

Abstract
Background
Endothelin-1 (ET-1) is important in the pathogenesis of systemic sclerosis (SSc). ET-1 binds two receptors, endothelin type A (ETA) and endothelin type B (ETB). Dual ETA/ETB receptor antagonists and a selective ETA receptor antagonist are used clinically to treat SSc, and the effect of these antagonists on fibroblast activation has been described. However, the role of ETB receptor signaling in fibrogenesis is less clear. This study was conducted to evaluate the profibrotic function of ETB receptor signaling in a murine model of bleomycin (BLM)-induced scleroderma.
Methods
We used ETB receptor–knockout (ETBKO) mice, which are genetically rescued from lethal intestinal aganglionosis by an ETB receptor transgene driven by the human dopamine β-hydroxylase (DβH)-gene promoter, and wild-type mice with DβH-ETB (WT). BLM or phosphate-buffered saline (PBS) was administered subcutaneously by osmotic minipump, and skin fibrosis was assessed by dermal thickness, subcutaneous fat atrophy, and myofibroblast count in the dermis. Dermal fibroblasts isolated from ETBKO and WT mice were cultured in vitro, stimulated with BLM or ET-1, and the expression of profibrotic genes was compared by quantitative PCR.
Results
Dermal thickness, subcutaneous fat atrophy, and myofibroblast counts in the dermis were significantly reduced in ETBKO mice compared to WT mice, after BLM treatment. Compared with wild-type, dermal fibroblasts isolated from ETBKO mice showed lower gene expressions of α-smooth muscle actin and collagen 1α1 in response to BLM or ET-1 stimulation in vitro.
Conclusions
ET-1–ETB receptor signaling is involved in skin sclerosis and in collagen synthesis by dermal fibroblasts.
Electronic supplementary material
The online version of this article (doi:10.1186/s13075-016-1011-4) contains supplementary material, which is available to authorized users.
Keywords: Systemic sclerosis, Endothelin type B receptor, Dermal fibroblast
Background
Systemic sclerosis (SSc), a connective-tissue disease of unknown etiology, is characterized by autoimmunity, microvascular impairment, chronic inflammation, and fibrotic changes in the skin and internal organs [1]. The pathogenesis of SSc has been studied in a bleomycin (BLM)-induced scleroderma model [2, 3]. Among fibrotic agents known to contribute to scleroderma, the role of endothelin-1 (ET-1) in SSc fibrosis has been well described [4]. The plasma concentration of ET-1 is elevated in SSc patients, and endothelin receptor expression is increased in the lungs and skin [5, 6]. ET-1 plays an important role in murine model of BLM-induced scleroderma because endothelin receptor antagonist therapy is reported to attenuate skin fibrosis of mice [4]. Recently, vascular endothelial cell-specific ET-1 knockout mice are also reported to attenuate skin sclerosis [7]. ET-1, which was first characterized as a potent vasoconstrictive peptide derived from endothelial cells, is an important profibrotic mediator that induces the differentiation of fibroblasts to myofibroblasts and increases the extracellular matrix. Therefore, ET-1 plays a critical role in vascular impairment and fibrosis in SSc patients.
ET-1 binds two receptor subtypes, the endothelin type A (ETA) and endothelin type B (ETB) receptors [8]. Treatment with a dual ETA/ETB receptor antagonist or a selective ETA receptor antagonist improves mortality in patients with pulmonary arterial hypertension [9–11]. ETA receptor signaling is critical for dermal fibroblast activation [12]. However, the role of ETB receptor signaling in fibrogenesis is less clear.
To investigate the profibrotic activity of the ET-1–ETB receptor signal in fibrosis, we used endogenous ETB receptor–knockout (ETBKO) mice with an ETB receptor transgene driven by the human dopamine β-hydroxylase (DβH) gene promoter, which generated “rescued” ETB-knockout mice [13–15]. ETB-receptor mutant mice and general (not rescued) ETBKO mice, which have aganglionic megacolon and white spotting on the coat, die before reaching adulthood because ETB receptor signaling is important in generating melanocytes and enteric neurons [16]. In the “rescued” ETBKO mice, a functional ETB receptor is expressed only in the enteric nervous system; other tissues lack ETB receptors. These mice survive into adulthood [17].
Here we show that ETBKO mice were resistant to BLM-induced scleroderma, and that compared to WT mice, ETBKO mice showed less fibroblast activation and myofibroblast formation in response to BLM or ET-1.
Methods
Animals
The mice were housed in the animal facility of Kobe Pharmaceutical University, with a 12-h dark/light cycle and ad libitum water and food. Heterozygous ETBKO mice (ETB+/-) on a C57BL/6 J genetic background were generated as described previously [17, 18]. The human DβH gene promoter–regulated ETB receptor transgene (DβH-ETB) and ETB+/- with DβH-ETB were generated as described previously [13–15]. ETB+/- mice were crossed with DβH-ETB mice to obtain three genotypes: wild-type ETB+/+ with DβH-ETB (WT mice), ETB+/- with DβH-ETB (heterozygous KO mice), and ETB-/- with DβH-ETB (ETBKO mice). The ETBKO mice had a partly white coat that distinguished them from heterozygous KO and WT mice. All experimental protocols were approved by the Ethics Review Committee for Animal Experimentation of Kobe Pharmaceutical University.
Reagents and antibodies
BLM and ET-1 (H-6995) were purchased from Nippon-Kayaku (Tokyo, Japan) and Bachem (Bubendorf, Switzerland), respectively. Dulbecco's modified Eagle's medium (DMEM) (Nissui-Seiyaku, Tokyo, Japan), RPMI 1640 (Wako Pure Chemical Industries, Osaka, Japan), fetal bovine serum (FBS) (MP Biomedicals, Santa Ana, CA, USA), 1 % penicillin–streptomycin (Lonza, Basel, Switzerland), L-glutamine (Thermo Fisher Scientific, Waltham, MA, USA), and type 1 collagenase (Worthington Biochemical Corporation, Lakewood, NJ, USA) were also used. Bovine serum albumin (BSA), 2 M acetic acid, and dispase were purchased from Sigma-Aldrich (St. Louis, MO, USA). For immunohistochemistry experiments, anti-alpha smooth-muscle actin (αSMA) antibody (ab32575), anti-collagen 1 antibody (ab21286), anti-CD3 antibody (ab16669), anti-F4/80 antibody (ab111101) and rabbit polyclonal IgG (ab27472) were purchased from Abcam (Cambridge, UK), and anti-myeloperoxidase antibody (PA5-16672) purchased from Thermo Fisher Scientific (Waltham, MA, USA). A rabbit ABC Staining System (sc-2018) was purchased from Santa Cruz Biotechnology (Dallas, TX, USA).
BLM administration
BLM was dissolved in phosphate-buffered saline (PBS). BLM or PBS was administered with osmotic minipumps according to previous reports with minor modifications [19–21]. Briefly, osmotic minipumps (Alzet2001; Durect, Cupertino, CA, USA) containing 200 μl of BLM (125 mg/kg) or PBS were implanted subcutaneously onto the back of WT or ETBKO mice aged 6–10 weeks; this was counted as day 0. The pumps delivered 1.0 μg/h for 7 days. The mice were sacrificed on day 28, and skin and lung tissues were taken. Skin samples were taken a short distance from the osmotic minipump to obtain samples that were not affected by pump implantation.
Histology and immunohistochemistry
The skin and lung samples were fixed in 4 % paraformaldehyde, embedded in paraffin, sectioned, and stained with Masson’s trichrome. To evaluate the BLM-induced scleroderma, we assessed dermal thickening and subcutaneous fat atrophy by measuring the distances between the epidermis and dermis and between the dermis and subcutaneous fat at 40× magnification. The degree of lung fibrosis was quantified using the Ashcroft score at 40× magnification [22]. Collagen 1 deposition area in the dermis was measured with ImageJ software (National Institutes of Health). Fibroblast activation was assessed by αSMA immunohistochemical staining of the skin sections, and αSMA-positive myofibroblasts in the dermis were counted at 100× magnification. To examine whether ETB receptor is involved in the inflammation of this model, we counted myeloperoxidase-positive neutrophils, CD3-positive T lymphocytes and F4/80-positive macrophages in the dermis at 100× magnification.
Collection of bronchoalveolar lavage fluid (BALF)
To evaluate lung inflammation, a cell count of BALF was performed. Immediately after the mice were sacrificed, a 20-gauge intravenous catheter was inserted into the trachea. A total of 0.5 ml of PBS was instilled three times and withdrawn from the lung via an intratracheal cannula. After BALF was centrifuged, the pellet was resuspended in 1 ml of PBS. Total BALF cells were counted with a hemocytometer. The BALF solutions were stained with May-Giemsa staining after cytospin centrifuge, and the white blood cell differentiation was evaluated by morphological criteria using a light microscope.
Murine dermal fibroblast isolation and culture
Dermal fibroblasts were isolated from WT and ETBKO mice at 3–4 weeks of age according to previous reports, with minor modification [23]. Skin samples were placed dermis-down in culture dishes containing RPMI + 3.6 % dispase, and incubated overnight at 4 °C. The dermis was separated from the epidermis, placed in RPMI + 0.05 % type I collagenase, and incubated at 37 °C for 30 min. The cell suspension was filtered through sterile gauze into a 50-mL conical tube. After adding an equal volume of DMEM + 10 % FBS containing penicillin, streptomycin, and L-glutamine, the suspension was centrifuged at 200 × g for 10 min. Fibroblasts were resuspended in DMEM + 10 % FBS, plated in 100-mm culture dishes, and incubated at 37 °C in 5 % CO2 and 95 % room air. For in vitro experiments, fibroblasts were seeded into 6-well plates (1 × 105 per well) and incubated in DMEM + 10 % FBS at 37 °C in 5 % CO2. When the fibroblasts had grown to approximately 80 % confluence, the medium was changed and the fibroblasts were treated with 20 μg/ml BLM or 500 nM ET-1 for 24 h. The BLM was dissolved in DMEM without FBS; the ET-1 was dissolved in 0.1 % acetic acid + 0.01 % BSA.
Quantitative real-time polymerase chain reaction (PCR)
Total RNA was isolated from fibroblasts using an RNeasy Mini kit (Qiagen, Hilden, Germany), followed by cDNA synthesis using a QuantiTect Reverse Transcription kit (Qiagen). PCR reaction mixtures were prepared using the QuantiTect SYBR Green PCR kit (Qiagen), followed by quantitative PCR on a PikoReal system (Thermo Fisher Scientific). The following primer pairs were used: collagen 1α1 (Col1α1), 5’-TGACTGGAAGAGCGGAGAGTACT-3’ (forward) and 5’-GGTCTGACCTGTCTCCATGTTG-3’ (reverse); αSMA, 5’-AGAGACTCTCTTCCAGCCATC-3’ (forward) and 5’-GACGTTGTTAGCATAGAGATC-3’ (reverse); ET-1, 5’-GTGTCTACTTCTGCCACCTGGACAT-3’ (forward) and 5’-GGGCTCGCACTATATAAGGGATGAC-3’ (reverse); endothelin receptor type A (EDNRA), 5’-CCTTATCTSCGTGGTCATTG-3’ (forward) and 5’-ACTGAGAGCACAGAGGTTC-3’ (reverse); endothelin receptor type B (EDNRB), 5’-GGAATCACAGTGCTGAGTC-3’ (forward) and 5’-CTTTGTAGTCCGACGTAATC-3’ (reverse); glyceraldahyde-3-phosphate dehydrogenase (GAPDH), 5’-AACTTTGGCATTGTGGAAGG-3’ (forward) and 5’-ACACATTGGGGGTAGGAACA-3’ (reverse). GAPDH was used as an internal control to normalize the amount of loaded , complementary DNA (cDNA).
Measurement of soluble collagen content
Sircol collagen assay (Biocolor Ltd., Belfast, Northern Ireland) was used to quantify soluble collagen contents in fibroblast culture supernatant according to the manufacturer’s instructions with minor modification. Briefly, 200 μl of supernatant was mixed with 1 ml of Sircol dye reagent for 30 minutes. After centrifugation, the pellets were dissolved in 1 ml Sircol alkali reagent and vortexed. Relative absorbance was measured at 540 nm.
Statistical analysis
Data are presented as mean ± standard error of the mean (SEM). Differences between groups were analyzed by Student’s t test using GraphPad Prism 5 software (GraphPad Software Inc., La Jolla, CA, USA) and p < 0.05 was considered statistically significant.
Results
ETBKO mice resisted BLM-induced scleroderma
WT and ETBKO mice were treated with BLM or PBS by osmotic minipump. No mice died due to the osmotic minipump implantation or BLM administration. To examine the biological significance of ETB receptor signaling after BLM administration, we measured body-weight changes from day 0 to day 28. ETBKO mice were smaller than WT mice of the same age, and ETBKO mice gained less body weight than did WT mice when treated with PBS. However, while BLM-treated WT mice did not gain body weight, BLM-treated ETBKO mice gained weight similarly to the PBS-treated ETBKO mice (Fig 1b).
Fig. 1.
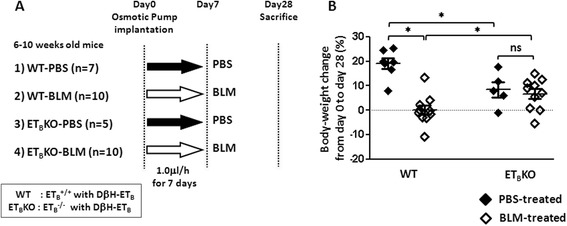
Study design and body-weight changes of each mice group after BLM treatment. a Summary of this experimental model and sample number of each group. Osmotic pumps containing 200 μl of BLM (125 mg/kg) or PBS were implanted subcutaneously onto the back of WT or ETBKO mice on day 0. Pumps deliver their contents 1.0 μg/h for 7 days. Mice were sacrificed on day28. b Body-weight changes from day 0 to day 28 in WT and ETBKO mice. The body-weight change was calculated as [(body weight on day 28) − (body weight on day 0)] × (body weight on day 0)-1 × 100 (%). Each dot indicates the body-weight change in an individual mouse (* p < 0.05). BLM bleomycin, DβH-ET B endothelin type B receptor transgene driven by the human dopamine β-hydroxylase gene promoter, ET B KO endothelin type B receptor knockout, PBS phosphate-buffered saline, WT wild-type
To determine the ETB receptor’s role in BLM-induced scleroderma, skin specimens were obtained from each group on day 28 after implanting the osmotic minipump. The skin samples were stained with Masson’s trichrome to evaluate the dermal thickness and subcutaneous fat atrophy. In WT mice, BLM treatment increased the distance between the epidermis and dermis, and reduced the distance between the dermis and subcutaneous fat. In contrast, these distances did not change significantly in the ETBKO mice treated with PBS or BLM (Fig. 2a-c). Likewise, collagen 1 deposition area in the dermis was increased by BLM-treatment in WT mice, but the increment was not seen in ETBKO mice (Fig. 2d). These results suggested that ETB receptor signaling is associated with BLM-induced skin sclerosis. Also lung fibrosis and inflammation were evaluated, but neither cell counts in BALF nor lung histological scores were not significantly different between WT and ETBKO with BLM treatment (Additional file 1: Figure S1).
Fig. 2.
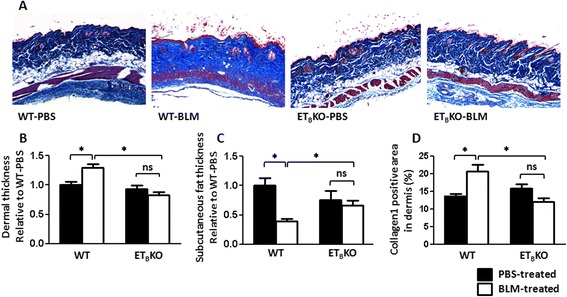
ETBKO mice resist BLM-induced skin sclerosis. a Representative images of dermis sections stained with Masson's trichrome at 40× magnification. b Changes in dermal thickness (epidermal–dermal distance) and c subcutaneous fat atrophy (dermal–subcutaneous fat distance) in BLM- or PBS-treated WT and ETBKO mice; values are shown as the mean fold change from PBS-treated WT (WT-PBS) mice. d Collagen 1 deposition area in dermis of each mice group. (* p < 0.05) (n = 5–10 mice per group). BLM bleomycin, ET B KO endothelin type B receptor knockout, PBS phosphate-buffered saline, WT wild-type
Inhibited fibroblast activation protects ETBKO mice against BLM-induced scleroderma
BLM-induced scleroderma is associated with the differentiation of fibroblasts into myofibroblasts. These myofibroblasts, which are identified by αSMA expression, promote fibrosis by producing collagen and other extracellular matrix components [24, 25].
To determine whether ETB receptor signaling contributes to BLM-induced fibroblast differentiation, we counted the number of αSMA-positive cells in the dermis of BLM- or PBS-treated WT and ETBKO mice. BLM increased the number of αSMA-positive myofibroblasts in the WT but not ETBKO dermis, indicating that ETB is involved in myofibroblast formation (Fig. 3).
Fig. 3.
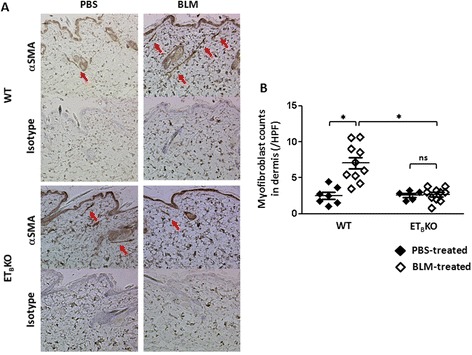
Fewer αSMA-expressing myofibroblasts are observed in the dermis of ETBKO than WT mice after BLM treatment. a Representative images showing the immunohistochemical staining of skin samples for αSMA (upper) and isotype (lower) at 100× magnification. Red arrows indicate myofibroblasts (αSMA-expressing spindle-shaped cells). b Average myofibroblast counts per field of view in the dermis, counted at 100× magnification (* p < 0.05); n = 5–10 mice per group. BLM bleomycin, HPF high-power field, ET B KO endothelin type B receptor knockout, PBS phosphate-buffered saline, WT wild-type
Inflammatory cell filtration in the dermis was counted to determine whether the degree of inflammation was different between WT and ETBKO skin fibrosis. The numbers of myeloperoxidase-positive neutrophils, CD3-positive T cells and F4/80-positive macrophages in the dermis were significantly increased when treated with BLM. However, the numbers of these inflammatory cells were not different between WT and ETBKO mice both before and after BLM treatment (Fig. 4).
Fig. 4.
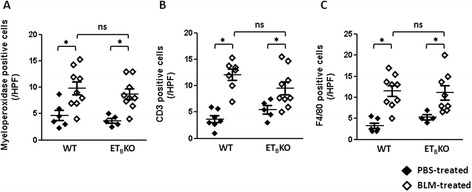
Infiltration of inflammatory cells in the dermis of WT and ETBKO mice after BLM treatment. The average cell counts of a myeloperoxidase, b CD3, and c F4/80-positive cells in the dermis. The cells were counted per field of view at 100× magnification; n = 5–10 mice per group. (* p < 0.05). BLM bleomycin, ET B KO endothelin type B receptor knockout, HPF high-power field, PBS phosphate-buffered saline, WT wild-type
Collectively ETB receptor signaling seemed to contribute to fibroblast activation independent of inflammation.
The ETB receptor is associated with dermal fibroblast activation and collagen synthesis in response to BLM or ET-1
Because fibroblasts play a critical role in fibrosis, we next examined the characteristics of dermal fibroblasts from WT and ETBKO mice. ET-1 or BLM stimulation is reported to induce fibroblasts to express profibrotic genes [12, 26]. Thus, we isolated dermal fibroblasts from WT and ETBKO mice and assessed their activation and collagen synthesis in response to ET-1 or BLM in vitro. Dermal fibroblasts from ETBKO mice expressed little or no EDNRB mRNA but expressed EDNRA normally, as expected (Fig. 5a, b).
Fig. 5.
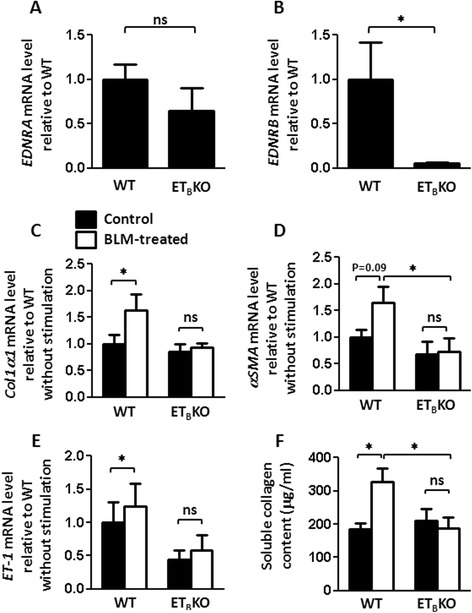
Knockout of the ETB receptor signal reduces the activation of skin-derived fibroblasts in response to BLM. a EDNRA and b EDNRB mRNA levels in skin-derived fibroblasts from WT and ETBKO mice (n = 5 each). c-e BLM-induced fibroblast activation in WT and ETBKO mice (n = 6–9 each), determined by the gene expression levels of Col1α1, αSMA, and ET-1. Values show the mean mRNA levels relative to WT without stimulation (* p < 0.05). f Soluble collagen production from WT and ETBKO (n = 4 each) fibroblasts with or without BLM treatment (* p < 0.05). WT wild-type, αSMA α-smooth muscle actin, BLM bleomycin, Col1α1 collagen 1α1, ET-1 endothelin-1, ET B KO endothelin type B receptor knockout, PBS phosphate-buffered saline
BLM stimulation induced Col1α1 and ET-1 gene expression in fibroblasts from WT mice, but not in those from ETBKO mice. When stimulated with BLM, WT fibroblasts expressed the αSMA gene at significantly higher levels than did ETBKO fibroblasts (Fig. 5c-e).
ET-1 stimulation induced Col1α1 expression in WT fibroblasts. ET-1 also tended to induce αSMA mRNA in WT fibroblasts, although this increase did not reach statistical significance. ET-1 stimulation did not influence the Col1α1 or αSMA expression in ETBKO fibroblasts (Fig. 6a, b).
Fig. 6.
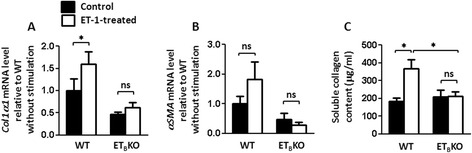
Knockout of the ETB receptor signal reduces the activation of skin-derived fibroblasts in response to ET-1. a, b ET-1-induced fibroblast activation in WT and ETBKO mice (n = 4 or 5 each), determined by the gene expression levels of Col1α1, αSMA. Values show the mean mRNA levels relative to WT without stimulation (* p < 0.05). c Soluble collagen production from WT and ETBKO (n = 4 each) fibroblasts with or without ET-1-treatment (* p < 0.05). αSMA α-smooth muscle actin, BLM bleomycin, Col1α1 collagen 1α1, ET-1 endothelin-1, ET B KO endothelin type B receptor knockout, PBS phosphate-buffered saline, WT wild-type
Next, we measured soluble collagen content in the supernatant with Sircol collagen assay to assess whether BLM or ET-1 stimulation increases collagen production by fibroblasts. BLM or ET-1 treatment of WT fibroblasts significantly induced collagens. Increase in collagen production by BLM or ET-1 stimulation was not seen in ETBKO fibroblasts (Figs. 5f and 6c). Collectively, ETBKO fibroblasts showed less profibrotic properties in response to BLM or ET-1 than WT.
Discussion
In this study, we demonstrated for the first time with genetic ETBKO mice that ETB receptor signaling in the presence of the ETA receptor promotes fibrosis in BLM-induced scleroderma. Myofibroblast formation was inhibited in ETBKO mice, allowing them to resist BLM-induced skin fibrosis. At least one mechanism of the ETB receptor appears to function through dermal fibroblasts, because the ETBKO fibroblasts did not respond to BLM or ET-1 stimulation, whereas WT fibroblasts showed increased Col1α1 and αSMA expression in vitro.
Rescued ETBKO rats and mice, like those used in this study, are useful for investigating ETB receptor signaling. ETBKO rats show deteriorating health due to hypoxia-induced pulmonary hypertension, and ETBKO mice show worsened vascular remodeling in a carotid artery ligation model [27, 28]. Our study is the first to demonstrate that the ETB receptor is critical for BLM-induced scleroderma using ETBKO mice.
ET-1 is important in fibrosis because it induces collagen production and myofibroblasts. We found that in WT fibroblasts, BLM induced ET-1, which in turn induced collagen production. On the other hand, ETBKO fibroblasts did not produce collagen when stimulated by ET-1, indicating that ETB is indispensable for the ET-1-induced collagen production. Thus, the ET-1–ETB system is critical for the collagen production by fibroblasts.
We showed that myofibroblast formation was strongly inhibited in the ETBKO mice in vivo. In addition, ETBKO fibroblasts did not express αSMA mRNA in response to BLM or ET-1. These results indicate that ETB is involved in myofibroblast formation. In our experiments, ET-1’s induction of αSMA in WT fibroblasts in vivo was stronger than that in vitro. This was not surprising, because there are multiple sources of myofibroblasts in vivo, including tissue-resident fibroblasts [29], epithelial or endothelial cells transitioning into mesenchymal cells (EMT or EndoMT) [30–33], or bone marrow-derived circulating fibrocytes [34, 35]. Thus, we believe that ETB is involved in myofibroblast formation from various types of cells.
Myofibroblast precursors differ in various tissues. For example, resident fibroblasts are the main contributors to myofibroblasts in lung fibrosis [36], and hepatic stellate cells are the most important source of myofibroblasts in liver fibrosis [37]. Although a recent study found that adipocytes differentiate into myofibroblasts in dermal fibrosis [38], the primary source of myofibroblasts in dermal fibrosis remains unclear. ETB receptor signaling seems to be important in liver and cardiac fibrosis [39–41], but not renal fibrosis [42]. The difference of the skin and lung fibrosis might come from the difference in both myofibroblast precursor and contribution of ETB receptor signaling in the organ. Further investigation is needed to reveal which cells are responsible for generating dermal myofibroblasts, and how the ETA and ETB receptors are involved in dermal or other organ fibrogenesis.
In dermal fibroblasts, both ETA and ETB receptor signaling are reported to be necessary for ET-1 to exert its profibrotic effect [12]; in that study, neither ETA nor ETB receptor selective antagonists inhibited the collagen synthesis in dermal fibroblasts stimulated with ET-1. Our data appear to conflict with that study; this discrepancy might be due to differences between a pharmacological blockade and genetic knockout. The genetic knockout is assumed to affect permanently and completely, while the effect of pharmacological blockade is usually temporary and depends on affinity. We did not perform in vivo and in vitro study with the ETB selective antagonist, because it was reported that existing inhibitors could not suppress the fibroblast activation in vitro as mentioned above. We hope that new ETB selective antagonists that suppress fibroblast function will be developed.
Clinically, dual ETA/ETB receptor antagonists (bosentan, macitentan) and a selective ETA receptor antagonist (ambrisentan) improve the hemodynamics, exercise capacity, and survival rate in patients with pulmonary arterial hypertension [9–11]. These ET receptor blockers are also effective for preventing and improving digital ulcers in SSc patients [43, 44]. Currently, there is no selective ETB receptor antagonist that can be safely administered to humans. However, our study suggests that ETB receptor blockade is a potential pharmaceutical treatment for progressive skin fibrosis in SSc patients.
Conclusions
This study described that ETBKO mice were resistant to BLM-induced skin sclerosis and that ETBKO mice showed less fibroblast activation and myofibroblast formation in response to BLM or ET-1. Thus, ET-1–ETB receptor signaling is involved in skin sclerosis and in collagen synthesis by dermal fibroblasts.
Acknowledgements
The authors thank Shino Tanaka for providing technical assistance.
Abbreviations
- αSMA
alpha-smooth muscle actin
- BALF
bronchoalveolar fluid lavage
- BLM
bleomycin
- BSA
bovine serum albumin
- cDNA
complementary DNA
- Col1α1
collagen 1α1
- DMEM
Dulbecco's modified Eagle's medium
- DβH
human dopamine β-hydroxylase
- EDNRA
endothelin receptor type A
- EDNRB
endothelin receptor type B
- ET-1
endothelin-1
- ETA
endothelin type A
- ETB
endothelin type B
- ETBKO
endothelin type B receptor-knockout
- FBS
fetal bovine serum
- GAPDH
glyceraldahyde-3-phosphate dehydrogenase
- PBS
phosphate-buffered saline
- PCR
polymerase chain reaction
- SEM
standard error of the mean
- SSc
systemic sclerosis
- WT
wild-type
Additional file
Figure S1. BLM-induced lung inflammation and fibrosis of WT and ETBKO mice. (A) Total cell, (B) macrophages, (C) neutrophils, and (D) lymphocytes counts in BALF collected from WT and ETBKO with PBS or BLM treatment (n = 5–10 mice per group) on day28 after osmotic implantation (* p < 0.05). (E) Representative images of lung sections stained with Masson's trichrome at 40 × magnification. (F) Ashcroft score of WT and ETBKO mice with PBS or BLM treatment (n = 5–10 mice per group) (* p < 0.05). BLM bleomycin, ET B KO endothelin type B receptor knockout, PBS phosphate-buffered saline, WT wild- type. (TIF 1160 kb)
Footnotes
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
KA carried out most of the experiments and drafted the manuscript. JS participated in the conception and design of the experiments, performed analysis and interpretation of data, and helped to draft the manuscript. SS and KN carried out the acquisition of the data, performed analysis and interpretation of the data, and helped to draft the manuscript. TO and KY carried out the acquisition of the data, performed analysis and interpretation of the data, and critically revised the manuscript. MY developed ETBKO mice used in this study and provided them, participated in the conception of the experiments, and critically revised the manuscript. NE participated in the conception and design of the experiments, performed interpretation of the data, and critically revised the manuscript. AM conceived of the study, participated in its design and coordination, performed analysis and interpretation of the data, and helped to draft the manuscript. All authors read and approved the final manuscript.
References
- 1.Ho YY, Lagares D, Tager AM, Kapoor M. Fibrosis—a lethal component of systemic sclerosis. Nat Rev Rheumatol. 2014;10:390–402. doi: 10.1038/nrrheum.2014.53. [DOI] [PubMed] [Google Scholar]
- 2.Yamamoto T, Takagawa S, Katayama I, Yamazaki K, Hamazaki Y, Shinkai H, et al. Animal model of sclerotic skin. I: Local injections of bleomycin induce sclerotic skin mimicking scleroderma. J Invest Dermatol. 1999;112:456–462. doi: 10.1046/j.1523-1747.1999.00528.x. [DOI] [PubMed] [Google Scholar]
- 3.Batteux F, Kavian N, Servettaz A. New insights on chemically induced animal models of systemic sclerosis. Curr Opin Rheumatol. 2011;23:511–518. doi: 10.1097/BOR.0b013e32834b1606. [DOI] [PubMed] [Google Scholar]
- 4.Lagares D, García-Fernández RA, Jiménez CL, Magán-Marchal N, Busnadiego O, Lamas S, et al. Endothelin 1 contributes to the effect of transforming growth factor beta1 on wound repair and skin fibrosis. Arthritis Rheum. 2010;62:878–889. doi: 10.1002/art.27307. [DOI] [PubMed] [Google Scholar]
- 5.Morelli S, Ferri C, Polettini E, Bellini C, Gualdi GF, Pittoni V, et al. Plasma endothelin-1 levels, pulmonary hypertension, and lung fibrosis in patients with systemic sclerosis. Am J Med. 1995;99:255–260. doi: 10.1016/S0002-9343(99)80157-0. [DOI] [PubMed] [Google Scholar]
- 6.Abraham DJ, Vancheeswaran R, Dashwood MR, Rajkumar VS, Pantelides P, Xu SW, et al. Increased levels of endothelin-1 and differential endothelin type A and B receptor expression in scleroderma-associated fibrotic lung disease. Am J Pathol. 1997;151:831–841. [PMC free article] [PubMed] [Google Scholar]
- 7.Makino K, Jinnin M, Aoi J, Kajihara I, Makino T, Fukushima S, et al. Knockout of endothelial cell-derived endothelin-1 attenuates skin fibrosis but accelerates cutaneous wound healing. PLoS One. 2014;9:e97972. doi: 10.1371/journal.pone.0097972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Miyauchi T, Masaki T. Pathophysiology of endothelin in the cardiovascular system. Annu Rev Physiol. 1999;61:391–415. doi: 10.1146/annurev.physiol.61.1.391. [DOI] [PubMed] [Google Scholar]
- 9.Rubin LJ, Badesch DB, Barst RJ, Galie N, Black CM, Keogh A, et al. Bosentan therapy for pulmonary arterial hypertension. N Engl J Med. 2002;346:896–903. doi: 10.1056/NEJMoa012212. [DOI] [PubMed] [Google Scholar]
- 10.Galiè N, Olschewski H, Oudiz RJ, Torres F, Frost A, Ghofrani HA, et al. Ambrisentan for the treatment of pulmonary arterial hypertension: results of the ambrisentan in pulmonary arterial hypertension, randomized, double-blind, placebo-controlled, multicenter, efficacy (ARIES) study 1 and 2. Circulation. 2008;117:3010–3019. doi: 10.1161/CIRCULATIONAHA.107.742510. [DOI] [PubMed] [Google Scholar]
- 11.Pulido T, Adzerikho I, Channick RN, Delcroix M, Galiè N, Ghofrani HA, et al. Macitentan and morbidity and mortality in pulmonary arterial hypertension. N Engl J Med. 2013;369:809–818. doi: 10.1056/NEJMoa1213917. [DOI] [PubMed] [Google Scholar]
- 12.Shi-Wen X, Denton CP, Dashwood MR, Holmes AM, Bou-Gharios G, Pearson JD, et al. Fibroblast matrix gene expression and connective tissue remodeling: role of endothelin-1. J Invest Dermatol. 2001;116:417–425. doi: 10.1046/j.1523-1747.2001.01256.x. [DOI] [PubMed] [Google Scholar]
- 13.Gariepy CE, Williams SC, Richardson JA, Hammer RE, Yanagisawa M. Transgenic expression of the endothelin-B receptor prevents congenital intestinal aganglionosis in a rat model of Hirschsprung disease. J Clin Invest. 1998;102:1092–1101. doi: 10.1172/JCI3702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Rice J, Doggett B, Sweetser DA, Yanagisawa H, Yanagisawa M, Kapur RP. Transgenic rescue of aganglionosis and piebaldism in lethal spotted mice. Dev Dyn. 2000;217:120–132. doi: 10.1002/(SICI)1097-0177(200001)217:1<120::AID-DVDY11>3.0.CO;2-U. [DOI] [PubMed] [Google Scholar]
- 15.Gariepy CE, Ohuchi T, Williams SC, Richardson JA, Yanagisawa M. Salt-sensitive hypertension in endothelin-B receptor-deficient rats. J Clin Invest. 2000;105:925–933. doi: 10.1172/JCI8609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Baynash AG, Hosoda K, Giaid A, Richardson JA, Emoto N, Hammer RE, et al. Interaction of endothelin-3 with endothelin-B receptor is essential for development of epidermal melanocytes and enteric neurons. Cell. 1994;79:1277–1285. doi: 10.1016/0092-8674(94)90018-3. [DOI] [PubMed] [Google Scholar]
- 17.Hosoda K, Hammer RE, Richardson JA, Baynash AG, Cheung JC, Giaid A, et al. Targeted and natural (piebald-lethal) mutations of endothelin-B receptor gene produce megacolon associated with spotted coat color in mice. Cell. 1994;79:1267–1276. doi: 10.1016/0092-8674(94)90017-5. [DOI] [PubMed] [Google Scholar]
- 18.Puffenberger EG. Hosoda K, Washington SS, Nakao K, deWit D, Yanagisawa M, et al. A missense mutation of the endothelin-B receptor gene in multigenic Hirschsprung’s disease. Cell. 1994;79:1257–1266. doi: 10.1016/0092-8674(94)90016-7. [DOI] [PubMed] [Google Scholar]
- 19.Lee R, Reese C, Bonner M, Tourkina E, Hajdu Z, Riemer EC, et al. Bleomycin delivery by osmotic minipump: similarity to human scleroderma interstitial lung disease. Am J Physiol Lung Cell Mol Physiol. 2014;306:L736–L748. doi: 10.1152/ajplung.00210.2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Harrison JH, Jr, Lazo JS. High dose continuous infusion of bleomycin in mice: a new model for drug-induced pulmonary fibrosis. J Pharmacol Exp Ther. 1987;243:1185–1194. [PubMed] [Google Scholar]
- 21.Aono Y, Kishi M, Yokota Y, Azuma M, Kinoshita K, Takezaki A, et al. Role of platelet-derived growth factor/platelet-derived growth factor receptor axis in the trafficking of circulating fibrocytes in pulmonary fibrosis. Am J Respir Cell Mol Biol. 2014;51:793–801. doi: 10.1165/rcmb.2013-0455OC. [DOI] [PubMed] [Google Scholar]
- 22.Ashcroft T, Simpson JM, Timbrell V. Simple method of estimating severity of pulmonary fibrosis on a numerical scale. J Clin Pathol. 1998;41:467–470. doi: 10.1136/jcp.41.4.467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gallucci RM, Sloan DK, Heck JM, Murray AR, O'Dell SJ. Interleukin 6 indirectly induces keratinocyte migration. J Invest Dermatol. 2004;122:764–772. doi: 10.1111/j.0022-202X.2004.22323.x. [DOI] [PubMed] [Google Scholar]
- 24.Abraham DJ, Eckes B, Rajkumar V, Krieg T. New developments in fibroblast and myofibroblast biology: implications for fibrosis and scleroderma. Curr Rheumatol Rep. 2007;9:136–143. doi: 10.1007/s11926-007-0008-z. [DOI] [PubMed] [Google Scholar]
- 25.Desmouliere A, Chaponnier C, Gabbiani G. Tissue repair, contraction, and the myofibroblast. Wound Repair Regen. 2005;13:7–12. doi: 10.1111/j.1067-1927.2005.130102.x. [DOI] [PubMed] [Google Scholar]
- 26.Yamamoto T, Eckes B, Krieg T. Bleomycin increases steady-state levels of type I collagen, fibronectin and decorin mRNAs in human skin fibroblasts. Arch Dermatol Res. 2000;292:556–561. doi: 10.1007/s004030000180. [DOI] [PubMed] [Google Scholar]
- 27.Ivy D, McMurtry IF, Yanagisawa M, Gariepy CE, Le Cras TD, Gebb SA, et al. Endothelin B receptor deficiency potentiates ET-1 and hypoxic pulmonary vasoconstriction. Am J Physiol Lung Cell Mol Physiol. 2001;280:L1040–L1048. doi: 10.1152/ajplung.2001.280.5.L1040. [DOI] [PubMed] [Google Scholar]
- 28.Murakoshi N, Miyauchi T, Kakinuma Y, Ohuchi T, Goto K, Yanagisawa M, et al. Vascular endothelin-B receptor system in vivo plays a favorable inhibitory role in vascular remodeling after injury revealed by endothelin-B receptor-knockout mice. Circulation. 2002;106:1991–1998. doi: 10.1161/01.CIR.0000032004.56585.2A. [DOI] [PubMed] [Google Scholar]
- 29.Hinz B. Formation and function of the myofibroblast during tissue repair. J Invest Dermatol. 2007;127:526–537. doi: 10.1038/sj.jid.5700613. [DOI] [PubMed] [Google Scholar]
- 30.Thiery JP, Acloque H, Huang RY, Nieto MA. Epithelial-mesenchymal transitions in development and disease. Cell. 2009;139:871–890. doi: 10.1016/j.cell.2009.11.007. [DOI] [PubMed] [Google Scholar]
- 31.Thiery JP, Sleeman JP. Complex networks orchestrate epithelialmesenchymal transitions. Nat Rev Mol Cell Biol. 2006;7:131–142. doi: 10.1038/nrm1835. [DOI] [PubMed] [Google Scholar]
- 32.Kalluri R, Neilson EG. Epithelial-mesenchymal transition and its implications for fibrosis. J Clin Invest. 2003;112:1776–1784. doi: 10.1172/JCI200320530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Arciniegas E, Sutton AB, Allen TD, Schor AM. Transforming growth factor beta 1 promotes the differentiation of endothelial cells into smooth muscle-like cells in vitro. J Cell Sci. 1992;103:521–529. doi: 10.1242/jcs.103.2.521. [DOI] [PubMed] [Google Scholar]
- 34.Herzog EL, Bucala R. Fibrocytes in health and disease. Exp Hematol. 2010;38:548–556. doi: 10.1016/j.exphem.2010.03.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Bellini A, Mattoli S. The role of the fibrocytes, a bone marrow-derived mesenchymal progenitor, in reactive and reparative fibroses. Lab Invest. 2007;87:858–870. doi: 10.1038/labinvest.3700654. [DOI] [PubMed] [Google Scholar]
- 36.Tsukui T, Ueha S, Abe J, Hashimoto S, Shichino S, Shimaoka T, et al. Qualitative rather than quantitative changes are hallmarks of fibroblasts in bleomycin-induced pulmonary fibrosis. Am J Pathol. 2013;183:758–773. doi: 10.1016/j.ajpath.2013.06.005. [DOI] [PubMed] [Google Scholar]
- 37.Guyot C, Lepreux S, Combe C, Doudnikoff E, Bioulac-Sage P, Balabaud C, et al. Hepatic fibrosis and cirrhosis: the (myo)fibroblastic cell subpopulations involved. Int J Biochem Cell Biol. 2006;38:135–151. doi: 10.1016/j.biocel.2005.08.021. [DOI] [PubMed] [Google Scholar]
- 38.Roberta GM, Benjamin DK, Jun W, Tammara AW, Lauren VG, Michael LW, et al. Myofibroblasts in murine cutaneous fibrosis originate from adiponectin-positive intradermal progenitors. Arthritis Rheumatol. 2015;67:1062–1073. doi: 10.1002/art.38990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Rockey DC, Chung JJ. Endothelin antagonism in experimental hepatic fibrosis. Implications for endothelin in the pathogenesis of wound healing. J Clin Invest. 1996;98:1381–1388. doi: 10.1172/JCI118925. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Gandhi CR, Kuddus RH, Uemura T, Rao AS. Endothelin stimulates transforming growth factor-beta1 and collagen synthesis in stellate cells from control but not cirrhotic rat liver. Eur J Pharmacol. 2000;406:311–318. doi: 10.1016/S0014-2999(00)00683-X. [DOI] [PubMed] [Google Scholar]
- 41.Seccia TM, Belloni AS, Kreutz R, Paul M, Nussdorfer GG, Pessina AC, et al. Cardiac fibrosis occurs early and involves endothelin and AT-1 receptors in hypertension due to endogenous angiotensin II. J Am Coll Cardiol. 2003;19:666–673. doi: 10.1016/S0735-1097(02)02860-7. [DOI] [PubMed] [Google Scholar]
- 42.Kalk P, Rückert M, Godes M, von Websky K, Relle K, Neumayer HH, et al. Does endothelin B receptor deficiency ameliorate the induction of peritoneal fibrosis in experimental peritoneal dialysis? Nephrol Dial Transplant. 2010;25:1474–1478. doi: 10.1093/ndt/gfp652. [DOI] [PubMed] [Google Scholar]
- 43.Matucci-Cerinic M, Denton CP, Furst DE, Mayes MD, Hsu VM, Carpentier P, et al. Bosentan treatment of digital ulcers related to systemic sclerosis: results from the RAPIDS-2 randomised, double-blind, placebo-controlled trial. Ann Rheum Dis. 2011;70:32–38. doi: 10.1136/ard.2010.130658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Parisi S, Peroni CL, Laganà A, Scarati M, Ambrogio F, Bruzzone M, et al. Efficacy of ambrisentan in the treatment of digital ulcers in patients with systemic sclerosis: a preliminary study. Rheumatology (Oxford) 2013;52:1142–1144. doi: 10.1093/rheumatology/ket019. [DOI] [PubMed] [Google Scholar]