

Abstract
Gastrointestinal duplication cyst is a rare congenital anomaly that may occur anywhere along the gastrointestinal tract from the tongue to the anus. Such cysts occur most commonly in the small bowel and about half are in the mesenteric border of the ileum. Such cystic duplications communicate only rarely with the intestinal lumen although the cysts are attached to the intestine and may even share a common wall with the adjacent alimentary tract. These lesions can vary in shape, being cystic or tubular, and often show the same structure of the adjacent normal bowel. It is usually asymptomatic and complications are rare but they may include obstruction by volvulus or intussusception, bleeding, infection, and perforation. When diagnosed these lesions should be surgically resected to avoid future possible complications. The authors present a case of enteric cystic duplication and its ultrasound appearance in a 12-month-old Caucasian female infant cause of acute abdominal pain and intestinal obstruction, thus requiring urgent surgery.
Keywords: Gastrointestinal duplication cyst, Ultrasound, Gut signature, Duplicazione digestiva cistica, Ecografia, Segno dell’intestino
Riassunto
La duplicazione digestiva è una rara anomalia congenita che può essere localizzata in ogni tratto del canale digestivo, dalla base della lingua all’ano. Si riconoscono più comunemente nel piccolo intestino e circa la metà sono a localizzazione ileale. Comunicano solo raramente con il lume intestinale spesso stabilendo intimo contatto con il canale alimentare adiacente con condivisione di parete. Può mostrare forma cistica o tubolare e tipicamente mostra la stessa struttura delle viscere normale adiacente. Di solito è asintomatica e le complicanze sono rare ma possono includere occlusione da volvolo o da invaginazione, emorragie, infezioni, e perforazione. Quando diagnosticata, questa lesione deve essere asportata chirurgicamente per evitare in futuro possibili complicazioni. Gli Autori presentano un caso di duplicazione di tipo cistico dell’ileo terminale e le sue caratteristiche ecografiche osservate in una infante di 12 mesi giunta alla nostra attenzione con dolore addominale acuto ed occlusione intestinale, che ha richiesto successivo intervento chirurgico in regime di urgenza.
Introduction
Intestinal duplications are rare congenital anomalies that can occur anywhere in the gastrointestinal tract. Duplication cysts most commonly occur in the distal ileum followed by the esophagus, colon, jejunum, stomach and duodenum. Typically, the duplication cyst is attached to the gastrointestinal tract, has smooth muscle in its wall and is lined with gastrointestinal epithelium [1, 2].
The authors present a case of enteric cystic duplication and its ultrasound appearance in a 12-month-old Caucasian, female infant. The cystic duplication is the cause of her acute abdominal pain and intestinal obstruction, prompting the need for urgent surgery.
Description of the case
A 12-month-old, Caucasian, female infant was admitted to the Pediatric Emergency Department with palpable swelling of the abdomen in the right paramedian side and a clinical picture of abdominal pain and bowel obstruction. The clinical examination revealed pain and tenderness around the periumbilical right paramedian area and a semi-mobile palpable mass in the lower abdomen. The infant presented as a healthy baby with timely achievement of the appropriate neurodevelopmental milestones and no significant medical history. She was referred to the Emergency Radiology Department for an ultrasound of the abdomen. The ultrasound (US) examination was performed with high frequency (10–15 MHz) linear probes (Logiq E9 GE) at the virtual convex setting typically adopted for infant patients. The US examination revealed that, over the bladder on the median/right paramedian side, there was a hypo-anechoic, round mass with contextual particulate matter and slightly thickened walls with a layered appearance: the so-called “gut signature.” The mass measured 60 × 38 mm in diameter and appeared to be strongly adherent to the last ileal loop, causing compressive phenomena on the digestive structure (Fig. 1). Given its location and ultrasound characteristics, the diagnosis deposed to the cystic duplication of the terminal ileum. The operating table subsequently obtained a confirmation of this (Fig. 2). The patient is continuing to do well and is currently undergoing outpatient follow-up with our pediatric surgeons.
Fig. 1.

High linear (10–15) MHz frequency probes with virtual convex setting. The cystic mass (C) measures 60 by 38 mm in diameter. Portions of the cyst wall show the characteristic double-layered appearance with echogenic mucosa internally (arrows) and hypoechoic muscle externally
Fig. 2.
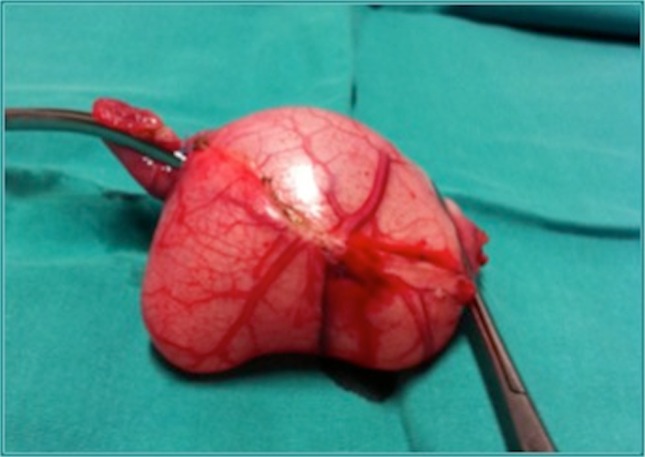
The surgical specimen shows the enteric duplication cyst
Discussion
The term “digestive duplications” refers to cystic or tubular formations in intimate contact with the various segments of the alimentary canal. They can be located anywhere between the base of the tongue and the anus. In 1937, Ladd et al. proposed the term “intestinal duplication” in an attempt to bring together under one condition all the previously used definitions, including “enterogenous cysts,” “enteric cysts,” “dual ileus,” “giant diverticula” and “abnormal Meckel’s diverticula” [3].
Many hypotheses have been proposed to explain the embryogenesis of intestinal duplication, but the precise mechanism remains to be elucidated. Some authors proposed a theory that is considered the most plausible theory for the origin of duplications: the abnormal recanalization hypothesis. They recalled that, in an embryo about 6 weeks old, the rapid proliferation of epithelial cells may completely occlude the lumen of portions of the intestinal tract [4]. Vacuoles begin to appear in this cell mass as the intestinal tract grows in length. After these spaces form, they coalesce and usually arrange themselves into longitudinal rows, parallel to the long axis of the bowel. Eventually, all such isolated vacuoles, of whatever size or shape, join one another to produce the normal lumen of the intestine [1, 4]. It is also evident how one or more connections (or even none) may occur between the bowel and its duplicate [4]. A duplication develops all muscle layers of the intestinal tract and may possess a common wall with the bowel or hang free on its own mesentery. It is also apparent that a duplication may assume a wide variety of shapes and sizes and may be located anywhere along the alimentary tract [4]. Other hypotheses include the persistent embryologic diverticular theory, bronchopulmonary-foregut malformation, the intrauterine vascular accident theory and the abortive twinning theory [1]. The most notable features of a duplication include a microscopic structure that bears a striking resemblance to a normal bowel with mucosa, one or several muscle layers and often a well-defined serosa. Each is lined with a mucosa, similar to a portion of the alimentary tract (unless ulceration or necrosis has occurred). Those lesions that are contiguous with a portion of the intestinal tract share a common wall in which interlacing muscles are present [4]. There are two general types of gastrointestinal duplication cyst: cystic duplications, which account for approximately 80 % of the cases, are spherical in shape and have no communication with the bowel lumen, and tubular duplications, which account for approximately 20 % of the cases and communicate directly with the bowel lumen [1]. They contain a clear mucoid substance that is secreted from the mucosa itself, sometimes hemorrhagic due to ectopic gastric mucosal ulceration [3]. Most gastrointestinal duplication cysts manifest during the first year of life [1]. Clinically, a duplication cyst may present as an asymptomatic mass or with an occlusive framework (intussusception or volvulus). Bleeding and melena are rare symptoms because the duplication cysts do not communicate with the adjacent bowel [3]. The tubular duplications are often ulcerated, especially downstream of the junction with the normal intestine (peptic ulcer). Clinically, they present with abdominal pain and melena. A long, distally closed tubular duplication can simulate chylous ascites [3]. Surgical excision is the treatment of choice because malignant tumors may develop from the mucosa [1]. Most authors recommend complete resection once duplication has been identified in order to avoid further complications or to correct such complications. Sometimes the resection of the normal intestine must accompany the removal of the duplication because of the intimate attachment of the common wall or because isolated resection would compromise blood flow to the adjacent bowel. However, it is generally easy to remove cystic duplications from their attachments to the surrounding tissues [1, 5]. US plays a critical role in the evaluation of duplication cysts [1]. Classic duplication cysts have a characteristic appearance on the ultrasound: that of the double layered wall, the so called “gut signature,” as in our case (Fig. 1). The inner layer is hyperechoic mucosa and the outer layer is hypoechoic muscle. Unfortunately, with inflammation, the layers may be obscured, lessening the specificity. Nonetheless, the demonstration of a cystic mass adjacent to the bowel should prompt the consideration of a duplication cyst [6].
Classically, children present with the cyst in early childhood as it distends with fluid. If gastric mucosa is present within the cyst, it may secrete enzymes, leading to inflammation and presentation with pain. Differential considerations for a fluid-filled cystic mass in the lower abdomen include omental or mesenteric cysts and ovarian neoplasm. Omental and mesenteric cysts are usually asymptomatic unto themselves unless there is an associated obstruction or torsion of the bowel [6]. However, the double-wall sign may be seen with other cystic lesions. This finding can be misleading [1]. Computed Tomography (CT) typically is not performed to evaluate a duplication cyst, but it may depict the location and extent of the cyst, as well as complications and other associated anomalies. At CT, a gastrointestinal duplication cyst manifests as a fluid-filled cystic mass with a thick, slightly enhancing wall that either arises from or is extrinsic to the gastrointestinal wall [1]. In conclusion, ultrasound plays a crucial role in the diagnosis of intestinal duplication because it identifies the cyst and its anatomical location and also allows us to identify the typical wall layers or “gut signature.” However, in some cases, this sign may not be detectable or, conversely, cysts of other geneses (such as ovarian cysts, Meckel’s diverticula and mesenteric cysts) may present a layered wall that simulates the sign. Despite these potential pitfalls, the presence of a bi-layered parietal cystic appearance is highly suggestive of intestinal duplication.
Compliance with ethical standards
Conflict of interest
Marco Di Serafino, Carmela Mercogliano and Gianfranco Vallone declare that they have no conflict of interest.
Informed consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, and its late amendments. Additional informed consented was obtained from all patients for which identifying information is not included in this article.
Human and animal rights
This article does not contain any studies with human or animal subjects performed by any of the authors.
References
- 1.Lee NK, et al. Complications of congenital and developmental abnormalities of the gastrointestinal tract in adolescents and adults: evaluation with multimodality imaging. RadioGraphics. 2010;30(6):1489–1507. doi: 10.1148/rg.306105504. [DOI] [PubMed] [Google Scholar]
- 2.Park JY, et al. A completely isolated intestinal duplication cyst mimicking ovarian cyst torsion in an adult. World J Gastroenterol. 2014;20(2):603–606. doi: 10.3748/wjg.v20.i2.603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Spinelli C. Chirurgia Neonatale Delle Malformazioni Dell’intestino Primitivo Di Maggiore Incidenza. Padova: PICCIN; 2001. [Google Scholar]
- 4.Gross RE, Holcomb GW, Jr, Farber S. Duplication of the alimentary tract. Pediatrics. 1952;9:449–468. [PubMed] [Google Scholar]
- 5.Cavallaro G, et al. Cystic duplication of transverse colon: an unusual case of abdominal pain and bowel obstruction. G Chir. 2010;31(5):236–238. [PubMed] [Google Scholar]
- 6.Strouse P. Sonographic evaluation of the child with lower abdominal or pelvic pain. Radiol Clin N Am. 2006;44(6):911–923. doi: 10.1016/j.rcl.2006.10.019. [DOI] [PubMed] [Google Scholar]