

We read with great interest the article video commentary on “imaging the coronary sinus (CS).”[1] Proper imaging of CS is essential for confirmation of retrograde cardioplegia cannula placement. Commonly used tranesophageal echocardiographic (TEE) views to direct retrograde cannulation are mid-esophageal CS view and modified the bicaval view. Mid-esophageal CS view is easy to obtain by doing slight retroflexion of probe in mid-esophageal 4 chamber view. CS can be seen in long axis view and good view to see entering retrograde cannula [Figures 1–3]. CS can also be imaged in cross-section in mid-esophageal two chamber view [Figure 4]. Recognizing CS in the modified bicaval view can be tricky because inferior vena cava (IVC) can be easily confused with CS. Relationship between the CS, tricuspid valve, and IVC must be understood to recognize the structures on echocardiography [Figures 5 and 6]. In this view, small caliber vessel on the left side of the display is usually CS, however if the imaging plane of echocardiography passes through IVC in an oblique direction, then IVC can be mistaken for CS. The Eustachian valve or Eustachian ridge separates the IVC and CS. As the TEE probe is turned from right to left, there is a transition of structures from the appearance of IVC to the double barrel view which can be seen sometimes. In this view, both IVC and CS can be seen separated by eustachian ridge [Figure 7]. CS will be away from the transducer and near the attachment of tricuspid valve leaflet. Rarely middle cardiac vein draining into CS can also be seen [Figure 8]. However, large CS can sometimes obscure IVC image [Figure 9].
Figure 1.

Mid-esophageal coronary sinus view showing coronary sinus in long axis
Figure 3.
Mid-esophageal coronary sinus view showing large coronary sinus due to left sided superior vena cava identified by saline bubbles in coronary sinus when agitated saline pushed through left cubital vein
Figure 4.

Mid-esophageal 2 chamber view showing coronary sinus in cross-section
Figure 5.

Schematic diagram showing relationship between inferior vena cava, coronary sinus and tricuspid valve. Also shows imaging plane passing in bicaval view and modified bicaval view
Figure 6.

Mid-esophageal bicaval view showing inferior vena cava, tricuspid valve, superior vena cava, right atrial appendage, left atrium, right atrium
Figure 7.

Mid-esophageal modified bicaval view showing coronary sinus and inferior vena cava separated by eustachian ridge
Figure 8.

Mid-esophageal modified bicaval view showing coronary sinus and middle cardiac vein draining into it
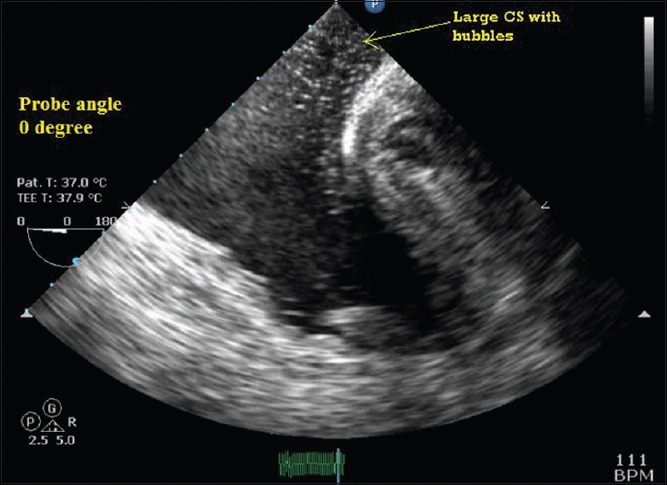
Figure 9.

Mid-esophageal modified bicaval view showing large coronary sinus due to left sided superior vena cava identified by saline bubbles in coronary sinus when agitated saline pushed through left cubital vein. Huge coronary sinus obscured inferior vena cava view
Figure 2.

Mid-esophageal coronary sinus view showing retrograde cannula in coronary sinus
Financial support and sponsorship
Nil.
Conflict of interest
There are no conflict of interest.
REFERENCE
- 1.Irpachi K, Kapoor PM, Narula J, Sahu M. Video commentary on “imaging the coronary sinus”. Ann Card Anaesth. 2015;18:216. doi: 10.4103/0971-9784.154483. [DOI] [PMC free article] [PubMed] [Google Scholar]