

Abstract
Background
Rib fracture stabilization has become a more accepted practice although stabilization of the most cephalad ribs presents a unique challenge. We present our experience with use of a 90° drill and screwdriver to bridge these difficult rib fractures.
Methods
This retrospective review included patients who underwent rib fracture stabilization from August 1, 2009, through September 30, 2012. Patients were divided into two groups: those whose procedure used the 90° device and those that did not. Data were compared using standard statistical analysis and reported as percentages and medians [interquartile ranges]. P values <0.05 were considered significant.
Results
We identified 89 patients: 29 (33 %) had 90° devices used and 60 (67 %) did not. There were no differences between groups in age, sex, Trauma-Related Injury Severity Score, the presence of flail chest, occurrence of pneumonia, and intensive care unit or hospital length of stay. The Injury Severity Score was higher in the 90° group (22 vs. 16; P = 0.03). The highest rib stabilized was different between the 2 groups (3 [2–5] vs. 5 [2–9]; P = 0.001), with more third rib stabilizations in the 90° group (38 vs. 20 %; P = 0.04) as well as more total number of ribs fixed (5 vs. 4; P = 0.001). There was no difference in operative time between the 2 groups.
Conclusions
The surgical reach for rib fracture stabilization has been extended with use of a 90° drill and screwdriver. High fractures under the scapula where access is technically challenging can be stabilized without prolonging operative times.
Introduction
Chest injuries are present in up to 15 % of all trauma admissions. Rib fractures are one of the most frequent diagnoses present at admission for blunt trauma, and up to 10 % of all hospitalized trauma patients have associated rib fractures. Previous studies have demonstrated a linear relationship between number of rib fractures and morbidity [1], with increased mortality in patients with more than six rib fractures [2]. Various patterns of rib fracture occur depending on the mechanism of injury, the vector of force delivered to the chest, and the fortitude of the underlying bone. Although surgical stabilization of fractured ribs remains controversial, there has been increasing acceptance of the practice [3, 4].
Surgical stabilization of the chest wall was introduced with wire stitches for broken ribs in 1950. Several other methods have since been introduced [5]. Plate and bicortical screw fixation, originally described in 1975, has become the preferred method of chest wall stabilization [3]. Recent literature suggests shorter intensive care unit (ICU) stays, decreased pain, decreased chest wall deformity, and reduced need for respiratory support in patients undergoing surgical stabilization of rib fractures [3, 6]. In the setting of flail chest, rib fracture stabilization is associated with decreased mortality, decreased pneumonia rates, decreased rates of tracheostomy, fewer days of mechanical ventilation, and shorter hospital stays [7].
The absolute indications for rib fracture fixation continue to be debated. Generally, accepted indications include obvious deformity from chest wall implosion, the presence of flail chest, or multiple displaced rib fractures with overlapping ends [8]. Stabilization of painful nonunion fractures appears to improve pain and activity levels but without significant change in functional or work status [9]. Patients with intractable pain and fracture repair within 7 days of injury may have improved outcomes if the main cause of respiratory failure is painful chest wall motion preventing adequate lung ventilation [10]. Pain as an indication for rib stabilization remains controversial because improved postoperative analgesia has not equated to improved patient outcomes [11]. At our institution, once a patient meets the criteria for surgical rib fracture stabilization, our goal is to repair as many fractures as possible without prolonging the operation or the morbidity of the incision.
The operative exposure is based on the location and extent of fractures. Posterolateral thoracotomy incisions are generally preferred because they allow exposure of the most rib levels [10]. Rib fracture stabilization for the cephalad, posterior ribs poses a unique challenge, given the configuration of the chest wall and the presence of the scapula. Different practices for accessing cephalad rib fractures include the use of counterincisions, stepladder incisions, modified trocar access (in which a surgical trocar is inserted through the skin to serve as a drill guide), and hanging retractors. We present our experience with use of a 90° drill and screwdriver, originally used for mandibular fracture stabilization, to access these difficult rib fractures, hypothesizing that these instruments will result in a greater number of stabilized rib fractures.
Methods
Our institution adopted surgical stabilization of rib fractures in selected patients in 2009. Patients met criteria if they had chest wall implosion, flail chest, severely displaced rib fractures, or early intractable pain. In March 2011, the 90° drill and screwdriver went into clinical practice. This device was adapted from the Depuy Synthes MatrixMandible and MatrixMidface kits, originally developed for orthognathic and facial reconstruction surgery. The device is commercially available but is not yet approved for rib fracture stabilization. Thus, this is an off-label use of the 90° drill and screwdriver.
With approval of the Mayo Clinic Institutional Review Board, we retrospectively reviewed a prospectively collected and maintained trauma database of all patients who underwent rib fracture stabilization procedures from August 1, 2009, through September 30, 2012. Data included patient demographics, mechanism of injury, Injury Severity Score (ISS), Trauma-Related Injury Severity Score (TRISS), complications, ICU and hospital length of stay (LOS), and the number of ventilator days. Operative reports were reviewed to determine the number of ribs stabilized, the most cephalad rib repaired, and operative time. Patients were divided into two groups: those whose procedure used the 90° devices and those that did not. Results were compared using χ2 analysis for categorical data and nonparametric comparisons using Wilcoxon rank sums for continuous variables and are presented as percentage and median [interquartile range], as appropriate. P values <0.05 were considered significant.
Operative technique
Four acute care surgeons at our Level I trauma center routinely perform rib fracture stabilization. Most patients had preoperative chest computed tomographic (CT) imaging in their initial trauma work-up. These images were reformatted to yield 3-dimensional (3D) reconstruction of the chest wall. The incision was created on the basis of the location of the most severely displaced rib fractures and typically followed the shape of a standard thoracotomy incision, caudad to the tip of the scapula and parallel to the direction of the ribs. Muscle-sparing approaches were used as appropriate, sparing either the latissimus dorsi or serratus anterior, depending on the location of the rib fractures (Fig. 1). Fractured ribs were débrided of bone fragments and reduced into anatomic position. The fractures were stabilized with either the Acute Innovations RibLoc or the Synthes MatrixRib system. Plates were cut to the desired length to provide adequate fixation on either side of the fracture, in some cases spanning fractures of a multiply fractured segment of rib. Before introduction of the 90° device, a straight drill (Fig. 2) was used to establish the pilot holes, and then a standard screwdriver was used to secure the screws in place. After introduction of the 90° drill, this device was used at the surgeon’s discretion (Fig. 3). A key difference in the devices is that the straight drill accepts drill guides to ensure a completely perpendicular pilot hole and subsequent screw placement, while the 90° drill and screwdriver require a freehand technique. The practice of our surgeons is to fix all the fractures that can be reached without extending the incision into a more morbid procedure. On completion of the procedure, patients are routinely extubated if indicated, regardless of preoperative respiratory failure.
Fig. 1.
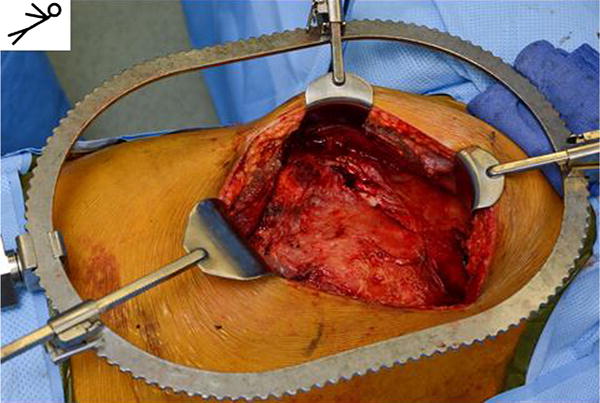
Intraoperative photograph of exposure via a standard left posterolateral thoracotomy incision located over the fifth intercostal space
Fig. 2.

Standard drill used in surgical stabilization of rib fractures. (Courtesy of DePuy Synthes. Used with permission)
Fig. 3.

A 90° drill and screwdriver
Results
We identified 89 patients, of whom 29 (33 %) had 90° devices used and 60 (67 %) did not. Thirty-two patients had fractures that were stabilized before introduction of the 90° devices (Fig. 2). Sixty-four patients (72 %) had preoperative chest CT imaging with 3D reconstruction; all patients had preoperative chest radiography. There were no statistically significant differences between the 90° group and the standard group in age (60 vs. 61 years); sex (male 69 vs. 77 %); TRISS [12 (7–12) vs. 12 (8–12)]; the presence of flail chest (40 vs. 48 %); ICU LOS [1 day (0–17 days) vs. 1 day (0–39 days)]; and hospital LOS [9 days (6–21 days) vs. 9 days (2–39 days)]. The ISS of the 90° group was significantly higher (22 vs. 16; P = 0.03). The highest rib stabilized was significantly different between the groups (3 [2–5] in the 90° group vs. 5 [2–9] in the standard group; P = 0.001), with more third rib stabilizations in the 90° group (38 vs. 20 %; P = 0.04) as well as more total number of ribs fixed (5 vs. 4; P = 0.001). There was no difference noted in operative times between the 90° group and the standard group [155 min (108–440 min) vs. 156 min (47–367 min)] (Table 1). Prior to the introduction of the 90° device, 10 of 60 patients (17 %) underwent stabilization using modified trocar access to stabilize fractured rib segments not amenable to repair via the standard thoracotomy incision. No patients had stepladder incisions. Ten of 15 patients (67 %) had third rib fractures that went unrepaired before the advent of the 90° device. In comparison, only 15 of 38 patients (39 %) did not have the third rib stabilized after introduction of the 90° device (P = .07).
Table 1.
Patient demographics, rib fracture numbers, and operative times in the 90° instrument group and standard instrument group
| Characteristic | 90° Device | Standard device | P value |
|---|---|---|---|
| (n = 29) | (n = 60) | ||
| Age, median (range), year | 61 (55–67) | 60 (55–64) | 0.40 |
| Male sex, No. (%) | 20 (69 %) | 46 (77 %) | 0.70 |
| Highest rib repaired, median (range) | 3 (2–5) | 5 (2–9) | 0.001 |
| Posterior repair, No. (%) | 8 (28 %) | 10 (17 %) | 0.20 |
| Third rib repair, No. (%) | 11 (38 %) | 12 (20 %) | 0.04 |
| Ribs plated, median (range) | 5 (2–12) | 4 (1–7) | 0.001 |
| OR time, median (range), min | 155 (108–440) | 156 (47–367) | 0.66 |
| Flail segment, No. (%) | 14 (48 %) | 24 (40 %) | 0.40 |
| ICU stay, median (range), days | 1 (0–17) | 1 (0–39) | 0.29 |
| LOS, median (range), days | 9 (6–21) | 9 (2–39) | 0.45 |
| ISS, median (range) | 22 (9–41) | 16 (4–29) | 0.03 |
| TRISS, median (range) | 12 (7–12) | 12 (8–12) | 0.06 |
ICU intensive care unit, ISS injury severity score, LOS length of stay, OR operating room, TRISS Trauma-Related Injury Severity Score
Discussion
Our results indicate that cephalad and posterior rib fractures can be reached via a single thoracotomy-type incision, extending the reach of surgical rib fracture fixation to routinely include the third rib. We accomplished this in more severely injured patients without significantly prolonging operative time. We were able to stabilize more ribs using a 90° device. Anecdotally, we believe that the 90° drill and screwdriver have extended the anterior–posterior reach as well, although these results were difficult to quantify on review of the operative notes.
At our institution, operative indications for rib fracture stabilization include restoration of anatomy, restoration of physiology, and early intractable pain. We routinely offer this procedure as a means to restore chest wall anatomy in patients with severe flail chest, chest wall implosion, rib fracture impalement, and severely displaced fractures at high risk of nonunion. Patients with worsening respiratory status, ineffective cough, shallow breathing, and worsening atelectasis are offered this procedure to prevent further progression of respiratory failure. Patients with early intractable pain or increasing analgesic requirements are also offered stabilization if the pain is clinically contributing to poor inspiratory effort and worsening respiratory status. We rarely perform this procedure as an “on the way out” stabilization after thoracotomy for other traumatic indications. It has been our practice to plan the operative exposure on the basis of the most severely displaced fractures or the most symptomatic fractures and then to stabilize as many fractures and levels of ribs as possible via the same incision.
For centers routinely performing rib fracture stabilization, our modified technique using the 90° drill and screwdriver will allow more ribs to be stabilized via a single thoracotomy incision and aid in the stabilization of subscapular rib fractures.
Our present study has several obvious limitations. First, this is a retrospective review, thus data are limited. Second, we acknowledge selection bias. That is, patients with higher rib fractures, more rib fractures, and more severe chest wall injuries were more likely to have procedures in which a 90° device was used. The decision to use a 90° device was often made intraoperatively on the basis of need for increased reach, but increasingly, it is recognized that such devices will be needed after review of the pattern and location of fractures. The 90° devices are valuable adjuncts in the surgical stabilization of rib fractures. Roughly, one-third of rib stabilization procedures in this series were performed before the introduction of the 90° drill, which was relatively early in the experience of our acute care surgeons. Increased proficiency with the procedure could account for shorter operative times. Finally, to date no data suggest that reaching the third rib is clinically necessary or is associated with improved outcomes. However, our practice is to stabilize all fractures that can be reached without extending the incision or increasing the morbidity from the operation.
This modification of the technique of rib fracture stabilization procedures will allow surgeons to have an extended reach without additional incisions or prolonged operative times.
Abbreviation
- CT
Computed tomographic
- ICU
Intensive care unit
- ISS
Injury Severity Score
- LOS
Length of stay
- 3D
3-dimensional
- TRISS
Trauma-Related Injury Severity Score
Footnotes
Mayo Clinic does not endorse the products mentioned in this article. Presented in part as a clinical research presentation at the Minnesota Surgical Society spring meeting, St. Paul, Minnesota, May 25, 2013, and as a free paper at the World Congress of Surgery International Surgical Week biannual meeting, Helsinki, Finland, August 28, 2013.
Conflict of interest The authors declare that they have no conflicts of interest relevant to the manuscript submitted to the World Journal of Surgery.
References
- 1.Sirmali M, Turut H, Topcu S, et al. A comprehensive analysis of traumatic rib fractures: morbidity, mortality and management. Eur J Cardiothorac Surg. 2003;24:133–138. doi: 10.1016/s1010-7940(03)00256-2. [DOI] [PubMed] [Google Scholar]
- 2.Flagel BT, Luchette FA, Reed RL, et al. Half-a-dozen ribs: the breakpoint for mortality. Surgery. 2005;138:717–723. doi: 10.1016/j.surg.2005.07.022. [DOI] [PubMed] [Google Scholar]
- 3.Molnar TF. Surgical management of chest wall trauma. Thorac Surg Clin. 2010;20:475–485. doi: 10.1016/j.thorsurg.2010.07.004. Epub 2010 Sep 6. [DOI] [PubMed] [Google Scholar]
- 4.Simon B, Ebert J, Bokhari F, et al. Management of pulmonary contusion and flail chest: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2012;73(Suppl 4):S351–S361. doi: 10.1097/TA.0b013e31827019fd. [DOI] [PubMed] [Google Scholar]
- 5.Bemelman M, Poeze M, Blokhuis TJ, et al. Historic overview of treatment techniques for rib fractures and flail chest. Eur J Trauma Emerg Surg. 2010;36:407–415. doi: 10.1007/s00068-010-0046-5. Epub 2010 Sep 23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Marasco SF, Davies AR, Cooper J, et al. Prospective randomized controlled trial of operative rib fixation in traumatic flail chest. J Am Coll Surg. 2013;216:924–932. doi: 10.1016/j.jamcollsurg.2012.12.024. Epub 2013 Feb 13. [DOI] [PubMed] [Google Scholar]
- 7.Leinicke JA, Elmore L, Freeman BD, et al. Operative management of rib fractures in the setting of flail chest: a systematic review and meta-analysis. Ann Surg. 2013;258:914–921. doi: 10.1097/SLA.0b013e3182895bb0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nirula R, Mayberry JC. Rib fracture fixation: controversies and technical challenges. Am Surg. 2010;76:793–802. [PubMed] [Google Scholar]
- 9.Fabricant L, Ham B, Mullins R, et al. Prospective clinical trial of surgical intervention for painful rib fracture nonunion. Am Surg. 2014;80:580–586. [PubMed] [Google Scholar]
- 10.Gasparri MG, Tisol WB, Haasler GB. Rib stabilization: lessons learned. Eur J Trauma Emerg Surg. 2010;36:435–440. doi: 10.1007/s00068-010-0048-3. [DOI] [PubMed] [Google Scholar]
- 11.de Moya M, Bramos T, Agarwal S, et al. Pain as an indication for rib fixation: a bi-institutional pilot study. J Trauma. 2011;71:1750–1754. doi: 10.1097/TA.0b013e31823c85e9. [DOI] [PubMed] [Google Scholar]