

Abstract
We report herein a clinical case of a patient with femur fracture due to metastasis from penile squamous cell carcinoma. A young man, who was treated for carcinoma penis, presented with pathological fracture of femur and lung metastasis from metastatic carcinoma penis after 18 months. Long bone metastasis from penile cancer is extremely rare, to the best of our knowledge; this is the first report of a patient with penile cancer spread to the femur from primary squamous cell carcinoma of the penis.
Keywords: Carcinoma penis, Squamous cell carcinoma, Lung secondary, Long bone metastasis, Fracture femur
Introduction
Carcinoma penis usually spreads by lymphatic route. Its hematogenous spread to bones is uncommon. This is the first reported case of penile cancer metastasizing to the femur, presented with pathological fracture with lung metastasis.
Case History
A 35-year-old man presented with an ulceroproliferative growth involving the glans penis and prepuce with bilateral Inguinal lymphadenopathy, diagnosed as keratinizing squamous cell carcinoma by biopsy. Partial penectomy with bilateral modified ilio-inguinal lymph node dissection was performed. Postoperative period was uneventful. Histopathological examination (HPE) showed moderately differentiated, keratinising squamous cell carcinoma grade II invading the corpus spongiosum and corpus carvernosa. Perineural and vascular invasion was not present. All lymph nodes were free from tumor. On follow-up at 3 months, there was no evidence of local recurrence and metastasis. Patient was then lost to follow-up.
One and half year later, he developed pain in the right thigh. He consulted a local physician at his place, who advised him to have an X-ray on his right femur that showed osteolytic lesion (Fig. 1a). He was advised to consult at a higher center but he refused. Two days later during defecation in squatting position, he developed severe pain in the right thigh. Repeated X-ray showed a pathological fracture of same site (Fig. 1a). The patient was referred back to us. The patient was admitted and thoroughly examined. There was no local recurrence. Metastatic workup was done. X-ray of the chest showed a right sided lung metastasis (Fig. 1b). Ultrasound abdomen did not show any visceral metastasis. The serum calcium level was normal (9.38 mg/dl). Internal fixation by interlocking nail was performed for the fracture of the femur. A histopathological examination of the biopsy taken from the lesion of the femur showed metastatic keratinizing squamous cell carcinoma (Fig. 2). The patient was than referred to a cancer hospital for further management.
Fig. 1.

a X-ray femur pathological fracture, b X-ray chest—secondary metastasis
Fig. 2.
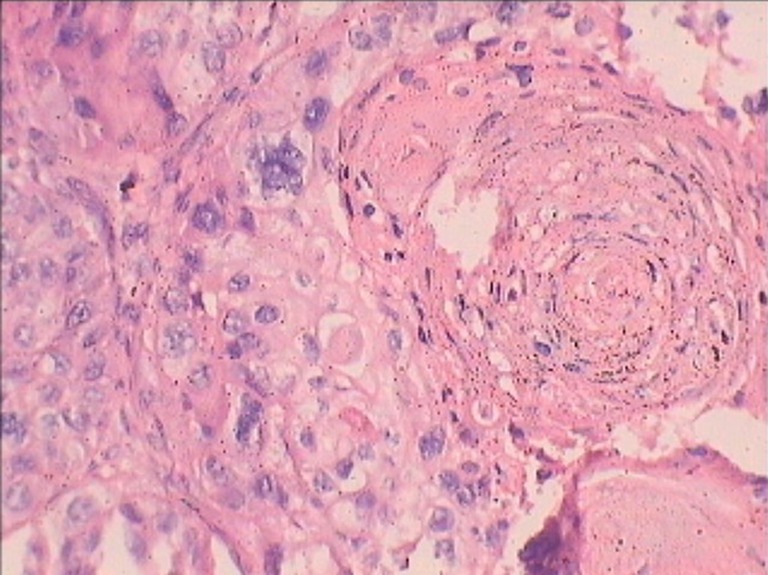
Histopathological picture of malignant lesion of bone showing keratin pearl (H&E staining, 10× magnification)
Discussion
Patients with primary penile malignancy with favorable histological features and no lymphatic spread have low risk for tumor metastasis. These patients are also best suited for organ-sparing or glans-sparing procedures. Distant metastasis is rare, and metastasis to the bones is even rarer. This patient had developed femur as well as asymptomatic lung metastasis.
Distant metastasis to the lung, liver, bone, or brain is uncommon [1] in the range of 1 to 10 %. A series of 224 patients, reported by Staubitz [2], showed 3.6 % (n = 8) incidence of distant metastasis.
Bony metastasis in cases of carcinoma penis is again very rare. Metastatic deposits to the iliac bone, ischial bone, and spine are reported [3]. This malignancy may mimic as a primary osteosarcoma of tibia [4] or as hypercalcemia and pathological fracture of the humerus [5]. Orbital [6], heart [7], and adrenal [8] metastasis are also reported in literature.
Our patient was a case of stage II (T2N0M0) disease with no lymphovascular invasion on histopathology, but after 18 months, he developed distant metastasis to the lungs and femur.
This is the first reported case of pathological fracture of the femur bone due to metastasis from grade II penile cancer, to the best of our knowledge.
Written informed permission was taken from the patient regarding publication of this case report. He had given consent to use his X-rays and histology report for publication None of the authors have any financial relationship with a biotechnology manufacturer, a pharmaceutical company, or other commercial entity that has an interest in the subject matter or materials discussed in the manuscript.
Acknowledgments
There is neither any financial interest, direct or indirect, those exist or may be perceived to exist for neither individual contributors nor any conflict of interest in connection with the content of this paper.
References
- 1.Curtis AP, Donald FL, John WD (2007) Tumors of the penis. Campbell-Walsh Urology, 9th Edition, Alain JW, Louis RK et al, Philadelphia, Saunders Elsevier. 1(31):959–992
- 2.Staubitz WJ, Melbourne HL, Oberkircher OJ. Carcinoma of the penis. Cancer. 1955;8:371–378. doi: 10.1002/1097-0142(1955)8:2<371::AID-CNCR2820080216>3.0.CO;2-#. [DOI] [PubMed] [Google Scholar]
- 3.Jacob R, Jyothirmayi R, Kumar A, Nair MK, Rajan B. Spinal metastasis from carcinoma of the penis. Br J Radiol. 1995;68:1367–1368. doi: 10.1259/0007-1285-68-816-1367. [DOI] [PubMed] [Google Scholar]
- 4.Ramachandran T, Subramanium PM, Prakasam K. A secondary carcinomatous lesion masquerading as a primary osteosarcoma—a case report. J Clin Diagn Res. 2013;7(3):563–5. doi: 10.7860/JCDR/2013/4098.2826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ho CCK, Nazri J, Zukifli MZ, Sritharan S, Hayati AR. Metastatic penile cancer presenting as hypercalcemia and pathological fracture of the humerus: a rare event. Med J Malaysia. 2006;61:503–505. [PubMed] [Google Scholar]
- 6.Shridhar PS, Asthana AK. Orbital metastasis from the carcinoma of penis in an elderly man. Asian J Ophthalmol. 2006;8:74–75. [Google Scholar]
- 7.Portero JN, Pardo FL, Pérez RC. Massive intracardiac metastases secondary to squamous cell carcinoma located at the level of the penis. Int J Cardiol. 2008;127(2):e96–e97. doi: 10.1016/j.ijcard.2007.04.092. [DOI] [PubMed] [Google Scholar]
- 8.Joshi 8, Joshi M, Basu S, Deshmukh M, Asopa R, Kane S. An original case of isolated unilateral adrenal metastasis from penile carcinoma: documentation by 18F-FDG-PET imaging and histopathology. Hell J Nucl Med. 2010;13(1):63–64. [PubMed] [Google Scholar]