

Abstract
Background
Major outbreaks of hand, foot and mouth disease (HFMD) have been reported in China since 2008, posing a great threat to the health of children. Although many studies have examined the effect of meteorological variables on the incidence of HFMD, the results have been inconsistent. This study aimed to quantify the relationship between meteorological factors and HFMD occurrence in different climates of mainland China using spatial panel data models.
Methods
All statistical analyses were carried out according to different climate types. We firstly conducted a descriptive analysis to summarize the epidemic characteristics of HFMD from May 2008 to November 2012 and then detected the spatial autocorrelation of HFMD using a global autocorrelation statistic (Moran’s I) in each month. Finally, the association between HFMD incidence and meteorological factors was explored by spatial panel data models.
Results
The 353 regions were divided into 4 groups according to climate (G1: subtropical monsoon climate; G2: temperate monsoon climate; G3: temperate continental climate; G4: plateau mountain climate). The Moran’s I values were significant with high correlations in most months of group G1 and G2 and some months of group G3 and G4. This suggested the existence of a high spatial autocorrelation with HFMD. Spatial panel data models were more appropriate to describe the data than fixed effect models. The results showed that HFMD incidences were significantly associated with average atmospheric pressure (AAP), average temperature (AT), average vapor pressure (AVP), average relative humidity (ARH), monthly precipitation (MP), average wind speed (AWS), monthly total sunshine hours (MSH), mean temperature difference (MTD), rain day (RD) and average temperature distance (ATD), but the effect of meteorological factors might differ in various climate types.
Conclusions
Spatial panel data models are useful and effective when longitudinal data are available and spatial autocorrelation exists. Our findings showed that meteorological factors were related to the occurrence of HFMD, which were also affected by climate type.
Keywords: Hand, foot and mouth disease; Spatial panel data model; Meteorological factors; Climate type
Background
Hand, foot and mouth disease (HFMD) is a common infectious disease, which is mainly caused by the enteroviruses coxsackie A16 and enterovirus 71 [1]. In most cases, the disease is mild and self-limiting, but sometimes serious neurological and cardiopulmonary complications may occur, particularly among those aged 5 years and younger [2]. HFMD was listed as a notifiable Class-C communicable disease since May 2008 [3]. In recent years, the trend of HFMD outbreaks has increased among children in China, which is regarded as an important public health problem [4, 5].
Many studies have been performed to analyze the association between meteorological factors and HFMD, but the results have been inconsistent. It has been found that temperature and relative humidity were positively associated with HFMD in most studies [6–11], whereas studies in Japan found that the number of days per week with an average temperature above 25°C was negatively associated with HFMD incidence [12]. Wind velocity was found to be positively associated with HFMD in Ma [13] and Li’s studies [13], but in Huang’s publication [8], no relationship was found between wind speed and HFMD. Furthermore, Wang [10] found a negative association. Other possible risk factors (total sunshine, difference in temperature, atmospheric pressure, vapor pressure, etc.) were examined in a few studies and require further research.
Most previous studies have not considered temporal or spatial effects (Multiple Linear Regression Model [13]/Negative Binomial Regression [14]/Generalized Additive Poisson Model [15]), or merely focused on the spatial dimension (Geographically Weighted Regression Models (GWR) [16]) or on time dimension (time-series analysis [8]) approaches, which might cause loss of information by ignoring the heterogeneity in both time and space and result in different conclusions.
Compared to traditional methods on the basis of time-series or cross-sectional data alone, spatial panel data models can control for both spatial dependency and unknown heterogeneity [17, 18]. In this study, spatial panel data models were used to explore the relationship between meteorological variables and HFMD incidence in 353 regions of mainland China according to climate types.
Methods
Data collection
Study area
Thirty-one provinces of mainland China were divided into 353 regions in this study. There were four main types of climate in mainland China. All the data were grouped by climate types, as shown in Fig. 1: subtropical monsoon climate (SMC, G1), temperate monsoon climate (TMC, G2), temperate continental climate (TCC, G3) and plateau mountain climate (PMC, G4).
Fig. 1.
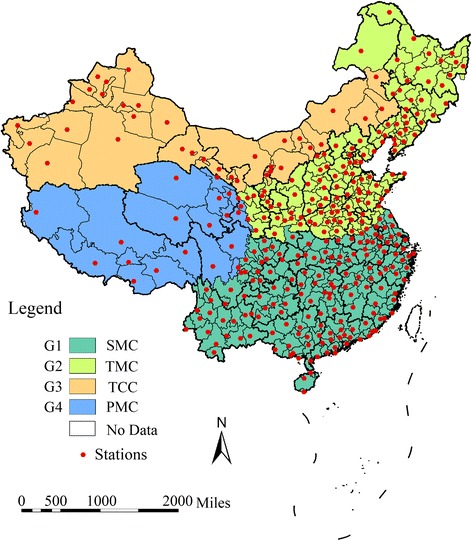
Climate types distribution and locations of meteorological monitoring stations in mainland China. SMC (Group 1, G1): subtropical monsoon climate; TMC (Group 2, G2): temperate monsoon climate; TCC (Group 3, G3): temperate continental climate; PMC (Group 4, G4): and plateau mountain climate
Surveillance data of HFMD
Data of monthly reported HFMD cases in each region in mainland China from May 2008 to November 2012 were obtained from the National Center for Public Health Surveillance and Information Services, at the China Center for Disease Control and Prevention (China CDC). All cases were diagnosed according to the clinical criteria provided in a guidebook published by the National Health and Family Planning Commission of the People’s Republic of China in 2008 [19]: with or without fever, a probable case of HFMD was defined as a patient with a papular or vesicular rash on or in the hands, feet, mouth, and/or buttocks. A confirmed case was defined as a probable case with laboratory evidence of enterovirus infection. The demographic data for each region were obtained from the National Bureau of Statistics of China [20]. The ethical approval and the consent from each individual subject was not required because we used only aggregated data (number of cases for each county in months) but not any individualized data in this study.
Meteorological data
Meteorological data from 328 monitoring stations that were nearest to the centers of 353 regions were obtained from the China Meteorological Data Sharing Service System (http://cdc.nmic.cn/home.do), which was publicly accessible. Monthly meteorological variables in this study included average atmospheric pressure (AAP), average temperature (AT), average vapor pressure (AVP), average relative humidity (ARH), monthly precipitation (MP), average wind speed (AWS), monthly total sunshine hours (MSH), mean temperature difference (MTD), monthly rainfall days (MRD), and average temperature distance (ATD).
Statistical analysis
Global spatial autocorrelation analysis
The autocorrelation statistic (global Moran’s I) [21] was used to detect the global spatial autocorrelation of reported HFMD incidences in the study area by climate types. The significance of Moran’s I was assessed by employing Monte Carlo randomization. A higher positive Moran’s I value with a statistically significant p-value (P < 0.05) indicates that the values of neighboring areas tend to cluster [22]. ArcGIS 10.1 (ESRI Inc. Redlands, CA, USA) was used to perform the analysis.
Spatial panel data models
Spatial panel data typically refer to data containing continuous observations of a number of spatial units. Spatial panel models, which could address data with spatial dependence and also enable researchers to consider spatial and/or temporal heterogeneity, were used to examine the role of different meteorological factors in this study. Spatial panel data models are more informative and contain more variation and less collinearity between the variables compared with cross-sectional or time series models [17].
The basic form of the simple panel data model with a spatial and temporal specific effect is:
where i and t are indices for the cross-sectional dimension (spatial units) and time dimension (time periods), respectively; yit is the dependent variable at i and t; Xit is the group of explanatory variables; β is the vector of regression coefficients that explains the relationship between Xit and yit; εit is an independently and identically distributed error term with zero mean and variance σ2; μi denotes a spatial specific effect and γt represents temporal specific effects. The spatial and/or temporal specific effects may be treated as fixed effects or random effects. A random effect is appropriate if a certain number of individuals is randomly sampled from a large population. The fixed effect model is favored [23–25] when the regression analysis is applied to a precise set of regions. For this reason, because our data contained all regions of the study area, we established fixed effects panel data models that included spatial error autocorrelation or a spatially lagged dependent variable. We also compared the random effects specification against fixed effects specification by Housman’s specification test [26, 27], which suggested that fixed effect specification was more appropriate.
The simple panel data models with specific effects can be extended to the spatial lag (including spatially lagged dependent variables) and the spatial error model (including spatial error autocorrelation terms). The dependent variable in the spatial lag model depends on the dependent variable observed in neighboring units [17]. The spatial lag model with spatial and temporal fixed effects could be specified as follows [28]:
The spatial error model assumed that the effect of spatial correlation is a representation of the ignored variable. The model with spatial and temporal fixed effects could be specified as below [28]:
where W is an N × N positive non-stochastic spatial weight matrix; ρ is the spatial autoregressive coefficient and λ is usually called the spatial autocorrelation coefficient.
Likelihood ratio (LR) tests were used to determine the spatial and/or time-period fixed effects in the extension of the model. The Lagrange multiplier (LM) and robust Lagrange multiplier (robust LM) test were used to determine whether the spatial lag model and/or the spatial error model are more appropriate than a simple panel data model to describe the data. The spatial error model is more appropriate if the LM error is more significant than the LM lag and the robust LM error test is significant and the robust LM lag is not significant and vice versa. R2 and log-likelihood were the commonly used effective criteria to evaluate the model [29–31]. Matlab R2014a (Mathworks Inc., Natick, MA, USA) was used to perform the analysis of the spatial panel data models, LR, and LM tests.
Results
Basic description
A total of 7,061,525 HFMD cases were reported in 353 regions of mainland China from May 2008 to November 2012. The number of cases of HFMD per month ranged from 0 to 11,730 in each region. The number of reported cases for each month is shown in Fig. 2, which indicates a potential seasonality of the incidence of HFMD, since more cases occurred in April-July.
Fig. 2.
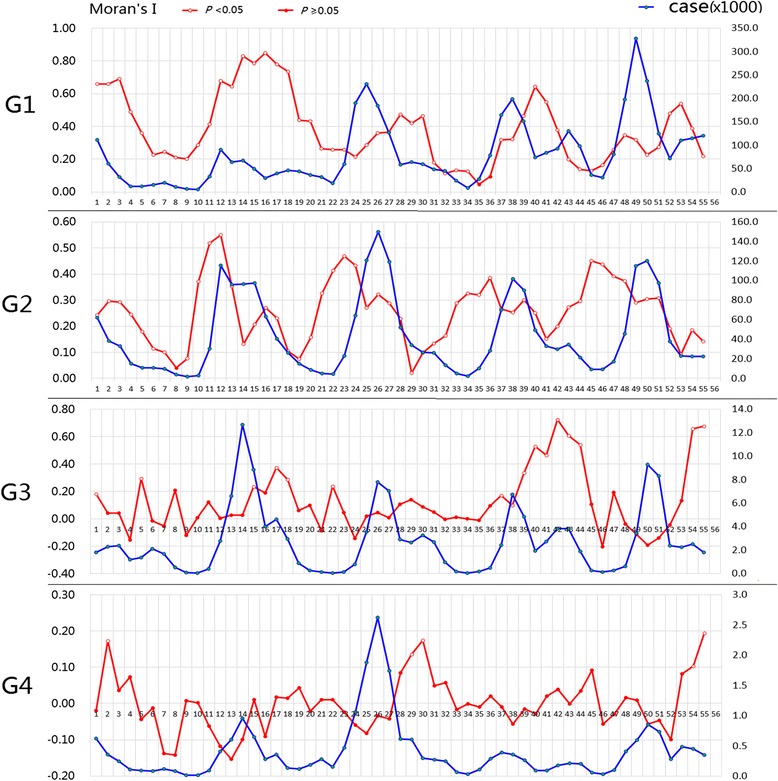
The number of reported cases and Moran’I indices (the spatial autocorrelation tests) for each month in different groups
Spatial autocorrelation of HFMD incidence
The spatial autocorrelation test for each month is shown in Fig. 2. The figure demonstrates that a high global spatial autocorrelation of HFMD was detected at the regional level in mainland China within each epidemic month during May 2008 to November 2012 in group G1 (Moran’s I from 0.046 to 0.848) and group G2 (Moran’s I from 0.020 to 0.550). In group G3 and group G4, the global Moran’s I value was only significant in some months. Because of the existence of a high spatial dependency on the occurrence of HFMD, a spatial autocorrelation should be included in the regression model and thus, the panel data models were more appropriate.
Spatial panel data models
Logarithmic transformation of the reported incidence was used due to the distribution of the reported disease incidence having a non-normal distribution. Because of some zeroes in the dependent variable, we assumed that there were 0.5 cases in the zones with no reported cases before calculating the incidence and the logarithmic transformation. Table 1 shows the basic descriptive statistics for meteorological variables and dependent variables (logarithmic transformation of the reported incidence) in each group.
Table 1.
Descriptive statistics for meteorological variables and dependent variables (Y)
| variables | G1 (172 regions) | G2 (127 regions) | G3 (34 regions) | G4 (20 regions) | ||||
|---|---|---|---|---|---|---|---|---|
| Mean(SD) | Median (interquartile range) | Mean(SD) | Median (interquartile range) | Mean(SD) | Median (interquartile range) | Mean(SD) | Median (interquartile range) | |
| Y | −4.36(0.71) | −4.28(−4.77,-3.85) | −4.65(0.83) | −4.52(−5.17,-4.03) | −5.02(1.00) | −4.88(−5.74,-4.23) | −5.34(0.71) | −5.52(−5.89,-4.89) |
| AAP | 974.27(63.13) | 999.80(969.60,1009.70) | 972.14(57.44) | 996.50(956.05,1009.50) | 895.15(53.07) | 889.65(858.90,933.03) | 695.40(87.98) | 685.25(625.55,729.80) |
| AT | 18.83(7.74) | 20.15(12.70,25.40) | 11.28(11.83) | 14.00(2.35,21.3) | 8.99(12.90) | 11.30(−2.30,20.30) | 5.83(8.74) | 7.00(−0.68,12.80) |
| AVP | 17.62(7.95) | 17.00(10.50,24.60) | 10.92(7.79) | 9.10(4.10,17.00) | 6.44(4.33) | 5.50(2.60,9.90) | 5.85(4.50) | 4.80(2.10,8.48) |
| ARH | 74.22(8.35) | 75.00(70.00,80.00) | 63.18(12.93) | 64.00(54.00,73.00) | 48.93(14.04) | 48.00(38.00,59.00) | 53.05(17.99) | 56.00(39.00,67.00) |
| MP | 115.57(116.65) | 83.60(33.20,161.68) | 55.37(68.67) | 30.70(9.00,77.30) | 17.38(26.82) | 6.95(1.10,22.13) | 46.20(64.02) | 23.95(2.5,71.08) |
| AWS | 1.94(0.86) | 1.80(1.30,2.30) | 2.24(0.91) | 2.10(1.70,2.60) | 2.24(0.78) | 2.10(1.70,2.70) | 1.87(0.82) | 1.70(1.30,2.20) |
| MSH | 139.12(60.42) | 136.90(95.10,182.80) | 189.24(51.18) | 190.20(155.20,224.70) | 246.24(59.85) | 250.80(209.38,290.75) | 212.39(55.90) | 217.55(183.95,248.83) |
| MTD | 7.92(2.14) | 7.70(6.60,9.00) | 10.38(2.39) | 10.30(8.60,11.90) | 12.88(2.42) | 12.90(11.40,14.40) | 13.43(3.07) | 13.50(11.60,15.48) |
| RD | 11.57(5.38) | 11.00(8.00,15.75) | 7.33(4.48) | 7.00(4.00,10.00) | 4.95(4.08) | 4.00(2.00,7.00) | 10.47(7.97) | 9.00(3.00,17.00) |
| ATD | 0.47(1.36) | 0.50(−0.30,1.2) | 0.37(1.49) | 0.40(−0.40,1.30) | 0.70(1.78) | 0.90(−0.20,1.90) | 0.96(1.20) | 0.95(0.30,1.70) |
Table 2 shows the results to determine which specific fixed effect and which type of spatial dependency term should be included in the model for each group. The LR tests showed that the extension of the model with both spatial and time-period fixed effects was more suitable (P < 0.001). LM and robust LM test results demonstrated that the spatial lag models were more appropriate than the spatial error models. Overall, the test results implied that the spatial lagged model with spatial and time-period fixed effects was more appropriate to process the data.
Table 2.
Results of tests to determine specific fixed effects and spatial dependency terms for each group
| Type of test | G1 | G2 | G3 | G4 | |
|---|---|---|---|---|---|
| LR_tests of fixed effects | Spatial fixed effects | 6732.35** | 2607.12** | 2021.77** | 415.62** |
| Temporal fixed effects | 7461.23** | 2729.13** | 753.29** | 309.58** | |
| LM_Tests | LM Lag test | 1506.82** | 2939.76** | 47.13** | 6.42* |
| Robust LM Lag test | 6.84** | 186.74** | 20.45** | 7.11** | |
| LM Error test | 1500.82** | 2773.34** | 39.29** | 4.62* | |
| Robust LM Error test | 0.84 | 20.32** | 12.61** | 5.30* | |
**: P < 0.01; *: P < 0.05
The results of the three models (fixed effects model, spatial lag panel model and spatial error panel model) for each group are shown in Table 3. It can be seen in Table 3 that the spatial lag panel model and the spatial error panel model were better than the classic fixed effects model, and the spatial lag model is more appropriate than the spatial error model at comparing the values of R2 and the log-likelihood in each group. Both the spatial autoregressive coefficient (ρ = 0.452, 0.615, 0.241 and 0.201 for G1, G2, G3, and G4, respectively) and the spatial autocorrelation coefficient (λ = 0.450, 0.616, 0.178 and 0.092 for G1, G2, G3, and G4, respectively) were positive and statistically significant, suggesting the HFMD incidence of a spatial unit correlates positively with the incidence of surrounding spatial units and unmeasured variables.
Table 3.
Results of the fixed effects model (FEM), spatial lag (SLM) and spatial error (SEM) fixed effects panel models in each group
| Variable | G1 | G2 | G3 | G4 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FEM | SEM | SLM | FEM | SEM | SLM | FEM | SEM | SLM | FEM | SEM | SLM | |
| AAP | 0.568** | 0.935** | 0.704** | 0.816** | 0.167 | 0.288 | 0.521 | 0.405 | 0.382 | 1.653 | 1.866 | 1.494 |
| AT | −0.096* | −0.044 | −0.020 | 0.619** | 0.498** | 0.236** | 0.682** | 0.520** | 0.529** | 0.461** | 0.425** | 0.379* |
| AVP | 0.208** | 0.233** | 0.157** | −0.497** | −0.362** | −0.227** | 0.098 | 0.134* | 0.099 | 0.584** | 0.548** | 0.512** |
| ARH | −0.007 | −0.031 | −0.013 | 0.287** | 0.094** | 0.110** | −0.030 | −0.050 | −0.043 | −0.142 | −0.135 | −0.132 |
| MP | 0.011 | 0.010 | 0.008 | 0.013 | −0.002 | 0.004 | −0.012 | −0.002 | −0.007 | −0.130** | −0.122** | −0.119** |
| AWS | −0.033* | −0.021 | −0.028* | −0.033 | −0.005 | −0.013 | −0.006 | −0.001 | 0.002 | −0.263** | −0.262** | −0.253** |
| MSH | 0.046** | 0.032* | 0.034** | 0.014 | 0.006 | 0.002 | −0.100** | −0.107** | −0.097** | −0.144* | −0.142* | −0.135* |
| MTD | −0.074** | −0.056** | −0.048** | 0.061** | 0.027 | 0.033 | 0.030 | 0.029 | 0.026 | 0.056 | 0.070 | 0.062 |
| RD | −0.003 | 0.006 | 0.002 | 0.007 | 0.023 | 0.007** | 0.044 | 0.036 | 0.037 | −0.019 | −0.012 | −0.014 |
| ATD | 0.040** | 0.014 | 0.016 | 0.073** | −0.009 | 0.026** | −0.022 | −0.007 | −0.014 | 0.001 | 0.015 | 0.008 |
| Lambda(λ) | - | 0.450** | - | - | 0.616** | - | - | 0.178** | - | - | 0.092* | - |
| Rho(ρ) | - | - | 0.452** | - | - | 0.615** | - | - | 0.241** | - | - | 0.201** |
| R2 | 0.765 | 0.764 | 0.803 | 0.700 | 0.692 | 0.802 | 0.789 | 0.789 | 0.797 | 0.565 | 0.565 | 0.570 |
| Log-likelihood | −3283.500 | −2676.000 | −2675.180 | −4390.400 | −3299.800 | −3280.479 | −1200.400 | −1181.126 | −1178.103 | −729.547 | −727.100 | −726.281 |
**: p < 0.01; *: p < 0.05
Different significant factors were found in different groups. The average atmospheric pressure (AAP), average vapor pressure (AVP), monthly total sunshine hours (MSH) and mean temperature difference (MTD) had a significant correlation with the HFMD incidence in the three models for regions, and average wind speed (AWS) was also significant in the spatial lag model for south/east China. Average temperature (AT), average vapor pressure (AVP), average relative humidity (ARH), rain day (RD) and average temperature distance (ATD) were risk factors in the spatial lag model in regions with a temperate monsoon climate (TMC). Average temperature (AT) has a significant positive correlation with the HFMD incidence, but monthly total sunshine hours (MSH) was found to have a significant negative correlation in both G3 and G4. Monthly precipitation (MP) and average wind speed (AWS) also had a significant negative association with the HFMD incidence in G4, although average vapor pressure (AVP) was positively significant. The collected variables and the spatial neighborhood effects could jointly explain approximately 80.0 % of the variation of the HFMD incidence in the first 3 groups (G1 [R2 = 0.803], G2 [R2 = 0.802] and G3 [R2 = 0.797]) and 57.0 % in group G4 (R2 = 0.570). We can also find that most coefficients of spatial panel models were smaller than the fixed effect model, which indicated that if the spatial autocorrelation is ignored, the effects of meteorological factors would be overestimated.
Discussion
The relationship between HFMD and meteorological factors was quantified using spatial panel data models based on longitudinal data from 353 regions of mainland China according to climate type from May 2008 to November 2012.
According to Elhorst [17], spatial panel data models contain more variation and less co-linearity among variables and are more informative than purely cross-sectional models or time-series models. The model tests justified the spatial and temporal fixed effects, which indicate that spatial and temporal heterogeneity do affect the robustness of statistical models, and taking the panel structure and spatial autocorrelation terms in the model simultaneously result in a better fit for the data [10]. Previous studies have confirmed the existence of spatial correlations in the incidence of HFMD in various regions, which is consistent with our study [32–35]. Both the spatial autoregressive coefficient in the spatial lag panel model and the spatial autocorrelation coefficient in the spatial error panel model are positive and statistically significant. This further indicates the importance and necessity to include the spatial correlation in exploring the risk factors of HFMD.
These results show that every meteorological factor might have an association with HFMD incidence, and the effect may differ with different climates. A positive relationship between temperature and HFMD incidence (in group G2, G3 and G4) as well as between relative humidity (in group G2) and HFMD incidence was found in our study, which was consistent with the finding of other recent studies [8–10, 13–16]. Average wind speed has a negative association with HFMD incidence (in group G1 and G4) in this study, which is inconsistent with Ma’s, Li’s and Yong Huang’s studies [8, 13, 14]. A negative effect was observed for sunshine at lag days 3–4 in Wu’s study [15], which is consistent with the results in groups G3 and G4 in our research. Deng’s study [9] showed a positive correlation between sunshine and HFMD, which was also consistent with our result in group G1. The differences in the results may be caused by different climate types, which need further research. AAP was found to be positively significant with HFMD in group G1 in this study, which was different from Li’s study in Guangzhou [14]. In Wang’s research [10], vapor pressure had a negative correlation with HFMD, which is consistent with our findings in G2. We also found opposite results in G1 and G4. We also found that monthly precipitation (MP) and mean temperature difference (MTD) were negatively correlated with HFMD in G4 and G1, respectively. Both rain day (RD) and average temperature distance (ATD) had a positive relationship with HFMD in G2, but not in G1, G3 and G4.
There are some limitations in this study. Although the spatial fixed effect and temporal fixed effect were included in the spatial panel models, the models did not consider the effect of space-time interaction, and we assumed that the effect of meteorological variables on HFMD was consistent in all regions. However, the population and climate distribution vary greatly in the world’s third biggest country. It would be difficult to keep the spatial stationarity assumption in such a complicated area. The geographical weighted regression model (GWR) or random coefficients models would be more useful to explore the local effect of factors of interest in the future. We selected the month as the temporal scale; more precise results or lag effects of meteorological factors may have been attained if detailed data were obtained and used for the analysis. Another limitation is that other factors, such as social/economic status, which may affect the HFMD, were not quantified in this study.
Conclusions
Spatial panel data models are useful and effective when longitudinal data are available and spatial autocorrelation exists. This study provides quantitative evidence that the incidence of HFMD could be affected by average atmospheric pressure, average temperature, average vapor pressure, average relative humidity, monthly precipitation, average wind speed, monthly total sunshine hours, mean temperature difference, rain day and average temperature distance. The effects of meteorological factors may be different in different climate types. This can facilitate a better understanding of epidemic trends and a preparedness for HFMD prevention and control strategies.
Acknowledgements
We thank the local health departments, hospitals, and CDC China for assistance in coordinating the data. The views expressed herein are those of the authors and do not necessarily reflect Chinese CDC policies.
Funding
This work was supported by The National S&T Major Project (2012ZX10005009-003 and 2014ZX10004005-001), National 973 Project (2011CB505404), and National Natural Science Foundation of China (81302516). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Availability of data and materials
The dataset(s) supporting the conclusions of this article is(are) available in the Data-center of China Public Health Science repository (hyperlink to dataset(s) in http://www.phsciencedata.cn/Share/en/index.jsp), the China Meteorological Data Sharing Service System (hyperlink to dataset(s) in http://cdc.nmic.cn/home.do) and the National Science & Technology Infrastructure of China, Data Sharing Infrastructure of Earth System Science (hyperlink to dataset(s) in http://www.geodata.cn), which are publicly accessible.
Authors’ contributions
CW participated in the design of the study, collected the data, performed the statistical analysis and drafted the manuscript. KC participated in the design of the study, collected the disease data, participated in the statistical analysis and helped to draft the manuscript. QX, FH, LT, JG and QG collected meteorological data, contributed data analysis and helped to draft the manuscript. YZ, LF and XL participated in the design of the study, collected disease data and the base map of China, and helped to draft the manuscript. XG conceived of the study and participated in its design and coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Not applicable.
Abbreviations
- AAP
average atmospheric pressure
- ARH
average relative humidity
- AT
average temperature
- ATD
average temperature distance
- AVP
average vapor pressure
- AWS
average wind speed
- China CDC
China Center for Disease Control and Prevention
- GWR
geographically weighted regression models
- HFMD
hand, foot and mouth disease
- LM
lagrange multiplier
- LR
likelihood ratio
- MP
monthly precipitation
- MSH
monthly total sunshine hours
- MTD
mean temperature difference
- PMC
plateau mountain climate
- RD
rain day
- Robust LM
robust Lagrange multiplier
- SMC
subtropical monsoon climate
- TCC
temperate continental climate
- TMC
temperate monsoon climate
References
- 1.Yang F, Jin Q, Zhang T, Hu Y, Wang S, Sun X, et al. Survey of enterovirus infections from hand, foot and mouth disease outbreak in China, 2009. Virol J. 2011;8:508. doi: 10.1186/1743-422X-8-508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.World Health Organization . A guide to clinical management and public health response for Hand, Foot and Mouth disease (HFMD) Geneva: WHO Press; 2011. [Google Scholar]
- 3.Chinese Center for Disease Control and Prevention (China CDC). National incidence and death cases of notifiable class A or class B infectious disease (2008, 2009, 2010, 2011, 2012). (http://www.chinacdc.cn). Accessed 03 Apr 2014.
- 4.Xing W, Liao Q, Viboud C, Zhang J, Sun J, Wu JT, et al. Hand, foot, and mouth disease in China, 2008–12: an epidemiological study. Lancet Infect Dis. 2014;14(4):308–18. doi: 10.1016/S1473-3099(13)70342-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wang C, Li X, Zhang Y, Xu Q, Huang F, Cao K, et al. Spatiotemporal cluster patterns of hand, foot, and mouth disease at the county level in mainland China, 2008–2012. PLoS One. 2016;11(1):e0147532. doi: 10.1371/journal.pone.0147532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Onozuka D, Hashizume M. The influence of temperature and humidity on the incidence of hand, foot, and mouth disease in Japan. Sci Total Environ. 2011;410–411:119–25. doi: 10.1016/j.scitotenv.2011.09.055. [DOI] [PubMed] [Google Scholar]
- 7.Ma E, Lam T, Chan KC, Wong C, Chuang SK. Changing epidemiology of hand, foot, and mouth disease in Hong Kong, 2001–2009. Jpn J Infect Dis. 2010;63:422–6. [PubMed] [Google Scholar]
- 8.Huang Y, Deng T, Yu S, Gu J, Huang C, Xiao G, et al. Effect of meteorological variables on the incidence of hand, foot, and mouth disease in children: a time-series analysis in Guangzhou, China. BMC Infect Dis. 2013;13(1):134. doi: 10.1186/1471-2334-13-134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Deng T, Huang Y, Yu S, Gu J, Huang C, Xiao G, et al. Spatial-temporal clusters and risk factors of hand, foot, and mouth disease at the district level in Guangdong Province, China. 2013. e56943. [DOI] [PMC free article] [PubMed]
- 10.Wang H, Du Z, Wang X, Liu Y, Yuan Z, Liu Y, et al. Detecting the association between meteorological factors and hand, foot, and mouth disease using spatial panel data models. Int J Infect Dis. 2015;34:66–70. doi: 10.1016/j.ijid.2015.03.007. [DOI] [PubMed] [Google Scholar]
- 11.Hii YL, Rocklov J, Ng N. Short term effects of weather on hand, foot and mouth disease. PLoS One. 2011;6(2):e16796. doi: 10.1371/journal.pone.0016796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Urashima M, Shindo N, Okabe N. Seasonal models of herpangina and hand-foot-mouth disease to simulate annual fluctuations in urban warming in Tokyo. Jpn J Infect Dis. 2003;56:48–53. [PubMed] [Google Scholar]
- 13.Ma E, Lam T, Wong C, Chuang SK. Is hand, foot and mouth disease associated with meteorological parameters? Epidemiol Infect. 2010;138(12):1779–88. doi: 10.1017/S0950268810002256. [DOI] [PubMed] [Google Scholar]
- 14.Li T, Yang Z, Liu X, Kang Y, Wang M. Hand-foot-and-mouth disease epidemiological status and relationship with meteorological variables in Guangzhou, southern China, 2008–2012. Rev Inst Med Trop Sao Paulo. 2014;56(6):533–9. doi: 10.1590/S0036-46652014000600014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Wu H, Wang H, Wang Q, Xin Q, Lin H. The effect of meteorological factors on adolescent hand, foot, and mouth disease and associated effect modifiers. Global health action, 2014, 7. doi: http://dx.doi.org/10.3402/gha.v7.24664. [DOI] [PMC free article] [PubMed]
- 16.Hu M, Li Z, Wang J, Jia L, Liao Y, Lai S, et al. Determinants of the incidence of hand, foot and mouth disease in China using geographically weighted regression models. PLoS One. 2012;7(6):e38978. doi: 10.1371/journal.pone.0038978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Elhorst JP. Spatial panel data models. Handbook of applied spatial analysis: 377–407; 2010.
- 18.Lee L, Yu J. Some recent developments in spatial panel data models. Reg Sci Urban Econ. 2010;40(5):255–71. doi: 10.1016/j.regsciurbeco.2009.09.002. [DOI] [Google Scholar]
- 19.The Ministry of Health of the People's Republic of China. Guide for the preparedness and control measures of hand, foot, and mouth disease in China. (2008 version) (in Chinese). (http://www.gov.cn/gzdt/2008-05/03/content_960347.htm).
- 20.National Bureau of Statistics of the People’s Republic of China. http://www.stats.gov.cn/tjsj/tjgb/rkpcgb/dfrkpcgb/. Accessed 14 Mar 2014.
- 21.Pfeiffer DU, Robinson TP, Stevenson M, Stevens KB, Rogers DJ, Clements AC. Spatial analysis in epidemiology. New York: Oxford University Press; 2008. [Google Scholar]
- 22.Chan TC, King CC. Surveillance and epidemiology of infectious diseases using spatial and temporal clustering methods. In: Castillo-Chavez C, Lober WB, Thurmond M, Zeng D, editors. Infectious disease informatics and biosurveillance: research, systems and case studies. U.S.A.: Springer; 2010. pp. 208–34. [Google Scholar]
- 23.Wooldridge JM. Econometric analysis of cross section and panel data. 2. Boston: The MIT press; 2010. [Google Scholar]
- 24.Hsiao C. Analysis of panel data. 2. London: Cambridge University Press; 2002. [Google Scholar]
- 25.LeSage J, Pace RK. Introduction to spatial econometrics: CRC press. 2010. [Google Scholar]
- 26.Hausman JA. Specification tests in econometrics. Econometrica. 1978;1251–1271.
- 27.Baltagi BH, Song SH, Jung BC, Koh W. Testing for serial correlation, spatial autocorrelation and random effects using panel data. J Econ. 2007;140(1):5–51. doi: 10.1016/j.jeconom.2006.09.001. [DOI] [Google Scholar]
- 28.Elhorst JP. Specification and estimation of spatial panel data models. Int Reg Sci Rev. 2003;26:244–68. doi: 10.1177/0160017603253791. [DOI] [Google Scholar]
- 29.Lee L, Yu J. Estimation of spatial autoregressive panel data models with fixed effects. J Econ. 2010;154:165–85. doi: 10.1016/j.jeconom.2009.08.001. [DOI] [Google Scholar]
- 30.Elhorst JP. Matlab software for spatial panels. Int Reg Sci Rev. 2012;15905357.
- 31.Kelejian HH, Prucha IR. Specification and estimation of spatial autoregressive models with autoregressive and heteroskedastic disturbances. J Econ. 2010;157:53–67. doi: 10.1016/j.jeconom.2009.10.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Liu Y, Wang X, Liu Y, Sun D, Ding S, Zhang B, et al. Detecting spatial-temporal clusters of HFMD from 2007 to 2011 in Shandong Province, China. PLoS One. 2013;8(5):e63447. doi: 10.1371/journal.pone.0063447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Wang J, Cao Z, Zeng DD, Wang Q, Wang X, Qian H. Epidemiological analysis, detection, and comparison of space-time patterns of Beijing hand-foot-mouth disease (2008–2012) PLoS One. 2014;9(3):e92745. doi: 10.1371/journal.pone.0092745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Xie YH, Chongsuvivatwong V, Tang Z, McNeil EB, Tan Y. Spatio-temporal clustering of hand, foot, and mouth disease at the county level in Guangxi, China. PLoS One. 2014;9(2):e88065. doi: 10.1371/journal.pone.0088065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Xiao GX, Hu YH, Ma JQ, Hao YT, Wang XF, Zhang E. Spatial clustering and changing trend of hand-foot-mouth disease during 2008–2011 in China. Zhonghua liu xing bing xue za zhi. 2012;33:808–12. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The dataset(s) supporting the conclusions of this article is(are) available in the Data-center of China Public Health Science repository (hyperlink to dataset(s) in http://www.phsciencedata.cn/Share/en/index.jsp), the China Meteorological Data Sharing Service System (hyperlink to dataset(s) in http://cdc.nmic.cn/home.do) and the National Science & Technology Infrastructure of China, Data Sharing Infrastructure of Earth System Science (hyperlink to dataset(s) in http://www.geodata.cn), which are publicly accessible.