

Abstract
Background:
This in vitro study investigated the marginal fit of two porcelain laminate veneers to help the selection of more accurate veneers in discolored teeth.
Materials and Methods:
Thirty impressions of metal master die created from the prepared labial surface of an acrylic maxillary central incisor were made and poured with Type IV stone. The dies were distributed into test groups (n = 15) for the construction of DuCeram and InCeram laminate veneers. An image-analysis program was used to measure the gap between the veneers and the master die at the labial, lingual, and proximal margins. Statistical analysis was performed with repeated measures ANOVA. Independent t-test was used to compare the mean values between the two groups. Values of P < 0.05 were judged to be significant.
Results:
Differences between marginal fit of two groups were significant (P < 0.001). The overall mean marginal gap values (μm) for InCeram and DuCeram were, respectively, 114.4 ± 40.81 and 282.3 ± 82.82. Independent t-test revealed significant differences between the marginal gaps of two materials at different predetermined points.
Conclusion:
Within the limitations of this study, the marginal gap in InCeram laminate veneer was within the clinically acceptable standard set at 120 μm.
Keywords: Dental marginal adaptation, dental porcelain, dental veneer
INTRODUCTION
Porcelain laminate restorations are of the most successful treatment modalities for cosmetic improvement of unsightly anterior teeth. Treatment of traumatic fractures, moderate tooth wear, and congenital tooth malformations as well as the esthetic reshaping of anterior teeth may also be accomplished with the use of these restorations.[1] Dental ceramics comprise a large family of inorganic nonmetal materials and are commonly divided into two groups: Silicate ceramics and oxide ceramics.[2]
Veneers were mainly fabricated from conventional low fusing feldspathic porcelain (silicate ceramics). Two methods of fabrication of these porcelain veneers are the platinum foil technique and the refractory die technique. At present, the refractory die technique is preferred to the platinum foil technique in most laboratories.[3]
The disadvantage of a conventional porcelain is that the particles are sintered together, resulting in microporosities within the porcelain itself. As a consequence, these inhomogeneities can initiate crack propagation, leading to the early failure of the restorations.[3] Due to the high glass contents in this material, they are much more susceptible to fracture under mechanical stress.[4] When the amount of functional loads is extensive, the use of material with great resistance to fracture is needed. Generally, higher tensile and shear stress occur when there are large areas of unsupported porcelain (as in cases of diastema closure and teeth with chipping or fracture), deep overbites, overlaps of teeth, when bonding veneers to more flexible substrates such as dentin and composite, when bruxism is present and when the restorations are placed more distally. In these higher risk clinical situations, high strength ceramics as alumina-based ceramics should be considered.[5]
Aluminum oxide ceramics include InCeram alumina, InCeram spinelle, InCeram zirconium, and Procera® AAllCeram. These are high resistance ceramics.[3]
The InCeram (Vita Zahnfabrik, Sackingen, Germany) ceramic system consists of a high-strength ceramic based on a matrix of sintered aluminum oxide infused with glass; the system is conventionally used as a core material in conjunction with a more translucent ceramic to enhance esthetic properties.[6]
The long-term clinical performance of the ceramic restoration mainly depends on several factors; the fit and the relative strength are of significant interest. The marginal inaccuracy might be a serious predisposing factor to the early failure of the restorations.[7]
The importance of marginal fit for clinical success of ceramic restoration has been emphasized in several clinical trials.[8,9] External marginal adaptation of ceramic veneers, which is defined as the vertical distance between the finish line of the prepared tooth and the margins of the fabricated veneers play an important role for their success.[10] Close proximity between the margin of the restorations and the tooth structure protects the adhesive resin cement from excessive exposure to the oral cavity leading eventually to slow process of gradual disintegration of its chemical, physical, and mechanical properties resulting in microleakage, recurrent decay, discoloration of the tooth structure, and fracture of the cemented veneers. On the other hand, internal marginal adaptation is a direct measure of the cement film thickness underneath the restoration and is significantly influenced by the accuracy of fabrication process used.[11] While external (noninvasive) marginal adaptation could be measured using different imaging methods as stereo or scanning electron microscopy, internal (invasive) marginal adaptation requires sectioning of these restorations in order to assess the cement film thickness underneath the cemented restorations.[9]
Variation exists regarding what constitutes a clinically acceptable margin.[12] McLean and von Fraunhofer[13] proposed that a restoration would be successful if marginal gaps of <120 μm could be achieved. This criterion has been cited in some articles.[14]
Despite the fact that InCeram ceramic system provides superior strength restorations, the information on its marginal fit is inadequate. The purpose of this study was to examine the external marginal gap of the feldespathic and Spinell InCeram laminate veneers and comparing marginal fit of laminates in two types of porcelains, testing the null hypotheses that there are no differences in the marginal gap between the resulted laminates.
MATERIALS AND METHODS
The labial surface of an acrylic maxillary central incisor (AB-3; Fraco, Tettang, Germany) was indexed by applying a condensation silicone impression material (Speedex; Colten, Switzerland) to ensure consistency of the definitive shape and thickness of finished laminate veneers. Then, this acrylic tooth was prepared with conventional design of discolored teeth that included reduction of the incisal edge for 2 mm and labial surface to a depth of 1.5 mm, 1 mm coronal to the cementoenamel junction. In addition; the finish line was extended 1 mm at proximal regions. This preparation was made free of any irregularities using a rounded chamfer (NTI Diamond Instrument 2850 016; NTI-Kahla Gmbts) preparation.[1]
The impression of prepared tooth was made using condensation silicone impression material with double mixing technique,[15] poured by acrylic resin (GC Pattern Resin; GC Corp, Tokyo, Japan), invested in phosphate-bonded investment (Rema-Exakt; Dentaurum, Ispringen Germany), burned out, and cast into Cr-Co alloy metal die (Rexillium III; Jenericy Pentron, Inc., Wallingford, Conn, Shenzhen, China). After finishing and polishing the master metal die (Dura-Green and Silicon Hardies Silicon Carbide Stones, Kyoto, Japan), the sites for evaluation of marginal adaptation all around the tooth were determined at 6 points as follows: Points A and B on the labial surface, D and E on the lingual surface and C and F on each proximal region.[8]
Thirty Impressions of the Cr-Co alloy master die were made using a condensation silicone, in 3-mm-relieved special trays (Light-polymerized Hanan-Wolfgang, Germany) and poured using Type IV dental stone (Silky-Rock; Whip Mix Corp, Louisrille, KY). The stone dies were allowed to set for 24 h. The stone dies were visually inspected under ×20 magnification (Stereoscopic Zoom Microscope; Nikon Corporation, Tokyo, Japan) for any irregularities, by a single operator. Then, the dies were individually allocated into 2 groups. The sample size of 15 was selected based on previous studies.[16]
Each group was assigned to a particular laminate system according to each manufacturer's recommendations: Feldespatic laminate veneers, DuCeram LFC (Ducera, Rosbach, Germany) sintered on refractory die technique, and InCeram laminate veneers (Vita Zahnfabrik, Sackingen, Germany) fabricated by slip-cast technique. Silicon index resembled the shape and thickness of veneers.
Each restoration was placed on the metal die and stabilized with hueless glue (Tenaz, Sao Paulo, Brazil) at two points of the facial and lingual margins. Then, the die was held under a uniform static labial load of 2 lbs (1.2 kg) for 30 s using the Hounsfield universal testing machine (Hounsfield, BK) [Figure 1].[17]
Figure 1.
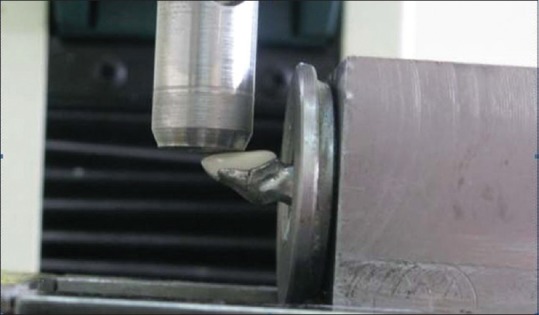
Die stabilization with die adhesive under a static labial load.
The marginal fit was evaluated perpendicular to the metal dies’ axis by measuring the gap between the edge of the laminate and the die margin at 6 predetermined points.
A stereomicroscope (Stereoscopic Zoom Microscope; Nikon Corporation, Tokyo, Japan) combined with a computer system was used to evaluate marginal gaps. The camera (Digital Sight Camera, Nikon, Tokyo, Japan) reproduced × 46 magnification so that a video image of the marginal gap could be examined using special software (Camera DS-LS).
A millimeter calibration slide was used during each viewing session at the same magnification and referenced for calibration. All measurements were performed 3 times by the same investigator [Figure 2].[8]
Figure 2.
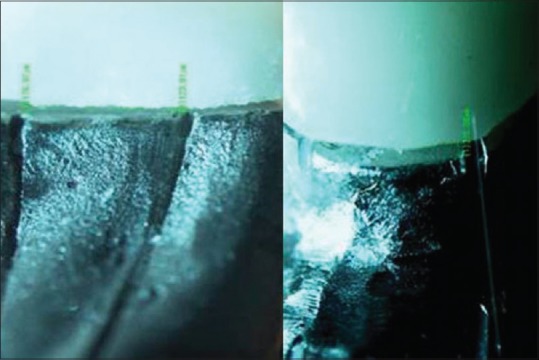
Labial margin of DuCeram (right) and lingual margin of InCeram under a stereomicroscope.
The data were statistically analyzed with statistical software (SPSS 12.0; SPSS, Inc., Chicago, III, USA). The Kolmogorov-Smirnov test was used to verify the normality of the data distribution. Data were analyzed with repeated measures ANOVA. Independent t-test was used for comparison of gaps between the groups. A P < 0.05 was considered to indicate statistical significance.
RESULTS
The mean values and standard deviations (SDs) of the average dimensions of marginal gap in points A and B were calculated as marginal gap on the labial aspect, points D and E as the gap on the lingual aspect and points C and F as the gap on the proximal aspect of veneers.
Tables 1 and 2 show the mean values and SDs of the average gap dimensions on the labial, lingual, and proximal surfaces of InCeram and DuCeram veneers, respectively. Based on data, the mean values and SDs of marginal gaps were 114.42 ± 30.52 and 282.31 ± 37.46 for the InCeram and DuCeram groups, respectively.
Table 1.
Means±standard deviations of marginal fit in the InCeram group
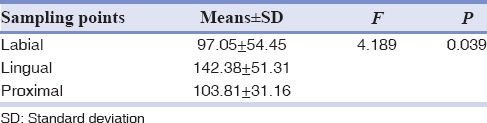
Table 2.
Means±standard deviations of marginal fit in the DuCeram group
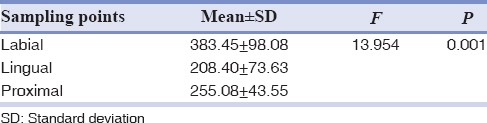
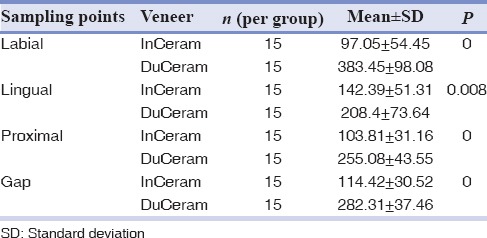
Table 3 presents comparison of marginal gap dimensions on facial, lingual, and proximal surfaces and of all gap dimensions between InCeram and DuCeram veneers. The results of independent t-test showed significantly higher marginal discrepancies on the facial (383.45 μm), lingual (208.4 μm), and proximal (255.08 μm) surfaces of DuCeram veneers compared to facial (97.05 μm), lingual (142.39 μm), and proximal (103.81 μm) surfaces of InCeram laminate veneers.
Table 3.
Independent t-test for comparison of gaps between the groups
DISCUSSION
The results of this study showed that types of ceramics in laminate veneers influenced marginal adaptation. Less marginal gap noted in InCeram veneers.
Previous studies indicated large variations of marginal gap in laminate veneer systems. The marginal gap of 114.4 μm for Vita InCeram laminate veneers was much less than marginal gap of DuCeram laminate veneers in this study (282.3 μm), and also the values reported by Sorensen et al.[18] (242 μm), Sim and Ibbetson[19] (290 μm), and Wall et al.[20] (132 μm).
An explanation of inconsistency between the results might be variations in the methods used by various investigators studying marginal accuracy. Sulaiman et al.[16] suggested that the use of different measuring instruments, sample sizes, and number of measurements per specimen might also have contributed to the variations.
Lim and Ironside[21] reported that divesting with aluminum oxide abrasive may account for inadvertent abrasion of the delicate inner porcelain surface and causes larger marginal discrepancies (114 mm with sandblasting vs. 97 mm without sandblasting).
Feldspathic porcelain restorations constructed by the traditional laboratory technique should shrink toward the die during firing, resulting in a better internal fit.[18] In addition, the proximal and labial aspects of the veneers made with conventional sintered feldspathic porcelain would have poorer marginal fit as a result of the shrinkage of the porcelain toward the region of greater bulk.[11,18] This study also reflected this finding.
The significantly higher marginal gap of DuCeram compared to InCeram veneers was attributed to the type of manufacturing of these 2 ceramic veneers; the distortion of the ceramic veneers was thought to be less in InCeram compared with DuCeram, as the fit of DuCeram at a certain location might further be influenced by nonuniform distortion during porcelain firing phase.
However, in InCeram, by sintering shrinkage during firing may be avoided, firing porcelain on ceramic copings. Hilgert showed that the addition of porcelain to the InCeram coping and repeated firing cycles involved in building a crown did not alter the fittness.[22]
Values proposed in the literature as acceptable marginal adaptations vary depending on the type of restoration and author McLean and Von Fraunhofer,[13] in a clinical study on 100 restorations in a 5-year period concluded that 120 μm represents the maximum clinically acceptable misfit. All the results in this study, except for labial and proximal surfaces of InCeram, therefore, would not be clinically acceptable.
In the present study, as well as those by Sim and Ibbetson,[19] Groten et al.,[23] Sulaiman et al.,[16] Nakamura et al.[24] and Tinschert et al.[25] external marginal gap was measured. In this method, as the samples are kept intact, it is possible to employ the same samples in other tests. The strength and the durability of the bond between the porcelain, the luting cement and the enamel/dentin interface play an important role in the outcome of ceramic veneers, particularly when dentin is involved.[11] It is not uncommon that, particularly in the gingival third of a veneer preparation, dentin will be exposed due to the thin layer of enamel present at this site.[26] Nonetheless, predictable adhesion to the dentin is an achievable goal using new multistep enamel-dentinal adhesive systems.[27]
There were some limitations in this study. Marginal fit of laminates after cementation and also internal adaptation of laminates were not determined, and it must be noted that seating veneers on test dies and measuring marginal discrepancy without cementation will not correctly reflect the actual marginal adaptation in the mouth because of higher marginal discrepancy occurs after cementation.[28] Possibly because of the excellent adaptation of the veneer, the cement was not pressed out of the inner surface to its lowest film thickness.[29] Furthermore, if veneers are not cemented, researchers cannot record the fracturing or chipping of ceramic margins that occur when porcelain margins are overextended and fracture from seating pressure. These chips in the porcelain margin can significantly increase the SD in the marginal discrepancy measurements.[30] Factors that affect the marginal and internal adaptation of porcelain laminate veneers require further investigations supported with clinical trials.
CONCLUSION
Within the limitations of this study, overall, external marginal gap of InCeram laminatesis considered clinically more acceptable than DuCeram.
Financial support and sponsorship
Nil.
Conflicts of interest
The authors of this manuscript declare that they have no conflicts of interest, real or perceived, financial or non-financial in this article.
ACKNOWLEDGMENTS
This research was carried out by financial support of the Vice Chancellor for Research at Tabriz University of Medical Sciences. The authors declare that they have no competing interests.
REFERENCES
- 1.Cehreli MC, Iplikçioglu H. Five-year follow-up of InCeram laminate restorations: A clinical report. J Prosthet Dent. 2000;84:487–9. doi: 10.1067/mpr.2000.110496. [DOI] [PubMed] [Google Scholar]
- 2.Puchades O, Solá MF, Martínez A, Labaig C, Fons A, Amigó V. Study of the composition and structure of full ceramic crowns. Int Rev PROTES Estomatol. 2004;6:330–8. [Google Scholar]
- 3.Wildgoose DG, Winstanley RB, van Noort R. The laboratory construction and teaching of ceramic veneers: A survey. J Dent. 1997;25:119–23. doi: 10.1016/s0300-5712(96)00017-6. [DOI] [PubMed] [Google Scholar]
- 4.McLaren EA, Whiteman YY. Ceramics: Rationale for material selection. Compend Contin Educ Dent. 2010;31:666–8. [PubMed] [Google Scholar]
- 5.McLaren EA, LeSage B. Feldspathic veneers: What are their indications? Compend Contin Educ Dent. 2011;32:44–9. [PubMed] [Google Scholar]
- 6.Fons-Font A, Solá-Ruíz MF, Granell-Ruíz M, Labaig-Rueda C, Martínez-González A. Choice of ceramic for use in treatments with porcelain laminate veneers. Med Oral Patol Oral Cir Bucal. 2006;11:E297–302. [PubMed] [Google Scholar]
- 7.Yeo IS, Yang JH, Lee JB. In vitro marginal fit of three all-ceramic crown systems. J Prosthet Dent. 2003;90:459–64. doi: 10.1016/j.prosdent.2003.08.005. [DOI] [PubMed] [Google Scholar]
- 8.Baig MR, Tan KB, Nicholls JI. Evaluation of the marginal fit of a zirconia ceramic computer-aided machined (CAM) crown system. J Prosthet Dent. 2010;104:216–27. doi: 10.1016/S0022-3913(10)60128-X. [DOI] [PubMed] [Google Scholar]
- 9.Beuer F, Aggstaller H, Edelhoff D, Gernet W, Sorensen J. Marginal and internal fits of fixed dental prostheses zirconia retainers. Dent Mater. 2009;25:94–102. doi: 10.1016/j.dental.2008.04.018. [DOI] [PubMed] [Google Scholar]
- 10.Celik C, Gemalmaz D. Comparison of marginal integrity of ceramic and composite veneer restorations luted with two different resin agents: An in vitro study. Int J Prosthodont. 2002;15:59–64. [PubMed] [Google Scholar]
- 11.Peumans M, Van Meerbeek B, Lambrechts P, Vanherle G. Porcelain veneers: A review of the literature. J Dent. 2000;28:163–77. doi: 10.1016/s0300-5712(99)00066-4. [DOI] [PubMed] [Google Scholar]
- 12.Hunter AJ, Hunter AR. Gingival margins for crowns: A review and discussion. Part II: Discrepancies and configurations. J Prosthet Dent. 1990;64:636–42. doi: 10.1016/0022-3913(90)90286-l. [DOI] [PubMed] [Google Scholar]
- 13.McLean JW, von Fraunhofer JA. The estimation of cement film thickness by an in vivo technique. Br Dent J. 1971;131:107–11. doi: 10.1038/sj.bdj.4802708. [DOI] [PubMed] [Google Scholar]
- 14.May KB, Russell MM, Razzoog ME, Lang BR. Precision of fit: The Procera AllCeram crown. J Prosthet Dent. 1998;80:394–404. doi: 10.1016/s0022-3913(98)70002-2. [DOI] [PubMed] [Google Scholar]
- 15.Krejci I, Duc O, Dietschi D, de Campos E. Marginal adaptation, retention and fracture resistance of adhesive composite restorations on devital teeth with and without posts. Oper Dent. 2003;28:127–35. [PubMed] [Google Scholar]
- 16.Sulaiman F, Chai J, Jameson LM, Wozniak WT. A comparison of the marginal fit of In-Ceram, IPS Empress, and Procera crowns. Int J Prosthodont. 1997;10:478–84. [PubMed] [Google Scholar]
- 17.Jemt T, Rubenstein JE, Carlsson L, Lang BR. Measuring fit at the implant prosthodontic interface. J Prosthet Dent. 1996;75:314–25. doi: 10.1016/s0022-3913(96)90491-6. [DOI] [PubMed] [Google Scholar]
- 18.Sorensen JA, Strutz JM, Avera SP, Materdomini D. Marginal fidelity and microleakage of porcelain veneers made by two techniques. J Prosthet Dent. 1992;67:16–22. doi: 10.1016/0022-3913(92)90040-h. [DOI] [PubMed] [Google Scholar]
- 19.Sim C, Ibbetson R. Comparison of fit of porcelain veneers fabricated using different techniques. Int J Prosthodont. 1993;6:36–42. [PubMed] [Google Scholar]
- 20.Wall JG, Reisbick MH, Espeleta KG. Cement luting thickness beneath porcelain veneers made on platinum foil. J Prosthet Dent. 1992;68:448–50. doi: 10.1016/0022-3913(92)90408-3. [DOI] [PubMed] [Google Scholar]
- 21.Lim C, Ironside JG. Grit blasting and the marginal accuracy of two ceramic veneer systems - A pilot study. J Prosthet Dent. 1997;77:359–64. doi: 10.1016/s0022-3913(97)70159-8. [DOI] [PubMed] [Google Scholar]
- 22.Hilgert E, Nesser M. Evaluation of the marginal adaptation of ceramic copings in function of the cervical endings and treatment of the internal surfaces. Cienc Odontol Bras 2003 out./dez. 6:9–16. [Google Scholar]
- 23.Groten M, Axmann D, Probster L. Determination of the minimum number of marginal gap measurements required for practical in vitro testing. J Prosthet Dent. 2006;95:315–22. doi: 10.1016/s0022-3913(00)70087-4. [DOI] [PubMed] [Google Scholar]
- 24.Nakamura T, Nonaka M, Maruyama T. In vitro fitting accuracy of copy-milled alumina cores and all-ceramic crowns. Int J Prosthodont. 2000;13:189–93. [PubMed] [Google Scholar]
- 25.Tinschert J, Natt G, Mautsch W, Spiekermann H, Anusavice KJ. Marginal fit of alumina-and zirconia-based fixed partial dentures produced by a CAD/CAM system. Oper Dent. 2001;26:367–74. [PubMed] [Google Scholar]
- 26.Ferrari M, Patroni S, Balleri P. Measurement of enamel thickness in relation to reduction for etched laminate veneers. Int J Periodontics Restorative Dent. 1992;12:407–13. [PubMed] [Google Scholar]
- 27.Eick JD, Miller RG, Robinson SJ, Bowles CQ, Gutshall PL, Chappelow CC. Quantitative analysis of the dentin adhesive interface by Auger spectroscopy. J Dent Res. 1996;75:1027–33. doi: 10.1177/00220345960750040501. [DOI] [PubMed] [Google Scholar]
- 28.Belser UC, MacEntee MI, Richter WA. Fit of three porcelain-fused-to-metal marginal designs in vivo: A scanning electron microscope study. J Prosthet Dent. 1985;53:24–9. doi: 10.1016/0022-3913(85)90058-7. [DOI] [PubMed] [Google Scholar]
- 29.Beschnidt SM, Strub JR. Evaluation of the marginal accuracy of different all-ceramic crown systems after simulation in the artificial mouth. J Oral Rehabil. 1999;26:582–93. doi: 10.1046/j.1365-2842.1999.00449.x. [DOI] [PubMed] [Google Scholar]
- 30.Sorensen JA. A standardized method for determination of crown margin fidelity. J Prosthet Dent. 1990;64:18–24. doi: 10.1016/0022-3913(90)90147-5. [DOI] [PubMed] [Google Scholar]