

Abstract
Background:
Laser therapy, for its established analgesic properties with minimal side effects, has been used for the treatment of chronic pain. However, it has not been used for the treatment of acute postoperative pain. This pilot study was designed to assess the feasibility and efficacy of Class IV laser on postoperative pain relief following off-pump coronary artery bypass graft (OPCABG) surgery, as a component of multimodal analgesia (MMA) technique.
Methods:
This open observational prospective study comprised of 100 adult patients (84 male, 16 female) who underwent OPCABG through sternotomy. For postoperative analgesia, they were subjected to laser therapy subjected to laser therapy in addition to the standard institutional pain management protocol comprising of IV infusion/bolus of tramadol and paracetamol and fentanyl bolus as rescue analgesic. Pain intensity was measured by Verbal Rating Scale (VRS). The laser therapy was scheduled as once a day regime for three consecutive postoperative days (PODs) starting on POD 1, 30 min following tracheal extubation. The subsequent laser applications were also scheduled at the same time of the day as on day 1 if VRS was ≥5. 10 W Class IV laser was applied over 150 cm2 sternal wound area for 150 s. VRS was used to assess pain severity and was recorded for statistical analysis using Friedman Test.
Results:
The mean (standard deviation [SD]) VRS of all the 100 patients just before application of the first dose of laser was 7.31 (0.94) while on MMT; the same fell to 4.0 (1.279) and 3.40 (2.697) at 1 h and 24 h respectively following first dose of laser. The change of VRS over first 24 h among all the 100 patients was statistically significant (P = 0.000). Laser was re-applied in 40 patients whose VRS was ≥5 (mean [SD] – 6.38 [0.868]) at 24th h. After receiving the 2nd dose of laser the VRS scores fell significantly (P = 0.000) and became 0 at 54th h. No patients required 3rd dose of the laser. No patient required rescue analgesic while on laser therapy.
Conclusion:
Class IV laser can be an effective technique for postoperative analgesia following OPCABG surgery through sternotomy when included as a component of MMA technique.
Keywords: Class IV laser, Low level laser therapy, Multimodal analgesia, Off-pump coronary artery bypass graft, Postoperative pain
INTRODUCTION
Pain after cardiac surgery has been known to be significant, with 30–75% of patients reporting moderate to severe acute pain.[1] Poorly controlled postoperative pain may not only cause hemodynamic disturbances in acute phase, it could also lead to delayed recovery, chronic pain, higher morbidity, longer hospital stay, overall increased costs overall increased costs, and poorer outcomes apart from a dissatisfied patient.[2] Adequate pain relief is expected to result in improved hemodynamics, myocardial oxygenation, and immunomodulation.[3] Improved minimally invasive surgical techniques coupled with economic pressures and patients’ expectations, more than ever before, expect anesthesiologist anesthesiologists to tailor perioperative care to facilitate early recovery and shorter hospital stay.
Multimodal analgesia (MMA) relies on a synergistic combination of different available therapeutic modalities like pharmacologic interventions, rehabilitative maneuvers, and psychological counseling to reduce doses of individual drugs. However, search for a truly effective and ideal combination of agents and techniques continues and remains a distant dream till date. It is this context, laser therapy with its established analgesic properties, and minimal side effects may come around as an effective adjuvant to the current available armamentarium to conquer pain.[4,5] Also, laser therapy has been found to accelerate tissue healing that can make it particularly useful in postoperative patients.[6,7] Laser therapy has been traditionally used for chronic pain, though hitherto available low-level lasers (Classes I-III) have not been very effective on account of poor tissue penetration achieved by them. Class IV laser appears to have overcome this limitation due to its longer wavelength and higher energy output, capable of triggering therapeutic cellular metabolic changes resulting in immediate pain relief and possibly a role in enhancing surgical wound healing as well. We conducted this observational pilot study with the aim to identify if Class IV laser could be used as an effective adjunct to the existing multimodal pain management modalities in postoperative patients following off-pump coronary artery bypass graft (OPCABG) surgery.
METHODS
Hundred consecutive patients of either sex, 18 years or older, scheduled for OPCAB surgery via median sternotomy were included in the study after obtaining approval from Institutional Review Board and Independent Ethics Committee. Each patient was individually visited by a member of the anesthesia team, was explained about the intended pain management protocol including laser therapy, apart from overall anesthetic management, queries if any were answered, and only after obtaining a written informed consent were included in the study. The exclusion criteria were as follows:
Patients with any kind of tumor or growth (benign or malignant) in the area around sternum
Patients receiving steroids or photosensitive drugs
Patients allergic to tramadol or paracetamol
Patients with abnormal liver function test
Patients with permanent or temporary pacemaker, and
Patients unwilling to take part in the study for any reason.
After enrollment, the following categories of patients (n = 13) were also excluded from the study in the postoperative period.
Deeply sedated, or unresponsive or those who had not regained full sensorium, or who appeared to be having poor cognitive function, or in delirium or psychosis (n = 3)
Patients with actively oozing sternal wound, patients who complained of heat-related discomfort during laser therapy despite all precautions and reassurance (n = 0)
Patients who could not be weaned off ventilator and trachea could not be extubated for any reason on postoperative day (POD) 1 (n = 5)
Patients who needed tracheal re-intubation and/or re-exploration due to any cause (n = 5)
Patients who otherwise could not complete the study for any reason (n = 0)
Severe discomfort felt during laser application even after taking all the precautionary measures (n = 0).
All the patients were subjected to general anesthesia as per the standard institutional protocol. Anesthesia was induced with fentanyl, midazolam, and thiopentone, followed by tracheal intubation facilitated with rocuronium. Anesthesia was maintained with intermittent doses of fentanyl and rocuronium, with isoflurane in oxygen and air mixture. All the patients received postoperative analgesia as per the standard institutional protocol, which included fentanyl infusion (1 μg/kg), paracetamol boluses over 20 min each (15 mg/kg/dose, 6 hourly) and tramadol infusion (100 mg over 8 h). All the drugs were administered through intravenous route and initiated in the postoperative recovery room soon after being transferred from OT. The average time interval between stoppage of fentanyl infusion and tracheal extubation was 2 h. Tramadol infusion was stopped immediately before extubation. After tracheal extubation, the tramadol and paracetamol were continued. The intensity of subjective pain assessment was determined by an 11-point Verbal Rating Scale (VRS) containing whole numbers 0–10; “0” representing “no pain” and “10” representing “worst pain imaginable.”
Laser therapy was initiated on POD 1, 30 min following tracheal extubation as a once a day regime, to be repeated next 2 days at the same time of the day if patient's own assessment of pain on VRS was ≥5. The patients receiving laser therapy continued to receive the standard institutional pain management regime comprising of injectable tramadol and paracetamol, and fentanyl bolus of 1 μg/kg as rescue analgesic during the intervening period between laser applications.
The dosage of laser applied was 10 J/cm2 over an area 150 cm2 (approximate) of sternum covering the sternal wound amounting to 1500 J (approximate). The duration of laser therapy was 150 s with a laser power output of 10 W and the laser frequency of 980 nm using “LCT-1000™” (LiteCure Medical) as the laser source. The operating mode used was CW. Both the caregiver and the patient were given laser protective eyewear as per the standard practice during laser therapy.
The VRS was recorded at the following times: Immediately before application of laser; 1 h after the laser application; and thereafter, every 6 hourly till 72 h following first laser application. The sternal wound was examined every day till discharge for following wound complications: wound gaping, serosanguinous discharge, hyperemia, induration and increase in local temperature. Patients were also monitored for heat-related complications such as discomfort, pain and redness, burn, and blister formation. A provision for temporary stoppage of laser application was kept if heat-related discomfort was stated by any patient while receiving laser application. Statistical analysis was performed using SPSS version 13 (SPSS Inc. Chicago, IL) and Microsoft Office Excel (Microsoft Corporation, Redmond, WA).
RESULTS
A total of 100 patients were included in the study, 84 were males and 16 were females. The details of patient demography are stated in Table 1.
Table 1.
Patient demography
| Number | Mean age (SD) (year) | Mean weight (SD) (kg) | Mean height (SD) (cm) | |
|---|---|---|---|---|
| Male | 84 | 60.24 (9.333) | 72.15 (13.1) | 167.98 (6.331) |
| Female | 16 | 56.44 (9.288) | 65.87 (14.341) | 158.35 (10.002) |
| Total | 100 | 59.63 (9.384) | 71.14 (13.343) | 166.44 (7.832) |
SD: Standard deviation
Mean (standard deviation [SD]) VRS of all the 100 patients immediately before application of the first dose of laser was 7.31 (0.94), which fell to 4.0 (1.279) and 3.40 (2.697) at 1 h and 24 h respectively after the laser application. The VRS during first 48 h among all the 100 patients is shown in Table 2. The changes in VRS scores are analyzed by Friedman test and found to be statistically significant (P = 0.000). Only 40 patients, who had VRS of 5 or more (mean [SD] – 6.38 [0.868]) at 24 h after the first application of laser, were given the second dose of laser. The changes of VRS score in this group of patients (n = 40) during first 24 h (after first laser application), and second 24 h (after second laser application at 24th h) are noted in Table 2. After receiving the 2nd dose of laser, the VRS fell significantly (P = 0.000) in those 40 patients and became 0 at 54th h. The changes of VRS scores among the remaining 60 patients who did not require 2nd dose of laser is shown separately in Table 2. Table 3 shows different P values, derived after applying “Friedman test” to test the significance of the changes of VRS scores in four different conditions.
Table 2.
VRS score of all the 100 patients in the first 48 h
| Group | Statistics | Before Laser | After 1 h | After 6 h | After 12 h | After 18 h | After 24 h | After 30 h | After 36 h | After 42 h | After 48 h |
|---|---|---|---|---|---|---|---|---|---|---|---|
| n=60 | Mean | 7.18 | 3.73 | 3.37 | 2.82 | 2.50 | 1.42 | 0.85 | 0.33 | 0.15 | 0.02 |
| SD | 1.05 | 1.36 | 1.29 | 1.23 | 1.67 | 1.31 | 1.40 | 0.77 | 0.48 | 0.13 | |
| Minimum | 3 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Maximum | 10 | 8 | 8 | 6 | 7 | 4 | 6 | 3 | 2 | 1 | |
| Median | 7 | 4 | 3 | 3 | 2 | 1 | 0 | 0 | 0 | 0 | |
| n=40 | Mean | 7.50 | 4.40 | 4.35 | 4.35 | 4.68 | 6.38 | 3.15 | 1.93 | 1.05 | 0.33 |
| SD | 0.72 | 1.03 | 1.08 | 1.39 | 1.58 | 0.87 | 1.51 | 1.16 | 1.08 | 0.80 | |
| Minimum | 6 | 3 | 3 | 2 | 1 | 5 | 0 | 0 | 0 | 0 | |
| Maximum | 10 | 7 | 8 | 7 | 8 | 8 | 8 | 5 | 5 | 4 | |
| Median | 7.5 | 4 | 4 | 4 | 5 | 6 | 3 | 2 | 1 | 0 | |
| Total (n=100) | Mean | 7.31 | 4.00 | 3.76 | 3.43 | 3.37 | 3.40 | 1.77 | 0.97 | 0.51 | 0.14 |
| SD | 0.94 | 1.28 | 1.30 | 1.49 | 1.95 | 2.70 | 1.83 | 1.23 | 0.89 | 0.53 | |
| Minimum | 3 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Maximum | 10 | 8 | 8 | 7 | 8 | 8 | 8 | 5 | 5 | 4 | |
| Median | 7 | 4 | 4 | 3 | 3 | 3 | 2 | 0 | 0 | 0 |
SD: Standard deviation, VRS: Verbal Rating Scale
Table 3.
P values derived after applying Friedman test for significance test among the changes of VRS scores in four different situations
| n | 100 | 60 | 40 | 40 |
|---|---|---|---|---|
| VRS scores (from-upto) | Baseline-at 24 h | Baseline-at 48 h | Baseline-at 24 h | At 24 h-at 48 h |
| Chi-square | 705.298 | 459.817 | 128.997 | 150.776 |
| df | 9 | 9 | 5 | 4 |
| Asymptotic significant | 0.000 | 0.000 | 0.000 | 0.000 |
VRS: Verbal Rating Scale
No patient needed 3rd dose of the laser. The VRS scores at different times (up to 48th h) are shown in Figure 1 (readings after 48th h were not included). No patients complained about any laser-induced discomfort or heat-related complications. Wound complications were not reported in any of the 100 patients until discharge. No patient needed rescue analgesia.
Figure 1.
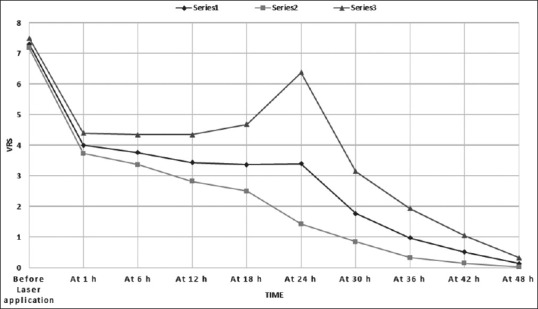
Verbal Rating Scale (VRS) scores of patients receiving laser therapy. Series 1: Average VRS scores of all the 100 patients; Series 2: Average VRS scores of the 60 patients who received laser on postoperative day (POD) 1 only; Series 3: Average VRS scores of the 40 patients who received laser on POD 1 and POD 2
DISCUSSION
Postoperative pain is typically managed by multimodal approach; pharmacological and rehabilitative therapies in particular. Among pharmacological agents, a combination of opioids, nonopioid analgesics, nonsteroidal anti-inflammatory drugs and local anesthetics helps avoid overdosing of anyone, thus minimizing undesirable side-effects. Our institutional postoperative pain management protocol includes continuation of injectable fentanyl and paracetamol from the operating room and addition of injectable tramadol in the recovery room. However, individual patient responses like respiratory depression, excessive sleepiness, nausea and vomiting often necessitate adjustments of dose and duration or even discontinuation of analgesic agents. This would at times result in heightened pain perception following tracheal extubation as is evident in mean (SD) VRS of 7.31 (0.94).
Faced with wide variations in pain scores in postoperative patients, it was felt that a laser with its well established analgesic properties could be studied for its suitability to relieve acute postoperative pain. Laser, though well established as a therapeutic modality in sports medicine and physical therapy for pain relief,[8,9,10,11] has never been used for acute postoperative pain relief, and thus merited a pilot study to evaluate its feasibility and efficacy in the new setting.
A systematic review of 11 trials that included 565 patients demonstrated that low-level laser therapy (LLLT - Classes I-III) used in a specific dose range significantly reduced pain in chronic joint disorders.[12] Another systematic review with meta-analysis of 18 randomized placebo-controlled trials evaluating LLLT in elbow tendonopathy concluded that LLLT provided short-term pain relief with less disability, when administered in optimal doses directly to the lateral elbow tendon insertions.[10] Laser has been known as a safe and effective treatment modality for relieving pain, reducing inflammation and to promote wound healing and soft tissue repair.[13,14,15] In a randomized placebo-controlled trial, Bjordal et al. treated activated Achilles tendonitis in seven patients with LLLT and found that LLLT suppresses inflammation, measured by reduction in the inflammatory marker PGE2 and improvement in clinical indices of pressure pain and sing hop function in these patients.[16]
Laser is said to act through photo-biomodulation, that involves essentially a series of tissue responses to laser: stabilization of the cellular membrane, enhancement of ATP production, vasodilatation, acceleration of leukocytic activity, increased prostaglandin synthesis, reduction in interleukin 1, enhanced lymphocyte response, increased angiogenesis, temperature modulation, enhanced superoxide dismutase levels, decreased C-reactive protein and neopterin levels.[17,18] All these tissue activities reduce acute inflammatory response. Photo-biomodulation also produces analgesia by increasing beta-endorphins and nitric oxide production, decreasing bradykinin levels, ion channel normalization, blocking depolarization of C-fiber afferent nerves, increasing nerve cell action potentials and release of acetylcholine, and axonal sprouting and nerve cell regeneration. The other biological response includes DNA and RNA synthesis, an increase in cAMP levels, protein and collagen synthesis and cellular proliferation. These activities lead to rapid normalization, regeneration and healing of damaged tissue.[19] Thus, the application of laser to a wound area reduces acute inflammation response and produces analgesia.
Therapeutic laser dosage is dependent on three factors: power output, wavelength and time. Laser light energy absorption by the skin and subcutaneous tissue is estimated to be 50–90%. The absorption by the skin and subcutaneous tissue increases as the wavelength, measured in nanometers (nm), decreases. Therefore, lasers with shorter wavelengths (Class I-III) fail to reach to the deeper target tissue adequately and thus, fail to deliver sufficient number of photons to the target tissue, the factor that determines wound healing, control of inflammation and pain relief. Indeed, several published clinical studies have found LLLT (Classes I-III) to be suboptimal in adequately treating pain in different clinical conditions. Longer wavelengths (up to 1000 nm) and higher power output result in deeper tissue penetration and higher dosage to the target tissue as seen with Class IV lasers. Certain Class IV lasers have been shown to provide both the wavelengths and power output levels necessary to trigger therapeutic cellular metabolic changes, especially when applied with scientifically based protocols. The clinical literature offers an increasing body of evidences supporting the use of Class IV lasers in a wide range of clinical conditions, demonstrating successful therapeutic results.[4,5]
The actual therapeutic benefit of laser therapy is determined by the power density at the target tissue, color and type of the tissues. In people with dark skin, due to high concentrations of epidermal melanin which absorbs light over a wide range of wavelengths, the laser is absorbed in the epidermal layer before it reaches to the targeted deeper tissue. However, Class IV lasers, because of their longer wavelength, can bypass the selective absorption by the melanin containing epidermis and reach to the deeper tissue targets effectively. The trend in laser therapy over the past decade has been to increase power density and dose. This has been shown to significantly improve therapeutic outcomes. The World Association of Laser Therapy has established that target tissues need a dose of 5–7 J/cm2 to elicit a biological cellular response. Given that the most likely origins of this postoperative pain lie below multiple layers of muscle and fascia, satisfactory pain relief requires a therapeutic laser system with adequate tissue penetration to stimulate the physiological events necessary to reduce inflammation and accelerate tissue healing. This study was conducted as a pilot study to evaluate its clinical application in cardiac surgical patients and the results are quite encouraging. The change in pain intensity as measured by VRS scores following the application of laser was found to be statistically significant (P = 0.000; analyzed by Friedman test). As a matter of precaution, the dose, duration, and frequency were decidedly on the lower side, but the results reaffirm our belief that Class IV laser has a role to play as a component of multimodal pain management in cardiac surgical patients also.
Despite the documented clinical benefits from the use of laser, there remains concern regarding tissue overstimulation and a retarded healing process that may result from the use of higher power laser systems. However, there are no in vivo studies in humans to validate this concern. In fact, several studies have documented the wound healing characteristics of the laser. In addition to analgesic property, deep penetrating photo-biostimulation produces reduces inflammation and accelerates tissue healing. It has been found that laser stimulates the production of the fibroblast growth factors. In a case report, Dixit et al. have demonstrated successful application of LLLT in a diabetic patient for treatment of delayed wound healing and pain in chronic dehiscent sternotomy.[20] As for concerns of safety, all the patients had their surgical wounds closely evaluated daily till their discharge from the hospital and none of the patients reported any suboptimal wound healing. On the contrary, we feel that based on results of earlier studies and our observation of no untoward effect on the wound healing, some nonhealing wounds can be subjected to laser irradiation to evaluate its healing properties.
The other safety concern could be thermal burns since laser gets absorbed into the skin and subcutaneous tissue and converted to heat which can cause thermal discomfort, redness, pain and even burn injury. This is of concern in subjects with melanoma, hyperpigmented scar or ethnically dark skin where a high concentration of melanin increases the absorption of laser and thereby produces increased heat. However, as the wavelength of the laser increases, the chance of being absorbed by the melanin decreases, thus Class IV lasers with higher wavelengths produce lesser incidences of heat-related injuries. Also, with the advent of newer generation of laser producing machines, which are equipped with cooling safety devices (e.g., sapphire cooled tip and cryogen spray cooling) and a wide range of laser wavelengths, the incidences of thermal injuries is much less. In our study, no patient suffered any heat-related discomfort or burn injury requiring the stoppage of laser application or other cooling measures.
This pilot study observed that Class IV laser can be an effective tool for the treatment of postoperative pain following OPCABG surgery, and could be included as a component of MMA technique. We found it safe, and it appeared well tolerated by the patients. Our study findings suggests that larger randomized controlled trials could be undertaken to further establish its role in postoperative analgesia and to ascertain its dose, duration and frequency besides its suitability and wider application in other cardiac cases like those with prosthetic valves and other mechanical devices in situ.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Bigeleisen PE, Goehner N. Novel approaches in pain management in cardiac surgery. Curr Opin Anaesthesiol. 2015;28:89–94. doi: 10.1097/ACO.0000000000000147. [DOI] [PubMed] [Google Scholar]
- 2.Carr DB, Goudas LC. Acute pain. Lancet. 1999;353:2051–8. doi: 10.1016/S0140-6736(99)03313-9. [DOI] [PubMed] [Google Scholar]
- 3.Chaney MA. Postoperative pain management for the cardiac patient. In: Kaplan JA, Reich DL, Savino JS, editors. Kaplan's Cardiac Anesthesia: The Eco Era. 6th ed. Saunders: Missouri; 2011. pp. 1107–37. [Google Scholar]
- 4.Roberts DB, Kruse RJ, Stoll SF. The effectiveness of therapeutic class IV (10 W) laser treatment for epicondylitis. Lasers Surg Med. 2013;45:311–7. doi: 10.1002/lsm.22140. [DOI] [PubMed] [Google Scholar]
- 5.Panton L, Simonavice E, Williams K, Mojock C, Kim JS, Kingsley JD, et al. Effects of Class IV laser therapy on fibromyalgia impact and function in women with fibromyalgia. J Altern Complement Med. 2013;19:445–52. doi: 10.1089/acm.2011.0398. [DOI] [PubMed] [Google Scholar]
- 6.Ottaviani G, Gobbo M, Sturnega M, Martinelli V, Mano M, Zanconati F, et al. Effect of class IV laser therapy on chemotherapy-induced oral mucositis: A clinical and experimental study. Am J Pathol. 2013;183:1747–57. doi: 10.1016/j.ajpath.2013.09.003. [DOI] [PubMed] [Google Scholar]
- 7.Zheng Z, Kang HY, Lee S, Kang SW, Goo B, Cho SB. Upregulation of fibroblast growth factor (FGF) 9 expression and FGF-WNT/β-catenin signaling in laser-induced wound healing. Wound Repair Regen. 2014;22:660–5. doi: 10.1111/wrr.12212. [DOI] [PubMed] [Google Scholar]
- 8.Basford JR, Sheffield CG, Mair SD, Ilstrup DM. Low-energy helium neon laser treatment of thumb osteoarthritis. Arch Phys Med Rehabil. 1987;68:794–7. [PubMed] [Google Scholar]
- 9.Morimoto Y, Saito A, Tokuhashi Y. Low level laser therapy for sports injuries. Laser Ther. 2013;22:17–20. doi: 10.5978/islsm.13-OR-01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bjordal JM, Lopes-Martins RA, Joensen J, Couppe C, Ljunggren AE, Stergioulas A, et al. A systematic review with procedural assessments and meta-analysis of low level laser therapy in lateral elbow tendinopathy (tennis elbow) BMC Musculoskelet Disord. 2008;9:75. doi: 10.1186/1471-2474-9-75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Simunovic Z, Trobonjaca T, Trobonjaca Z. Treatment of medial and lateral epicondylitis – Tennis and golfer's elbow – With low level laser therapy: A multicenter double blind, placebo-controlled clinical study on 324 patients. J Clin Laser Med Surg. 1998;16:145–51. doi: 10.1089/clm.1998.16.145. [DOI] [PubMed] [Google Scholar]
- 12.Bjordal JM, Couppé C, Chow RT, Tunér J, Ljunggren EA. A systematic review of low level laser therapy with location-specific doses for pain from chronic joint disorders. Aust J Physiother. 2003;49:107–16. doi: 10.1016/s0004-9514(14)60127-6. [DOI] [PubMed] [Google Scholar]
- 13.Chung H, Dai T, Sharma SK, Huang YY, Carroll JD, Hamblin MR. The nuts and bolts of low-level laser (light) therapy. Ann Biomed Eng. 2012;40:516–33. doi: 10.1007/s10439-011-0454-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Avci P, Gupta A, Sadasivam M, Vecchio D, Pam Z, Pam N, et al. Low-level laser (light) therapy (LLLT) in skin: Stimulating, healing, restoring. Semin Cutan Med Surg. 2013:41–52. [PMC free article] [PubMed] [Google Scholar]
- 15.Piva JA, Abreu EM, Silva Vdos S, Nicolau RA. Effect of low-level laser therapy on the initial stages of tissue repair: Basic principles. An Bras Dermatol. 2011;86:947–54. doi: 10.1590/s0365-05962011000500013. [DOI] [PubMed] [Google Scholar]
- 16.Bjordal JM, Lopes-Martins RA, Iversen VV. A randomised, placebo controlled trial of low level laser therapy for activated Achilles tendinitis with microdialysis measurement of peritendinous prostaglandin E2 concentrations. Br J Sports Med. 2006;40:76–80. doi: 10.1136/bjsm.2005.020842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Colombo F, Neto Ade A, Sousa AP, Marchionni AM, Pinheiro AL, Reis SR. Effect of low-level laser therapy (λ660 nm) on angiogenesis in wound healing: A immunohistochemical study in a rodent model. Braz Dent J. 2013;24:308–12. doi: 10.1590/0103-6440201301867. [DOI] [PubMed] [Google Scholar]
- 18.dos Santos SA, Alves AC, Leal-Junior EC, Albertini R, Vieira Rde P, Ligeiro AP, et al. Comparative analysis of two low-level laser doses on the expression of inflammatory mediators and on neutrophils and macrophages in acute joint inflammation. Lasers Med Sci. 2014;29:1051–8. doi: 10.1007/s10103-013-1467-2. [DOI] [PubMed] [Google Scholar]
- 19.Moshkovska T, Mayberry J. It is time to test low level laser therapy in Great Britain. Postgrad Med J. 2005;81:436–41. doi: 10.1136/pgmj.2004.027755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dixit S, Maiya A, Umakanth S, Borkar S. Photobiomodulation of surgical wound dehiscence in a diabetic individual by low-level laser therapy following median sternotomy. Indian J Palliat Care. 2013;19:71–5. doi: 10.4103/0973-1075.110242. [DOI] [PMC free article] [PubMed] [Google Scholar]