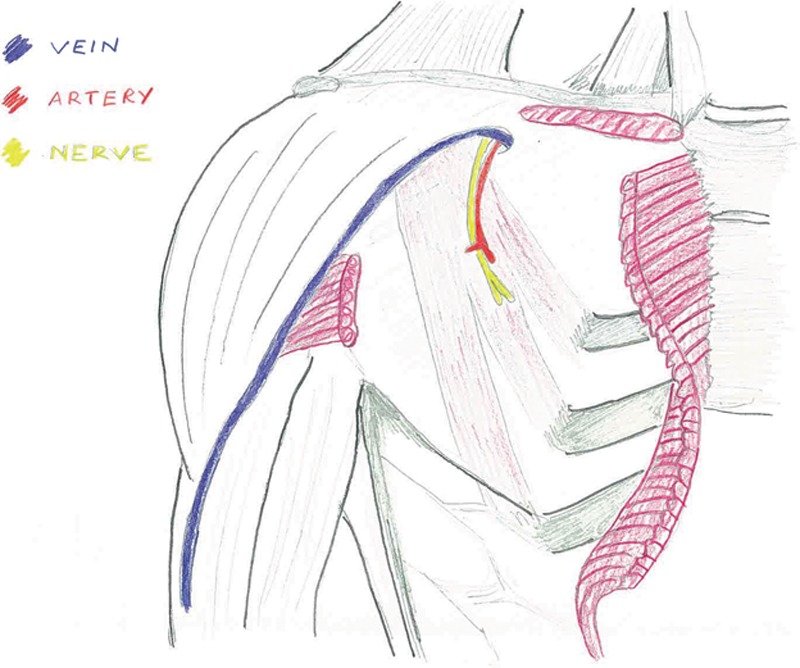
Schematic demonstrating the lateral pectoral nerve emerging from the clavipectoral fascia with the pectoral branch of the thoracoacromial artery and the cephalic vein (pectoralis major muscle cut and reflected).
We routinely do this procedure on all subpectoral prosthetic breast reconstructions and subpectoral breast augmentation and agree with Blanco et al2 that it significantly reduces postoperative pain and opiate requirements. Before introduction of the lateral pectoral nerve block, our usual practice was to prescribe regular paracetamol and COX 2 NSAID with a patient controlled analgesia device containing fentanyl. With the use of routine lateral pectoral nerve block performed by the surgeon before insertion of the subpectoral prosthesis, most of our patients no longer utilize the patient controlled analgesia device and manage their postoperative pain with paracetamol and NSAIDS with the additional likely benefit of reducing the opiate-related side effects of sedation, nausea, and constipation. Further studies should quantify the efficacy of this block by assessing postoperative opiate requirements and patient satisfaction (Fig. 2).
Fig. 2.
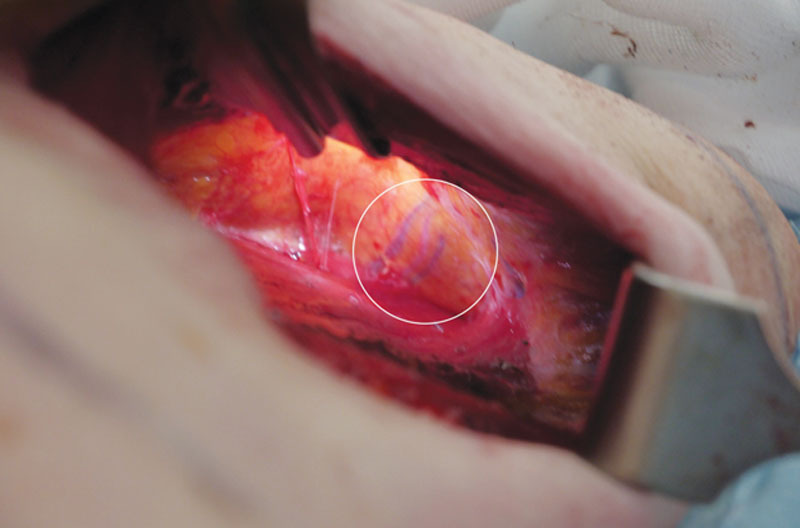
Intraoperative image—left breast inframammary fold incision, visualizing the lateral pectoral nerve on the undersurface of the pectoralis major muscle.
Footnotes
Disclosure: The authors have no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the authors.
REFERENCES
- 1.Soto Pérez A., Luis Juan C, Bosser J, et al. Peripheral blocks for analgesia in breast cancer surgery. Eur J Anaesthesiol. 2014;31:137. [Google Scholar]
- 2.Blanco R, Fajardo M, Parras Maldonado T. Ultrasound description of Pecs II (modified Pecs I): a novel approach to breast surgery. Rev Esp Anestesiol Reanim. 2012;59:470–475. doi: 10.1016/j.redar.2012.07.003. [DOI] [PubMed] [Google Scholar]
- 3.Semenza M. Lateral pectoral nerve blocks after breast augmentation. In: ASRA 38th Annual Regional Anesthesia and Acute Pain Medicine Meeting, Boston, Massachusetts. 2013 May;Spring 2013 [Google Scholar]
- 4.Leiman D, Barlow M, Carpin K, et al. Medial and lateral pectoral nerve block with liposomal bupivacaine for the management of postsurgical pain after submuscular breast augmentation. Plast Reconstr Surg Glob Open. 2014;2:e282. doi: 10.1097/GOX.0000000000000253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Downs CS, Cooper MG. Continuous extrapleural intercostal nerve block for post thoracotomy analgesia in children. Anaesth Intensive Care. 1997;25:390–397. doi: 10.1177/0310057X9702500412. [DOI] [PubMed] [Google Scholar]
- 6.McMinn RMH. 9th ed. United Kingdom: Churchill Livingstone;; Last’s Anatomy Regional and Applied. [chapter 2] [Google Scholar]