

Abstract
Background:
Unwanted pregnancy induces adverse attitudes regarding pregnancy which is a natural event by increasing mental and socio-economic difficulties. Insufficient maternal care and low adjustment to parental role are known as consequences of unwanted pregnancy. Perceived social support and self-efficacy in pregnancy influence health related behaviors and may play a crucial role in adaptation to pregnancy; this study was conducted to examine and compare the self-efficacy and social support among two groups of women with wanted and unwanted pregnancy.
Methods:
This analytical descriptive research was conducted on 315 women referred to 13 health centers in the east and west of Ahvaz in 2011. Data were collected via random stratified sampling method through interview. The instrument of this study was a questionnaire in three distinct parts including demographic, modified Persian version of Vaux General social support (Chronbach`s alpha =0.80) and Persian version of self-efficacy scale (Chronbach`s alpha =0.80). Data were analyzed through independent t-test and ANOVA. A P<0.05 was considered significant.
Results:
The mean age of the subjects was 25.8±5.6; unwanted pregnancy occurred in 135 women (42.2%). The mean scores of social support in the two given groups with wanted and unwanted pregnancy were 26.62±4.16 and 22.28±7.57, respectively (P<0.001). Furthermore, the mean scores of self-efficacy for the wanted pregnancy group was 37.77±6.66 and for unwanted pregnancy group it was 31.03±6.31 (P<0.001). Women and their husbands’ age, the number of male offspring in family and marriage years were significantly different in the two groups (P<0.05).
Conclusion:
This study showed that unwanted pregnant women are more likely to be exposed to low level of perceived social support and self-efficacy. Therefore more studies and interventions are recommended to be conducted to analyze the effect of family and friends’ supports on unwanted pregnant women’s perceived social support and self-efficacy and its adverse consequences.
KEYWORDS: Social support, Self-efficacy, Unwanted pregnancy
INTRODUCTION
Pregnancy can be such a pleasant event for couples in marriage life; however, it is sometimes an undesirable experience. Unwanted pregnancy is a type of pregnancy in which at least one of the couples is not pleased to happen.1 There are different reports for unwanted pregnancy rate around the world. In countries like Bangladesh and Indonesia, it is about 30%2 and 17%,3 respectively. Unwanted pregnancy is common in Iran; according to a systematic review study in Iran, the average rate of unwanted pregnancy is 30.6%;4 furthermore, other studies conducted in different regions and provinces of Iran addressed a range of 8-32% of unwanted pregnancy rate.5 In Ahvaz where situated in the southwest of Iran, prevalence of unwanted pregnancy is 26% according to a study result.6
Abortion is one of the adverse outcomes of unwanted pregnancies. Among 200 million pregnancies around the world, about one-third are unwanted; approximately 50 million of these unwanted pregnancies will lead to abortion to finish this period earlier. Twenty millions of these abortions are unsafe and take place in unhealthy condition.4 Unsafe abortions are responsible for approximately one in seven maternal deaths and five million women hospitalized in the developing countries estimated annually.7
Available evidences have proved that unwanted pregnancies have some undesirable side effects for maternal and children health; it effects the maternal care during pregnancy. These pregnancies also have adverse effects regarding the mother’s mental health such as fear, depression, and anxiety.8 It might cause negative attitudes about pregnancy and postpone or damage the parental role complementary process gradually.1 Having put millions of women and children’s health in risk, unwanted pregnancy is such a difficulty for families and even public and social health.2
Several studies have reported that pregnancy acceptance in social point of view is significantly driven from superior social support, self-efficacy and commitment to pregnancy.9 Social support could play an important role in healthy behavior, lifestyle and habits during pregnancy.10 However, this is probably not the same in unwanted pregnancy as there is more likelihood of facing socio-psycho stressors. These stressors may diminish the couple’s social support for each other leading to depression and low level of life satisfaction.11 Women with unwanted pregnancy may receive low level of social support.12 Social support as a multidimensional concept which is a social fact initiates from a person’s perception. Perceived social support reflects the people’s thought about provided support. It is one of the crucial emotion-focused coping strategies that can affect the life potentially.13 Researchers have revealed that providing social support to women leads to life quality improvement and mental health promotion.14 It could be a buffer in stressful life events of pregnant women and have a potential supportive factor in their mental health.10 Thus, studying social support of pregnant women with unwanted pregnancy may be effective efforts in guiding the proper interventions. Pregnant women not only need to understand social support, but also should understand their capability for pregnancy and adaptation to new circumstances.
Self-efficacy plays an important role in maternal transition into motherhood.15 It is based on theidea that one thinks s/he is able to organize events in order to reach self-desirable situation through proper manners and behaviors.16 When people with low level of self-efficacy face difficulties, they easily become convinced that their behavior is inefficient and stop trying their best. However, those with high self-efficacy pass difficulties with no trouble due to their skills and management; they aim to achieve during their lives resulting in better behavioral outcome compared to people with low level of self-efficacy.17
If a pregnant woman does not receive support well, not only will she experience low maternal parental self-efficacy, but the well-being of both the mother and her child may be affected. Hence, to improve the maternal and child health, it is significant to understand the influencing factors.15,18
As self-efficacy is a component to help understanding people’s behavior17 and to maintain heath promotional behaviors19 and due to social support roles in healthy positive behaviors during pregnancy,20 more scientific-based studies are needed to determine the level of taking advantage of these two components among wanted and unwanted pregnant women. Thus, in regard to high prevalence of unintended pregnancy in Ahvaz, this study aimed to compare the level of both self-efficacy and social support among two groups of wanted and unwanted pregnancies in Ahvaz.
MATERIAL AND METHODS
It was a descriptive analytical cross-sectional study which was conducted on pregnant women living in Ahvaz in 2011. This research was funded by Ahvaz Jundishapur University of Medical Sciences under ethical Code: SDH-9206, 89s191. Based on unwanted pregnancy rate (P=0.26) reported in similar studies,21 sample size was calculated as 296 subjects (α=0.05, d=0.05) and due to 10% missing prediction, 325 cases were enrolled.
Heath centers were selected by randomized stratified sampling method and13 health centers of Ahvaz (6 in west and 7 in East) were chosen. According to our sampling criteria study, the subjects were15-49 year old pregnant women who were attending these selective centers. They filled formal consent forms. The subjects were chosen by using easy access sampling method in an equal proportion and 315 women participated in the study. Women who had no consent to complete all parts of the questionnaire were excluded. To observe the research ethics, we took the approval of the ethics committee, cared about data confidentiality and filled written consent forms.
To gather the data, after training data collectors on how to use the study tool, valid questionnaires were completed through interview. Sampling started in July and lasted by the end of November. The questionnaire had three main parts: demographic and obstetrical history, social support and self-efficacy sections. The first part included demographic characteristics and obstetrics history questions such as the age, education level, spouse’s job, number of pregnancy, sex and number of live birth, number of unwanted pregnancy, and if the current pregnancy was unwanted. Unwanted pregnancy including unplanned pregnancies have been defined as the status that a woman, her couple or both are reluctance to have a new baby. In the second part of the questionnaire, there were questions regarding social support to measure the perceived general social support. The original tool have been developed by Vaux et al. (1991)22 and then translated and validated into Farsi by Ebrahimi Ghavam.23 The original edition’s conceptual framework was based on Cobb`s definition of social support (1976)24 including 23-item 4-point likert scale from strongly agree to strongly disagree in 3 domains of family (8 questions), friends (8questions), and others (7questions). In the Farsi version, the scoring system was changed into dichotomous scale (Cronbach’s alpha=0.90). In case a question was opposite the social support, scores were calculated in adverse way; that is, we put score 0 and 1 for yes and no response, respectively.23 Nine specific questions about social support in pregnancy period were added to the initial questions based on the women’s view with pregnancy experience. In order to assess the reliability and validity of the questionnaire, panel of seven experts was formed including Health education and promotion experts (2 persons), Midwifery and obstetrics experts (2 persons), prenatal care providers (2 individuals) and statistician (1 person). In this stage, Cronbach’s alpha of the questionnaire was 0.80, which proved to have an acceptable reliability. In the third part, general self-efficacy scale was used which was based on Bandura’s Self-efficacy Theory (1977)16 and has been translated and validated by Nezami and colleagues in 199625 including 10 items scored from 1 to 5 ranging from “I totally agree” to “totally disagree”, respectively. The total obtained score from each item was calculated between 1 and 5 and the total added scores was obtained as each woman’s self-efficacy. The value of Cronbach’s alpha for Farsi version self-efficacy questionnaire was 0.80. To analyze the collected data, normality of data was checked using Kolmogorov Smirnov test. Then, analysis of variances and t-tests (P<0.05) were used through SPSS version 16.
RESULTS
This study aimed to compare the level of social support and self-efficacy among 315 cases categorized into two distinct groups of women with wanted and unwanted pregnancy who referred to Ahvaz Health centers. Their mean age was 25.8±5.6; the youngest case was 15and the oldest one was 45 years old. 14.6% (N=46) and 5.1 %(N=16) were under 20 and more than 35, respectively. More than half of the cases (58.4%, N=184) were diploma or higher and only 13% (N=41) were employed.
The mean age of samples’ spouse was 29.38±6.71 and self-employment was their most frequent job (53.3% N=168); their education level was mainly in diploma level and higher (46.4%, N=146). The mean duration between their marriage and first birth and mean birth spacing between their two last pregnancies were 63.67±60.8 and 23.3±31.8 (months), respectively. Pregnancy was unwanted in 42.2% (N=135) of the cases; in 76.3% (N=103) of the unwanted pregnancies, there were no interest in having a baby in both couples. In 5.2% (N=7) of them only the women liked to have a baby and in 18.5% (N=25) of the cases husbands preferred to become father and have a baby. First pregnancy was reported in 41.6% (N=131) of the subjects. Having enough number of offspring was mentioned as the most frequent reason of assigning their pregnancy as an unwanted one in 38 cases (28.1%). Having young children (19.3%, N=26), low level income (23.7%, N=32), unsuitable accommodation and facilities (17%, N=22) and physical appearance (11.9%, N=13) were the other mentioned reasons.
The result of independent t-test (table 1) indicated a significant difference between the mean of social support and self-efficacy scores of the two groups including wanted and unwanted pregnant women(P<0.001).
Table 1.
Comparison of mean and other related quantitative measures of wanted and unwanted pregnancies among two groups of pregnant women
| Variables | Pregnancy Type | No. | Mean±SD | Independent t test |
|---|---|---|---|---|
| Social support | W* | 180 | 26.6167±4.15923 | P<0.001 |
| UW** | 135 | 22.2815±7.57416 | ||
| Self-efficacy | W | 180 | 37.7722±6.66084 | P<0.001 |
| UW | 135 | 31.0296±8.31555 | ||
| Women Age | W | 180 | 24.8000±4.90627 | P<0.004 |
| UW | 135 | 26.5037±5.68957 | ||
| Husband Age | W | 180 | 28.7222±6.21321 | P<0.03 |
| UW | 135 | 30.2667±7.26081 | ||
| Marriage length (month) | W | 180 | 44.3833±42.35132 | P<0.001 |
| UW | 135 | 89.4000±71.57954 | ||
| No. of people in family | W | 180 | 3.2056±1.72299 | P<0.001 |
| UW | 135 | 4.2815±2.00615 | ||
| Distance of marriage to the first pregnancy (month) | W | 180 | 16.5056±19.71770 | P<0.04 |
| UW | 135 | 10.0074±13.17534 | ||
| Distance of last two pregnancies (month) | W | 180 | 16.6333±28.78390 | P<0.04 |
| UW | 135 | 32.2963±32.11130 | ||
| No. of son in family | W | 180 | 0.2556±0.48580 | P<0.001 |
| UW | 135 | 0.8148±0.83026 | ||
| No. of pregnancies | W | 180 | 1.5389±0.76490 | P<0.001 |
| UW | 135 | 2.9704±1.52071 | ||
| No. of alive children | W | 180 | 0.4500±0.67910 | P<0.001 |
| UW | 135 | 1.6444±1.37389 | ||
| No. of UW ever | W | 180 | 0.000±0.000 | P<0.001 |
| UW | 135 | 1.2222±0.45164 |
W=Wanted pregnancy;
UW=Unwanted pregnancy; P<0.05 is significant; Independent T test was used
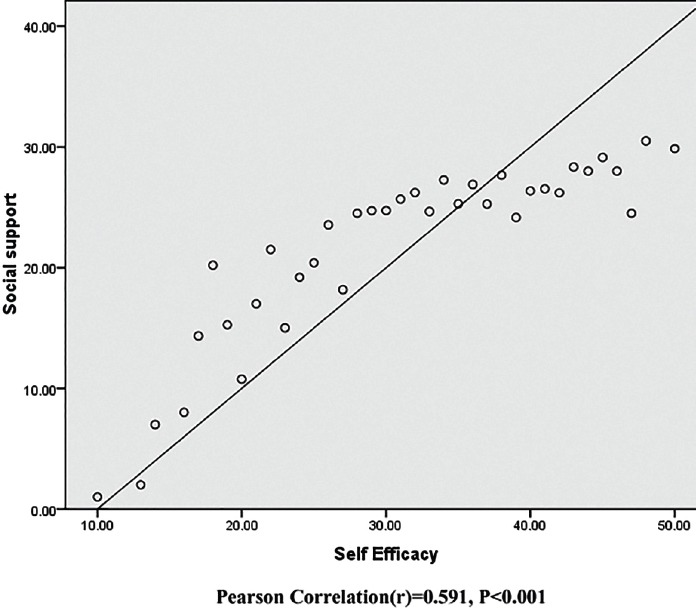
Furthermore, the results of variance analysis in the two above-mentioned groups revealed discrepancy of self-efficacy mean score between the two groups based on their education level, women’s jobs, and spouses’ job subgroups (P<0.05); table 2 shows more details. The result of independent t-test revealed a significant difference in self-efficacy of the two groups of employed and housekeepers wanted and unwanted pregnant women (wanted: t=-4.055- P<001, unwanted: t=-2.805 P<0.005). Moreover, independent t-test addressed the difference of social support means score in both wanted and unwanted pregnant women based on some women’s and their husbands’ personal factors (P<0.05). Similar to other listed variables in table 3, women’s perceived social support score in the two groups was significantly different based on their education and job and their husbands’ job and education level (P<0.005). There was a significant correlation (r=0.591, P<0.001) between social support and self-efficacy among pregnant women (figure 1).
Table 2.
The comparison of mean of self-efficacy score among different groups based on quantitative variables
| Variables | Self-efficacy | ||||||
|---|---|---|---|---|---|---|---|
| Unwanted | Wanted | ||||||
| N (%) | mean±SD | Sig | N (%) | mean±SD | Sig | ||
| Women education level | Illiterate and primary | 40 (29.63) | 26.300±8.933 | P<0.001 | 15 (8.33) | 30.53±6.534 | P<0.001 |
| Secondary school | 37 (27/4) | 30.0541±8.359 | 39 (21.67) | 37.43±6.137 | |||
| Diploma | 45 (33.3) | 34.8000±5.837 | 81 (45) | 37.308±5.444 | |||
| Academic | 13 (9.62) | 35.307±5.250 | 45 (25) | 41.31±7.022 | |||
| Husband education level | Illiterate and primary | 37 (27.4) | 25.864±9.321 | P<0.001 | 19 (10.56) | 32.789±7.307 | P<0.001 |
| Secondary school | 54 (40) | 31.518±6.976 | 59 (32.77) | 38.050±5.928 | |||
| Diploma | 27 (20) | 33.777±7.148 | 70 (38.88) | 37.085±6.310 | |||
| Academic | 17 (12.6) | 36.352±5.803 | 32 (17.77) | 41.718±6.186 | |||
| Women job | Housewife | 121 (89.6) | 30.363±8.310 | *P=0.006 | 153 (85) | 36.96±6.360 | P<0.001 |
| Employee | 14 (10.4) | 36.785±5.950 | 27 (15) | 42.37±6.564 | |||
| Husband job | Worker | 39 (28.9) | 29.436±8.518 | P<0.001 | 41 (22.78) | 35.439±6.877 | P=0.004 |
| Employee | 18 (13.3) | 36.278±7.185 | 32 (17.78) | 40.937±6.676 | |||
| Business | 70 (51.7) | 31.414±7.715 | 98 (54.44) | 37.898±6.266 | |||
| Unemployed | 8 (5.9) | 23.625±8.279 | 9 (5) | 35.777±5.890 | |||
P<0.05 is significant; Statistical Test is Analysis Variance;
Independent t-test
Table 3.
The comparison of mean of social support score among different groups based on quantitative variables
| Variables | Social support | ||||||
|---|---|---|---|---|---|---|---|
| Wanted | Unwanted | ||||||
| N (%) | mean±SD | Test Sig. | N (%) | mean±SD | Test Sig. | ||
| Women education level | Illiterate and primary | 40 (29.63) | 18.525±9.800 | P=0.005 | 15 (8.33) | 25.13±5.792 | P<0.001 |
| Guidance school | 37 (27.4) | 22.351±6.129 | 39 (21.67) | 25.82±3.803 | |||
| Diploma | 45 (33.3) | 24.155±5.414 | 81 (45) | 26.135±4.155 | |||
| academic | 13 (9.62) | 27.153±4.723 | 45 (25) | 28.666±3.126 | |||
| Husband education level | Illiterate and primary | 37 (27.4) | 17.378±10.166 | P<0.001 | 19 (10.56) | 25.779±4.043 | P=0.024 |
| Guidance school | 54 (40) | 22.944±5.608 | 59 (32.77) | 26.315±5.164 | |||
| Diploma | 27 (20) | 24.740±5. 027 | 70 (38.88) | 26.528±4.07 | |||
| academic | 17 (12.6) | 26.941±3.508 | 32 (17.77) | 28.531±3.426 | |||
| Women job | Housewife | 121 (89.6) | 21.686±7.693 | *P=0.007 | 153 (85) | 26.222±4.166 | *P=0.002 |
| Employee | 14 (10.4) | 27.428±3.631 | 27 (15) | 28.851±3.393 | |||
| Husband job | Worker | 39 (28.9) | 21.410±7.9.147 | P=0.004 | 41 (22.78) | 25.170±4.403 | P=0.002 |
| Employee | 18 (13.3) | 28.833±3.698 | 32 (17.78) | 28.187±3.031 | |||
| Business | 70 (51.7) | 22.347±6.762 | 98 (54.44) | 26.969±4.082 | |||
| Unemployed | 8 (5.9) | 15.750±7.324 | 9 (5) | 23.777±4.603 | |||
P<0.05 is significant; Statistical Test is Analysis Variance;
Independent t-test
Figure 1.
Scatter Dot of the social support and self-efficacy among pregnant women
DISCUSSION
The major aim of this study was to compare the perceived social support and self-efficacy in two distinct groups of wanted and unwanted pregnant women in Ahvaz. Results revealed that there was a lower level of perceived social support in unwanted pregnant cases compared to wanted pregnant women. According to the results of the study conducted in Dorham among 1321 pregnant women, the lowest scores of self-efficacy and social support were reported in unwanted pregnant women.12 In Ethiopia, it has been proved that unwanted pregnant women take a low level of support from their partner.11 Other studies have reported that unwanted pregnancies increase health risks. Also, insufficient support from the partner, family and friends during pregnancy in addition to undergoing abortion expose them to physical and mental problems10,26,27 such as psychological disorders (anxiety and depression); thus, unwanted pregnancy due to low level of social support is a well-known risk factor for the couple’s mental health and social isolation.28 It is supposed that social support can play a role in buffering stress in pregnancy.29 Low level of perceived social support may influence the maternal role and health and endanger the baby’s health after delivery.30 A meta-analysis study from 48 researches showed that unplanned and unwanted pregnancy, insufficient social support and improper marital relationship might be postpartum depression risk factors.31 This indicates that there is a need to conduct more extended studies to screen high risk pregnant women and perform proper interventions and solutions.
Perceived self-efficacy of wanted and unwanted pregnant women was compared; it was found that unwanted pregnant women were more likely at the exposure of low level of perceived self-efficacy. Some researchers also obtained comparable results in their studies.12,32 These findings are inconsistent with the results of the study on primiparous women indicating that there was no association between self-efficacy and intention of parents to have a baby.33 This different result may be due to the difference between the target groups in the current study compared to the above study. However, there are a few studies conducted about unwanted pregnancy and self-efficacy both together. Research indicates that perceived social support and self-efficacy are both influential factors on women’s health.34 According to Durham’s study, unwanted pregnant women were not only in a low self-efficacy mood, but their perceived social support was lower than other pregnant cases. They were stressful and significantly depressed.12 Moreover, the present study revealed that social support and self-efficacy were significantly correlated. A study carried out about 30 minutes after abortion in women who underwent induced abortion showed that perceived social support through direct effect on self-efficacy increase may improve the women’s acceptance of unwanted pregnancy.26 Women who simply receive more advocacy and support from their partner, family and friends may have a better status to cope with this issue. In fact, the more support the unwanted pregnant cases receive, the better mental health they would enjoy.26 There are more researches to be conducted among women with unwanted pregnancy as there is an increasing trend of unwanted pregnancy prevalence in Iran and the world. For example, the prevalence of unwanted pregnancy in Ahvaz is more than two fifth of all pregnant cases. Furthermore, in Bangladesh and Ethiopia unwanted pregnancy percentages were 30% and 32%, respectively.2,11 Based on a study in the west of Iran (Kermanshah), 35.6% of the total pregnancies were unwanted and it was a risk factor for depression in Iranian women.35 In our study setting (Ahvaz), the major attributable reason to assign the type of pregnancies as unwanted might be the increase in the level of women’s education, increase in their knowledge about family planning and contraception methods, and more than two decades of family planning endeavors in the country; that is, generally people would like to have a small family.
The researcher in this study concluded that women and their partner need to receive more efficient and higher quality education about pregnancy decision making. It is also addressed that the age of women in the unwanted pregnancy group was older than the wanted pregnant women in other studies.2,6,35,36 There are some studies about social support addressing adolescents with unplanned pregnancies; however, there are a few researches in other women facing unplanned pregnancies.29
In this research, women and their spouse’s education level was related to unwanted pregnancy; as the level of education increased, there was lower number of unwanted pregnancies. It has also been proved by the results of other studies.36,37 The number of offspring was another variable to be studied; results showed a significant difference between the two wanted and unwanted pregnancy groups. Number of children in families with unwanted pregnancy was more than the wanted one; in fact, normally we label unwanted to those pregnancies in families with enough number of children and no need for a new one. As the numbers of children increase, there is higher probability of unwanted pregnancy occurrence.2,21,36
There were some limitations in the present study. First, the samples were not segmented based on the important factors such as study subjects’ socioeconomic status, disease and health condition, satisfaction of previous experiences of pregnancies and their outcomes and sexual satisfaction; this might be a limitation as social support and self-efficacy needs to be various based on different situations of this context. Furthermore, in this study both unplanned and unwanted pregnancy cases have been considered as the “unwanted pregnancy” category and not in separate classes; this might be a study limitation as these two might have different definitions.
As we pointed earlier, unwanted pregnant cases need support and advocacy. In health care centers, we might not be able to manage supports for all of the unwanted pregnant women actively. We suggest intelligent screening tools built based on predictive mathematical modeling methods to find those risky cases that are at risk of adverse effect of unwanted pregnancy and support them based on their specific situation by consultation services, friends, families, and local communities. Also, more studies and interventions are suggested to analyze the effect of family and friends’ supports growth on unwanted pregnant women’s perceived social support and self-efficacy and its adverse consequences.
CONCLUSION
According to the results of the present study, a low level of social support and self-efficacy among unwanted pregnant women is revealed. Unwanted pregnant women need to be selected as those cases who need more support by family and friends in order to raise self-efficacy, social support and welcome their new baby. These activities could reduce the load of problem and disappointments which may lead to a decrease in adverse consequences of unwanted pregnancies such as intentional abortion. Therefore, researchers have suggested more studies and interventions to increase the perceived social support and self-efficacy in women with unwanted pregnancy.
ACKNOWLEDGMENT
This research was funded by Ahvaz Jundishapur University of Medical Sciences. Special thanks go to deputy of Research and Technology, Deputy of Health and staffs at Health Centers of Ahvaz Jundishapur Medical University for their kind attention and great cooperation.
Conflict of Interest: None declared.
REFERENCES
- 1.Boroumandfar Kh, Saghafi Z, Abedi H, Bahadoran P. Unwanted pregnancy outcomes. Nursing and Midwifery Research Journal. 2010;29:25–35. [In persian] [Google Scholar]
- 2.Kamal M, Islam A. Prevalence and socioeconomic correlates of unintented pregnancy among women in rural Bangladesh. Salud Pública De México. 2011;53:108–15. doi: 10.1590/s0036-36342011000200003. [DOI] [PubMed] [Google Scholar]
- 3.Hardee K, Eggleston E, Wong EL, et al. Unintended pregnancy and women’s psychological well-being in Indonesia. Journal of Biosocial Science. 2004;36:617–26. doi: 10.1017/s0021932003006321. [DOI] [PubMed] [Google Scholar]
- 4.Moosazadeh M, Nekoei-Moghadam M, Emrani Z, Amiresmaili M. Prevalence of unwanted pregnancy in Iran: a systematic review and meta-analysis. The International Journal of Health Planning and Management. 2014;29:e277–90. doi: 10.1002/hpm.2184. [DOI] [PubMed] [Google Scholar]
- 5.Motlaq ME, Eslami M, Yazdanpanah M, Nakhaee N. Contraceptive use and unmet need for family planning in Iran. International Journal of Gynecology & Obstetrics. 2013;121:157–61. doi: 10.1016/j.ijgo.2012.11.024. [DOI] [PubMed] [Google Scholar]
- 6.Najafian M, Karami KB, Cheraghi M, Mohammad Jafari R. Prevalence of and Some Factors Relating with Unwanted Pregnancy, in Ahwaz City, Iran 2010. ISRN Obstetrics and Gynecology. 2011;2011:523430. doi: 10.5402/2011/523430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Singh S, Sedgh G, Hussain R. Unintended pregnancy: worldwide levels, trends, and outcomes. Stud Fam Plann. 2010;41:241–50. doi: 10.1111/j.1728-4465.2010.00250.x. [DOI] [PubMed] [Google Scholar]
- 8.Hayatbakhsh MR, Najman JM, Khatun M, et al. A longitudinal study of child mental health and problem behaviours at 14 years of age following unplanned pregnancy. Psychiatry research. 2011;185:200–4. doi: 10.1016/j.psychres.2010.05.019. [DOI] [PubMed] [Google Scholar]
- 9.Hui Choi WH, Lee GL, Chan CH, et al. The relationships of social support, uncertainty, self-efficacy, and commitment to prenatal psychosocial adaptation. Journal of Advanced Nursing. 2012;68:2633–45. doi: 10.1111/j.1365-2648.2012.05962.x. [DOI] [PubMed] [Google Scholar]
- 10.Elsenbruch S, Benson S, Rucke M, et al. Social support during pregnancy: effects on maternal depressive symptoms, smoking and pregnancy outcome. Human Reproduction. 2007;22:869–77. doi: 10.1093/humrep/del432. [DOI] [PubMed] [Google Scholar]
- 11.Dibaba Y, Fantahun M, Hindin MJ. The association of unwanted pregnancy and social support with depressive symptoms in pregnancy: evidence from rural Southwestern Ethiopia. BMC Pregnancy and Childbirth. 2013;13:135. doi: 10.1186/1471-2393-13-135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Maxson P, Miranda ML. Pregnancy intention, demographic differences, and psychosocial health. Journal of Women’s Health. 2011;20:1215–23. doi: 10.1089/jwh.2010.2379. [DOI] [PubMed] [Google Scholar]
- 13.Ersoy-Kart M, Güldü Ö. Vulnerability to stress, perceived social support, and coping styles among chronic hemodialysis patients. Dialysis & Transplantation. 2005;34:662–71. [Google Scholar]
- 14.Salazar LF, Wingood GM, DiClemente RJ, et al. The role of social support in the psychological well-being of African American girls who experience dating violence victimization. Violence and Victims. 2004;19:171–87. doi: 10.1891/vivi.19.2.171.64100. [DOI] [PubMed] [Google Scholar]
- 15.Shorey S, Chan SW, Chong YS, He HG. Predictors of Maternal Parental Self-Efficacy Among Primiparas in the Early Postnatal Period. Western Journal of Nursing Research. 2015;37:1604–22. doi: 10.1177/0193945914537724. [DOI] [PubMed] [Google Scholar]
- 16.Bandura A. Perceived self-efficacy in cognitive development and functioning. Educational Psychologist. 1993;28:117–48. [Google Scholar]
- 17.Bandura A. Health promotion by social cognitive means. Health Education & Behavior. 2004;31:143–64. doi: 10.1177/1090198104263660. [DOI] [PubMed] [Google Scholar]
- 18.Cheng D, Schwarz EB, Douglas E, Horon I. Unintended pregnancy and associated maternal preconception, prenatal and postpartum behaviors. Contraception. 2009;79:194–8. doi: 10.1016/j.contraception.2008.09.009. [DOI] [PubMed] [Google Scholar]
- 19.Pajares F, Urdan T. Self-efficacy beliefs of adolescents. Greenwich (US): Information Age; 2006. [Google Scholar]
- 20.Cannella BL. Mediators of the relationship between social support and positive health practices in pregnant women. Nursing Research. 2006;55:437–45. doi: 10.1097/00006199-200611000-00008. [DOI] [PubMed] [Google Scholar]
- 21.Tavafian SS, Ramezanzade F. Demographic characteristics affecting the decision of induced abortions in attending women to hospitals based on the Health Belief Model. Payesh. 2007;6:157–64. [In persian] [Google Scholar]
- 22.Vaux A, Phillips J, Holly L, et al. The social support appraisals (SS-A) scale: Studies of reliability and validity. American Journal of Community Psychology. 1986;14:195–218. [Google Scholar]
- 23.EbrahimiGhavam S. Determine of validity and correlation coefficients of three scales: locus of control, social support and social anxiety in Tehran students [Thesis] Tehran (Iran): Tehran Islamic Azad University; 1991. [In persian] [Google Scholar]
- 24.Cobb S. Social support as moderator of life stress. Psychosomatic Medicine. 1976;38:300–14. doi: 10.1097/00006842-197609000-00003. [DOI] [PubMed] [Google Scholar]
- 25.Rajabi Gh. The survey of reliability and validity of General self-efficacy scale in students of Faculty of Psychology and Education in Ahvaz Shahid Chamran University and Marvdasht Azad University. Quarterly Journal of New Thoughts on Education. 2008;2:111–22. [In persian] [Google Scholar]
- 26.Major B, Cozzarelli C, Sciacchitano AM, et al. Perceived social support, self-efficacy, and adjustment to abortion. Journal of Personality and Social Psychology. 1990;59:452–63. doi: 10.1037//0022-3514.59.3.452. [DOI] [PubMed] [Google Scholar]
- 27.Coleman PK. Abortion and mental health: quantitative synthesis and analysis of research published 1995-2009. The British Journal of Psychiatry: the Journal of Mental Science. 2011;199:180–6. doi: 10.1192/bjp.bp.110.077230. [DOI] [PubMed] [Google Scholar]
- 28.Kroelinger CD, Oths KS. Partner support and pregnancy wantedness. Birth. 2000;27:112–9. doi: 10.1046/j.1523-536x.2000.00112.x. [DOI] [PubMed] [Google Scholar]
- 29.Gray JB. The social support process in unplanned pregnancy. Journal of Communication in Healthcare. 2014;7:137–46. [Google Scholar]
- 30.Leahy-Warren P, McCarthy G, Corcoran P. First-time mothers: social support, maternal parental self-efficacy and postnatal depression. Journal of Clinical Nursing. 2012;21:388–97. doi: 10.1111/j.1365-2702.2011.03701.x. [DOI] [PubMed] [Google Scholar]
- 31.Beck CT. Predictors of postpartum depression: an update. Nurs Res. 2001;50:275–85. doi: 10.1097/00006199-200109000-00004. [DOI] [PubMed] [Google Scholar]
- 32.Zamani Alavijeh F, Nouhjah S, Kheiriat M, Haghigh zade MH. Related Factors ofUnwanted Pregnancy and Intention of Women to Continue or Terminate PregnancyBased on Health Belief Modelh. Payesh. 2012;11:877–85. [In persian] [Google Scholar]
- 33.Azmoude E, Jafarnejade F, Mazlom SR. The Predictors for Maternal Self-efficacy in Early Parenthood. Journal of Midwifery and Reproductive Health. 2015;3:368–76. [Google Scholar]
- 34.Seyedfatemi N, Salsali M, Rezaee N, Rahnavard Z. Women’s Health Concept: A Meta-Synthesis Study. Iranian Journal of Public Health. 2014;43:1335–44. [PMC free article] [PubMed] [Google Scholar]
- 35.Iranfar S, Shakeri J, Ranjbar M, et al. Is unintended pregnancy a risk factor for depression in Iranian women? East Mediterr Health J. 2005;11:618–24. [PubMed] [Google Scholar]
- 36.Calvert C, Baisley K, Doyle AM, et al. Risk factors for unplanned pregnancy among young women in Tanzania. Journal of Family Planning and Reproductive Health Care. 2013;39:e2. doi: 10.1136/jfprhc-2012-100389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Takahashi S, Tsuchiya KJ, Matsumoto K, et al. Psychosocial determinants of mistimed and unwanted pregnancy: the Hamamatsu Birth Cohort (HBC) study. Maternal and Child Health Journal. 2012;16:947–55. doi: 10.1007/s10995-011-0881-y. [DOI] [PubMed] [Google Scholar]