

Abstract
Background and study aims: Techniques to optimize endoscopic ultrasound-guided tissue acquisition (EUS-TA) in a variety of lesion types have not yet been established. The primary aim of this study was to compare the diagnostic yield (DY) of endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) to endoscopic ultrasound-guided fine needle biopsy (EUS-FNB) for pancreatic and non-pancreatic masses.
Patients and methods: Consecutive patients referred for EUS-TA underwent randomization to EUS-FNA or EUS-FNB at four tertiary-care medical centers. A maximum of three passes were allowed for the initial method of EUS-TA and patients were crossed over to the other arm based on on-site specimen adequacy.
Results: A total of 140 patients were enrolled. The overall DY was significantly higher with specimens obtained by EUS-FNB compared to EUS-FNA (90.0 % vs. 67.1 %, P = 0.002). While there was no difference in the DY between the two groups for pancreatic masses (FNB: 91.7 % vs. FNA: 78.4 %, P = 0.19), the DY of EUS-FNB was higher than the EUS-FNA for non-pancreatic lesions (88.2 % vs. 54.5 %, P = 0.006). Specimen adequacy was higher for EUS-FNB compared to EUS-FNA for all lesions (P = 0.006). There was a significant rescue effect of crossover from failed FNA to FNB in 27 out of 28 cases (96.5 %, P = 0.0003). Decision analysis showed that the strategy of EUS-FNB was cost saving compared to EUS-FNA over a wide range of cost and outcome probabilities.
Conclusions: Results of this RCT and decision analysis demonstrate superior DY and specimen adequacy for solid mass lesions sampled by EUS-FNB.
Introduction
Endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) is the standard of care for tissue sampling of pancreatic masses along with lesions within and adjacent to the gastrointestinal tract 1. The diagnostic yield of EUS-FNA has been reported to be between 50 % to 98 % depending on the lesion type 2 3. Techniques to optimize EUS-FNA in a variety of lesion types have not yet been established. Several technical variables have been studied, including needle gauge, use of stylet, and use of suction or capillary (“slow pull”) techniques. While various observational studies have shown some impact on EUS-FNA, alterations within these variables have not been demonstrated to consistently improve diagnostic yield 4 5 6 7 8. In addition, EUS-FNA has limitations. The adequacy of a specimen may be dependent on the availability of on-site cytopathology evaluation 9 10 11 12 13. Tissue architecture and morphology is often difficult to maintain in EUS-FNA samples 14 15 16. This may limit immunohistochemistry or immunophenotyping, which is often helpful to establish a diagnosis for neoplasms such as lymphoma, metastasis, or subepithelial lesions 17 18 19 20 21.
Given these shortcomings, new approaches have shifted to the development of EUS-guided fine needle biopsy (EUS-FNB). Initial experience with a tru-cut (Quick CoreTM, Cook Medical, Winston-Salem, NC) biopsy needle was limited by the needle stiffness and difficulty with the firing mechanism 22. More recently, a new generation of core biopsy needles have been introduced (Echotip ProcoreTM, Cook Medical, Winston-Salem, NC). Multiple prospective cohort studies have suggested a significant improvement in diagnostic yield with EUS-FNB, while one RCT and some retrospective series have shown varying results 19 22 23. To date, there is limited published data comparing EUS-FNA and EUS-FNB with regard to diagnostic yield in pancreatic and non-pancreatic masses. In addition, the cost effectiveness of EUS-FNA and EUS-FNB tissue acquisition techniques has not been previously evaluated. We hypothesized that EUS-FNB provides higher diagnostic yield than EUS-FNA. In this multicenter, prospective, randomized controlled trial, we aimed to compare the diagnostic yield between EUS-FNA and EUS-FNB in patients undergoing EUS-guided tissue acquisition (EUS-TA) for pancreatic and non-pancreatic masses.
Patients and methods
Study design
This prospective, randomized, cross-over, multicenter trial was conducted at four tertiary-care medical centers: Northwestern Memorial Hospital, Chicago, IL; California Pacific Medical Center, San Francisco, CA; Moffitt Cancer Center, Tampa, FL; and University of California Los Angeles, Los Angeles, CA. The study was approved by the institutional review board at each participating center.
Study population
Consecutive patients referred for EUS-TA of solid masses (pancreas, lymph nodes, metastases, and subepithelial lesions) were prospectively enrolled from January 2013 through May 2014. The inclusion criteria included age greater than 18 years and presence of a solid mass lesion confirmed by at least one single investigational modality mainly computed tomography, magnetic resonance imaging, or endoscopy. Exclusion criteria were coagulopathy (INR > 1.5), thrombocytopenia (< 50,000), episode of acute pancreatitis in the preceding 4 weeks, inability to safely perform EUS-TA, and refusal or inability to provide informed consent.
EUS-FNA/FNB procedure
All procedures were performed by experienced endosonographers, each of whom had performed more than 1000 cases. The curvilinear array echoendoscope (GF-UC140P or GF-UCT140, Olympus America, Center Valley, PA) was used in all cases.
EUS-FNA was performed using commercially available needles (EchotipTM, Cook Medical, Winston-Salem, NC; ExpectTM, Boston Scientific, Natick MA). Randomization of needle gauge, use of suction or “slow pull” technique, and use of stylet was not performed for this RCT and left to the discretion of the endosonographer. After the lesion was identified, it was punctured under Doppler guidance and approximately 10 to 15 back-and-forth movements were performed with the FNA needle into the target lesion using 10 mL of suction or the capillary “slow pull” technique.
EUS-FNB was performed using the (Echotip ProcoreTM, Cook Medical, Winston-Salem, NC) needle. The ProcoreTM needle is composed of nitinol, contains a novel reverse cutting bevel design for procurement of a core specimen, and is available in 19 – 22-, and 25-G sizes. The needle gauge was again left to the discretion of the endosonographer. For FNB, the capillary technique was used with a stylet (no syringe suction) with approximately 10 to 15 back-and-forth movements in the target lesion to acquire the core specimen. Endosonographers were not permitted to change needle gauge or use of suction/stylet during the 3 passes.
Randomization
Patients were centrally randomized to one of two arms: EUS-FNA or EUS-FNB. Randomization was performed by a computerized binary random number generator at the primary site (Northwestern University). The order of EUS-TA technique was determined using an opaque sealed envelope.
Study protocol
After randomization, a needle (FNA/FNB) was selected by the endosonographer. A maximum of three passes were allowed to obtain an adequate specimen as assessed by an on-site cytopathologist/cytotechnologist. If an adequate specimen was not obtained after three passes, the patient was crossed over to the alternate EUS-TA modality. An additional three passes were permitted in order to obtain an adequate specimen (Fig. 1).
Fig. 1 .
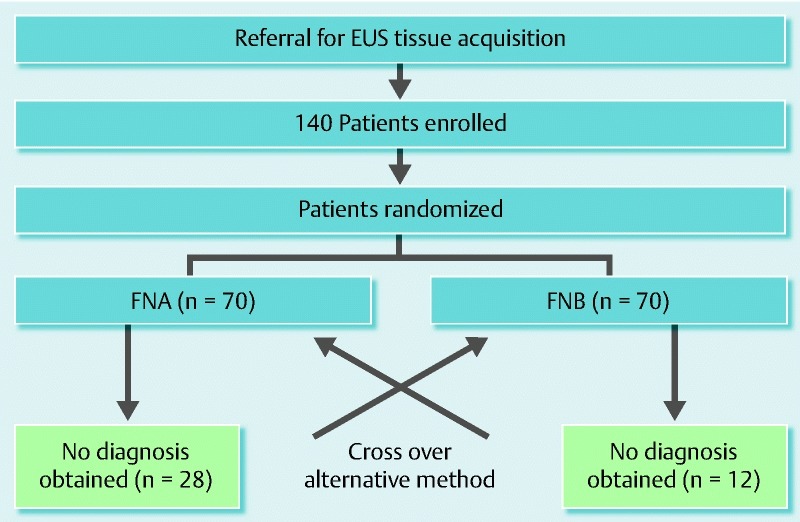
Study flow chart
Cytopathologic and histologic assessment
After tissue acquisition, the specimens were expressed onto a slide using a stylet and/or air flush. All FNA and FNB smears were prepared and assessed for adequacy on site by a cytotechnician/cytopathologist and subsequently confirmed by an experienced cytopathologist. Cytopathologists/cytotechnicans were not blinded to the tissue acquisition method due to the need for specialized preparation of the sample depending on the technique used. Furthermore, the acquisition of a tissue core by EUS-FNB would be clearly visible, and lead to unblinding of the cytotechnician/cytopathologist. When performing EUS-FNA, one slide was air dried and prepared with Diff-Quik stain for on-site analysis. The second slide was fixed in alcohol solution to be stained later with Papanicolaou stain. Remaining FNA aspirate was placed into a standard cytologic solution for cell block preparation. When performing EUS-FNB, core specimens were prepared on slides using either smash or touch preparation according to the presence of fragmented tissue or a visible core specimen 24. If the tissue acquired contained a visible core, a standard touch preparation was utilized. The touch preparation technique was performed by carefully placing the visible core specimen onto a slide and slowly moving the specimen around the slide before placing the specimen into a container with formalin for subsequent histologic evaluation. In the event that only fragmented or scant tissue was obtained, the smash protocol was performed: the tissue was put on a slide, and a second slide was used to gently crush the tissue between the two slides to prepare an air-dried crush preparation; any residual tissue was fixed in formalin for subsequent H&E staining and histologic evaluation.
Each pass was assessed immediately for cellular adequacy and a final diagnosis was determined after review of all FNA or FNB material. Once an adequate specimen was obtained, the procedure was terminated. The final diagnosis was categorized as diagnostic or non-diagnostic (defined to include suspicious and atypical readings) and was standardized among all participating cytopathologists.
Outcome measures and study definitions
The primary aim of this study was to compare the diagnostic yield of EUS-FNA and EUS-FNB overall for all lesions. Our secondary aims included comparison of: (1) technical success; (2) diagnostic yield for pancreas and non-pancreas mass subgroups; (3) on-site specimen adequacy for EUS-FNA and EUS-FNB; (4) salvage effect of EUS-FNA and EUS-FNB; (5) cost-effectiveness analysis comparing EUS-FNA and EUS-FNB for pancreatic and non-pancreatic masses; and (6) adverse events. For this study we used the following standardized definitions: (1) diagnostic yield: percentage of the lesions sampled for which a tissue diagnosis is obtained; and (2) on-site specimen adequacy: the percentage of lesions sampled in which the obtained material is representative of the target site.
Sample size and statistical analysis
A sample size calculation was performed to conduct a between-subjects comparison of EUS-FNA and EUS-FNB. Based on a literature review of EUS-FNA and EUS-FNB for heterogeneous indications, we expected a difference in diagnostic yield of 20 % for all lesion types (pancreatic and non-pancreatic) between EUS-FNB (90 %) and EUS-FNA (70 %) after three needle passes. Using these criteria, a total of 140 patients were required with 70 patients in each arm. Results for continuous variables are expressed by using mean ± standard deviation. Frequencies and percentages were calculated for categorical variables. Student's t-test was used to compare normally distributed continuous variables. Wilcoxon rank-sum test was used for variables not normally distributed and χ 2analysis was used to compare the association between categorical variables and outcomes. McNemar test was used to compare paired binary data. A P value < 0.05 was considered significant and all statistical analyses were conducted using SAS version 9.2 (SAS Institute, Inc., Cary, North Carolina). The results are reported in accordance with the CONSORT statement 25.
Decision analysis
A decision analysis tree was constructed using decision analysis software (TreeAge Pro, TreeAge Software, Williamstown, MA) and two competing strategies were evaluated from a third-party-payer perspective in a hypothetical cohort of patients with pancreatic and non-pancreatic masses undergoing EUS for EUS-guided tissue acquisition ( Fig. 2). Under strategy I, all patients underwent EUS-FNB without on-site cytopathology evaluation and specimens obtained were submitted to pathology for histologic evaluation. Under strategy II, all patients underwent EUS-FNA and slides from each EUS FNA pass were prepared by an on-site cytology technician and a cytopathologist interpreted the slides immediately during the procedure to assess for adequacy and preliminary diagnosis. It was assumed that all cases were performed under monitored anesthesia care. In this decision analysis model, unlike the RCT, no cross-over design was followed. Under both strategies, repeat EUS was performed if clinically indicated in case the first EUS FNA/FNB was non-diagnostic. The model did not consider any cost associated with further work-up beyond two non-diagnostic EUS procedures. Data on parameters such as diagnostic yield and adequacy of sampling with EUS-FNA and FNB and incremental diagnostic yield with second EUS procedures were obtained from results of this study and published data. The analysis was performed from a third-party-payer perspective, and Centers for Medicare and Medicaid Services (CMS) data on EUS FNA/FNB procedural reimbursement, procedural sedation costs with monitored anesthesia care, and pathology interpretation of on-site and off-site cytology slides were used. Cost parameters in terms of utilization and salary of the cytology technician were obtained from institutional data. Baseline estimates (data from the current randomized controlled trial and available literature) and costs were varied by using a sensitivity analysis through the ranges as shown in Table 1 26 27 28 29 30 31 32. Monte Carlo simulation analysis was performed in a hypothetical cohort of 1000 patients undergoing EUS and the incremental costs were calculated.
Fig. 2.
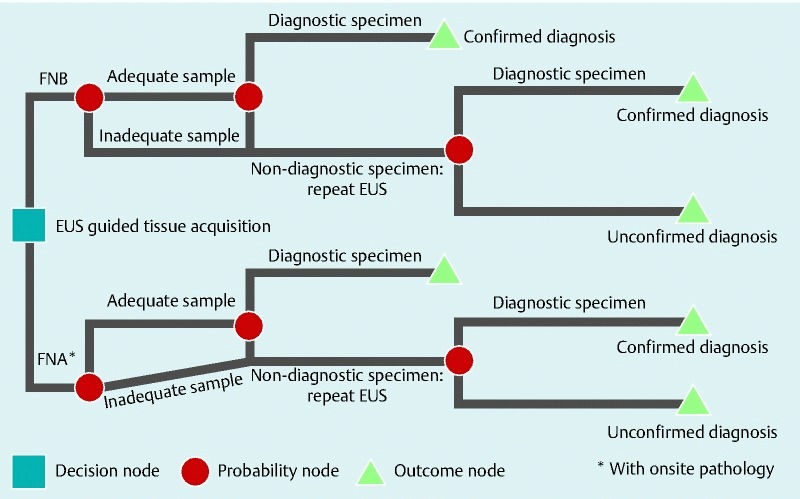
Decision analysis tree showing the structure of the decision analysis model comparing the two competing strategies: EUS-FNB and EUS-FNA. In the decision tree, squares, circles, and triangles represent decision, probability and outcome nodes, respectively.
Table 1. Relevant clinical probability estimates and costs used in the decision analysis.
| Clinical probabilities and costs | Baseline (range) | Source |
| Cost variables | ||
| EUS FNA/FNB reimbursement | $ 1315 (900 – 1500) | CMS |
| Cost of FNB histology interpretation | $ 48 (45 – 60) | CMS |
| Cost of slide interpretation: onsite cytology | CMS | |
| a) First slide | $ 45.58 | |
| b) Subsequent slide each | $ 20.56 | |
| Annual salary of cytology technician | $ 65,000 (40,000 – 80,000) | Institutional data |
| National CMS reimbursement 2013, Anesthesiologist per unit | $ 21.95 | CMS |
| Clinical probabilities | ||
| Number of passes | ||
| a) with EUS FNA and onsite cytology | 5 (3 – 7) | 13 19 26 |
| b) with EUS-FNB | 2 | 26 |
| Pancreatic lesions | ||
| Probability of adequate sample with FNB | 0.81 (0.54 – 0.9) | Current study, 23 24 27 28 29 |
| Probability of adequate sample with FNA and onsite cytology evaluation | 0.65 (0.5 – 0.95) | Current study, 11 13 |
| Diagnostic yield of malignancy with FNB | 0.92 (0.7 – 0.95) | Current study, 23 24 27 28 29 |
| Diagnostic yield of malignancy with FNA | 0.78 (0.55 – 0.85) | Current study, 12 30 |
| Non-pancreatic lesions | ||
| Probability of adequate sample with FNB | 0.82 (0.54 – 0.9) | Current study, 19 23 24 28 29 |
| Probability of adequate sample with FNA and onsite cytology evaluation | 0.52 (0.5 – 0.95) | Current study, 12 31 32 |
| Diagnostic yield of malignancy with FNB | 0.88 (0.7 – 0.95) | Current study, 19 23 24 28 29 |
| Diagnostic yield of malignancy with FNA | 0.55 (0.5 – 0.85) | Current study, 12 31 32 |
Results
Patients
A total of 140 (70 EUS-FNA, 70 EUS-FNB) consecutive subjects were enrolled in the study over a 17-month period. Seventy-four patients (52.8 %) were male. There were no differences in patient demographics and lesion characteristics between the two groups. Furthermore, pancreatic and non-pancreatic lesions were distributed evenly between EUS-FNA and EUS-FNB (Table 2).
Table 2. Patient demographics and lesion characteristics.
| Characteristic | FNA(n = 70) | FNB(n = 70) | P value |
| Mean age (SD) | 63.7 (14.4) | 64.0 (14.4) | 0.88 |
| Male (n, %) | 34 (48.6) | 40 (57.1) | 0.24 |
| Caucasian (n, %) | 43 (61.4) | 44 (62.9) | 0.13 |
| Mean lesion size mm (SD) | 30.2 (18.7) | 29.2 (14.1) | 0.71 |
| Pancreatic masses (n, %) | 37 (52.9) | 36 (51.4) | 0.99 |
| Non-pancreatic masses (n, %) | 33 (47.1) | 34 (48.6) | 0.98 |
| Thoracic/abdominal/pelvic mass | 16 | 15 | 0.78 |
| Lymphadenopathy | 10 | 11 | 0.88 |
| Subepithelial lesions | 7 | 8 | 0.67 |
Tissue acquisition techniques
EUS-TA was technically successful in all patients without any adverse events. For patients randomized to the EUS-FNA arm, a 22 G needle was used in 48 (68.6 %) while a 25 G needle was used in 22 (31.4 %). For patients randomized to the EUS-FNB arm, a 19 G needle was used in 7 (10 %), a 22 G needle in 37 (52.8 %), and a 25 G needle in 26 (37.1 %). There was no significant difference in needle gauge or the number of passes performed (FNA mean ± [SD] 3.0 ± (1.0), FNB mean ± [SD] 2.8 ± (1.0), P = 0.20) with FNA and FNB techniques (Table 3).
Table 3. Summary of tissue acquisition results.
| Characteristic | FNA (n = 70) | FNB (n = 70) | P value |
| Mean no. of passes mean (SD) | 3.0 (1.0) | 2.8 (1.0) | 0.20 |
| Needle Size (n, %) | 0.051 | ||
| 19-G | 0 (0) | 7 (10) | |
| 22-G | 48 (68.6) | 37 (52.9) | |
| 25-G | 22 (31.4) | 26 (37.1) | |
| Diagnostic yield (n, %) | 47/70 (67.1) | 63/70 (90) | 0.002 |
| Pancreatic | 29/37 (78.4) | 33/36 (91.7) | 0.19 |
| Non-pancreatic | 18/33 (54.5) | 30/34 (88.2) | 0.006 |
| Specimen adequacy (n, %) | 42/70 (60.0) | 58/70 (82.8) | 0.006 |
| Pancreatic | 25/37 (67.5) | 30/36 (83.3) | 0.19 |
| Non-pancreatic | 17/33 (51.5) | 28/34 (82.4) | 0.019 |
| Crossover diagnostic yield (n, %) | |||
| FNA to FNB (n = 28) | 27 (96.4 %) | 0.0003 | |
| FNB to FNA (n = 12) | 5 (41.7)% | 0.99 |
Diagnostic yield
The overall DY was significantly higher with specimens obtained by EUS-FNB compared to EUS-FNA (90 % vs. 67.1 %, P = 0.002). Non-pancreatic lesions were associated with a higher diagnostic yield with the FNB technique compared to FNA (88.2 % vs. 54.5 %, P = 0.006). There was no statistically significant difference between EUS-FNA and EUS-FNB for pancreas masses (91.7 % vs. 78.4 %, P = 0.19). The differences observed were independent of lesion size, number of passes, use of suction or stylet, or needle gauge (Table 3). Final diagnosis by lesion type is listed in supplementary Table 1.
Specimen adequacy
The overall specimen adequacy was significantly greater for EUS-FNB compared to EUS-FNA (82.8 % vs. 60.0 %, P = 0.006). Greater specimen adequacy was observed in non-pancreatic lesions sampled by EUS-FNB (82.4 % vs. 51.5 %, P = 0.019). There was no statistically significant difference in specimen adequacy for pancreatic masses between EUS-FNA and EUS-FNB (83.3 % vs. 67.5 %, P = 0.19).
Crossover salvage effect
We also evaluated the salvage effect of the alternative tissue acquisition method when the initial three passes with either EUS-FNA or EUS-FNB failed to provide an adequate specimen. There was a significant salvage effect in diagnostic yield for crossover from failed EUS-FNA to EUS-FNB in 27 out of 28 cases (96.4 %, P = 0.0003). This effect was independent of lesion subtype (15 non-pancreatic vs. 12 pancreatic, P = 0.12). In contrast, a diagnosis was established in only 5/12 cases (41.7 %, P = 0.99) of failed EUS-FNB that were crossed over to EUS-FNA. This effect was also independent of lesion subtype (3 non-pancreatic vs. 2 pancreatic, P = 0.76).
Decision analysis results
The results of baseline analysis are shown in Table 4. Comparing the two strategies for pancreatic and non-pancreatic masses, strategy II of EUS-FNA was dominated by strategy I of EUS-FNB in that it was more expensive. The results of the Monte Carlo analysis for pancreatic masses showed that under strategy I, EUS-FNB confirmed diagnosis in 988 patients at an average cost of $ 2,152 (95 % CI, 2070 – 2162) per patient and under strategy II, EUS-FNA confirmed diagnosis in 921 patients at an average cost of $ 2,605 (95 % CI, 2263 – 2664) per patient. The results of the Monte Carlo analysis for non-pancreatic masses showed that under strategy I, EUS-FNB confirmed diagnosis in 991 patients at an average cost of $ 1921 (95 % CI, 1874 – 1968) per patient and under strategy II, EUS-FNA confirmed diagnosis in 725 patients at an average cost of $ 2942 (95 % CI, 2901 – 2985) per patient. Supplementary Fig. 1 is a Tornado diagram showing the results of one-way sensitivity analyses of the important variables impacting the outcomes of the decision analysis. Besides the costs of the EUS procedure and sedation, sample adequacy and diagnostic yield of EUS-FNB had the most influence on the results. Supplementary Fig. 2 a and b show the results of the two-way sensitivity analyses when probability of sample adequacy and diagnostic yield with both tissue sampling techniques are varied simultaneously. The robustness of the results of this decision analysis is highlighted by the analyses (with all the reported values of adequacy of sampling and diagnostic yield from the current study and published data) and suggests that EUS-FNB is potentially more economical compared to EUS-FNA.
Table 4. Results of baseline analysis.
| Baseline analysis | Cost ($) per procedure | Incremental cost |
| Pancreatic lesions | ||
| FNB | $ 1926 | |
| FNA with on-site cytopathology | $ 2538 | $ 612 |
| Non-pancreatic lesions | ||
| FNB | $ 1931 | |
| FNA with on-site cytopathology | $ 2926 | $ 995 |
Supplementary Fig. 1.
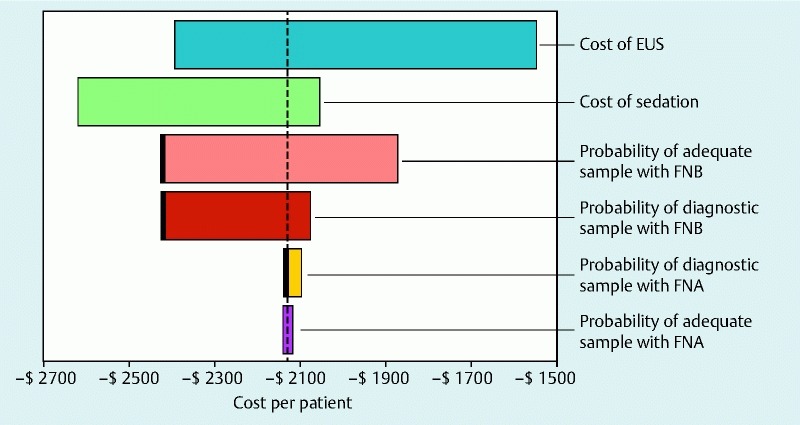
Tornado diagram examining the impact of important cost and outcome variables on the results of the decision analysis, with cost per patient along the X axis. In the tornado diagram, the uncertainty in the parameter associated with the largest bar, the one at the top of the chart has the maximum impact on the result, with each successive lower bar having a lesser impact. Also, thick vertical lines in the tornado diagram identify the threshold points where EUS-FNA becomes more economical (i. e. model conclusion is reversed). When the probability of adequate sampling by EUS-FNB falls below 0.38, probability of diagnostic yield of EUS-FNB falls below 0.65 and the probability of diagnostic yield of EUS-FNA is higher than 0.87. Similar results were noted for pancreatic and non-pancreatic masses.
Supplementary Fig. 2 a.
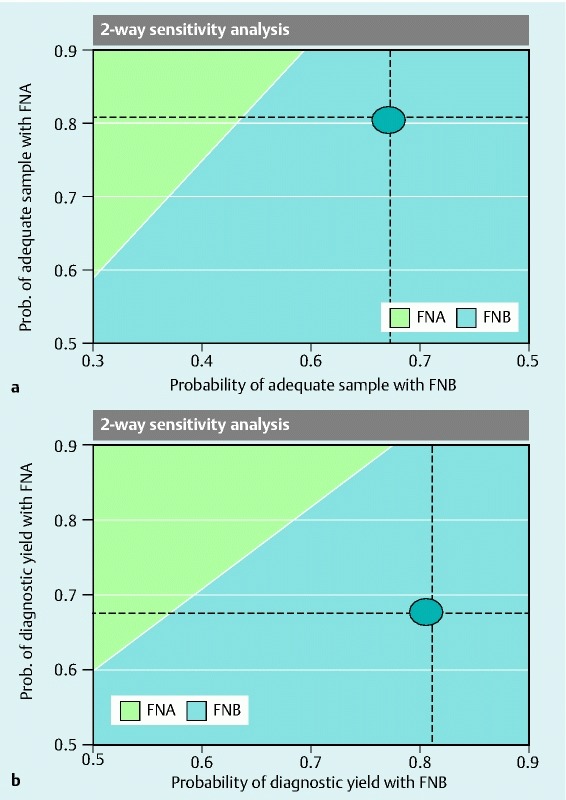
and b Results of a two-way sensitivity analysis with the X axis showing probability of adequate sampling by EUS-FNB and the Y axis showing probability of adequate sampling of EUS-FNA. When both these variables are simultaneously varied in the model, and the output of the model is plotted, any point in the blue shaded area favors EUS-FNB-based strategy and any point in the green cross-hatched area favors EUS-FNA-based strategy. Similarly, Supplementary Fig. 2 b shows the result of a two-way sensitivity analysis with the X axis showing probability of diagnostic yield by EUS-FNB and the Y-axis showing probability of diagnostic yield of EUS-FNA. Blue circles in both figures represent when the data from the current RCT were plotted. It is evident that in a wide range of possibilities of these parameters around the point derived from this study, the EUS-FNB-based strategy is more economical. Similar results were noted for pancreatic and non-pancreatic masses.
Discussion
The optimal EUS-TA technique has not been clearly defined. This gap is further underscored by the lower DY for non-pancreatic mass lesions. However, recent data suggest that EUS-FNB may improve DY 23 33 34 35. In this multicenter, randomized controlled trial with crossover design, we compared the diagnostic yield of EUS-FNA and EUS-FNB in pancreatic and non-pancreatic mass lesions. Results of this study demonstrated a significantly higher overall DY of EUS-FNB over EUS-FNA in non-pancreatic lesions.
Data are limited from randomized controlled trials comparing EUS-FNA to EUS-FNB in non-pancreatic mass lesions. 35 36 The published diagnostic yield of EUS-FNA for gastric subepithelial masses ranges from 42 % to 92 % 37 38. Recently, Kim et al. conducted a randomized controlled trial of 22 patients with gastric subepithelial tumors. Patients who were randomized to EUS-FNB had significantly higher diagnostic yield compared to patients who underwent EUS-FNA (75 % vs. 20 %, P = 0.010) 28. Previously published prospective studies have also noted high diagnostic accuracy of the FNB technique in non-pancreatic mass lesions 23 35. A recent study evaluated 125 patients with non-pancreatic masses using the 22-G core biopsy needle. They demonstrated a diagnostic yield of 83 % 34. In another prospective cohort study, Iglesias-Garcia and colleagues evaluated the performance of the 19-G FNB needle in 114 patients. They reported a diagnostic accuracy of 83.5 % in the 67 patients with non-pancreatic lesions 23. Our study results indicate a significantly greater diagnostic yield with EUS-FNB of non-pancreatic lesions of 88.2 % compared to 54.5 % with EUS-FNA (P = 0.006), suggesting that EUS-FNB is the optimal modality for tissue acquisition in non-pancreatic masses.
The role of EUS-FNA for pancreatic mass lesions is well established with diagnostic yield greater than 90 % 39. The pooled sensitivity from five meta-analyses on EUS-FNA for solid pancreatic mass lesions is 85 % to 89 %, with higher diagnostic accuracy in prospective, multicenter studies 10 40 41 42. In addition, prior prospective studies comparing FNA and FNB techniques for pancreatic mass lesions have failed to show a benefit for the FNB technique. In another prospective, randomized, controlled trial of 28 patients, Bang and colleagues evaluated the efficacy of a 22-G FNA and FNB needle 19. They found no significant difference in diagnostic yield or number of passes required to obtain a diagnosis between the two techniques. However, this study was limited by a very small sample size. In a prospective cohort study of 32 patients with solid pancreatic masses comparing FNA cytology to FNB core histology, Strand et al. actually found that the FNB technique with a 22-G needle was associated with a significantly reduced diagnostic yield compared to FNA (FNA: 93.8 %, FNB: 28.1 %, P < 0.001) 43. However, this study used suction during procurement of FNB, which may have increased the bloodiness and contamination of specimens. Two recently published prospective, randomized trials have also shown no difference in diagnostic yield between EUS-FNA and EUS-FNB for pancreas mass lesions 44 45. Consistent with the previously published literature, results from this randomized controlled trial also showed no difference in diagnostic yield between EUS-FNA and EUS-FNB for pancreatic masses (FNB: 91.7 %, FNA: 78.4 %, P = 0.19).
False-negative diagnoses during EUS-FNA have been reported in 4 % to 45 % of solid pancreatic masses and 6 % to 14 % of lymph nodes 46. False-negative cytology is most often due to inaccurate tissue sampling, lesion characteristics (e. g. necrosis), insufficient endosonographer experience, or misinterpretation of specimens 3. Our study not only highlights the value of EUS-FNB in non-pancreatic lesions, but also demonstrates the value of an FNB specimen as salvage for inadequate FNA. Furthermore, this effect was not dependent on lesion subtype. Therefore, it is important to recognize the lesion characteristics that may pose a challenge to obtaining a tissue diagnosis and use the most appropriate tissue acquisition technique.
Using probabilities from published data and results from this randomized controlled trial, a cost-effectiveness analysis from a societal perspective showed that EUS-FNB (strategy of EUS-FNB – two passes without on-site cytopathology evaluation) was more cost-effective than EUS-FNA (strategy of FNA – passes dictated by on-site cytopathology evaluation) of pancreatic and non-pancreatic masses. While the strategy of EUS-FNB was more cost effective, the authors acknowledge that the decision analysis does not mirror the methodology of the current randomized controlled trial. The strategies used in this decision model reflect current clinical practice with regard to the use of these EUS tissue acquisition techniques. These results were even more pronounced when probabilities regarding specimen adequacy and diagnostic yield from this study were used for the decision model. Results from the Monte Carlo analysis and sensitivity analysis confirmed the above results. Variables with the maximal impact on the results were cost of EUS procedure and sedation, specimen adequacy, and diagnostic yield associated with EUS-FNB.
Our study has several inherent strengths. The study was designed as a prospective, multicenter, randomized controlled trial, thereby minimizing selection and assignment bias. Our sample size was heterogeneous with nearly proportionate number of pancreatic and non-pancreatic masses. There are a few limitations to this study that warrant mention. Patients in the study were not followed longitudinally and, in the absence of a gold standard reference of surgical specimens, accuracy rates could not be determined. Previous data have established the optimal number of passes as seven for EUS-FNA without on-site cytopathology, and three in the presence of on-site cytopathology 6 47. No further significant yield was demonstrated above these threshold numbers. As a result, we allotted three passes per technique prior to crossover. This is potentially responsible for the lower specimen adequacy and DY of EUS-FNA for pancreatic and non-pancreatic masses than what is seen in clinical practice. However, given the standardization across both arms, the effect of this design on the difference in DY is likely minimal 13. Our study was powered to compare diagnostic yield for EUS-FNA and EUS-FNB for pancreatic and non-pancreatic masses combined. Therefore, it was underpowered to detect differences for the subgroup of pancreatic mass lesions, leading to a possible type II error. Our diagnostic yield of EUS-FNA of 78 % for pancreatic lesions is lower than reported in recent randomized trials 19. However, studies with comparable methodologies have reported similar diagnostic yield 48. Furthermore, our DY for EUS-FNA is higher than the recommended threshold of 70 % for quality indicators in EUS 49. The FNA technique and use of needle gauge was not standardized in our study, but rather, left at the discretion of the endosonographer in this multicenter RCT in order to best simulate true clinical practice in addition to the fact that there is lack of level 1 evidence that these variables significantly affect the diagnostic yield. Meta-analysis data has demonstrated increased diagnostic yield of 25-G needles for pancreatic mass lesions, howeve,r in our RCT there was no significant difference between needle gauge in the FNA and FNB groups in our study, thus eliminating any potential bias or benefit in either group 30 50. Our study was performed at high-volume tertiary centers, therefore, there was a bias toward malignant lesions. EUS-FNA was performed in patients with a high pretest probability of malignancy (mass on cross sectional imaging, jaundice, weight loss, elevated CA 19 – 9) as there is increasing utilization of neoadjuvant chemotherapy in the United States which requires a tissue diagnosis. This may limit the broad application of our results to practice settings outside of tertiary centers in the United States.
Lastly, it was not possible to mirror the methodology of the decision analysis with that of the randomized controlled trial, however, the decision analysis adds credence to the RCT results and our recommendations.
In summary, the current RCT demonstrates superior diagnostic yield of EUS-FNB over EUS-FNA. The difference was primarily due to the significantly greater DY of EUS-FNB for non-pancreatic masses. Our results also provide further evidence for the continued use of EUS-FNA for tissue acquisition in pancreatic mass lesions. However, EUS-FNB should be considered as the initial sampling technique for non-pancreatic masses and as a salvage technique when on-site assessment of cytology samples is inadequate. Based on these results, the investigators propose an algorithmic approach to EUS-TA in patients with pancreatic and non-pancreatic masses 3. These results and the approach to EUS-TA need to be validated in future prospective, multicenter, randomized controlled trials.
Supplementary Table 1. Final diagnosis by lesion type.
| Pancreatic lesions (n = 73) | n (%) |
| Adenocarcinoma | 42 (57.5) |
| Pancreatic neuroendocrine tumor | 9 (12.3) |
| Metastatic adenocarcinoma | 9 (12.3) |
| Benign lymphoid cells (reactive LN) | 6 (8.2) |
| Abscess | 1 (1.4) |
| Chronic pancreatitis | 1 (1.4) |
| Leiomyoma | 1 (1.4) |
| Non-diagnostic | 4 (5.5) |
| Non-pancreatic lesions (n = 67) | n (%) |
| Benign lymphoid cells (reactive LN) | 14 (20.9) |
| GIST | 12 (17.9) |
| B-cell Lymphoma | 6 (9.0) |
| Adenocarcinoma | |
| Metastatic adenocarcinoma of unknown primary | 7 (10.5) |
| Metastatic pancreas adenocarcinoma | 4 (6.0) |
| Lung adenocarcinoma | 3 (4.5) |
| Gallbladder adenocarcinoma | 1 (1.5) |
| Metastatic colon adenocarcinoma | 1 (1.5) |
| Metastatic breast adenocarcinoma | 1 (1.5) |
| Leiomyoma/leiomyomasacroma | 3 (4.5) |
| Hepatocellular carcinoma | 2 (3.0) |
| Myxoid tumor | 1 (1.5) |
| Paraganglioma | 1 (1.5) |
| Abscess | 1 (1.5) |
| Pseudopapillary tumor | 1 (1.5) |
| Non-diagnostic | 9 (13.4) |
Competing interests: Drs. Muthusamy and Komanduri are consultants for Boston Scientific and Covidien; Dr. Bhat is a consultant for Covidien; Dr. Das has received research support from RedPath Integrated Pathology and is a consultant for Boston Scientific; Dr. Wani is a consultant for Covidien and has received Educational Grant support from Cook Medical.
Meeting presentations: Digestive Disease Week, May 2014
References
- 1.Early D S, Ben-Menachem T. ASGE Standards of Practice Committee et al. Appropriate use of GI endoscopy. Gastrointest Endosc. 2012;75:1127–1131. doi: 10.1016/j.gie.2012.01.011. [DOI] [PubMed] [Google Scholar]
- 2.Dumonceau J-M, Polkowski M, Larghi A. et al. Indications, results, and clinical impact of endoscopic ultrasound (EUS)-guided sampling in gastroenterology: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy. 2011;43:897–912. doi: 10.1055/s-0030-1256754. [DOI] [PubMed] [Google Scholar]
- 3.Wani S, Muthusamy V R, Komanduri S. EUS-guided tissue acquisition: an evidence-based approach (with videos) Gastrointest Endosc. 2014;80:939–959. doi: 10.1016/j.gie.2014.07.066. [DOI] [PubMed] [Google Scholar]
- 4.Siddiqui U D, Rossi F, Rosenthal L S. et al. EUS-guided FNA of solid pancreatic masses: a prospective, randomized trial comparing 22-gauge and 25-gauge needles. Gastrointest Endosc. 2009;70:1093–1097. doi: 10.1016/j.gie.2009.05.037. [DOI] [PubMed] [Google Scholar]
- 5.Camellini L, Carlinfante G, Azzolini F. et al. A randomized clinical trial comparing 22 G and 25 G needles in endoscopic ultrasound-guided fine-needle aspiration of solid lesions. Endoscopy. 2011;43:709–715. doi: 10.1055/s-0030-1256482. [DOI] [PubMed] [Google Scholar]
- 6.Wani S, Early D, Kunkel J. et al. Diagnostic yield of malignancy during EUS-guided FNA of solid lesions with and without a stylet: a prospective, single blind, randomized, controlled trial. Gastrointest Endosc. 2012;76:328–335. doi: 10.1016/j.gie.2012.03.1395. [DOI] [PubMed] [Google Scholar]
- 7.Lee J K, Choi J H, Lee K H. et al. A prospective, comparative trial to optimize sampling techniques in EUS-guided FNA of solid pancreatic masses. Gastrointest Endosc. 2013;77:745–751. doi: 10.1016/j.gie.2012.12.009. [DOI] [PubMed] [Google Scholar]
- 8.Bang J Y, Ramesh J, Trevino J. et al. Objective assessment of an algorithmic approach to EUS-guided FNA and interventions. Gastrointest Endosc. 2013;77:739–744. doi: 10.1016/j.gie.2012.11.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Alsohaibani F, Girgis S, Sandha G S. Does onsite cytotechnology evaluation improve the accuracy of endoscopic ultrasound-guided fine-needle aspiration biopsy? Can J Gastroenterol. 2009;23:26–30. doi: 10.1155/2009/194351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hébert-Magee S, Bae S, Varadarajulu S. et al. The presence of a cytopathologist increases the diagnostic accuracy of endoscopic ultrasound-guided fine needle aspiration cytology for pancreatic adenocarcinoma: a meta-analysis. Cytopathology. 2013;24:159–171. doi: 10.1111/cyt.12071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Iglesias-Garcia J, Dominguez-Munoz J E, Abdulkader I. et al. Influence of on-site cytopathology evaluation on the diagnostic accuracy of endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) of solid pancreatic masses. Am J Gastroenterol. 2011;106:1705–1710. doi: 10.1038/ajg.2011.119. [DOI] [PubMed] [Google Scholar]
- 12.Klapman J B, Logrono R, Dye C E. et al. Clinical impact of on-site cytopathology interpretation on endoscopic ultrasound-guided fine needle aspiration. Am J Gastroenterol. 2003;98:1289–1294. doi: 10.1111/j.1572-0241.2003.07472.x. [DOI] [PubMed] [Google Scholar]
- 13.Wani S, Mullady D, Early D S. et al. Clinical impact of immediate on-site cytopathology (CyP) evaluation during endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) of pancreatic mass: Interim analysis of a multicenter randomized con- trolled trial. Gastrointest Endosc. 2013;77:2. [Google Scholar]
- 14.Wiersema M J, Vilmann P, Giovannini M. et al. Endosonography-guided fine-needle aspiration biopsy: diagnostic accuracy and complication assessment. Gastroenterology. 1997;112:1087–1095. doi: 10.1016/s0016-5085(97)70164-1. [DOI] [PubMed] [Google Scholar]
- 15.Ribeiro A, Vazquez-Sequeiros E, Wiersema L M. et al. EUS-guided fine-needle aspiration combined with flow cytometry and immunocytochemistry in the diagnosis of lymphoma. Gastrointest Endosc. 2001;53:485–491. doi: 10.1067/mge.2001.112841. [DOI] [PubMed] [Google Scholar]
- 16.Erickson R A, Sayage-Rabie L, Beissner R S. Factors predicting the number of EUS-guided fine-needle passes for diagnosis of pancreatic malignancies. Gastrointest Endosc. 2000;51:184–190. doi: 10.1016/s0016-5107(00)70416-0. [DOI] [PubMed] [Google Scholar]
- 17.Levy M J, Wiersema M J. EUS-guided Trucut biopsy. Gastrointest Endosc. 2005;62:417–426. doi: 10.1016/j.gie.2005.04.044. [DOI] [PubMed] [Google Scholar]
- 18.Jenssen C, Dietrich C F. Endoscopic ultrasound-guided fine-needle aspiration biopsy and trucut biopsy in gastroenterology – An overview. Best Pract Res Clin Gastroenterol. 2009;23:743–759. doi: 10.1016/j.bpg.2009.05.006. [DOI] [PubMed] [Google Scholar]
- 19.Bang J Y, Hebert-Magee S, Trevino J. et al. Randomized trial comparing the 22-gauge aspiration and 22-gauge biopsy needles for EUS-guided sampling of solid pancreatic mass lesions. Gastrointest Endosc. 2012;76:321–327. doi: 10.1016/j.gie.2012.03.1392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Bhutani M S, Gress F G, Giovannini M. et al. The No Endosonographic Detection of Tumor (NEST) Study: a case series of pancreatic cancers missed on endoscopic ultrasonography. Endoscopy. 2004;36:385–389. doi: 10.1055/s-2004-814320. [DOI] [PubMed] [Google Scholar]
- 21.Varadarajulu S, Tamhane A, Eloubeidi M A. Yield of EUS-guided FNA of pancreatic masses in the presence or the absence of chronic pancreatitis. Gastrointest Endosc. 2005;62:728–736. doi: 10.1016/j.gie.2005.06.051. [DOI] [PubMed] [Google Scholar]
- 22.Gerke H, Rizk M K, Vanderheyden A D. et al. Randomized study comparing endoscopic ultrasound-guided Trucut biopsy and fine needle aspiration with high suction. Cytopathology. 2010;21:44–51. doi: 10.1111/j.1365-2303.2009.00656.x. [DOI] [PubMed] [Google Scholar]
- 23.Iglesias-Garcia J, Poley J-W, Larghi A. et al. Feasibility and yield of a new EUS histology needle: results from a multicenter, pooled, cohort study. Gastrointest Endosc. 2011;73:1189–1196. doi: 10.1016/j.gie.2011.01.053. [DOI] [PubMed] [Google Scholar]
- 24.Krishnan K, Dalal S, Nayar R. et al. Rapid on-site evaluation of endoscopic ultrasound core biopsy specimens has excellent specificity and positive predictive value for gastrointestinal lesions. Dig Dis Sci. 2013;58:2007–2012. doi: 10.1007/s10620-013-2613-1. [DOI] [PubMed] [Google Scholar]
- 25.Schulz K F, Altman D G, Moher D. et al. CONSORT 2010 statement: updated guidelines for reporting parallel group randomized trials. Ann Intern Med. 2010;152:726–732. doi: 10.7326/0003-4819-152-11-201006010-00232. [DOI] [PubMed] [Google Scholar]
- 26.Iwashita T, Nakai Y, Samarasena J B. et al. High single-pass diagnostic yield of a new 25-gauge core biopsy needle for EUS-guided FNA biopsy in solid pancreatic lesions. Gastrointest Endosc. 2013;77:909–915. doi: 10.1016/j.gie.2013.01.001. [DOI] [PubMed] [Google Scholar]
- 27.Larghi A, Iglesias-Garcia J, Poley J-W. et al. Feasibility and yield of a novel 22-gauge histology EUS needle in patients with pancreatic masses: a multicenter prospective cohort study. Surg Endosc. 2013;27:3733–3738. doi: 10.1007/s00464-013-2957-9. [DOI] [PubMed] [Google Scholar]
- 28.Hucl T, Wee E, Anuradha S. et al. Feasibility and efficiency of a new 22 G core needle: a prospective comparison study. Endoscopy. 2013;45:792–798. doi: 10.1055/s-0033-1344217. [DOI] [PubMed] [Google Scholar]
- 29.Keswani R N, Krishnan K, Wani S. et al. Addition of Endoscopic Ultrasound (EUS)-guided fine needle aspiration and on-site cytology to EUS-guided fine needle biopsy increases procedure time but not diagnostic accuracy. Clin Endosc. 2014;47:242–247. doi: 10.5946/ce.2014.47.3.242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Madhoun M F, Wani S B, Rastogi A. et al. The diagnostic accuracy of 22-gauge and 25-gauge needles in endoscopic ultrasound-guided fine needle aspiration of solid pancreatic lesions: a meta-analysis. Endoscopy. 2013;45:86–92. doi: 10.1055/s-0032-1325992. [DOI] [PubMed] [Google Scholar]
- 31.Cleveland P, Gill K RS, Coe S G. et al. An evaluation of risk factors for inadequate cytology in EUS-guided FNA of pancreatic tumors and lymph nodes. Gastrointest Endosc. 2010;71:1194–1199. doi: 10.1016/j.gie.2010.01.029. [DOI] [PubMed] [Google Scholar]
- 32.Ecka R S, Sharma M. Rapid on-site evaluation of EUS-FNA by cytopathologist: an experience of a tertiary hospital. Diagn Cytopathol. 2013;41:1075–1080. doi: 10.1002/dc.23047. [DOI] [PubMed] [Google Scholar]
- 33.Witt B L, Adler D G, Hilden K. et al. A comparative needle study: EUS-FNA procedures using the HD ProCore™ and EchoTip® 22-gauge needle types. Diagn Cytopathol. 2013;41:1069–1074. doi: 10.1002/dc.22971. [DOI] [PubMed] [Google Scholar]
- 34.Paik W H, Park Y, Park D H. et al. Prospective evaluation of new 22 gauge endoscopic ultrasound core needle using capillary sampling with stylet slow-pull technique for intra-abdominal solid masses. J Clin Gastroenterol. 2014;49:199–205. doi: 10.1097/MCG.0000000000000084. [DOI] [PubMed] [Google Scholar]
- 35.Kim G H, Cho Y K, Kim E Y. et al. Comparison of 22-gauge aspiration needle with 22-gauge biopsy needle in endoscopic ultrasonography-guided subepithelial tumor sampling. Scandinavian J Gastro. 2014;49:347–354. doi: 10.3109/00365521.2013.867361. [DOI] [PubMed] [Google Scholar]
- 36.Nagula S, Pourmand K, Aslanian H, Orlando FL: 2013. EUS-Fine Needle Aspiration (FNA) vs. EUS-Fine Needle Biopsy (FNB) for solid mass lesions: Interim analysis of a large multicenter, randomized clinical trial. DDW.
- 37.Polkowski M, Larghi A, Weynand B. et al. Learning, techniques, and complications of endoscopic ultrasound (EUS)-guided sampling in gastroenterology: European Society of Gastrointestinal Endoscopy (ESGE) Technical Guideline. Endoscopy. 2012;44:190–206. doi: 10.1055/s-0031-1291543. [DOI] [PubMed] [Google Scholar]
- 38.Varadarajulu S, Hasan M K, Bang J Y. et al. Endoscopic ultrasound-guided tissue acquisition. Dig Endosc. 2014;26 01:62–69. doi: 10.1111/den.12146. [DOI] [PubMed] [Google Scholar]
- 39.Eloubeidi M A, Varadarajulu S, Desai S. et al. A prospective evaluation of an algorithm incorporating routine preoperative endoscopic ultrasound-guided fine needle aspiration in suspected pancreatic cancer. J Gastrointest Surg. 2007;11:813–819. doi: 10.1007/s11605-007-0151-x. [DOI] [PubMed] [Google Scholar]
- 40.Hewitt M JM, McPhail M JWM, Possamai L L. et al. EUS-guided FNA for diagnosis of solid pancreatic neoplasms: a meta-analysis. Gastrointest Endosc. 2012;75:319–3331. doi: 10.1016/j.gie.2011.08.049. [DOI] [PubMed] [Google Scholar]
- 41.Chen G, Liu S, Zhao Y. et al. Diagnostic accuracy of endoscopic ultrasound-guided fine-needle aspiration for pancreatic cancer: a meta-analysis. Pancreatology. 2013;13:298–304. doi: 10.1016/j.pan.2013.01.013. [DOI] [PubMed] [Google Scholar]
- 42.Puli S R, Bechtold M L, Buxbaum J L. et al. How good is endoscopic ultrasound-guided fine-needle aspiration in diagnosing the correct etiology for a solid pancreatic mass? A meta-analysis and systematic review. Pancreas. 2013;42:20–26. doi: 10.1097/MPA.0b013e3182546e79. [DOI] [PubMed] [Google Scholar]
- 43.Strand D S, Jeffus S K, Sauer B G. et al. EUS-guided 22-gauge fine-needle aspiration versus core biopsy needle in the evaluation of solid pancreatic neoplasms. Diagn Cytopathol. 2014;42:751–758. doi: 10.1002/dc.23116. [DOI] [PubMed] [Google Scholar]
- 44.Vanbiervliet G, Napoléon B, Paul M CS. et al. Core needle versus standard needle for endoscopic ultrasound-guided biopsy of solid pancreatic masses: a randomized crossover study. Endoscopy. 2014;46:1063–1070. doi: 10.1055/s-0034-1377559. [DOI] [PubMed] [Google Scholar]
- 45.Lee Y N, Moon J H, Kim H K. et al. Core biopsy needle versus standard aspiration needle for endoscopic ultrasound-guided sampling of solid pancreatic masses: a randomized parallel-group study. Endoscopy. 2014;46:1056–1062. doi: 10.1055/s-0034-1377558. [DOI] [PubMed] [Google Scholar]
- 46.Fujii L L, Levy M J. Pitfalls in EUS FNA. Gastrointest Endosc Clin N Am. 2014;24:125–142. doi: 10.1016/j.giec.2013.08.003. [DOI] [PubMed] [Google Scholar]
- 47.LeBlanc J K, Ciaccia D, Al-Assi M T. et al. Optimal number of EUS-guided fine needle passes needed to obtain a correct diagnosis. Gastrointest Endosc. 2004;59:475–481. doi: 10.1016/s0016-5107(03)02863-3. [DOI] [PubMed] [Google Scholar]
- 48.Turner B G, Cizginer S, Agarwal D. et al. Diagnosis of pancreatic neoplasia with EUS and FNA: a report of accuracy. Gastrointest Endosc. 2010;71:91–98. doi: 10.1016/j.gie.2009.06.017. [DOI] [PubMed] [Google Scholar]
- 49.Wani S, Wallace M B, Cohen J. et al. Quality indicators for EUS. Am J Gastroenterol. 2015;110:102–113. doi: 10.1038/ajg.2014.387. [DOI] [PubMed] [Google Scholar]
- 50.Affolter K E, Schmidt R L, Matynia A P. et al. Needle size has only a limited effect on outcomes in EUS-guided fine needle aspiration: a systematic review and meta-analysis. Dig Dis Sci. 2013;58:1026–1034. doi: 10.1007/s10620-012-2439-2. [DOI] [PubMed] [Google Scholar]