

Abstract
Background
According to health technology assessment, patients deserve the best medicine. The development of drugs associated with solubility enhancers, such as cyclodextrins, represents a measure taken in order to improve the management of patients. Different drugs, such as estradiol, testosterone, dexamethasone, opioids, non-steroidal anti-inflammatories (NSAIDs; i.e. diclofenac), and progesterone are associated with cyclodextrins. Products containing the association of diclofenac/cyclodextrins are available for subcutaneous, intramuscular, and intravenous administration in doses that range from 25 to 75 mg. Medicinal products containing the association of progesterone/cyclodextrins are indicated for intramuscular and subcutaneous injection at a dose equal to 25 mg.
Objectives and Methods
The effects of cyclodextrins have been discussed in the solubility profile and permeability through biological membranes of drug molecules. A literature search was performed in order to give an overview of the pharmacokinetic characteristics, and efficacy and safety profiles of diclofenac/hydroxypropyl-β-cyclodextrin (HPβCD) and progesterone/HPβCD associations.
Results
The results of more than 20 clinical studies were reviewed. It was suggested that the new diclofenac/HPβCD formulation gives a rapid and effective response to acute pain and, furthermore, has pharmacokinetic and efficacy/safety profiles comparable to other medicinal products not containing cyclodextrins. One of the principal aspects of these new diclofenac formulations is that in lowering the dose (lower than 50 mg) the drugs could be more tolerable, especially in patients with comorbid conditions. Moreover, results of studies investigating the characteristics of progesterone and cyclodextrins showed that the new formulation (progesterone/HPβCD 25 mg solution) has the same bioavailability as other products containing progesterone. It is more rapidly absorbed and allows the achievement of peak plasma concentrations in a shorter time. Finally, the new formulation of progesterone was shown to be safe and not inferior to other products already on the market, with the exception of progesterone administered vaginally.
Conclusions
As shown by the results of clinical studies presented in this review, the newly approved medicines containing cyclodextrins have been found to be as effective and as well-tolerated as other medicinal products that do not contain cyclodextrins. Moreover, the newly approved lower dose of diclofenac associated with cyclodextrins is consistent with the European Medicines Agency recommendations reported in the revision of the Assessment Report for Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) and Cardiovascular Risk. Finally, the use of cyclodextrins led to significant increases in solubility and bioavailability of drugs, such as diclofenac and progesterone, and improvement in the efficacy and safety of these drugs.
Introduction
As a result of the introduction of Health Technology Assessment (HTA) in healthcare systems, the evaluation of a patient’s health and proper use of resources are becoming more important. Accordingly, HTA processes aim to ensure the choice of the best drug, in terms of safety and efficacy, and hence the development of drugs associated with solubility enhancers, such as cyclodextrins, represents one of the measures taken in order to improve patient management. When cyclodextrins are associated with drugs, the pharmacokinetic characteristics of these drugs can be modified, leading to an increase in the dissolution profile, solubility, and bioavailability.
The Biopharmaceutics Classification System (BCS) guidance stipulated by the US FDA categorizes drugs into four classes according to their solubility and permeability: Class I: high permeability, high solubility; Class II: high permeability, low solubility; Class III: low permeability, high solubility; Class IV: low permeability, low solubility [1]. In order to improve the solubility, dissolution rate and, therefore, the bioavailability of compounds belonging to the classes BCS II and IV, many techniques can be used. In particular, these include micronization, self-emulsification, complexation with cyclodextrins, co-crystallization, supercritical fluid technology, and several other techniques [2].
Cyclodextrins, Solubility Enhancers
Cyclodextrins, described for the first time in 1891, are cyclic oligosaccharides, characterized by an outer hydrophilic portion and a central lipophilic cavity [3]. As shown in Table 1, each cyclodextrin is characterized by the presence of a specific functional group. Among these, the most widely used are α-, β- and γ-cyclodextrin. In 1976, β-cyclodextrin was used for the first time in a pharmaceutical formulation. In the year 2014, several medicines containing cyclodextrins, in formulations for oral, parenteral, ophthalmic, and topical administration, were authorized worldwide (Table 2) [3–5].
Table 1.
Functional groups of main cyclodextrins used in the pharmaceutical industry
| Cyclodextrin | Functional group |
|---|---|
| α-Cyclodextrin (α-CD) | H4 |
| β-Cyclodextrin (β-CD) | H5 |
| γ-Cyclodextrin (γ-CD) | H6 |
| Diethyl-ethyl-β-cyclodextrin (DE-β-CD) | CH2CH3 or H |
| Dimethyl-ethyl-β-cyclodextrin (DM-β-CD) | CH3 or H |
| Hydroxypropyl-β-cyclodextrin (HP-β-CD) | CH2CH0HCH3 or H |
| Hydroxypropyl-γ-cyclodextrin (HP-γ-CD) | CH2CH0HCH3 or H |
| Methyl-β-cyclodextrin (M-β-CD) | CH3 or H |
| Sulfobutylether-β-cyclodextrin (SBE-β-CD) | (CH2)4SO3Na or H |
Table 2.
Examples of drugs associated with cyclodextrins in medicinal products
| Active ingredient | Cyclodextrin | Route of administration |
|---|---|---|
| Alprostadil | α-CD | Intracavernous |
| Aceclofenac | β-CD | Oral |
| Benexate | β-CD | Oral |
| Cetirizine | β-CD | Oral |
| Cholecalciferol | β-CD | Oral |
| Diphenhydramine HCl | β-CD | Chewing tablet |
| Ethinylestradiol/drospirenone | β-CD | Oral |
| Fenofibrate | β-CD | Oral |
| Flunarizine | β-CD | Oral |
| Metronidazole | β-CD | Topical |
| Naphazoline | β-CD | Ophthalmic |
| Nicotine | β-CD | Oral |
| Nimesulide | β-CD | Oral |
| Nitroglycerin | β-CD | Sublingual |
| Omeprazole | β-CD | Oral |
| Desloratadine | β-CD | Oral |
| Piroxicam | β-CD | Oral |
| Pramipexole | β-CD | Oral |
| Itraconazole | HB-β-CD | Intravenous |
| Levothyroxine sodium | HB-β-CD | Oral |
| Mitomycin | HB-β-CD | Intravenous |
| Octinoxate/avobenzone | HB-β-CD | Topical |
| Risperidone | HB-β-CD | Oral |
| Chloramphenicol | M-β-CD | Ophthalmic |
| Amiodarone | SBE-β-CD | Intravenous |
| Aripiprazole | SBE-β-CD | Intramuscular |
| Carfilzomib | SBE-β-CD | Intravenous |
| Maropitant | SBE-β-CD | Subcutaneous |
| Ziprasidone | SBE-β-CD | Intramuscular |
Drugs mentioned in this table are BCS Class I, II, III and IV
Cyclodextrins are used in the pharmaceutical industry because of their ability to form inclusion complexes with hydrophobic drugs, thus causing an increase in their water solubility. The complexes are easily absorbed. Studies suggest that cyclodextrins are able to increase the oral bioavailability of drugs belonging to BCS Class II, but to reduce the bioavailability of the drugs of Class I and III [6, 7]. Cyclodextrins can enhance the permeation of lipophilic drugs through biological membranes, and increase the chemical stability of drugs at the aqueous membrane exterior. Specifically, only the free drug permeates the lipophilic membranes, while cyclodextrins, except for an insignificant amount, cannot penetrate through biological membranes. These effects can be explained by different mechanisms. First, the development of inclusion complexes increase the amount of dissolved drug molecules in the aqueous donor phase, with a consequent increase in the concentration gradient of the drug over the unstirred water layer (UWL). The rapid release of the drug from the complex increases the availability of free drug molecules close to the lipophilic membrane surface. Moreover, cyclodextrin complexation of drug may reduce the interaction between drug molecules and other molecules in the UWL, enhancing the global delivery of the drug to the membrane surface. Additional mechanisms of action are not excluded [8].
Cyclodextrins have multiple effects on the body’s organs. In particular, they increase the transendothelial permeability of hydrophobic drugs and boost the effects of estradiol, testosterone, and dexamethasone on the central nervous system (in rats). Cyclodextrins also prolong the analgesic effects of opioid peptides, morphine, lofentanil, alfentanil and sulfentanil, and enhance the intestinal penetration of peptides. Absorption through the nasal mucosa and the bioavailability of hydrophobic drugs, oligopeptides, and peptides is also enhanced, while the irritant effects on the oral cavity, throat, and pharynx are reduced [9].
In the lungs, cyclodextrins reduce smells, taste, and local irritation associated with the drugs administered by inhalation. Solubility and the degree of permeation of drugs through the skin with minimal occurrence of adverse events are also influenced [9]. Moreover, cyclodextrins increase the shelf-life of the product they are complexed with [10].
Data obtained from scientific literature confirm that cyclodextrins reduce drug toxicity. In particular, the association of hydroxypropyl-β-cyclodextrin (HPβCD)/flurbiprofen showed a reduction in gastroduodenal toxicity in rats. The association of 5-fluorouracil and folinic acid/β-cyclodextrin resulted in a reduced phlebitis in a rabbit ear vein model [11, 12]. Moreover, other preclinical studies suggested that the administration of complexes HPβCD or β-cyclodextrin and ketorolac, meloxicam, or naproxen led to a reduction in the risk of ulcers and gastric damage [11, 13, 14].
Although the same cyclodextrins can be associated with gastrointestinal, metabolic, and renal events, as well as increase in neoplasms of acinar cells in animals, the safety profile in humans is favorable [15, 16].
Association of Hydroxypropyl-β-Cyclodextrin (HPβCD) and Diclofenac
Diclofenac is a phenylacetic acid derivative belonging to the class of non-steroidal anti-inflammatory drugs (NSAIDs). NSAIDs include a heterogeneous group of molecules having anti-inflammatory, antipyretic, analgesic, antiplatelet and, in some cases, uricosuric action. They share the same mechanism of action, the inhibition of the cyclooxygenase enzyme [COX or prostaglandin H2 (PGH2) synthase], which catalyses the conversion of arachidonic acid to PGH2 by reducing the synthesis of prostanoids. The two enzymes, COX-1 and COX-2, play different roles in the inflammatory process and in the regulation of the local homeostasis, depending on the effects of prostanoids in the kidney, platelets, vascular system, etc. (Fig. 1) [17, 18].
Fig. 1.
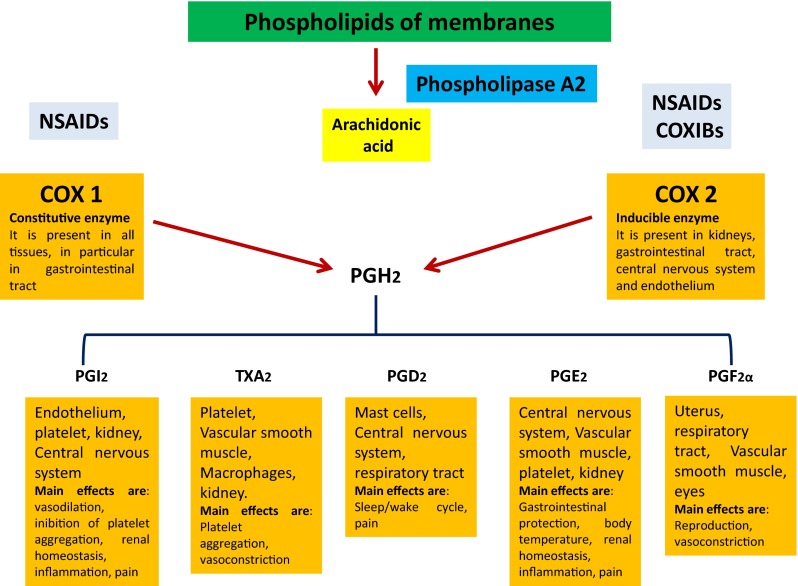
Effects mediated by COX-1 and COX-2. COX cyclooxygenase, NSAIDs non-steroidal anti-inflammatory drugs, PGH2 prostaglandin-H2, PGI2 prostaglandin I2, TxA2 thromboxane A2, PGD2 prostaglandin D2, PGE2 prostaglandin E2, PGF2 prostaglandin F2α
The main clinical uses of NSAIDs include the treatment of inflammatory diseases and pain. Some also have good antipyretic activity. Acetylsalicylic acid, which inhibits COX-1 in platelets, is used as an antiplatelet agent in the prevention of cardiovascular diseases. Moreover, some NSAIDs are indicated in the treatment of acute and chronic gout and hypercalcemia associated with tumors. The selective COX-2 inhibitors (COXIBs) are also indicated in the treatment of inflammatory diseases.
NSAIDs can be administered via different routes. Among the available formulations, oral administration is usually preferred by patients as being easier to use. It allows self-administration but can be associated with different gastrointestinal adverse events. A delay in analgesic efficacy compared with intramuscular and intravenous administration can be observed [19]. Intramuscular formulations can give volume of drug equal to 2–5 ml, and are feasible for drugs that irritate subcutaneous tissue. Finally, several advantages are derived from subcutaneous administration. This route allows self-administration of multiple doses, does not require a specific muscle mass (unlike the intramuscular preparation), and is characterized by a better tolerability profile [20].
However, these drugs are not risk-free. Therapy with NSAIDs is associated with adverse events linked to hypersensitivity, gastrointestinal, renal, cardiovascular, hepatic, and central nervous systems [17, 21].
It is known that NSAIDs associated with β-cyclodextrin have a more rapid onset of action after oral administration and a better gastrointestinal tolerability. A drug with such characteristics is piroxicam-β-cyclodextrin [22]. A recent work by Hanumegowda et al. revealed that the use of HPβCD and β-cyclodextrin reduced gastric damage, gastric lesion, and the extent of ulceration associated with etodolac, phenylbutazone, naproxen, indomethacin, and ketorolac [11].
In addition, diclofenac, one of the more prescribed NSAIDs worldwide [23–25], was associated with cyclodextrins, and was marketed in formulations for subcutaneous, intramuscular, and intravenous administration. The drug, not associated with cyclodextrins, is also available in formulations for oral and topical administration. In Fig. 2 phase solubility diagrams of the diclofenac/HPβCD complex is illustrated. In Fig. 3 guest–host complex equilibrium equation of the diclofenac/HPbCD complex is reported.
Fig. 2.

Type A phase solubility diagram of HPB/D 1:1 complex. The stoichiometry and complex formation constant of the HPB/D complex were measured according to Higuchi and Connors [64], by phase solubility experiment. The resulting diagram is a type A curve with a 1:1 guest:host complex stoichiometry. HPB hydroxypropyl-β-cyclodextrin, D diclofenac
Fig. 3.
Guest–host complex equilibrium
Diclofenac has remarkable antirheumatic, anti-inflammatory, analgesic, and antipyretic properties, in addition to being an effective painkiller in rheumatic and non-rheumatic pain. For oral and injectable formulations, a maximum dose of 150 mg/day and 75–150 mg/day is recommended, respectively. Like other NSAIDs, diclofenac exerts its effect mainly at the level of COX-1 and COX-2, with greater selectivity for COX-2, although a recent review showed that it may have had additional mechanisms of action [26]. Relative to the pharmacokinetic characteristics, diclofenac has an oral bioavailability of 54 ± 2 %, a time to reach maximum concentration (tmax) of 2.5 h, a maximum concentration (Cmax) of 0.42–2 µg/ml, and a volume of distribution equal to 12 L. The drug is 99.7 % bound to plasma proteins. The metabolism of diclofenac is primarily operated by oxidation and glucoronidation. Less than 1 % is excreted as unchanged through the urinary tract [17].
Diclofenac is associated with gastrointestinal, cardiovascular, and hepatic events, hypersensitivity reactions, and headaches [27–29]. In relation to cardiovascular risk, its use is recommended at the minimum effective dose [30], which is facilitated by associating diclofenac with HPβCD.
As previously mentioned, diclofenac, belonging to BCS Class II, was associated with HPβCD in two pharmaceutical products—Dyloject® 75 mg/2 ml and 37.5 mg/ml, and Akis® 25, 50, and 75 mg. HPβCD increases diclofenac solubility from 138 to 1030 μg/ml [31]. Dyloject® is available as a solution for intramuscular and intravenous use, while Akis® is available as a solution for subcutaneous and intramuscular use. Akis® is available in the classical doses of 50 mg and 75 mg/ml, and in a new dose of 25 mg/ml in an aqueous volume reduced by 66 % compared with an intramuscular solution (1 ml instead of 3 ml).
The main innovation of these products is the reduced dose. The availability of doses lower than 50 mg allows the lowest effective dose to be used and the therapy to be modulated, depending on the patient, especially if the patient is elderly and/or with comorbid conditions. The innovation also includes the type of device. Akis® is marketed as a pre-filled syringe for subcutaneous injection, which allows self-administration of multiple doses, does not require a specific muscle mass, and is characterized by a better tolerability profile.
Thus, these new drug treatments offer many advantages, among which the ease of administration, the rapidity of action (which is typical of an injection), and the maintenance of the painkiller effect even in the presence of a reduced dose are the most important.
Clinical Study Evaluating Pharmacokinetic Characteristics, Efficacy, and Safety Profile of Diclofenac/HPβCD Formulations
Several clinical studies evaluated the pharmacokinetic characteristics, efficacy, and safety profile of Dyloject® (diclofenac for intramuscular and intravenous use) and Akis® (diclofenac for subcutaneous and intramuscular use) alone or in comparison with other drugs indicated for the treatment of pain [19, 32–41]. The study by Zeitlinger et al. compared the bioavailability of diclofenac HPβCD (75 mg/ml, administered intramuscularly or subcutaneously) with Voltaren® [diclofenac complexed with polyethylene glycol (PEG) and benzyl alcohol (BA); 75 mg/3 ml, administered intramuscularly] in 24 healthy volunteers. Based on the parameters of Cmax and area under the concentration–time curve (AUC), the authors concluded that the new formulation for subcutaneous and intramuscular use of diclofenac HPβCD 75 mg/ml can be considered bioequivalent to Voltaren®. Although there was a slightly higher peak plasma concentration with intramuscular diclofenac HPβCD compared with the reference formulation, this difference was not statistically significant [32].
Similarly, the randomized, single-dose, three-way, crossover relative bioavailability study of Salomone et al. evaluated the relative bioavailability of the new subcutaneous formulation of diclofenac HPβCD (50 mg/1 ml) administered in three different body sites—quadriceps, gluteus, and abdomen—in 12 healthy males. The injection of diclofenac HPβCD was administered on 3 different days, with a washout period of 5 days. Results demonstrated that tmax was rapid for the three administrations, with a median value of 30 min, without significant differences. The analysis of AUC from time zero to time t (AUCt) and AUC from time zero to infinity (AUC∞) revealed that exposure to the drug was comparable for the three sites. Furthermore, Cmax was comparable after injection in the quadriceps and abdomen areas, but was 17 % higher after administration in the gluteus. Regarding the safety profile, no serious adverse events were observed, and the only adverse events (n = 22 in 12 subjects) included injection site reactions [33]. Finally, Mermelstein et al. conducted two separate studies in healthy volunteers. The first was a single-dose, randomized, four-way, crossover study in which the pharmacokinetic characteristics of Dyloject® versus Voltarol® (diclofenac/PEG) after intravenous and intramuscular administration were compared. The second study was a multiple-dose, randomized, three-way, crossover study that compared the pharmacokinetics after intravenous administration of single and multiple doses of 18.75 and 37.5 mg of diclofenac HPβCD versus Cataflam® (oral immediate-release diclofenac). The results of these studies revealed that the bioavailability of diclofenac HPβCD was equivalent to Voltarol® after intravenous and intramuscular administration. Diclofenac HPβCD also showed dose proportionality after single- and multiple-dose administration, without evidence of accumulation [34].
Other studies evaluated the efficacy and safety profile of diclofenac HPβCD. A recent phase III, randomized clinical trial compared the efficacy and safety of diclofenac HPβCD (for subcutaneous and intramuscular use) versus placebo in patients with moderate to severe pain after third molar extraction. Enrolled patients were randomized into the following groups: diclofenac HPβCD 25 mg (n = 77), diclofenac HPβCD 50 mg (n = 76), diclofenac HPβCD 75 mg (n = 78), or placebo (n = 75). The primary endpoint was the evaluation of the pain intensity difference (PID) 1.5 h after drug administration. Results showed that PID was higher in all patients treated with diclofenac, without significant difference between diclofenac groups. Results also revealed that, after 5 h of drug administration, diclofenac 50 and 75 mg were statistically superior to placebo (p < 0.001), while after 6 h only diclofenac 50 mg was statistically superior to placebo (p = 0.027). Regarding tolerability, 57 patients experienced 107 adverse events, of which only 16 were considered to be related to the pharmacological treatment. Although no differences between groups were detected with regard to the percentage of patients reporting an adverse event, the authors stated that diclofenac 25 mg was associated with a lower incidence of adverse events, such as gastrointestinal and injection site reactions [35].
Leeson et al. compared the efficacy and safety of diclofenac HPβCD 75 mg versus Voltarol® 75 mg and placebo in the treatment of pain for molar extraction in 155 patients. The authors evaluated the superiority of diclofenac HPβCD versus placebo and non-inferiority versus Voltarol® on the basis of the total pain relief in the 4 h following administration of the drug, through the visual analog scale (VAS). Diclofenac HPβCD was found to be superior to placebo and Voltarol®. Fifteen minutes after drug administration, the intensity of pain reduced by 30 in 52 % of patients treated with diclofenac HPβCD and 21 % of patients treated with Voltarol® (p = 0.0022). The incidence of adverse events was similar among groups, with the exception of the adverse event ‘phlebitis’, which was more frequent in the group treated with Voltarol® [36].
The randomized clinical trial DIRECT compared the efficacy and safety of diclofenac HPβCD 75 mg, administered subcutaneously or intramuscularly, versus Voltaren® 75 mg, administered intramuscularly, in 325 hospitalized patients with programmed orthopedic surgery with moderate to severe pain. The primary endpoint was the evaluation of local tolerability within 18 h after the injection. The appearance of local signs or symptoms was evaluated through a 4-point scale (0 = missing symptoms or signs; 3 = severe symptoms or signs). The study also assessed the analgesic efficacy of the drugs and the percentage of patients who requested a second injection of the drug on the second day after surgery. A very good tolerability for all formulations of diclofenac was observed. The average safety scores for diclofenac HPβCD, administered subcutaneously and intramuscularly, and Voltaren® was equal to 0.57, 0.31, and 0.26, respectively. A higher number of patients in the subcutaneous diclofenac HPβCD group experienced an adverse event or an adverse drug reaction compared with the other groups (no statistically significant differences). Three serious adverse events occurred in two patients (one treated with subcutaneous diclofenac HPβCD and one treated with Voltaren®). Regarding the efficacy endpoint, pain rapidly decreased after administration of diclofenac, without significant differences between the groups. A second injection of the drug was requested in 12 (11.0 %), 18 (16.8 %), and 14 (12.8 %) patients in the groups treated with diclofenac subcutaneously, diclofenac intramuscularly, and Voltaren®, respectively. These results showed that, in terms of efficacy and safety, the new formulation of diclofenac was comparable to Voltaren®. Therefore, diclofenac HPβCD may represent a valid alternative to the already existing formulation for intramuscular use [37].
Lastly, Mazzotti et al. compared the efficacy and tolerability of subcutaneous and intramuscular diclofenac HPβCD (groups 1 and 2) versus intramuscular diclofenac PEG–BA (group 3) in 299 patients undergoing orthopedic surgery of the lower limb. The primary endpoint was the evaluation of the reduction in postoperative pain, while the secondary endpoint was the evaluation of injection site reactions. The presence of skin redness and skin swelling was evaluated with a 4-point scale (0 = absent symptoms; 3 = severe symptoms). According to the results of the study, no significant differences in the reduction of postoperative pain were observed (p = 0.3). A second injection of the drug was requested for 10 patients in group 1 (10.3 %), 18 in group 2 (17.6 %) and 12 patients in group 3 (12.0 %). Between groups, no statistically significant differences in the occurrence of adverse events were observed, with the exception of the adverse event ‘persistent swelling’ in the subcutaneous diclofenac HPβCD group (0.50 ± 0.98 in group 1; 0.32 ± 0.67 in group 2; 0.27 ± 0.52 in group 3) [19].
The efficacy and safety of diclofenac HPβCD were also compared with ketorolac tromethamine in three clinical studies [38–40]. In the first, a randomized, phase III, clinical trial, 331 patients undergoing surgery received diclofenac HPβCD (18.75 or 37.5 mg) or ketorolac tromethamine (30 mg). Results revealed that both diclofenac HPβCD and ketorolac determined a significant reduction in pain intensity compared with placebo (p < 0.05). Moreover, both drugs significantly reduced the need to take opioid analgesics [38]. Similar results were obtained from a single-dose, randomized, double-blind, placebo- and comparator-controlled, parallel-group study in which 353 patients with moderate to severe pain received intravenous diclofenac HPβCD 3.75, 9.4, 18.75, 37.5, or 75 mg, or placebo, or ketorolac 30 mg. The authors evaluated the effects of the drugs on the total pain relief over 6 h through the VAS. Results showed that diclofenac was superior to placebo (p < 0.0001). Moreover, a higher proportion of patients in the diclofenac 37.5 and 75 mg groups reported 30 % or greater pain relief compared with ketorolac 30 mg or placebo groups [39]. In the study by Daniels et al., adult patients with moderate and severe pain were treated with Dyloject®, ketorolac tromethamine, or placebo within 6 h after surgery. According to efficacy results, the sum of PIDs (SPID) was significantly better with HPβCD diclofenac and ketorolac than placebo (p < 0.0001). Furthermore, a better SPID score, faster onset of analgesia, and lower opioid requirement were observed in the diclofenac HPβCD cohort than in the ketorolac cohort (p < 0.008). The incidence of treatment-related adverse events was similar across groups [40].
Finally, Chelly et al. evaluated the safety profile of an intravenous bolus of diclofenac HPβCD in a multicenter, open-label, repeated dose, multiple-day, single-arm safety study. Of a total of 1171 patients screened, 971 received diclofenac HPβCD at different doses (65 % of patients received 37.5 mg, while 35 % of patients received 50 mg due to a higher body weight). Diclofenac was administered every 6 h. Results revealed that diclofenac HPβCD was well-tolerated [41].
In conclusion, data from the literature showed that the new diclofenac formulations may be considered comparable, in terms of efficacy and safety, to pharmaceutical products containing diclofenac already available, as well as drugs belonging to the same class of diclofenac, such as ketorolac tromethamine.
Finally, the new approved doses (25 and 37.5 mg) are in line with the European Medicines Agency (EMA) recommendations mentioned in the Assessment Report for Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) and Cardiovascular Risk report. In this assessment, the EMA defined the cardiovascular toxicity associated with diclofenac and other NSAIDs as dose-related and, for this reason, recommended a reduction in doses of these drugs [30].
Association of HPβCD and Progesterone in Gynecology
In men and women, the reproductive function is regulated by the hypothalamus-hypophysis-gonadal axis. At the hypothalamic level there are neurons that synthesize the gonadotropin-releasing hormone (GnRH), which promotes the production and release of the follicle-stimulating hormone (FSH) and luteinizing hormone (LH). These gonadotropins are essential for the maturation of the follicle, production of estrogen, induction of ovulation, and the production of progesterone by the corpus luteum in the luteinic phase in women. They are also essential for spermatogenesis and testosterone production in men. The release of GnRH and gonadotropins is controlled by estrogens and progestogens [42].
Progesterone is the progestin hormone produced by gonads, adrenal glands, and placenta. It interacts with two nuclear receptors, PR-A and PR-B. Once tied to receptors, progesterone induces effects on the reproductive system and metabolic effects. At hypothalamic level, progesterone induced a time-dependent reduction of the release of gonadotropins with a reduction of LH pulse [42, 43].
Synthetic progestins, widely used in clinical practice, inhibit ovulation and cause an endometrial transformation [25, 44]. These drugs are indicated in preparation for gynecologic and extra-gynecologic surgery during pregnancy, threatened abortion, hyper- or hypo-menorrhea and other menstrual disorders, premenstrual syndrome, and prophylaxis of postnatal depression. They are also indicated as a progestin supplement in the luteinic phase during spontaneous or induced cycles, assisted pregnancies or primitive or secondary ovarian failure [45, 46].
Synthetic progestins are available in formulations for oral, vaginal, intramuscular, and intrauterine device (IUD) administration. Moreover, synthetic progestins were recently approved in a new formulation for subcutaneous use.
Oral formulations of progesterone are not widely used because they are associated with reduced bioavailability. The vaginal administration is preferred as it is easy to administer, avoids first-pass metabolism, ensures the achievement of high concentrations of progesterone in the uterus, and does not cause systemic effects, although it may be associated with the occurrence of local adverse events. Finally, intramuscular administration ensures the achievement of good plasma concentrations of progesterone but can be associated with injection site reactions. With regard to pharmacokinetic characteristics, after administration of a vaginal capsule (100 mg), the mean Cmax is equal to 31.53 ± 9.15 nmol/l, with a tmax equal to 6.92 ± 3.12 h, and a terminal half-life of 16.39 ± 5.25 h. After intramuscular administration, the 17α-hydroxyprogesterone caproate is released from the deposit [BA and ethyl oleate (EO)] in biphasic mode and with half-lives of 5–11 days. It is rapidly excreted unchanged or in the form of metabolites. The elimination of the drug is predominantly biliary, and half-life is approximately 10 h [47, 48].
Regarding tolerability, medicines containing progesterone can induce the occurrence of peripheral thromboembolic, pulmonary, ocular, and cerebral events [48]. Moreover, in recent years, estrogen–progestin combinations were also associated with a two to fourfold increase in the risk of breast cancer when compared with the therapy with estrogen only [49, 50].
Progesterone, belonging to BCS Class II, presents a reduced solubility in water, amounting to 0.007 mg/ml at 25 ± 2 °C. The addition of solubility enhancer, such as PEG 400, polysorbate 80, Captisol 3 % [sulfobutyl ether beta-cyclodextrin (SBEβCD)] or Trappsol® 3 % (HPβCD) determines an increase of progesterone solubility up to 15.3 ± 0.03, 11.9 ± 2.31, 1.6, and 1.1 mg/ml, respectively [51].
In February 2013, the Medicines and Healthcare products Regulatory Agency (MHRA) granted marketing authorization for ‘Lubion® 25 mg solution for intramuscular and subcutaneous injection’, indicated as luteal phase support during assisted reproductive technology (ART) in infertile women who are unable to use or tolerate vaginal preparations. In this product, progesterone is complexed with hydroxypropylbetadex or HPβCD. In Figs. 4 and 5, phase solubility diagrams of the progesterone/HPβCD complex and mechanism of the molecular association of the complex are reported. In November 2013 and September 2014, two other products with the same composition (progesterone and HPβCD) were marketed, as well as indications for Lubion®, Pleyris® 25 mg solution for intramuscular and subcutaneous injection, and Prolutex® 25 mg solution for subcutaneous injection.
Fig. 4.

Type A phase solubility diagram of HPB/Prg 2:1 complex. The stoichiometry and complex formation constant of HPB/Prg complex were measured according to Higuchi and Connors [64], by phase solubility experiment. The resulting diagram is a type A curve with a 1:2 guest:host complex stoichiometry. HBP hydroxypropyl-β-cyclodextrin, Prg progesterone
Fig. 5.

Mechanism of molecular association of the progesterone/hydroxypropyl-β-cyclodextrin complex. HBP hydroxypropyl-β-cyclodextrin, Prg progesterone
The addition of HPβCD leads to an increase in the solubility of progesterone. According to Dahan et al., a linear increase in the solubility of progesterone with increasing concentrations of HPβCD was observed [52]. This increase results in a consequent increase in bioavailability. In this respect, the results of differential scanning calorimetry and Fourier transformed infrared spectroscopy showed that progesterone, which diffuses into the cavity of cyclodextrin, has an increase in bioavailability after oral administration [53]. Moreover, it is known that the use of nanoaggregates of polyethylene oxide-polypropylene oxide and β-cyclodextrin copolymer significantly improves the release, efficacy, and tolerability of progesterone [54, 55]. The inclusion of progesterone in HPβCD leads to a stable pharmaceutical product, easy self-administration and potentially characterized by good compliance [56]. In addition, the subcutaneous administration of progesterone could represent a good alternative for patients who cannot be treated vaginally.
Clinical Study Evaluating Pharmacokinetic Characteristics, Efficacy, and Safety Profile of the Progesterone/HPβCD Formulation
Lubion® authorization clinical studies evaluated the pharmacokinetic characteristics (studies CRO-PK-03-55 and CRO-PK-05-143), the effects on the endometrium and the pharmacodynamic characteristics (study CRO-05-66), the clinical efficacy (studies 07EU/Prg06 and 07US/Prg05), and the tolerability (study CRO-06-82) of the association of progesterone/HPβCD. A single-center, open-label, randomized, three-way, crossover pharmacokinetic study (CRO-PK-05-143) evaluated the linearity of 25, 50, or 100 mg of progesterone in a 1 ml volume by subcutaneous injection in 12 postmenopausal female healthy volunteers. Results showed a proportional increase in Cmax and AUCt values for doses of 25–100 mg. Regarding efficacy, two randomized, non-inferiority studies (07EU/Prg06 and 07US/Prg05) compared Lubion® with Crinone® (progesterone vaginal gel) and Endometrin® (progesterone vaginal insert), respectively, in women undergoing in vitro fertilization (IVF). The primary efficacy endpoint was the proportion of patients who were pregnant 10 weeks after the start of treatment, while the secondary efficacy endpoint was the implantation rate, positive β-HCG test rate, biochemical pregnancy, clinical pregnancy rate and early spontaneous abortions, as well as delivery rate, including live rate and newborn status. Results of the 07EU/Prg06 study demonstrated that subcutaneous progesterone was non-inferior to Crinone®, while results of the 07US/Prg05 study showed that, at 10 weeks, ongoing pregnancy rates were comparable between the two treatment groups [56].
Similarly, the pharmacokinetic characteristics of the new formulation of progesterone versus Prontogest® (progesterone complexed with BA and EO) were evaluated by Sator et al. in three clinical studies that enrolled post-menopausal women and healthy female volunteers aged 18–45 years. The results revealed that the new formulation of progesterone had the same bioavailability of Prontogest®, but allowed the achievement of peak serum concentrations in a shorter time frame (1 vs. 7 h; p < 0.0001). In light of the data obtained, the formulations of progesterone were found to be bioequivalent [57]. The efficacy and safety of progesterone HPβCD (Prolutex®, 25 mg) versus Crinone® (progesterone gel, 8 %) in support of the luteal phase in patients undergoing ART were assessed in a recent non-inferiority randomized clinical trial. The study enrolled 683 patients randomized into the following groups: Prolutex® 25 mg/day subcutaneously (n = 339) and Crinone® (progesterone gel) 90 mg/day (n = 344). The ongoing pregnancy rate at the week ten amounted to 27.4 % in the group treated with Protulex® and 30.5 % in the group treated with Crinone® (difference between the groups was not significant). These data confirmed the non-inferiority of Prolutex® compared with Crinone® [58]. Efficacy of Prolutex® was also compared with Endometrin® (progesterone for vaginal use) in a prospective, open-label, randomized, controlled, parallel-group, multicenter, two-arm, non-inferiority study. The study enrolled 800 women, aged 18–42 years, who have completed ART cycles and are currently undergoing IVF. The primary efficacy endpoint was the proportion of patients who had an ongoing pregnancy of 10 weeks after the start of progesterone treatment. According to study results, the ongoing pregnancy rates at 12 weeks of gestation were comparable between the Prolutex® and Endometrin® groups (41.6 vs. 44.4 %), with a difference between groups of 22.8 % (95 % CI 29.7–4.2). With regard to safety results, adverse events occurred with similar frequency in each group. The most common adverse events in the Prolutex® group were injection site reactions (injection site bruising, inflammation, oedema and injection site pain), with the majority of these adverse events being reported as mild [59].
In conclusion, the results of the above clinical studies did not show significant differences between the new formulation of progesterone for subcutaneous use, complexed with HPβCD, and the products already marketed. Therefore, the new formulation of progesterone represents a valid alternative to the existing formulations.
Discussion
The ability of cyclodextrins to form inclusion complexes with a remarkable variety of organic compounds allowed wide use of these products in the pharmaceutical, cosmetic, food, and textiles industries. Cyclodextrins allow significant increases to be obtained in the stability, solubility, and bioavailability of drugs they are complexed with. Cyclodextrins are used for the development of several pharmaceutical products in different formulations, such as tablets, nasal sprays, aqueous parenteral solutions, and eye-drop solutions. Frequently used cyclodextrins are β-CD, for example in cetirizine and cisapride products, γ-CD in minoxidil solution, SBE-β-CD voriconazole for intravenous use, and HPβCD in itraconazole for intravenous and oral use [60]. HPβCD properties have now been confirmed by clinical studies that evaluated the pharmacokinetic characteristics, efficacy, and tolerability of diclofenac and progesterone in inclusion complexes of HPβCD.
The results of pharmacokinetic studies revealed that diclofenac HPβCD for subcutaneous and intramuscular use is bioequivalent to other diclofenac formulations not containing cyclodextrins [32, 34]. Data from clinical studies evaluating the efficacy and safety profile of diclofenac HPβCD showed no difference in PID or in the occurrence of adverse events between diclofenac groups. Furthermore, the results of the DIRECT trial, as well as the results of the Mazzotti et al. study, confirmed that no statistical differences were detected between the groups in the reduction of pain after administration of diclofenac [19, 35, 37].
When diclofenac HPβCD was compared with ketorolac tromethamine in the treatment of pain [38–40], these drugs showed a comparable efficacy profile, although it is important to highlight that in the diclofenac HPβCD cohort, better SPID scores, a faster onset of analgesia, and a lower opioid requirement were observed [40]. With regard to the safety profile, as reported by Dietrich et al., although no differences between groups were detected in the percentage of patients reporting an adverse event, diclofenac 25 mg was associated with a lower incidence of adverse events, such as gastrointestinal and injection site reactions [35]. Leeson et al. also reported a good safety profile. According to results, the adverse event ‘phlebitis’ was more frequent in the group treated with Voltarol® than in patients treated with diclofenac HPβCD [36]. This better safety profile could be explained by the substitution of PEG–BA excipients, which are known vascular irritants and the cause of pain at the injection site, with HPβCD, which is non-toxic and minimally irritating to veins [61]. Furthermore, cyclodextrins prevent the direct contact of drugs with biological membranes. In that way, they are able to reduce drug toxicity and local irritation with no loss of therapeutic benefits [62]. On the other hand, the study by Chiarello et al. revealed that the adverse event ‘pain at the injection site’ was more common among patients treated with subcutaneous diclofenac HPβCD, and that a higher number of patients in this group experienced an adverse event or an adverse drug reaction compared with the other groups (no statistically significant differences) [37]. Similarly, the results of the study by Mazzotti et al. showed that the adverse event ‘persistent swelling’ was more severe in patients treated with subcutaneous diclofenac HPβCD [19].
Several clinical studies evaluated the pharmacokinetic characteristics, clinical efficacy, and safety of progesterone/HPβCD. According to these studies, Lubion® and Prolutex® are not inferior to Crinone® and Endometrin® [56, 58, 59]. Progesterone HPβCD seemed to be more tolerable compared with progesterone not associated with cyclodextrins. Results obtained from Lubion® authorization clinical studies revealed that, although no statistically significant difference was detected, patients treated with Prontogest® had pain at the injection site for a longer period of time than patients treated with Lubion®. Similarly, it was found that the adverse events ‘swelling’ and ‘redness’ were more frequent in patients treated with Prontogest® compared with patients treated with Lubion® (3.8 vs. 0; 30.97 vs. 23.87 %) [56].
Conclusions
As shown by the results of clinical studies presented in this review, the medicinal products containing the association of diclofenac/HPβCD and progesterone/HPβCD have been found to be effective and well-tolerated, as well as other medicinal products not containing cyclodextrins. The presence of HPβCD resulted in good stability, solubility, and bioavailability of the preparations; therefore, clear benefits will derive from the use of these drugs in clinical practice. Moreover, according to HTA processes, evaluation of the efficacy, effectiveness, and efficiency of diclofenac/HPβCD and progesterone/HPβCD associations will confirm the good efficacy/safety profile already found in clinical studies presented in this review.
As a result of the characteristics of the cyclodextrins, i.e. versatility, typical structure, and chelating properties, these substances will play an increasingly important role in the pharmaceutical area, improving the bioavailability, and, in some cases, the tolerability, of the drugs that they will be associated with [63].
Compliance with Ethical Standards
Tiziano Fossati is Head of R&D Pharmaceuticals, IBSA, Switzerland. Cristina Scavone, Angela Colomba Bonagura, Sonia Fiorentino, Daniela Cimmaruta, Rosina Cenami, Marco Torella and Francesco Rossi declare no conflicts of interest.
References
- 1.Guidance for Industry. Waiver of in vivo bioavailability and bioequivalence studies for immediate-release solid oral dosage forms based on a biopharmaceutics classification system. US Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER). August 2000 BP. Available at: http://www.fda.gov/downloads/Drugs/…/Guidances/ucm070246.pdf. Accessed 14 Jan 2016.
- 2.Kumar S, Bhargava D, Thakkar A, Arora S. Drug carrier systems for solubility enhancement of BCS class II drugs: a critical review. Crit Rev Ther Drug Carrier Syst. 2013;30:217–256. doi: 10.1615/CritRevTherDrugCarrierSyst.2013005964. [DOI] [PubMed] [Google Scholar]
- 3.Gidwani B, Vyas A. Synthesis, characterization and application of epichlorohydrin-β-cyclodextrin polymer. Colloids Surf B Biointerfaces. 2014;114:130–137. doi: 10.1016/j.colsurfb.2013.09.035. [DOI] [PubMed] [Google Scholar]
- 4.Loftsson T, Duchêne D. Cyclodextrins and their pharmaceutical applications. Int J Pharm. 2007;329:1–11. doi: 10.1016/j.ijpharm.2006.10.044. [DOI] [PubMed] [Google Scholar]
- 5.Tiwari G, Tiwari R, Rai AK. Cyclodextrins in delivery systems: applications. J Pharm Bioallied Sci. 2010;2:72–79. doi: 10.4103/0975-7406.67003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Murtaza G, Khan SA, Najam-ul-Haq M, Hussain I. Comparative evaluation of various solubility enhancement strategies for furosemide. Pak J Pharm Sci. 2014;27:963–973. [PubMed] [Google Scholar]
- 7.Semalty M, Panchpuri M, Singh D, Semalty A. Cyclodextrin inclusion complex of racecadotril: effect of drug-β-cyclodextrin ratio and the method of complexation. Curr Drug Discov Technol. 2014;11:154–161. doi: 10.2174/15701638113106660043. [DOI] [PubMed] [Google Scholar]
- 8.Loftsson T, Vogensen SB, Brewster ME, Konrádsdóttir F. Effects of cyclodextrins on drug delivery through biological membranes. J Pharm Sci. 2007;96(10):2532–2546. doi: 10.1002/jps.20992. [DOI] [PubMed] [Google Scholar]
- 9.Vecsernyés M, Fenyvesi F, Bácskay I, et al. Cyclodextrins, blood-brain barrier, and treatment of neurological diseases. Arch Med Res. 2014;45:711–729. doi: 10.1016/j.arcmed.2014.11.020. [DOI] [PubMed] [Google Scholar]
- 10.Pinho E, Grootveld M, Soares G, Henriques M. Cyclodextrins as encapsulation agents for plant bioactive compounds. Carbohydr Polym. 2014;101:121–135. doi: 10.1016/j.carbpol.2013.08.078. [DOI] [PubMed] [Google Scholar]
- 11.Hanumegowda UM, Wu Y, Adams SP. Potential impact of cyclodextrin-containing formulations in toxicity evaluation of novel compounds in early drug discovery. J Pharm Pharmacol. 2014;2(1):5. [Google Scholar]
- 12.Stutchbury TK, Vine KL, Locke JM, Chrisp JS, Bremner JB, Clingan PR, et al. Preclinical evaluation of novel, all-in-one formulations of 5-fluorouracil and folinic acid with reduced toxicity profiles. Anticancer Drugs. 2011;22(1):24–34. doi: 10.1097/CAD.0b013e32833f6d22. [DOI] [PubMed] [Google Scholar]
- 13.Nagarsenker MS, Meshram RN, Ramprakash G. Solid dispersion of hydroxypropyl beta-cyclodextrin and ketorolac: enhancement of in-vitro dissolution rates, improvement in anti-inflammatory activity and reduction in ulcerogenicity in rats. J Pharm Pharmacol. 2000;52(8):949–956. doi: 10.1211/0022357001774831. [DOI] [PubMed] [Google Scholar]
- 14.Otero Espinar FJ, Anguiano Igea S, Blanco Medez J, Vila Jato JL. Reduction in the ulcerogenicity of naproxen by complexation with β-cyclodextrin. Int J Pharm. 1991;70:35–41. doi: 10.1016/0378-5173(91)90161-G. [DOI] [Google Scholar]
- 15.Koutsou GA, Storey DM, Bär A. Gastrointestinal tolerance of gamma-cyclodextrin in humans. Food Addit Contam. 1999;16:313–317. doi: 10.1080/026520399283984. [DOI] [PubMed] [Google Scholar]
- 16.Stella VJ, He Q. Cyclodextrins. Toxicol Pathol. 2008;36:30–42. doi: 10.1177/0192623307310945. [DOI] [PubMed] [Google Scholar]
- 17.Capuano A, Parretta E. Farmaci dell’infiammazione. In: Rossi F, Cuomo V, Riccardi C, editors. Farmacologia per le professioni sanitarie. 1. Torino: Edizione Minerva Medica; 2014. [Google Scholar]
- 18.Smith FG, Wade AW, Lewis ML, Qi W. Cyclooxygenase (COX) inhibitors and the newborn kidney. Pharmaceuticals (Basel). 2012;5:1160–1176. doi: 10.3390/ph5111160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mazzotti A, Chiarello E, Tedesco G, et al. Utilizzo del diclofenac idrossipropil-β-ciclodestrina nella gestione del dolore post-operatorio in pazienti trattati per chirurgia minore dell’arto inferiore. G Ital Ortop Traumatolog. 2015;41:30–35. Available at: http://www.giot.it/wp-content/uploads/2015/05/GIOT_1-2015.pdf. Accessed 14 Jan 2016.
- 20.Prettyman J. Subcutaneous or intramuscular? Confronting a parenteral administration dilemma. Medsurg Nurs. 2005;14(2):93–8 (quiz 99). [PubMed]
- 21.Unzueta A, Vargas HE. Nonsteroidal anti-inflammatory drug-induced hepatoxicity. Clin Liver Dis. 2013;17:643–656. doi: 10.1016/j.cld.2013.07.009. [DOI] [PubMed] [Google Scholar]
- 22.Scarpignato C. Piroxicam-β-cyclodextrin: a GI safer piroxicam. Curr Med Chem. 2013;20:2415–2437. doi: 10.2174/09298673113209990115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Carr DB, McDonnell Moorehead T, Bouchard A, et al. Effects of injectable HPβCD-diclofenac on the human delayed rectifier potassium channel current in vitro and on proarrhythmic QTc in vivo. Clin Ther. 2013;35:646–658. doi: 10.1016/j.clinthera.2013.03.014. [DOI] [PubMed] [Google Scholar]
- 24.Pavelka K. A comparison of the therapeutic efficacy of diclofenac in osteoarthritis: a systematic review of randomized controlled trial. Curr Med Res Opin. 2012;28:172–178. doi: 10.1185/03007995.2011.649848. [DOI] [PubMed] [Google Scholar]
- 25.The Medicines Utilization Monitoring Centre. National report on medicine use in Italy 2013. Rome: Italian Medicines Agency; 2014. Available at: http://www.agenziafarmaco.gov.it/sites/default/files/Rapporto_OsMED_2013.pdf. Accessed 14 Jan 2016.
- 26.Gan TJ. Diclofenac: an update on its mechanism of action and safety profile. Curr Med Res Opin. 2010;26:1715–1731. doi: 10.1185/03007995.2010.486301. [DOI] [PubMed] [Google Scholar]
- 27.Iraji F, Siadat AH, Asilian A, et al. The safety of diclofenac for the management and treatment of actinic keratoses. Expert Opin Drug Saf. 2008;7:167–172. doi: 10.1517/14740338.7.2.167. [DOI] [PubMed] [Google Scholar]
- 28.Castellsague J, Riera-Guardia N, Calingaert B, et al. Individual NSAIDs and upper gastrointestinal complications: a systematic review and meta-analysis of observational studies (the SOS project) Drug Saf. 2012;35:1127–1146. doi: 10.1007/BF03261999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Gagnier P. Review of the safety of diclofenac/misoprostol. Drugs. 1993;45(Suppl 1):31–35. doi: 10.2165/00003495-199300451-00008. [DOI] [PubMed] [Google Scholar]
- 30.Assessment report for non-steroidal anti-inflammatory drugs (NSAIDs) and cardiovascular risk. Review under article 5(3) of Regulation (EC) No 726/2004. Procedure no: EMEA/H/A-5(3)/1319. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/Report/2012/11/WC500134717.pdf. Accessed 14 Jan 2016.
- 31.Dias MM, Raghavan SL, Pellett MA, Hadgraft J. The effect of beta-cyclodextrins on the permeation of diclofenac from supersaturated solutions. Int J Pharm. 2003;263:173–181. doi: 10.1016/S0378-5173(03)00366-1. [DOI] [PubMed] [Google Scholar]
- 32.Zeitlinger M, Rusca A, Oraha AZ, et al. Pharmacokinetics of a new diclofenac sodium formulation developed for subcutaneous and intramuscular administration. Int J Clin Pharmacol Ther. 2012;50:383–390. doi: 10.5414/CP201600. [DOI] [PubMed] [Google Scholar]
- 33.Salomone S, Piazza C, Vitale DC, et al. Pharmacokinetics of a new subcutaneous diclofenac formulation administered to three body sites: quadriceps, gluteus, and abdomen. Int J Clin Pharmacol Ther. 2014;52:129–134. doi: 10.5414/CP201963. [DOI] [PubMed] [Google Scholar]
- 34.Mermelstein F, Hamilton DA, Wright C, et al. Single-dose and multiple-dose pharmacokinetics and dose proportionality of intravenous and intramuscular HPβCD-diclofenac (Dyloject) compared with other diclofenac formulations. Pharmacotherapy. 2013;33:1012–1021. doi: 10.1002/phar.1304. [DOI] [PubMed] [Google Scholar]
- 35.Dietrich T, Leeson R, Gugliotta B, Petersen B. Efficacy and safety of low dose subcutaneous diclofenac in the management of acute pain: a randomized double-blind trial. Pain Pract. 2014;14:315–323. doi: 10.1111/papr.12082. [DOI] [PubMed] [Google Scholar]
- 36.Leeson RM, Harrison S, Ernst CC, et al. Dyloject, a novel injectable diclofenac formulation, offers greater safety and efficacy than voltarol for postoperative dental pain. Reg Anesth Pain Med. 2007;32:303–310. doi: 10.1097/00115550-200707000-00006. [DOI] [PubMed] [Google Scholar]
- 37.Chiarello E, Bernasconi S, Gugliotta B, Giannini S. Subcutaneous injection of diclofenac for the treatment of pain following minor orthopedic surgery (DIRECT study): a randomized trial. Pain Pract. 2015;15:31–39. doi: 10.1111/papr.12140. [DOI] [PubMed] [Google Scholar]
- 38.Gan TJ, Daniels SE, Singla N, et al. A novel injectable formulation of diclofenac compared with intravenous ketorolac or placebo for acute moderate-to-severe pain after abdominal or pelvic surgery: a multicenter, double-blind, randomized, multiple-dose study. Anesth Analg. 2012;115:1212–1220. doi: 10.1213/ANE.0b013e3182691bf9. [DOI] [PubMed] [Google Scholar]
- 39.Christensen K, Daniels S, Bandy D, et al. A double-blind placebo-controlled comparison of a novel formulation of intravenous diclofenac and ketorolac for postoperative third molar extraction pain. Anesth Prog. 2011;58:73–81. doi: 10.2344/0003-3006-58.2.73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Daniels S, Melson T, Hamilton DA, et al. Analgesic efficacy and safety of a novel injectable formulation of diclofenac compared with intravenous ketorolac and placebo after orthopedic surgery: a multicenter, randomized, double-blinded, multiple-dose trial. Clin J Pain. 2013;29:655–663. doi: 10.1097/AJP.0b013e318270f957. [DOI] [PubMed] [Google Scholar]
- 41.Chelly JE, Singla SK, Melson TI, et al. Safety of a novel parenteral formulation of diclofenac after major orthopedic or abdominal/pelvic surgery in a population including anticoagulated, elderly or enally insufficient patients: an open-label, multiday, repeated dose clinical trial. Pain Med. 2013;14:749–761. doi: 10.1111/pme.12076. [DOI] [PubMed] [Google Scholar]
- 42.Canonico PL, Schettini G. Ormoni e farmaci del sistema endocrino. In: Rossi F, Cuomo V, Riccardi C, editors. Farmacologia—principi di base e applicazioni terapeutiche. 1. Torino: Edizione Minerva Medica; 2005. [Google Scholar]
- 43.DeMayo FJ, Zhao B, Takamoto N, Tsai SY. Mechanisms of action of estrogen and progesterone. Ann N Y Acad Sci. 2002;955:48–59 (discussion 86–8, 396–406). [DOI] [PubMed]
- 44.Benagiano G, Primiero FM, Farris M. Clinical profile of contraceptive progestins. Eur J Contracept Reprod Health Care. 2004;9:182–193. doi: 10.1080/13625180400007736. [DOI] [PubMed] [Google Scholar]
- 45.Prontogest® (IBSA Farmaceutici Italia). Summary of product characteristics. Available at: https://farmaci.agenziafarmaco.gov.it/aifa/servlet/PdfDownloadServlet?pdfFileName=footer_007166_005239_RCP.pdf&retry=0&sys=m0b1l3. Accessed 14 Jan 2016.
- 46.Antela® (Farmitalia Industria Chimico Farmaceutica). Summary of product characteristics. Available at: https://farmaci.agenziafarmaco.gov.it/aifa/servlet/PdfDownloadServlet?pdfFileName=footer_000959_040389_RCP.pdf&retry=0&sys=m0b1l3. Accessed 14 Jan 2016.
- 47.Levy T, Yairi Y, Bar-Hava I, et al. Pharmacokinetics of the progesterone-containing vaginal tablet and its use in assisted reproduction. Steroids. 2000;65:645–649. doi: 10.1016/S0039-128X(00)00121-5. [DOI] [PubMed] [Google Scholar]
- 48.Lentogest® (IBSA Farmaceutici Italia). Riassunto delle Caratteristiche del Prodotto. Available at: https://farmaci.agenziafarmaco.gov.it/aifa/servlet/PdfDownloadServlet?pdfFileName=footer_007166_024542_RCP.pdf&retry=0&sys=m0b1l3. Accessed 14 Jan 2016.
- 49.Berrino F, Campagnoli C, Veronesi U. Progesterone, progestinici e rischio di cancro mammario nella terapia ormonale sostitutiva. Available at: https://www.progettoasco.it/riviste/rivista_simg/2005/04_2005/8.pdf. Accessed 14 Jan 2016.
- 50.Diep CH, Daniel AR, Mauro LJ, Knutson TP, Lange CA. Progesterone action in breast, uterine, and ovarian cancers. J Mol Endocrinol. 2015;54:R31–R53. doi: 10.1530/JME-14-0252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Nandi I, Bateson M, Bari M, Joshi HN. Synergistic effect of PEG-400 and cyclodextrin to enhance solubility of progesterone. AAPS PharmSciTech. 2003;4:E1. doi: 10.1208/pt040101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Dahan A, Miller JM, Hoffman A, et al. The solubility-permeability interplay in using cyclodextrins as pharmaceutical solubilizers: mechanistic modeling and application to progesterone. J Pharm Sci. 2010;99:2739–2749. doi: 10.1002/jps.22033. [DOI] [PubMed] [Google Scholar]
- 53.Lahiani-Skiba M, Barbot C, Bounoure F, et al. Solubility and dissolution rate of progesterone-cyclodextrin-polymer systems. Drug Dev Ind Pharm. 2006;32:1043–1058. doi: 10.1080/03639040600897093. [DOI] [PubMed] [Google Scholar]
- 54.Ragab DM, Rohani S, Consta S. Controlled release of 5-fluorouracil and progesterone from magnetic nanoaggregates. Int J Nanomedicine. 2012;7:3167–3189. doi: 10.2147/IJN.S30190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Patil A, Swamy G, Murtha A, Heine RP, Grotegut C. Comparative efficacy of water-soluble progesterone vs traditional progesterone formulation on uterine contractility. Am J Obste Gynecol. 2015;212(1 Suppl):S304. Available at: http://www.ajog.org/article/S0002-9378(14)01873-0/pdf. Accessed 14 Jan 2016.
- 56.Public assessment report: decentralised procedure. Lubion 25 mg powder for solution for injection; Lubion 25 mg solution for injection. Progesterone. UK/H/4170/001-02/DC. Available at: http://www.mhra.gov.uk/home/groups/par/documents/websiteresources/con270678.pdf. Accessed 14 Jan 2016.
- 57.Sator M, Radicioni M, Cometti B, et al. Pharmacokinetics and safety profile of a novel progesterone aqueous formulation administered by the s.c. route. Gynecol Endocrinol. 2013;29:205–208. doi: 10.3109/09513590.2012.736560. [DOI] [PubMed] [Google Scholar]
- 58.Lockwood G, Griesinger G. Cometti B; 13 European Centers. Subcutaneous progesterone versus vaginal progesterone gel for luteal phase support in in vitro fertilization: a noninferiority randomized controlled study. Fertil Steril. 2014;101:112–119. doi: 10.1016/j.fertnstert.2013.09.010. [DOI] [PubMed] [Google Scholar]
- 59.Baker VL, Jones CA, Doody K, et al. A randomized, controlled trial comparing the efficacy and safety of aqueous subcutaneous progesterone with vaginal progesterone for luteal phase support of in vitro fertilization. Hum Reprod. 2014;29:2212–2220. doi: 10.1093/humrep/deu194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.European Medicines Agency. Background review for cyclodextrins used as excipients. EMA/CHMP333892/2013. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/Report/2014/12/WC500177936.pdf. Accessed 14 Jan 2016.
- 61.Colucci RD, Wright C, IV, Mermelstein FH, Gawarecki DG, Carr DB. Dyloject®, a novel injectable diclofenac solubilised with cyclodextrin: reduced incidence of thrombophlebitis compared to injectable diclofenac solubilised with polyethylene glycol and benzyl alcohol. Acute Pain. 2009;11:15–21. doi: 10.1016/j.acpain.2008.11.001. [DOI] [Google Scholar]
- 62.Rasheed A, Ashok Kumar CK, Sravanthi VV. Cyclodextrins as drug carrier molecule: a review. Sci Pharm. 2008;76:567–598. doi: 10.3797/scipharm.0808-05. [DOI] [Google Scholar]
- 63.Martin Del Valle EM. Cyclodextrins and their uses: a review. Process Biochem. 2004;39:1033–1046. doi: 10.1016/S0032-9592(03)00258-9. [DOI] [Google Scholar]
- 64.Higuchi T, Connors KA. Phase-solubility techniques. Adv Anal Chem Instrum. 1965;4:117–212. [Google Scholar]