

Abstract
Double free-flaps are necessary when tissue cover cannot be sufficed with a single flap. The other factors to be considered when using two free flaps for resurfacing of distal limb defects are the availability of more than one recipient vessel, the risk of distal limb ischaemia and the donor site morbidity of double flap harvest. If these factors are adequately addressed, double free-flaps can be safely executed for resurfacing distal limb defects with minimal morbidity. We report the simultaneous harvest and transfer of the anterolateral and anteromedial thigh flaps inset and vascularised as double free-flaps to resurface a large bimalleolar defect in a 14-year-old boy with no additional morbidity as compared to that of a single free tissue transfer.
Keywords: Bimalleolar defect, double free-flap, distal limb defects
INTRODUCTION
Double free-flaps are technically challenging due to the complex nature of the defect, harvest of two flaps and use of two pairs of recipient's vessels. In such limb defects more than one recipient vessel is necessary when end to side anastomosis is not feasible. Further the risk of distal limb ischaemia is imminent when collateral circulation is not adequate. Harvest of second free flap is an additional morbidity. Double fasciocutanous flaps either perfused independently or as chimeric flaps fulfil the requirements provided suitable recipient vessels are available. The risk of distal limb ischaemia is minimal when a single vascular axial limb vessel is used as the recipient. Harvest of such flaps from a common donor site avoids the morbidity of distant second donor site. The lateral circumflex femoral system is one such potential donor area. We report successful resurfacing of large bimalleolar defects in a 14-year-old boy using the anterolateral and anteromedial fasciocutanous perforator flaps harvested independently and anastomosed to the proximal and distal cut ends of the anterior tibial vessels.
CASE REPORT
A 14-year-old boy presented to us with a 2 weeks old infected bimalleolar defect with dimensions of 12 cm × 7 cm medially and 8 cm × 4 cm laterally [Figure 1] at the ankle. The patient was treated with cast application elsewhere for swelling of the ankle following a fall and had no bony injury. He developed severe pain in the ankle soon after and fever a week later,. On removal of the cast, necrosis of the skin was noted over the both malleoli which was debrided at the referral hospital and then he was referred to our institute for further management. Malleoli and the adjacent lower ends of tibia and fibula were exposed with open ankle joint-draining frank pus. The foot was sensate and well vascularised with good dorsalis pedis and posterior tibial pulsations. After containment of purulent discharge, flap cover was planned. Considering the dimensions and proximity of the two defects, a chimeric fasciocutanous anteromedial thigh (AMT) and anterolateral thigh (ALT) flap [Figure 2] based on the lateral circumflex, femoral vessels was planned and their perforators marked with hand held Doppler. The flaps were raised based on these perforators and the pedicles traced proximally for their confluence. It was found to be very close to the origin of the lateral circumflex femoral artery precluding chimeric flap design and due to gross vessel size mismatch and excess pedicle length. The second team explored the anterior tibial artery and both vena comitans. The vessels were healthy and amenable for the use with good pulsatile flow from both the proximal and distal cut ends of the recipient artery. Both the flaps were harvested independently with adequate pedicle length. Both flap vessels were anstomosed to the proximal and distal cut ends of the anterior tibial artery, in an end to end fashion. The corresponding flap veins were anastomosed to the available two vena comitans of the anterior tibial artery in an antegrade direction. Both the flaps survived without any complications [Figure 3]. At 11 months follow-up, the patient is ambulatory with a stiff ankle in slight varus position with X-ray showing extensive post-septic arthritic sequale of the ankle joint [Figure 4].
Figure 1.

Medial and lateral malleolar defect
Figure 2.
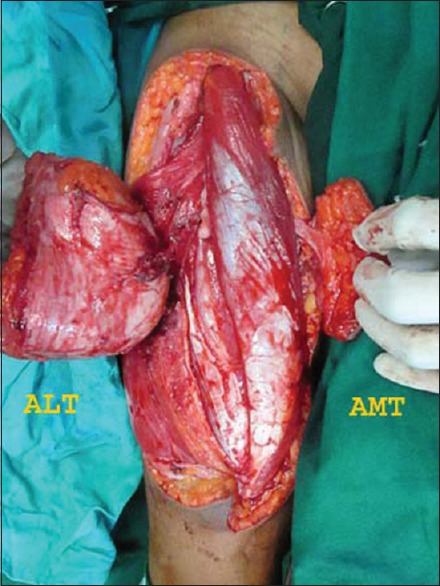
Chimeric anterolateral thigh and anteromedial thigh flaps
Figure 3.

Settled anterolateral thigh and anteromedial thigh flaps
Figure 4.

X-ray showing post arthritic sequele
DISCUSSION
Distal lower limb defects requiring double flaps can be resurfaced by a combination of two separate distally based flaps laterally and medially,[1] a single pedicled flap with de-epithelisation of intervening skin bridge[2] and use of chimeric free flaps.[3] Double free-flaps have not been popular for reconstructing the limb defects.[4]
Chimeric free flaps resurface more than one defect based on single pedicle by innovation in the flap design. Lin et al. have demonstrated the feasibility of harvesting more than one skin and muscle components on the lateral circumflex femoral system.[3] Two separate skin paddles based on the anterolateral and anteromedial perforators of the descending branch of the lateral circumflex femoral artery can be harvested as a chimeric flap.[5] However, the pedicle of the AMT flap can arise from the lateral circumflex femoral artery or the femoral artery.[6] When the chimeric anterolateral and anteromedial flap is harvested in such circumstances, the confluence would be in a much more proximal position which was the case in our patient. Routine imaging has not been advocated for the harvest of these flaps by[7] However, when chimeric flap harvest is planned, imaging can be helpful in assessing the location of the confluence. The harvest of both the flaps did not incur additional morbidity in our case though the potential exists.
Lin et al. in their preference for choosing chimeric flaps over double free-flaps have observed the following difficulties in advocating double free-flaps for limb defects namely, (1) the need for more than one pair of recipient vessels or a flow-through flap (2) morbidity of the second flap harvest and (3) the additional time for second anastomosis.[3]
The choice of the recipient vessel for a free flap in the limb will depend on the location and the vascular status of the limb.[8] Collateral circulation maintains distal limb perfusion and hence its intactness and adequacy are vital when one of the major limb axial vessels is utilised. This is all the more crucial when more than one recipient vessel is needed. Reverse flow from a vessel has been utilised to perfuse free flaps.[8] This is possible because of presence of collaterals at multiple levels between the anterior tibial, posterior tibial and peroneal vessels. In 3 of the 50 cases of Park et al. reverse flow from anterior tibial was used as the recipient vessel, and they suggested angiography and pulsatile flow intra-op to be usable criteria for the vessel. Thus, if both the proximal and distal cut ends have good flow, they can be utilised for perfusion of two flaps assuming that collateral circulation is adequate.
Both superficial and deep veins in the lower limb can be used for venous anastomosis. Park et al. have found the vena comitans to be better suited than superficial veins as they are less vulnerable to injury and located in the same operative field.[8] We also used the vena comitans for the same reasons in our case.
The end to side technique avoids sacrifice of the vessel. Even though patency rates are similar to that of an end to end anastomosis, it has technical difficulties (angle of vessel take off, arteriotomy, difficulty in diseased vessels) and flow problems (turbulence, insufficient flow, thrombosis).[9,10] Although it gives a safer and more satisfactory outcome in size discrepancy,[9] it is not feasible when flap vessel is larger than the recipient vessel which was the situation in our case.
Thus, in a properly selected patient double free-flaps can be done safely with minimal additional morbidity as demonstrated in this case.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Liu L, Zou L, Cao X, Cai J. Two different flaps for reconstruction of gunshot wounds to the foot and ankle in a child. J Pediatr Surg. 2012;47:E13–7. doi: 10.1016/j.jpedsurg.2012.03.084. [DOI] [PubMed] [Google Scholar]
- 2.Caddick JF, Peach H, Burge TS. Distally based double paddle fasciocutaneous island flap following lower limb trauma. Br J Plast Surg. 2003;56:712–4. doi: 10.1016/s0007-1226(03)00357-6. [DOI] [PubMed] [Google Scholar]
- 3.Lin YT, Lin CH, Wei FC. More degrees of freedom by using chimeric concept in the applications of anterolateral thigh flap. J Plast Reconstr Aesthet Surg. 2006;59:622–7. doi: 10.1016/j.bjps.2005.07.015. [DOI] [PubMed] [Google Scholar]
- 4.Hwang KT, Kim YH. Double skin perforator flaps for aesthetic resurfacing of extensive limb defects. J Plast Reconstr Aesthet Surg. 2015;68:e47–9. doi: 10.1016/j.bjps.2014.10.051. [DOI] [PubMed] [Google Scholar]
- 5.Wang WH, Deng JY, Xu B, Zhu J, Xia B, Zhang BJ. Double anterior (anterolateral and anteromedial) thigh flap for oral perforated defect reconstruction. J Craniomaxillofac Surg. 2014;42:2041–4. doi: 10.1016/j.jcms.2014.09.011. [DOI] [PubMed] [Google Scholar]
- 6.Cigna E, Chen HC, Ozkan O, Sorvillo V, Maruccia M, Ribuffo D. The anteromedial thigh free flap anatomy: A clinical, anatomical, and cadaveric study. Plast Reconstr Surg. 2014;133:420–9. doi: 10.1097/01.prs.0000437258.85951.a1. [DOI] [PubMed] [Google Scholar]
- 7.Riva FM, Tan NC, Liu KW, Hsieh CH, Jeng SF. Anteromedial thigh perforator free flap: Report of 41 consecutive flaps and donor-site morbidity evaluation. J Plast Reconstr Aesthet Surg. 2013;66:1405–14. doi: 10.1016/j.bjps.2013.06.012. [DOI] [PubMed] [Google Scholar]
- 8.Park S, Han SH, Lee TJ. Algorithm for recipient vessel selection in free tissue transfer to the lower extremity. Plast Reconstr Surg. 1999;103:1937–48. doi: 10.1097/00006534-199906000-00019. [DOI] [PubMed] [Google Scholar]
- 9.Tsai YT, Lin TS. The suitability of end-to-side microvascular anastomosis in free flap transfer for limb reconstruction. Ann Plast Surg. 2012;68:171–4. doi: 10.1097/SAP.0b013e3182275cf8. [DOI] [PubMed] [Google Scholar]
- 10.Kim JT, Kim CY, Kim YH. T-anastomosis in microsurgical free flap reconstruction: An overview of clinical applications. J Plast Reconstr Aesthet Surg. 2008;61:1157–63. doi: 10.1016/j.bjps.2008.03.048. [DOI] [PubMed] [Google Scholar]