

Abstract
In this review, we discuss in detail our current procedure for treating craniosynostosis using multidirectional cranial distraction osteogenesis (MCDO). The MCDO method allows all phenotypes of skull deformity to be reshaped by distraction osteogenesis, except in patients who are 5 months of age or younger and patients with posterior cranial vault problems. We report the results of clinical data of 36 children with craniosynostosis who underwent MCDO between 2005 and 2014 in our institute. This method has the following benefits, such as a high flexibility of reshaping, shorter treatment period and less invasive secondary intervention. We also discuss the other distraction osteogenesis techniques that are used to treat craniosynostosis and compare them with MCDO. The preferred procedure for correction of craniosynostosis may depend on the patient's age, the extent of deformity, and the extent of correction achievable by surgery. We can arrange the combinations of various methods according to the advantage and disadvantage of each technique.
Keywords: Craniosynostosis, Distraction osteogenesis, Multidirectional cranial distraction osteogenesis, Posterior cranial vault distraction osteogenesis
INTRODUCTION
Various surgical procedures have been reported for the treatment of craniosynostosis. Early techniques included linear strip craniectomy, and in the 1960's, the more complicated total cranial remodeling was introduced. Traditional techniques in cranial vault remodeling have been the mainstream of craniosynostosis surgeries. Since the 1990's, less invasive surgical techniques have been popular, such as distraction osteogenesis procedures and endoscopic linear strip craniectomy with the molding helmet method.
Distraction osteogenesis was first applied as a treatment for facial bone deformities in 199024). Distraction osteogenesis for the treatment of craniosynostosis was applied in the late 1990's11,35), and has been accepted by many craniofacial surgeons1,3,12,17,25,26,41). This procedure is less invasive compared with the conventional cranial vault remodeling because the dissection of the dura mater is limited, which results in a shorter operation time, less bleeding, and good blood flow to the dura mater. Additionally, stress to the scalp is limited.
Distraction osteogenesis has several advantages, but is still in need of improvement. The disadvantages of this technique include a prolonged treatment period and secondary surgical intervention. The greatest disadvantage is the limitation of morphological correction because a large piece of bone is moved in a single direction36).
To address these limitations, Sugawara36) designed a completely new type of distraction system called multidirectional cranial distraction osteogenesis (MCDO) in 2003. After several steps of development, the results of clinical data of this system for the treatment of craniosynostosis were published in 201036). Since then, we have used this MCDO procedure mainly for the treatment of craniosynostosis in our institute. Derderian and Bartlett6) described that this novel method has "perhaps the most ambitious and innovative distraction concept used to treat craniosynostosis". In this review, we introduce this procedure in detail, and discuss the differences compared with other unidirectional distraction osteogenesis techniques. We also review the novel variations of distraction osteogenesis techniques for craniosynostosis surgery, particularly posterior cranial vault distraction osteogenesis.
THE MCDO PROCEDURE
Devices
The MCDO system consists of a disposable clear plastic frame, anchor pins and extension rods for fixing the frame to the cranium, traction pins for pulling the bone pieces up, a distractor fixed on the frame, and plastic flanges for protecting the holes. We use two types of plastic frames, where one covers only the anterior part of the cranium and another covers the whole cranium. We call the latter type MCDO-T, where T means total. The weight of the frame is approximately 170 g and the MCDO-T frame is approximately 250 g.
Surgical technique
Through a zigzag coronal approach, subgaleal dissection of the scalp is followed by subperiosteal dissection from 10 to 15 mm above the supraorbital rim (Fig. 1A). The temporal muscles are attached with the scalp flap. The lines of osteotomy and the points of drilling are then decided on the skull (Fig. 1B).
Fig. 1. Multidirectional cranial distraction osteogenesis (MCDO) procedure. A : Zigzag coronal incision. B : Designing the lines of osteotomy and the drilling points. C : Attachment of the template for anchor pins. D : Drilling the screw holes for anchor pins. E : Osteotomy in small rectangular pieces with an ultrasonic bone curette. F : Rectangular pieces without dural dissection. G : Fixation of traction pins. H : The heads of the traction pins and anchor pins penetrating the scalp. I : Screw of the anchor pins. J : Fixation of the frame on the anchor pins. K : The wires passing through holes in the frame. L : Fixation of the wires to the distractors.

Four or five screw holes each are drilled in the bilateral temporal bones under the guide holes of the template (Fig. 1C, D). These holes are for the anchor pins. The anchor pins are not screwed in immediately, but drilling holes for the anchor pins are needed before osteotomy to tightly fix the template and pins.
The skull is osteotomized in small rectangular pieces with an ultrasonic bone curette (Sonopet; developed by Mutoh Co. Ltd., Tokyo, Japan; distributed by Stryker Co. Ltd.) (Fig. 1E). The ultrasonic bone curette is a bone-cutting saw with a hard metal tip that vibrates at a high frequency. This useful curette facilitates safe osteotomy and is efficacious to avoid tearing the dura mater. Dissection of the dura mater from each bone piece is unnecessary, so that vascularity of the bones is left intact (Fig. 1F).
We can arrange the design of osteotomy and the number of bone pieces depending on the shape and severity of the deformity. In the case of sagittal synostosis, we first determine the design of osteotomy at the midline, and arrange the shapes of side bone fragments depending on the deformity. Our procedure of reshaping the skull includes gradual active expansion and passive contraction. During the activation periods, the bone fragments with a traction pin are pulled outward, while some of the others without traction pins move inward. The traction pins are fixed in the center of the bone pieces that are selected depending on the reshaping strategy (Fig. 1G).
After the anchor pins are secured, we close the wound with the heads of the traction pins and anchor pins penetrating the scalp (Fig. 1H). Skin closure should be performed with the appropriate absorbable sutures because they cannot be removed for approximately 40 days. The frame is then fixed on the anchor pins in the bilateral temporal bones (Fig. 1I, J). The wires secured in holes of the traction pins are passed through holes in the frame (Fig. 1K), such that the bone pieces can be pulled in the appropriate direction. Finally, the wires are fixed to the distractors that are attached on the frame (Fig. 1L).
Management after surgery
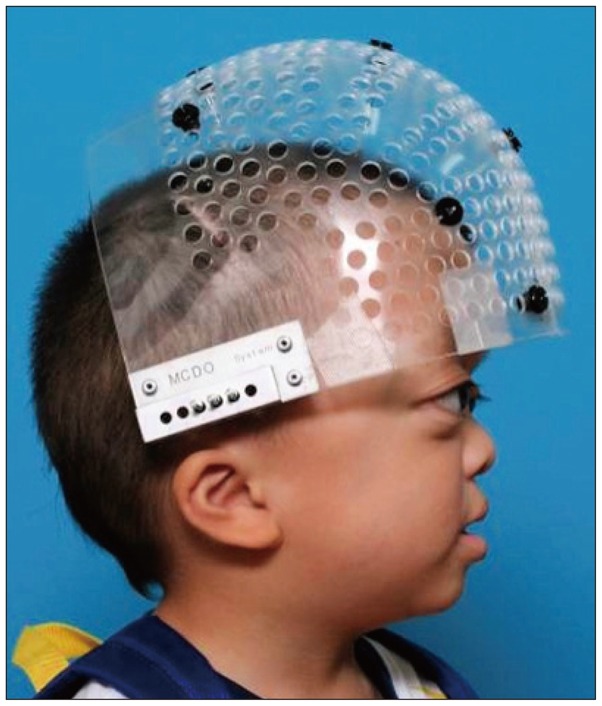
Distraction is initiated at approximately 5 days after surgery. Activating distractors enable the bones to be pulled up. At the time of first activation, the distractors need to be wound several times to strain the wire because the bone pieces are shifted outward as a result of spontaneous brain expansion during the latency periods. Distraction is activated at the rate of 1–1.5 mm per day for approximately 10 days until the desired skull shape is achieved by controlling the amount of distraction of each selected bone piece. The skull shape is easily checked by direct observation through the transparent frame. After completing the distraction, all distractors are removed and the wire ends are tied to the plastic rings on the frame to prevent loosening. Patients can lead their usual life with no limitations (Fig. 2). They can sleep without a special pillow. A handled brush is necessary for shampooing. Patients are usually discharged from hospital after activation is complete. The consolidation period is 3–4 weeks. The frame and all pins are removed in a 5-minute procedure under sedation without any incision.
Fig. 2. After completion of the distraction, all distractors were removed, and the ends of the wires were tied onto the plastic rings to prevent loosening.
We show a case of sagittal synostosis in a 7-month-old boy in Fig. 3.
Fig. 3. A case of sagittal synostosis in a 7-month-old boy. A : Photograph of the patient before surgery. B : Photograph at the surgery. Bioresorbable plates were used in this patient as base stones to strengthen the stability of anchor pins and traction pins. C : Wearing the MCDO-T frame. D : Photograph of the patient at 12 months after surgery. E, F, and G : Three-dimensional CT findings before surgery. H, I, and J : Three-dimensional CT findings at 12 months after surgery. This patient underwent 9 days of activation and 35 days of consolidation.

CLINICAL RESULTS OF MCDO IN OUR INSTITUTE
We select our method for craniosynostosis, except for lambdoid synostosis, for patients aged older than 5 months. Our procedure is difficult in children under the age of 4 months because the stability of the anchor screws depends on the thickness of temporal bone.
We retrospectively analyzed the clinical data of 36 children with craniosynostosis who underwent MCDO between 2005 and 2014 in our institute (Table 1). Thirty cases were initial cases and six cases were secondary cases. The involved sutures included a sagittal suture in 14 patients, a bicoronal suture in four patients, a unicoronal suture in three patients, a metopic suture in one patient, and multiple sutures in 14 patients. Twelve cases of syndromic craniosynostosis included Crouzon syndrome in eight patients, Pfeiffer syndrome in three patients, and Apert syndrome in one patient. The patients' ages ranged from 4 to 139 months (mean, 25.2 months; median, 12 months) and the follow-up period ranged from 18 to 125 months (mean, 63.6 months; median, 60 months). The mean age of 22 patients from 2005 to 2011 was 32 months, while the mean age of 14 patients from 2012 to 2014 was 15.2 months. The ages of the patients became younger according to the development of technical skill. Surgical time ranged from 230 to 507 minutes (mean, 347 minutes=5 hours and 40 minutes). Mean surgical time before 2011 was 370 minutes (6 hours), whereas after 2012, it was 303 minutes (5 hours). The amount of blood transfused ranged from 0 to 127 mL/kg body weight (mean, 32.3 mL/kg; median, 24 mL/kg). The mean amount of blood transfusion was 29.8 mL/kg in initial cases and 48.3 mL/kg in secondary cases.
Table 1. Summary of the patients.

The number of bone pieces ranged from nine to 30 (mean, 14.4), the number of traction pins ranged from six to 18 (mean, 10.8), and the number of anchor pins ranged from six to 10 (mean, 8). The phase of activation ranged from 8 to 14 days (mean, 10.5 days) and the consolidation period ranged from 14 to 63 days (mean, 43.4 days; median, 42 days). The mean hospitalization period was 19 days. Surgical results of all patients were good.
Six of 37 (16.2%) anchor pins used in the first six patients loosened because of bone absorption during the consolidation period. The number of anchor pins was six (three for each side) in these cases. After we altered the screw shape and fixed eight pins (four for each), loosening occurred in 18 of 232 (7.8%) pins in six of 30 patients. In two of these six patients, all anchor pins loosed because of local infection. Loosening of anchor pins occurred only in four of 218 (1.8%) pins in the patients, except for these two patients. Even in the case of infection, it was controlled with antibiotic administration and daily disinfection, and activation and consolidation were completed.
We applied bioresorbable plates as base stones to strengthen the stability of anchor pins in 10 patients, especially in those with syndromic craniosynostosis at the age of 4 to 5 months with a thin cranium. This supporting method was effective in eight of 10 patients. However, infection of anchor pins occurred in one patient, and a foreign body granuloma in temporal lobe caused by passive intraosseous translocation of a resorbable plate occurred in one patient16).
Loosening occurred in 29 of 390 (7.4%) traction pins, and in 19 of 184 (10.3%) pins before 2010 and in 10 of 206 (4.9%) pins after 2011. In the patients in whom the number of traction pins was under and equal to 10 pins, loosening occurred in 11 of 133 (8.3%) pins, while loosening occurred in 18 of 257 (7%) pins in patients with over 11 pins. Loosening of one or two traction pins did not affect activation and consolidation in patients in whom the number of traction pins was over 11 pins.
Nine patients had complications, including one with meningitis, four with transient subcutaneous cerebrospinal fluid (CSF) leakage, and two with pin-track infections that caused loosening of the frame. However, they were all healed with medication or daily shampooing to maintain cleanliness. All of the patients achieved the scheduled consolidation. Removal of the anchor pin was unnecessary to control infection.
ADVANTAGES OF MCDO COMPARED WITH THE OTHER TYPES OF DISTRACTION OSTEOGENESIS
The advantages of MCDO compared with the other distraction osteogenesis techniques are discussed below. Table 2 shows clinical data of previous reports with various treatment methods for craniosynostosis.
Table 2. Clinical data of various treatment methods for craniosynostosis.

The treatment period was defined as the period from the first surgery for attachment of the device to the second surgery of removal. FODO : fronto-orbital distraction osteogenesis, TSDO : transsutural distraction osteogenesis, PCDO : posterior calvarial distraction osteogenesis, E & H : endoscopic suturectomy and helmet molding, MCDO : multidirectional cranial distraction osteogenesis, DO : distraction osteogenesis, NA : not available
Distraction osteogenesis techniques have various advantages over the conventional cranial vault remodeling techniques1,4,17). These advantages include a shorter surgical time, less bleeding, and good blood supply to the cranial bone because of limited dissection of the dura mater, and safe and large expansion of skull because of simultaneous soft tissue expansion. However, various complications have been reported for distraction osteogenesis, such as pin-track infections, dural tears, CSF leakage, skull fracture during activation, internal device exposure, dislocation and distortion of the device, and breakage of the device2,9,22,30). Several disadvantages of this technique also exist, such as a prolonged treatment period and secondary surgical intervention to remove the devices. The greatest disadvantage is the limitation in morphological correction because a large piece of bone is moved in a single direction.
The MCDO method with a multidirectional external distraction device was developed to eliminate the disadvantages of conventional distraction osteogenesis. This method has the following benefits. First, the MCDO method provides better control when reshaping the cranial vault than unidirectional distraction osteogenesis because every small bone fragment can be moved appropriately with a wide range by each distractor. The extent to which each bone fragment moves can be varied according to the shape of the skull as determined by direct observation through the clear frame or on radiographic imaging. Bone fragments with traction pins move outward by active expansion, while fragments without traction pins can move passively outward or sometimes inward. Therefore, more flexible remodeling of the cranial vault achieves a normal skull shape. The MCDO method can be applied to all phenotypes in any craniosynostosis, excluding posterior calvarial vault deformity.
A high flexibility of reshaping of MCDO methods affects the surgical strategy. Unidirectional distraction osteogenesis methods need accurate pre-surgical planning of osteotomy and the position of distraction devices to achieve better reshaping. The MCDO method also needs planning. However, high flexibility of reshaping during the activation period provides flexibility of osteotomy and selection of bone fragments to drill the holes for the traction pins, except for the key bone fragments. We finally select the drilled fragments after osteotomy according to the degree of natural expansion of the skull.
Second, the MCDO method shortens the period of treatment. This is because the intracranial volume that can be increased by a given amount of distraction with multidirectional expansion is greater than that achieved by unidirectional expansion. We analyzed the amount of expansion with 3-dimensional volumetric analysis, and these results will be published separately. An approximate simulation of the expansion volume is shown in Fig. 4. A quarter volume of a sphere with a radius of r cm before surgery is VA. With the MCDO method, the amount of expansion after the activation period is at least 1 cm in radius, so that the quarter volume of a sphere goes up to VB. With the unidirectional distraction method the volume becomes VC. Calculation of the difference between VA and VB, or between VA and VC, showed that a quarter sphere of a radius of 5, 6, and 7 cm needs to shift parallel by 2.42, 2.35, and 2.3 cm, respectively, with unidirectional distraction to achieve the same amount of volume expansion with the MCDO method. The mean number of bone fragments was 14.4 in our series. As a result, the gap of each bone fragment with the MCDO method is much less than that with the previous distraction osteogenesis procedures. This finding means that the periods of not only activation, but also consolidation, are shortened because bone regeneration is faster owing to the fact that the distance between the bone fragments is smaller. Activation in the MCDO method started 5 days after surgery, the mean activation period was 10.5 days, and the mean consolidation period was 43.4 days. Therefore the frame could be removed under 60 days after surgery in our institution. Recent reports of conventional unilateral distraction osteogenesis methods showed that the period from the first surgery of attachment of the device to the second surgery of removal ranged from 70 to 100 days (Table 2)23,31,34,37,39,41).
Fig. 4. We calculated the expansion volume by a rough simulation. Because an infant skull resembles a sphere, the volume of the upper anterior quarter of the skull can be calculated using the formula shown in this figure. A quarter volume of a sphere with a radius of r cm before surgery is VA. VB and VC are the volume after the MCDO procedure and unidirectional frontal distraction surgery, respectively.

Third, secondary intervention in the MCDO method is much less invasive compared with the other distraction osteogenesis procedures, because it takes only 5 minutes with the patients under sedation and requires no incision. This means an improvement in medical outcome and in comfort for the patient and family.
Fourth, in unidirectional expansion, the skin is stretched along the single osteotomized line. Multidirectional expansion disperses the stretching forces on the whole scalp, which reduces resistance to skull expansion and the rate of postoperative relapse caused by skin contracture. Finally, there is no limitation to the osteotomy line and the size of the bone fragment. This is especially beneficial in secondary cases with extensive bone defects.
LIMITATIONS OF MCDO
There are limitations to this procedure. Although there were no major complications, minor complications, such as loosening of pins, CSF leakage, and minor infection, occurred during activation periods or consolidation periods in our institution. These issues need to be addressed.
The surgical time in our institution was longer compared with recent reports of other distraction osteogenesis procedures. Our mean surgical time was approximately 300 minutes, even in cases from 2011. Recent reports of the various unidirectional distraction osteogenesis procedures showed that the mean surgical times ranged from 115 to 230 minutes (Table 2)23,31,34,37,39). Our relatively longer surgical time may depend on the time of osteotomy to create many smaller bone fragments. We use an ultrasonic bone curette for osteotomy, and this equipment is useful for osteotomy with minimum bone dissection from the dura mater. Additionally, the ultrasonic bone curette prevents laceration of the dura mater, while it causes a long osteotomy time because of its safe and gentle power.
The stability of the anchor screw depends on the thickness of the temporal bone; therefore, application for a child who is younger than 4 months will be difficult. There were four patients younger than the age of 5 months in our series, and all of them had multiple synostosis, including three cases of syndromic craniosynostosis. We used bioresorbable plates as base stones to strengthen the stability of anchor pins in all four cases. However, we currently use no absorbable plate for the support of the anchor pins because we experienced some complications as mentioned above. The youngest patients from 2011 in our series are 8 months old. We discuss the optimal timing of surgery and the surgical strategies for younger patients separately below.
The MCDO method currently does not manage the problem of the posterior cranial vault. Further efforts, such as development of a new frame for the posterior cranial vault, should be made. Recently, many articles of posterior cranial vault distraction osteogenesis have been reported. These reports are also discussed below.
The MCDO system can be purchased from Keisei Medical Industrial Co. Ltd. only in Japan. This system consists of some disposable devices as mentioned above and special drills, screwdrivers, and the template for anchor pins. The cost is covered by the Japanese national health insurance as an external fixator system, and depends on the numbers of applied pins.
OPTIMAL TIMING OF SURGEY AND SURGERY FOR YOUNGER PATIENTS
The MCDO method allows all phenotypes of skull deformity to be reshaped by distraction osteogenesis. However, there are two exceptions, namely patients who are 5 months of age or younger and patients with posterior cranial vault problems.
There are two major aims of surgery for craniosynostosis. The first aim is to create natural brain development by expanding the cranial vault volume to reduce oppression to the brain parenchyma. The second aim is to produce an aesthetically prominent skull shape. Generally, early surgery is better for promoting brain development. However, the benefits of surgery must be balanced against the risks of the operative procedure. Therefore, most surgeons elect to operate after the postpartum infant hematopoietic nadir is passed (i.e., between 3 and 6 months of age). The properties of bones are also important factors. Bone before 3 months of age is thin and pliable, and can be cut and remodeled easily. However, rigid stabilization is difficult.
All 4 patients who underwent the MCDO procedure at the age of 4 to 5 months had multiple synostosis and required early interventions because of the severely increased intracranial pressure. In such cases, we consider that releasing intracranial pressure as soon as possible is more important than morphological outcome. The optimal timing of surgery for patients with simple suture synostosis is still under debate. Early interventions for patients with simple synostosis may be acceptable if the morphological and functional benefits exceed the surgical risks.
Jimenez et al.13,14,15) reported that early treatment of simple synostosis with endoscope-assisted strip craniectomy combined with helmet molding achieved a good outcome, and the mean age of the series was 3.1 months. This minimally invasive procedure may be suitable for younger patients. However, some potential drawbacks should be discussed5,10). First, an injury to the sagittal sinus could have disastrous effects with limited access incisions. A second drawback is the prolonged postoperative compressive helmet therapy. The helmet must be worn 23 hours per day, often until the child's first birthday, and requires frequent visits to an orthotist. Additionally, the long-term morphological and functional outcomes are still controversial, and this procedure cannot be elected for patients with multiple or syndromic craniosynostosis who require early intervention to reduce intracranial pressure. In addition, the helmets should be remade according to development of the cranial vault of the patients, and it is not covered by the national health insurance in Japan. However, all types of distraction devices, including the MCDO system, are covered. The procedure with endoscope-assisted strip craniectomy combined with helmet molding may be beneficial to a limited amount of younger patients with simple synostosis.
Ages at surgery in previous reports of distraction osteogenesis were varied (Table 2). Most surgeons appear to consider that the ideal age for distraction osteogenesis procedures is from 1 to 2 years. Patients younger than 6 months who underwent distraction osteogenesis are rare. Tahiri et al.37) reported 6 patients with unicoronal synostosis who were treated with distraction osteogenesis methods, and that the mean age was 4.8 months. According to the reported procedure and a case presentation, they placed the distraction device at the dissected coronal suture. Park et al.31) also reported the clinical results of transsutural distraction osteogenesis methods for 285 children with craniosynostosis. The mean age at surgery of bicoronal synostosis was 5.3 months, while that with other types of synostosis ranged from 10 to 33 months. These results show that transsutural distraction osteogenesis methods with dissection of the coronal suture and placement of the device at the dissected coronal suture are acceptable, even in younger patients. However, aesthetical outcomes are still controversial. Endoscopy-assisted craniectomy with the postoperative helmet molding method is more beneficial than transsutural distraction osteogenesis methods in younger patients because of lower invasiveness.
POSTERIOR CRANIAL VAULT DISTRACTION
The MCDO system is structurally not suitable for posterior cranial vault problems, such as lambdoid synostosis, although further development will negate this disadvantage. Posterior cranial vault expansion by the unidirectional distraction osteogenesis method has been used not only for posterior cranial vault problems, but also for all types of craniosynostosis. We review posterior cranial vault distraction below.
Expansion of the posterior cranial vault is preferred as a primary procedure because it directly addresses the posterior fossa. Additionally, this procedure has the potential to offer a far greater increase in intracranial volume than anterior expansion, such as fronto-orbital advancement, because of the larger volume that can be gained8,33,39). However, long-term results of posterior calvarial movement are not favorable because a prolonged supine posture in the postsurgical phase can impede expansion and result in relapse and early ossification of the craniotomy site18,39). Adoption of distraction techniques in the posterior cranium negates this issue because the bone flap can be fixed.
Posterior cranial vault expansion by distraction has been widely performed since first described by White et al. in 200939). Posterior distraction has the same advantages and disadvantages of the other distraction methods. The advantages of posterior distraction include limited dissection of the dura mater, lower risk of dural injury, less bleeding, the remaining bone is vascularized, and a decreased surgical time. There are also some complications, including wound infection and necrosis of the tissue overlying the device resulting in its exposure.
Initial attempts at cranial vault distraction were performed using devices that were designed for maxillary and mandibular distraction. Many authors have described the development of distraction devices and modified surgical procedures19,27,28,29,32,34). Ong et al.29) described the evolution of distraction devices and distraction use. They designed a modified device to address cranial vault distraction, and upgraded the devices in the subsequent version to prevent relapse after distraction. They also arranged the number of distractors. Four distractors were initially placed. However, difficulty was noted in distraction to regulate the vectors of all distractors to ensure that they were working in the same direction. Eventually, they found that two distractors provide the optimum balance between ease of use, stability, and ability to execute a planned distraction vector. Derderian and Bartlett6) and Steinbecher et al.34) also described that the appropriate number of distractors was two in the posterior cranial distraction osteogenesis method.
Thomas et al.38) and Wiberg et al.40) classified posterior cranial vault distraction techniques into two types, the "hinge" technique and the "push-back" technique. In the hinge technique, the posterior panel is hinged inferiorly in the midline and downward during distraction, with the aim of reducing the vertex height in addition to expanding the posterior vault. In patients in whom expansion of the posterior fossa is the primary goal, the released posterior panel is left unhinged (the "push-back" technique), enabling it to be displaced in line with the distraction vector without rotation. This increases expansion of the posterior cranial fossa.
Some authors have described a staged surgery for patients with fronto-orbital deformities18,38). After the first surgery of posterior cranial vault distraction to reduce intracranial pressure, they performed a second surgery of fronto-orbital remodeling with remodeling or distraction techniques. Staged surgeries have also been reported for patients with thin cranial vaults29). The first step of pressure-releasing procedures, such as craniotomy and modified vault remodeling, and secondary procedures of cranial vault distraction were recommended.
In patients with posterior cranial vault problems or syndromic craniosynostosis, the volume of the posterior fossa becomes smaller, resulting in formation of acquired Chiari malformation type I. Therefore, there is an issue of where we should spread posterior osteotomy for posterior cranial vault distraction. Furthermore, narrowing of the transverse-sigmoid sinus is usual. This results in the development of venous collaterals of the emissary veins, especially in patients with syndromic craniosynostosis. Advanced osteotomies are sometimes limited because of developed emissary veins. Most reports described that the lower line of posterior osteotomy was at the level of the inion (torcular herophili)6,10). However, whether intracranial pressure of the posterior fossa can be decreased with osteotomy up to the inion remains controversial. Komuro et al. described posterior cranial vault distraction osteogenesis with barrel stave osteotomy18,19,20). Biparietal osteotomy is performed and a transverse occipital osteotomy is performed approximately 2 cm below the inion. Barrel stave osteotomy is also performed to expand the subtentorial region6). This additional osteotomy may contribute to reduction of intracranial pressure of the posterior fossa and improvement of tonsillar herniation. Derderian and Bartlett6) also described that posterior cranial vault distraction and barrel stave osteotomy on the inferior occipital segment improve contours and obviate a difference in level between the distracted segment and cranial base7).
Posterior cranial vault distraction osteogenesis methods can improve posterior cranial problems and also provide greater expansion of whole cranial volume. Modified methods and combined methods using this procedure have been developed. However, long-term morphological and functional outcomes of posterior cranial vault distraction osteogenesis are still controversial. In addition, whether posterior cranial distraction methods are suitable for younger patients, and how to dissect or preserve well developed collateral emissary veins are also still controversial.
SPRINGS
The distraction osteogenesis procedure can use springs for the treatment of craniosynostosis5,21). Lauritzen et al.21) advocate the use of springs in any of the symmetric patterns of craniosynostosis. For sagittal synostosis, the procedure consists of strip craniectomy, with application of two to three springs in obliquely drilled holes near the edge of craniectomy. The spring distraction osteogenesis method has several potential advantages. This method is optimally used at younger ages when the cranial bones are most pliable. Compared with distractors, springs are completely covered by soft tissue, which can reduce the risk for infections. However, the distraction vectors, forces, and degrees cannot be controlled, resulting in an increased risk of complications. These complications include bleeding, CSF leakage, and unwarranted less expansion or overexpansion of the cranium with an undesirable cosmetic outcome6,27,31,32). There are also spring-related complications, such as dislodgement of springs, skin penetration, and pressure sores. As a result, indication of the spring distraction osteogenesis procedure has been limited.
CONCLUSION
We have introduced the MCDO procedure and reviewed the various techniques, including distraction osteogenesis methods for craniosynostosis surgery. We cannot conclude which method is the best because randomized studies may be difficult in this field. The preferred procedure for correction of craniosynostosis may depend on the patient's age, the extent of deformity, and the extent of correction achievable by surgery. We do not persist in using one procedure, and we can arrange the combinations of various methods according to the advantage and disadvantage of each technique. The authors will focus on developing the MCDO system and encouraging its use worldwide.
References
- 1.Akai T, Iizuka H, Kawakami S. Treatment of craniosynostosis by distraction osteogenesis. Pediatr Neurosurg. 2006;42:288–292. doi: 10.1159/000094064. [DOI] [PubMed] [Google Scholar]
- 2.Akai T, Shiraga S, Sasagawa Y, Iizuka H, Yamashita M, Kawakami S. Troubleshooting distraction osteogenesis for craniosynostosis. Pediatr Neurosurg. 2013;49:380–383. doi: 10.1159/000369029. [DOI] [PubMed] [Google Scholar]
- 3.Cho BC, Hwang SK, Uhm KI. Distraction osteogenesis of the cranial vault for the treatment of craniofacial synostosis. J Craniofac Surg. 2004;15:135–144. doi: 10.1097/00001665-200401000-00034. [DOI] [PubMed] [Google Scholar]
- 4.Choi JW, Ra YS, Hong SH, Kim H, Shin HW, Chung IW, et al. Use of distraction osteogenesis to change endocranial morphology in unilateral coronal craniosynostosis patients. Plast Reconstr Surg. 2010;126:995–1004. doi: 10.1097/PRS.0b013e3181e6c4b7. [DOI] [PubMed] [Google Scholar]
- 5.David LR, Proffer P, Hurst WJ, Glazier S, Argenta LC. Spring-mediated cranial reshaping for craniosynostosis. J Craniofac Surg. 2004;15:810–816. doi: 10.1097/00001665-200409000-00021. discussion 817-818. [DOI] [PubMed] [Google Scholar]
- 6.Derderian CA, Bartlett SP. Open cranial vault remodeling : the evolving role of distraction osteogenesis. J Craniofac Surg. 2012;23:229–234. doi: 10.1097/SCS.0b013e318241b93a. [DOI] [PubMed] [Google Scholar]
- 7.Derderian CA, Bastidas N, Bartlett SP. Posterior cranial vault expansion using distraction osteogenesis. Childs Nerv Syst. 2012;28:1551–1556. doi: 10.1007/s00381-012-1802-0. [DOI] [PubMed] [Google Scholar]
- 8.Derderian CA, Wink JD, McGrath JL, Collinsworth A, Bartlett SP, Taylor JA. Volumetric changes in cranial vault expansion : comparison of fronto-orbital advancement and posterior cranial vault distraction osteogenesis. Plast Reconstr Surg. 2015;135:1665–1672. doi: 10.1097/PRS.0000000000001294. [DOI] [PubMed] [Google Scholar]
- 9.Esparza J, Hinojosa J. Complications in the surgical treatment of craniosynostosis and craniofacial syndromes : apropos of 306 transcranial procedures. Childs Nerv Syst. 2008;24:1421–1430. doi: 10.1007/s00381-008-0691-8. [DOI] [PubMed] [Google Scholar]
- 10.Governale LS. Craniosynostosis. Pediatr Neurol. 2015;53:394–401. doi: 10.1016/j.pediatrneurol.2015.07.006. [DOI] [PubMed] [Google Scholar]
- 11.Hirabayashi S, Sugawara Y, Sakurai A, Harii K, Park S. Frontoorbital advancement by gradual distraction. Technical note. J Neurosurg. 1998;89:1058–1061. doi: 10.3171/jns.1998.89.6.1058. [DOI] [PubMed] [Google Scholar]
- 12.Imai K, Komune H, Toda C, Nomachi T, Enoki E, Sakamoto H, et al. Cranial remodeling to treat craniosynostosis by gradual distraction using a new device. J Neurosurg. 2002;96:654–659. doi: 10.3171/jns.2002.96.4.0654. [DOI] [PubMed] [Google Scholar]
- 13.Jimenez DF, Barone CM. Early treatment of coronal synostosis with endoscopy-assisted craniectomy and postoperative cranial orthosis therapy : 16-year experience. J Neurosurg Pediatr. 2013;12:207–219. doi: 10.3171/2013.4.PEDS11191. [DOI] [PubMed] [Google Scholar]
- 14.Jimenez DF, Barone CM. Endoscopic craniectomy for early surgical correction of sagittal craniosynostosis. J Neurosurg. 1998;88:77–81. doi: 10.3171/jns.1998.88.1.0077. [DOI] [PubMed] [Google Scholar]
- 15.Jimenez DF, Barone CM, Cartwright CC, Baker L. Early management of craniosynostosis using endoscopic-assisted strip craniectomies and cranial orthotic molding therapy. Pediatrics. 2002;110(1 Pt 1):97–104. doi: 10.1542/peds.110.1.97. [DOI] [PubMed] [Google Scholar]
- 16.Katsuragi YT, Gomi A, Sunaga A, Miyazaki K, Kamochi H, Arai F, et al. Intracerebral foreign body granuloma caused by a resorbable plate with passive intraosseous translocation after cranioplasty. J Neurosurg Pediatr. 2013;12:622–625. doi: 10.3171/2013.9.PEDS13187. [DOI] [PubMed] [Google Scholar]
- 17.Kim SW, Shim KW, Plesnila N, Kim YO, Choi JU, Kim DS. Distraction vs remodeling surgery for craniosynostosis. Childs Nerv Syst. 2007;23:201–206. doi: 10.1007/s00381-006-0209-1. [DOI] [PubMed] [Google Scholar]
- 18.Komuro Y, Shimizu A, Shimoji K, Miyajima M, Arai H. Posterior cranial vault distraction osteogenesis with barrel stave osteotomy in the treatment of craniosynostosis. Neurol Med Chir (Tokyo) 2015;55:617–623. doi: 10.2176/nmc.ra.2014-0401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Komuro Y, Shimizu A, Ueda A, Miyajima M, Nakanishi H, Arai H. Whole cranial vault expansion by continual occipital and fronto-orbital distraction in syndromic craniosynostosis. J Craniofac Surg. 2011;22:269–272. doi: 10.1097/SCS.0b013e3181f7dc08. [DOI] [PubMed] [Google Scholar]
- 20.Komuro Y, Yanai A, Hayashi A, Miyajima M, Nakanishi H, Arai H. Treatment of unilateral lambdoid synostosis with cranial distraction. J Craniofac Surg. 2004;15:609–613. doi: 10.1097/00001665-200407000-00015. [DOI] [PubMed] [Google Scholar]
- 21.Lauritzen CG, Davis C, Ivarsson A, Sanger C, Hewitt TD. The evolving role of springs in craniofacial surgery : the first 100 clinical cases. Plast Reconstr Surg. 2008;121:545–554. doi: 10.1097/01.prs.0000297638.76602.de. [DOI] [PubMed] [Google Scholar]
- 22.Lee JA, Park DH, Yoon SH, Chung J. Distractor breakage in cranial distraction osteogenesis for children with craniosynostosis. Pediatr Neurosurg. 2008;44:216–220. doi: 10.1159/000121378. [DOI] [PubMed] [Google Scholar]
- 23.Lee MC, Shim KW, Park EK, Yun IS, Kim DS, Kim YO. Expansion and compression distraction osteogenesis based on volumetric and neurodevelopmental analysis in sagittal craniosynostosis. Childs Nerv Syst. 2015;31:2081–2089. doi: 10.1007/s00381-015-2843-y. [DOI] [PubMed] [Google Scholar]
- 24.McCarthy JG, Schreiber J, Karp N, Thorne CH, Grayson BH. Lengthening the human mandible by gradual distraction. Plast Reconstr Surg. 1992;89:1–8. discussion 9-10. [PubMed] [Google Scholar]
- 25.Nishimoto S, Oyama T, Nagashima T, Shimizu F, Tsugawa T, Takeda M, et al. Gradual distraction fronto-orbital advancement with 'floating forehead' for patients with syndromic craniosynostosis. J Craniofac Surg. 2006;17:497–505. doi: 10.1097/00001665-200605000-00019. [DOI] [PubMed] [Google Scholar]
- 26.Nonaka Y, Oi S, Miyawaki T, Shinoda A, Kurihara K. Indication for and surgical outcomes of the distraction method in various types of craniosynostosis. Advantages, disadvantages, and current concepts for surgical strategy in the treatment of craniosynostosis. Childs Nerv Syst. 2004;20:702–709. doi: 10.1007/s00381-004-0917-3. [DOI] [PubMed] [Google Scholar]
- 27.Nowinski D, Di Rocco F, Renier D, SainteRose C, Leikola J, Arnaud E. Posterior cranial vault expansion in the treatment of craniosynostosis. Comparison of current techniques. Childs Nerv Syst. 2012;28:1537–1544. doi: 10.1007/s00381-012-1809-6. [DOI] [PubMed] [Google Scholar]
- 28.Nowinski D, Saiepour D, Leikola J, Messo E, Nilsson P, Enblad P. Posterior cranial vault expansion performed with rapid distraction and time-reduced consolidation in infants with syndromic craniosynostosis. Childs Nerv Syst. 2011;27:1999–2003. doi: 10.1007/s00381-011-1563-1. [DOI] [PubMed] [Google Scholar]
- 29.Ong J, Harshbarger RJ, 3rd, Kelley P, George T. Posterior cranial vault distraction osteogenesis : evolution of technique. Semin Plast Surg. 2014;28:163–178. doi: 10.1055/s-0034-1390169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Park DH, Chung J, Yoon SH. Rotating distraction osteogenesis in 23 cases of craniosynostosis : comparison with the classical method of craniotomy and remodeling. Pediatr Neurosurg. 2010;46:89–100. doi: 10.1159/000319005. [DOI] [PubMed] [Google Scholar]
- 31.Park DH, Yoon SH. Transsutural distraction osteogenesis for 285 children with craniosynostosis : a single-institution experience. J Neurosurg Pediatr. 2015;18:1–10. doi: 10.3171/2015.5.PEDS14585. [DOI] [PubMed] [Google Scholar]
- 32.Serlo WS, Ylikontiola LP, Lähdesluoma N, Lappalainen OP, Korpi J, Verkasalo J, et al. Posterior cranial vault distraction osteogenesis in craniosynostosis : estimated increases in intracranial volume. Childs Nerv Syst. 2011;27:627–633. doi: 10.1007/s00381-010-1353-1. [DOI] [PubMed] [Google Scholar]
- 33.Sgouros S, Goldin JH, Hockley AD, Wake MJ. Posterior skull surgery in craniosynostosis. Childs Nerv Syst. 1996;12:727–733. doi: 10.1007/BF00366158. [DOI] [PubMed] [Google Scholar]
- 34.Steinbacher DM, Skirpan J, Puchała J, Bartlett SP. Expansion of the posterior cranial vault using distraction osteogenesis. Plast Reconstr Surg. 2011;127:792–801. doi: 10.1097/PRS.0b013e318200ab83. [DOI] [PubMed] [Google Scholar]
- 35.Sugawara Y, Hirabayashi S, Sakurai A, Harii K. Gradual cranial vault expansion for the treatment of craniofacial synostosis : a preliminary report. Ann Plast Surg. 1998;40:554–565. doi: 10.1097/00000637-199805000-00021. [DOI] [PubMed] [Google Scholar]
- 36.Sugawara Y, Uda H, Sarukawa S, Sunaga A. Multidirectional cranial distraction osteogenesis for the treatment of craniosynostosis. Plast Reconstr Surg. 2010;126:1691–1698. doi: 10.1097/PRS.0b013e3181ef8fc8. [DOI] [PubMed] [Google Scholar]
- 37.Tahiri Y, Swanson JW, Taylor JA. Distraction osteogenesis versus conventional fronto-orbital advancement for the treatment of unilateral coronal synostosis : a comparison of perioperative morbidity and short-term outcomes. J Craniofac Surg. 2015;26:1904–1908. doi: 10.1097/SCS.0000000000002020. [DOI] [PubMed] [Google Scholar]
- 38.Thomas GP, Wall SA, Jayamohan J, Magdum SA, Richards PG, Wiberg A, et al. Lessons learned in posterior cranial vault distraction. J Craniofac Surg. 2014;25:1721–1727. doi: 10.1097/SCS.0000000000000995. [DOI] [PubMed] [Google Scholar]
- 39.White N, Evans M, Dover MS, Noons P, Solanki G, Nishikawa H. Posterior calvarial vault expansion using distraction osteogenesis. Childs Nerv Syst. 2009;25:231–236. doi: 10.1007/s00381-008-0758-6. [DOI] [PubMed] [Google Scholar]
- 40.Wiberg A, Magdum S, Richards PG, Jayamohan J, Wall SA, Johnson D. Posterior calvarial distraction in craniosynostosis - an evolving technique. J Craniomaxillofac Surg. 2012;40:799–806. doi: 10.1016/j.jcms.2012.02.018. [DOI] [PubMed] [Google Scholar]
- 41.Winston KR, Ketch LL, Dowlati D. Cranial vault expansion by distraction osteogenesis. J Neurosurg Pediatr. 2011;7:351–361. doi: 10.3171/2011.1.PEDS10330. [DOI] [PubMed] [Google Scholar]