

Abstract
Modifiable behavioral risk factors such as cigarette smoking, physical inactivity, and obesity contribute to over 40 % of premature deaths in the USA. Advances in digital and information technology are creating unprecedented opportunities for behavior analysts to assess and modify these risk factors. Technological advances include mobile devices, wearable sensors, biomarker detectors, and real-time access to therapeutic support via information technology. Integrating these advances with behavioral technology in the form of conceptually systematic principles and procedures could usher in a new generation of effective and scalable behavioral interventions targeting health behavior. In this selective review of the literature, we discuss how technological tools can assess and modify a range of antecedents and consequences of healthy and unhealthy behavior. We also describe practical, methodological, and conceptual advantages for behavior analysts that stem from the use of technology to assess and treat health behavior.
Keywords: Behavioral assessment, Contingency management, Health behavior, mHealth, Technology
Advances in technology are creating unprecedented opportunities for behavior analysts to assess and promote health behavior. Technological advances include mobile devices, wearable sensors, biomarker detectors, and real-time access to therapeutic interventions via information technology. In light of these innovations, Asch et al. (2012) have called for a new health-care model that enables “automated hovering,” or real-time monitoring, of patients’ behavior while they engage in everyday activities. Because most choices about health are made during everyday activities, influencing these choices constitutes the “single greatest opportunity to improve health and reduce premature deaths” in the USA (Schroeder 2007, p. 1222). Even chronically ill patients spend only a few hours per year with a doctor or nurse, leaving 5,000 h per year in which they are engaged in other health-related behavior, including “deciding whether to take prescribed medications or follow other medical advice, deciding what to eat and drink and whether to smoke, and making other choices about activities that can profoundly influence their health” (Asch et al. 2012, p. 1).
Technology is already in place to perform some forms of automated hovering of health behavior. There are over 1.5 billion Internet users and 5.6 billion cell phone users worldwide (International Telecommunications Union 2011). In the USA, 76 % of the population has home access to the Internet and 91 % owns at least one mobile phone (Brennan 2013). The prevalence of information technology suggests that most humans are already connected to a potential intervention device throughout most of the day. The ubiquity of technology, however, is just one part of the equation to promote behavior change. The second part is a science of behavior to inform developers and researchers about how technology can change behavior. In a major review of mobile health interventions, also known as mHealth, Kaplan and Stone (2013) noted that “many application developers seem unaware that there is a basic science of behavior change” (p. 491).
In this article, we discuss how behavior analysis can inform technology-based assessment and treatment of health behavior. We hope to appeal to two audiences: behavior analysts interested in applying technology to health behavior and developers and researchers in the field of health behavior interested in harnessing behavioral principles to change behavior. First, we introduce a behavior-analytic conceptual framework. Second, we discuss innovative applications of technology to assess and change health-related behavior. Rather than performing a comprehensive review, we focus on illustrative developments to inform future intra- and interdisciplinary work in behavior analysis and allied fields. We also restrict our discussion to technological developments that have appeared in the scientific literature, as opposed to the vast array of largely untested consumer-oriented technologies and web sites. Third, we describe several practical, methodological, and conceptual advantages for the field of behavior analysis that stem from the use of technology.
Technology and Health Behavior: a Conceptual Framework
The Four-Term Functional Unit of Analysis
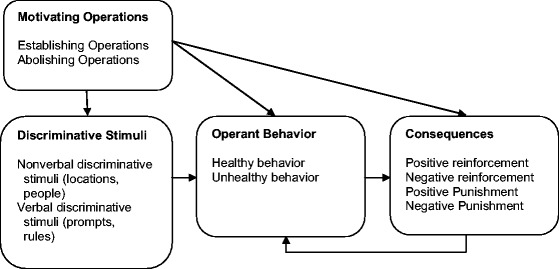
Most health-related behavior can be conceptualized as operant behavior. Operant behavior is any activity influenced by its consequences. Physical activity, eating fruit, taking a medication, and following a medical regimen are operant behavior because their consequences influence their future probability. Similarly, unhealthy behavior such as being sedentary, eating high fat foods, seeking illicit drugs, and refusing a medication are also examples of operant behavior because such behavior is maintained by its consequences. Once these activities are recognized as such, it follows that technology-based methods to change them will need to change one or more components of the functional unit of analysis. The functional unit consists of four components and their dynamic interaction: (a) motivating operations, (b) discriminative stimuli, (c) operant responses, and (d) consequences (Glenn et al. 1992; Thompson 2007). Figure 1 presents a schematic of the four-term unit. These components are relevant to health behavior interventions that assess and introduce antecedents and consequences to change unhealthy behavior, which constitute the majority of technology-based interventions (Kaplan and Stone 2013; Riley et al. 2011; Tomlinson et al. 2013).
Fig. 1.
The four-term functional unit of analysis
Motivating operations (MOs) can increase or decrease the efficacy of consequences as reinforcers or punishers (Laraway et al. 2003; Michael 2000; Sundberg 2013; for an MO account of eating behavior, see Tapper 2005; for an MO account of side effects of medications, see Valdovinos and Kennedy 2004). Events that increase the efficacy of consequences are establishing operations. Deprivation from cigarettes in a dependent smoker increases the efficacy of cigarettes as a reinforcer (a value-altering effect). An establishing MO will also evoke behaviors that have led to the reinforcer in the past, such as searching for a pack of cigarettes (a behavior-altering effect). Other examples of events that function as establishing operations include conditions of deprivation (from food, sex, sleep, social interaction, drugs of abuse), aversive stimulation (e.g., a headache, illness, heartburn), and the presence of illicit and licit drugs of abuse (e.g., marijuana may increase the value of food and evoke behavior that has led to food in the past). An MO can also decrease the efficacy of consequences, in which case the event is an abolishing operation (e.g., drinking a large volume of soda reduces the efficacy of soda as a reinforcer). In some cases, events may function as both establishing and abolishing operations. For example, the environmental conditions that lead to “stress” may enhance the value of certain activities such as sleep, drug use, or watching television, and simultaneously weaken others such as physical activity, socializing, and work-related tasks (Anderson et al. 2000; Dougher and Hackbert 2000). Conceptually, the physiological correlates, or endogenous events, associated with stress are concordant with the function of MOs (Thompson 2007). This is relevant because many engineers and health behavior scientists are using wearable sensors to detect endogenous events involving the autonomic nervous system (Boyer et al. 2012; Burns et al. 2011; Ertin et al. 2011; Plarre et al. 2011; Sun et al. 2012). The hope is that detecting endogenous events will help illuminate patterns between endogenous events and subsequent unhealthy behavior, which could lead to interventions to prevent the occurrence of unhealthy behavior.
Discriminative stimuli occasion responses, or make them more likely, by virtue of a differential history of reinforcement in the presence versus absence of these stimuli. Assuming that skipping a medication or binge eating, for instance, is maintained by attention from particular family members, the presence of those family members may serve as discriminative stimuli and make these responses more likely. In addition to stimuli that may occasion unhealthy behavior in naturalistic contexts, one purpose of technology-delivered stimuli is to serve as verbal discriminative stimuli1 to promote health behavior (Hayes et al. 1986). Verbal discriminative stimuli to promote health behavior may be called prompts, cues, or reminders. If these messages occasion the relevant behavior (e.g., exercise, medication adherence, abstaining from smoking), the behavior is considered an instance of rule-following. The consequences for rule-following may be social (in which case the rule is called a ply, and the behavior is called pliance), or they may be embedded in the natural consequences for following a rule (in which case the rule is called a track, and the behavior is called tracking; Hayes et al. 1986). A text message to take a medication may serve as a ply or a track, depending on the reinforcing consequences, for example, avoiding a scolding parent (ply) or attenuating a headache (track). Alternatively, a technology-based message may occasion behavior and require no explicit reinforcement due to a long history of reinforcement for similar rule-following behavior, which then generalizes to the novel technology-based stimulus (i.e., generalized rule-following; Palmer 2012).
Establishing operations such as food or drug deprivation can also enhance and broaden discriminative control (Lotfizadeh et al. 2012). In their review of the literature, Lotfizadeh et al. argued that establishing operations can increase not only the evocative strength of established discriminative stimuli but also of stimuli that are similar to the established discriminative stimuli. These findings may be relevant to understanding maintenance and relapse to substance use and other unhealthy behavior. Specifically, abstinence may increase stimulus control by already established stimuli such as particular people or settings, and this control may also generalize across a range of “untrained” stimuli. If drinking alcohol occurs in familiar bars, a lapse following abstinence may be occasioned by an unfamiliar restaurant or residence. This process should also apply to other health behavior where deprivation plays a role (e.g. eating, illicit drug use).
There are two main approaches to addressing the consequences associated with health behavior. The first approach, which is the most common approach in applied behavior analysis, is to identify the consequences that maintain unhealthy behavior and then eliminate or attenuate their influence on behavior (Beavers et al. 2013; Hanley 2012; Iwata et al. 1994). The assumption, born out by hundreds of studies, is that unhealthy behavior serves a function, or multiple functions, for the individual. Speaking loosely, the behavior serves a purpose (e.g., social attention, automatic reinforcement, escape or attenuation of an unpleasant event). A clinician using a function-based approach would assess and then eliminate or modify the consequences of unhealthy behavior, or teach new, healthy behavior that serves the same function as the unhealthy behavior. A function-based account can also be applied to behavior that occurs infrequently. For example, behavior such as medication taking or physical activity may occur at a low rate or not at all because they are punished by aversive consequences such as side effects or physical discomfort.
The second approach, which is the most common in the field of health behavior, is to introduce immediate, desirable consequences based on evidence of health behavior (Higgins et al. 2008). Behavioral theories of choice and behavioral economics posit that choice for one of two options is influenced by the relative reinforcing value associated with each option (Bickel et al. 1993; Bigelow et al. 1998; Heyman 2009; Silverman 2004). Thus, choices to abstain or use drugs, eat healthy food or unhealthy food, or take or skip a medication can be influenced by introducing immediate, desirable consequences for the healthy choices. Immediate consequences may be critical given that many of the consequences for healthy choices are intermittent and delayed (e.g., social consequences for weight loss). Some potential reinforcers in the case of technology-delivered stimuli are social and monetary consequences (Alessi and Petry 2013; Dallery and Raiff 2011; Higgins et al. 2008), points, and game-based stimuli (Hackenberg 2009; Morford et al. 2014; Raiff et al. 2012).
Technology-Based Assessment
Below we discuss technology-based assessment of antecedents, health behavior, and consequences. We have collapsed motivating operations and discriminative stimuli into one category labeled antecedents. In part, this is for convenience, but also because an antecedent could have motivative or discriminative functions, respondent functions, or no function for a particular individual. For example, the presence of friends could function as a discriminative stimulus or as an establishing operation depending on the individual’s history with respect to his or her friends and the behavior in question. Conceptual and empirical analysis should clarify whether the event signals the differential availability of a reinforcer (discriminative stimulus) or whether the event affects the differential value of an event as a reinforcer (motivating operation), or whether the antecedent functions in ways that we have not addressed in our basic outline of the four-term unit of analysis.
Assessing Antecedents with Active Input Using Handheld Computers or Smartphones
Ecological momentary assessment (EMA) is the most common method to conduct technology-based assessment of antecedents (Shiffman 2009a; Shiffman et al. 2008). Most applications of EMA use handheld computers or smart phones, and end users input information based on prompts at various times or based on events such as smoking a cigarette (Shiffman et al. 2008). EMA has been used to assess antecedent events associated with behavior such as alcohol use (Todd et al. 2009), illicit drug use (Buckner et al. 2012; Marhe et al. 2013; Shiffman 2009a, b), self-injury (Anestis et al. 2012; Armey et al. 2011), and behavior associated with mood and anxiety disorders (Forbes et al. 2012). Typically, EMA (a) occurs in naturalistic settings, (b) focuses on the participant’s internal experiences and antecedent situations, (c) samples behavior over long durations (e.g., weeks), and (d) occurs frequently (e.g., several times per day). EMA can therefore reveal behavioral variation over time and across contexts. Shiffman et al. note that EMA methods are well-suited to health-related behavior because it occurs repeatedly and usually in discrete bouts, thus enabling “prospective assessments of the flow of behavior and experience, and of the antecedents and consequences of events…” (p. 10).
Although a thorough review of EMA is beyond the scope of this article, research using EMA suggests that certain situations are more reliably associated with health behavior than others (Shiffman et al. 2008). In one relatively straightforward example, Mulvaney et al. (2012) tested the feasibility of using mobile phone-based EMA to assess adherence to diabetes self-management (e.g., glucose testing, insulin administration) in adolescents with type 1 diabetes. They found that the method was feasible, and moreover, that for a subset of adolescents, diabetes management was particularly challenging in the morning. This narrowing of the time window for deficient management could lead to further assessment and more targeted and efficient interventions.
In general, compliance with completing EMA assessments is good, particularly when the assessment is prompted by the electronic device (Shiffman et al. 2008). For example, several studies report over 90 % compliance with prompted EMA (e.g., Cain et al. 2009). High rates are not observed universally, however, and recent research has examined the conditions that may influence compliance. Sokolovsky et al. (2012) identified several predictors of compliance in a sample of adolescents. Five to seven times per day for 7 days, adolescents were prompted to report on social context, location, and mood. On average, adolescents completed 67.5 % of the 14,105 prompted EMAs. Sokolovsky et al. found that greater negative affect, cigarette smoking rate, alcohol use, and male gender predicted lower compliance with random EMA prompts. When analysis focused on predicting compliance from one completed prompt to the next prompt, the authors found that increased positive affect, being outside of the home, and longer interprompt interval predicted lower compliance.
Understanding sources of potential bias in EMA recording will be critical if researchers are to use EMA to assess the potential antecedents of unhealthy behavior. In addition, the validity of EMA in detecting antecedents will require further research. To our knowledge, no study has compared EMA to direct observation methods (or another gold standard) of antecedents of health behavior (for a discussion of direct observation, see Thompson and Borrero 2011). However, because many antecedents assessed with EMA consist of reports of endogenous events, direct observation methods may have limited utility in this domain. Although behavior analysts may be understandably skeptical about self-report methods, EMA offers advantages relative to traditional, questionnaire-based methods that occur at one or two time points during a study (e.g., real-time, frequent, longitudinal assessment in naturalistic settings). As such, EMA may be a valid and useful transducer of environmental and behavioral events (Critchfield et al. 1998), and these methods warrant more empirical attention by behavior analysts.
Assessing Antecedents with Wearable Sensors
Endogenous Antecedents
Several systems use a combination of wearable passive sensors and active input by the end user to detect physiological antecedents to unhealthy behavior (Ali et al. 2012; Crowley-Koch and Van Houten 2013; Ertin et al. 2011; Kaplan and Stone 2013; Kumar et al. 2013a; Plarre et al. 2011). For example, Boyer et al. (2012) developed the iHeal system to detect antecedents to drug use. The system consists of sensors to measure electrodermal responses, body motion, skin temperature, and (optionally) heart rate. The sensors wirelessly transmit the data to a mobile phone, and if elevated levels of activity are detected, the iHeal software triggers an EMA assessment of mood, behavior, and environmental context. The sensors and EMA data are used to iteratively train a machine learning algorithm to recognize the sensor-based profiles that may precede drug use (as opposed to other behavior like exercise). The system is still in the development phase, so no reliability or validity data are available.
One goal of the iHeal system is to detect risk, as measured by the sensors, early enough to allow treatment delivery via a mobile phone before drug use occurs. Other approaches use additional sensors such as electrocardiogram (ECG), respiratory-inductive plethysmograph bands to measure relative thorax volume and respiratory frequency, global positioning systems (GPS), and accelerometers to measure physical activity (Ertin et al. 2011; Kumar et al. 2013a; Plarre et al. 2011). Many of these approaches also use machine learning algorithms, in combination with user input to report emotional states and environmental variables, to detect a profile that indicates a particular physiological state or behavior. For example, Sun et al. (2012) used galvanic skin response (GSR), ECG, accelerometers, and various machine learning algorithms to differentiate experimentally induced stress from other physical activities such as walking. They found that one algorithm was able to isolate stress from physical activity with 90 % accuracy. One key in this work was the use of accelerometers, which allowed the algorithm to learn that activity-induced physiological responses did not reflect stress responses. The approach of Sun et al. (2012) and others like it are promising, but have yet to be thoroughly tested in naturalistic contexts.
To the extent that endogenous events are a function of MOs, it might be useful for future work to explicitly assess the potential MOs in addition to the sequence involving endogenous events and unhealthy behavior. Moreover, it might be useful to collect information about the full context in which endogenous responding is occurring, which means information about the components of the functional unit of analysis: MOs, discriminative stimuli, operant behavior, and consequences. Just as with overt behavior, endogenous events cannot be understood apart from the functional unit in which they participate (see Fig. 1; Thompson 2007). Although a virtue of mobile technology is that an intervention could be delivered in real-time in a naturalistic setting if some sequence were detected, the type of intervention may depend critically on the context in which the sequence occurs (Heron and Smyth 2010; Kaplan and Stone 2013). A conceptually systematic view of the interactions between endogenous events and their context will help broaden the range of possible interventions. For example, knowledge about the originating conditions of endogenous events and the consequences of unhealthy behavior may suggest interventions that remediate these conditions and consequences (Skinner 1953, p. 167). Such knowledge may even contraindicate certain interventions. If unhealthy behavior is maintained by social attention, for instance, then it may be counterproductive to provide access to peer-based support based on physiological precursors to unhealthy behavior.
Exteroceptive Antecedents
Functionality present in most mobile phones can be used to assess environmental antecedents to unhealthy behavior (e.g., smoking, consuming excessive amount of alcohol or food). Mobile phones can track a user’s location via GPS (Kerr et al. 2011), which can generate automated signals when a user is entering a risky area (e.g., a bar). Microphones in mobile phones have also been used to infer whether an individual is alone or surrounded by others (Lane et al. 2011). McClernon and Roy Choudhury (2013) discuss how mobile phones could be used to detect a number of antecedents to cigarette smoking, including driving in a car (assessed via accelerometer input), the presence of other people (assessed via microphone or Bluetooth detection of other mobile devices in the area), or standing outside (assessed via camera). The authors also noted that multiple inputs could be integrated to identify an antecedent. For example, arriving at a bar, a potential antecedent to smoking, could be assessed based on a mobile phone’s clock (e.g., 10:00 p.m.), GPS, and/or accelerometer. Although these examples pertain to smoking, they also apply to detecting antecedents of other health-related operant behavior such as overeating, inactivity, or use of illicit drugs.
A few researchers have harnessed technology to detect exteroceptive antecedents in the ways outlined above. Burns et al. (2011) developed a mobile phone- and Internet-based application, called Mobilyze!, to treat depression using behavioral activation therapy. Mobilyze! uses so-called context sensing techniques to predict patients’ mood, emotional, and motivational states, as well as contextual variables (e.g., activities, location, social context). Antecedent variables were derived from 38 sensors, most of which were housed in the mobile phone (e.g., GPS, accelerometer, missed call count, ambient light). In combination with EMA to identify mood, a machine learning algorithm was employed to generate individualized prediction models to identify specific user states (e.g., mood) from sensor values. In addition, based on the sensor data, Mobilyze! provided individualized behavioral activation treatment recommendations via phone and a website. Preliminary data suggest that this mHealth treatment is feasible and efficacious in treating depression (Burns et al. 2011). Another example is a mobile phone-based intervention to support recovering alcoholics (Gustafson et al. 2014). The intervention included a wide range of support services, including GPS detection of geographical areas that were identified as high risk for drinking. Upon detection of these areas via the mobile device, a message was sent to the individual inquiring whether he/she wished to be in that area. Although individuals in the mobile intervention showed lower drinking levels than a control group, it is not possible to determine whether the detection of risky areas contributed to these group differences.
Assessing Health Behavior
Active Input by an End User
EMA requiring active input by an end user into a mobile device represents the most common method to assess health behavior (Kaplan and Stone 2013; Shiffman et al. 2008). Just as with EMA assessment of antecedents, however, the validity of EMA in measuring health behavior requires further research. Space limitations preclude a thorough discussion of these issues in light of the heterogeneity of EMA methods, the health behavior targeted, and the standard used to evaluate EMA measures of behavior (see Shiffman et al. 2008). The lack of a true gold standard like direct observation is perhaps the greatest limitation in studies on the validity of EMA (Shiffman et al. 2008). Direct observation, however, is complicated because some unhealthy activities occur surreptitiously and at low rates (e.g., binge eating, drug use). In some cases, notably drug use, EMA can be compared to biochemical products of behavior as the standard for comparison. For example, Shiffman (2009b) found a statistically significant relation between EMA-reported cigarettes per day and breath carbon monoxide (CO; Pearson’s r = 0.35). When analysis was restricted to those subjects who showed high variability in breath CO, which presumably meant greater variation in smoking behavior, the correlation improved to r = 0.69. However, this study and others suggest considerable individual differences in agreement between self-reported EMA measures of drug use and biomarker levels. As just one example, Perrine et al. (1995) reported that within-subject correlations between self-reported drinks per day and blood alcohol concentration (BAC) ranged from −0.07 to 0.92. The sources of variability may stem from either the self-report or the BAC measures, as both entail measurement error. As new, potentially more accurate, biomarkers for alcohol and other substances are developed (see below), it will be useful to use them as standards for comparison for EMA methods. In addition, for more easily observed health behavior (e.g., activity, inactivity, eating), it will be useful to further evaluate the relation between EMA and direct observation measures under controlled conditions (Thompson and Borrero 2011).
Passive Input via Sensors
In addition to methods that require active input by the end user, researchers and software developers are generating a plethora of new devices to assess health behavior using passive sensors (Ali et al. 2012; Crowley-Koch and Van Houten 2013; Kumar et al. 2013a; Makeyev et al. 2012; for discussion of technology to detect health status and diagnostics, see Kumar et al. 2013a and Topol 2012). The sensors are passive in that they do not require active input by an end user, but they still require the end user to interact with or wear the device.
Several technologies assess discrete instances of behavior such as medication adherence (Bosworth 2012; Granger and Bosworth 2011). Medication event monitoring systems (MEMS) are pill bottles or containers that are fitted with microcircuitry. The microcircuitry records the time and date of each opening and closing of the container. This information is transmitted to research or medical personnel to track medication adherence, and it can be used to provide prompts, and monetary or social consequences to promote adherence (see below). MEMS have been used to assess adherence to a wide variety of medications such as highly active antiretroviral therapy (HAART; Krummenacher et al. 2011), analgesics (Oldenmenger et al. 2007), antipsychotics (Acosta et al. 2009; Remington et al. 2013), antidepressants (Lee et al. 2010a, b), antiepileptic medication (Brown et al. 2009), blood pressure-lowering medications (Zeller et al. 2007), and psychostimulants in children with ADHD (Charach et al. 2008). Smart blister packs accomplish the same functionality as MEMS. A blister pack houses each pill in one of many pockets in a thin card made of aluminum and paper. Instead of detecting pill container openings, they detect packet openings by using sensors attached to the packaging, or by placing sensor “stickers” on the back of an existing blister pack (van Onzenoort et al. 2012).
A limitation of MEMS and blister packs is that pill ingestion per se cannot be verified. One way to verify pill ingestion is to watch the process via video-enabled phones. The in-person equivalent to this process is called directly observed therapy (DOT), which is the model recommended by the World Health Organization to promote adherence to medication regimens such as tuberculosis treatment. DeMaio et al. (2001) used videophones to observe patients swallowing medication for tuberculosis. Adherence using video-based DOT (95 %) was equivalent to adherence using traditional DOT (97.5 %). Further, video-based DOT required only 20 h of staff time, compared to the 288 h (and 8,830 miles of travel) that would have been required had traditional DOT been used (see also Hoffman et al. 2010; Wade et al. 2012). In addition, new technologies are being explored to verify pill ingestion. For example, digital pills contain small microchips that interact with gastric juices to produce a voltage. The voltage can be detected by a small sensor adhered to the skin, similar to a Band-Aid, and the sensor can also record information about heart rate and body temperature (Zullig et al. 2014).
Future research should compare MEMS with other measures to evaluate whether MEMS openings reflect pill ingestion and the conditions under which discrepancies arise. Denhaerynck et al. (2008) examined the correspondence between the patient opening an electronic bottle cap and the immediate ingestion of the prescribed dose as measured by self-report. Participants (250 adult renal transplant patients) were asked to record discrepancies between MEMS openings and the ingestion of immunosuppressive drugs throughout a 3-month period. Twenty-three patients did not use the MEMS device as prescribed and were removed from analysis. Although results revealed that participants dosed correctly on 96.3 % of days, 155 (62 %) reported discrepancies between openings and actual medication ingestion (resulting in 1,084 deviations out of 44,761 events) Twenty-eight percent of the deviations involved early decants of pills that were ingested later. Other frequently noted reasons patients gave for the discrepancies were going out, being on a trip, and having a meeting. It is possible that the large size of the MEMS device limited its portability, which may become less of a concern as devices become smaller (e.g., smart blister packs). Overall, despite some potential discrepancies between MEMS openings and actual ingestion, MEMS are still considered a “gold standard” for medication assessment (Barnett et al. 2011; Riekert and Rand 2002; Williams et al. 2013).
Physical activity is another health behavior that can be monitored remotely with sensors. For example, accelerometers collect information about physical activity and inactivity by measuring changes in velocity over time (acceleration; Intille et al. 2011; King et al. 2013). This permits quantification of the intensity of physical activity. Most accelerometers estimate caloric expenditure, duration and intensity of physical activity, as well as sleep/wake patterns. The reliability and validity of these devices in estimating energy expenditure depends on several factors, such as the type of accelerometer, the location of the accelerometer on the body, the amount of time per day the device is worn, the type of activity (ambulatory versus isometric exercise), and the particular equation used to convert acceleration counts to energy expenditure (Fridlund Dunton et al. 2012; Rothney et al. 2008; see Plasqui et al. 2013 for a review).
Several accelerometers (e.g., the Actigraph triaxial accelerometer) can measure physical activity associated with most ambulatory movements (e.g., walking, running) and the absence of such activity (i.e., sedentary behavior). Thus far, most accelerometers are less capable of detecting energy expenditure associated with weight lifting, biking, and other nonambulatory activities. Although new devices are fusing sensors to measure physical activity by measuring perspiration, skin temperature, and heart rate (e.g., the BasisBand, BASIS Science, Inc.), evidence suggests that they do not improve estimation of energy expenditure (when compared to doubly labeled water estimates; Plasqui et al. 2013). One promising development is the use of new activity sensors, such as piezo-resistive sensors, which may permit detection of different activity types, such as lying, sitting or standing, active standing, walking, running, and cycling (Plasqui et al. 2013).
Transient Products of Health Behavior
Biomarkers can detect an increasing range of health behavior, and the technologies to detect biomarkers are becoming more affordable and practical. For example, paper microfluidics has been used to detect biomarkers of medication adherence (Lee et al. 2010b; for a review of applications of microfluidics, see Li et al. 2012). The technology involves a small test strip embedded with chemicals that react with the urine of individuals that adhere to a medication regimen (e.g., the first-line tuberculosis drug isoniazid). In one innovative application of paper microfluidics to isoniazid adherence (Barclay 2009), the test strip revealed a unique code which participants then transmitted via text to a server to verify adherence.
Another example of verifying medication adherence is through breath output. Morey et al. (2013) combined a food additive (2-butanol) with a medication. After ingestion, the additive was converted to 2-butanone, which was detected in breath output. The authors found that the method was safe, feasible, and not impacted by food intake, but future work is necessary to identify whether genetic differences may impact accuracy (due to genetic polymorphisms in enzymes responsible for the conversion to 2-butaone).
Technology-based methods to detect licit and illicit drug use are also becoming more practical and versatile (Bough et al. 2013). For example, Meredith et al. (2014) recently developed a prototype of a mobile phone-based breath CO monitor to detect smoking status. New alcohol breathalyzers include cameras, GPS, and face recognition software to remotely monitor intake and to authenticate the end user’s identity (Alcohol Monitoring 2013; see also Leffingwell et al. 2013). Recent drug use can also be detected in sweat (Gambelunghe et al. 2013). The Secure Continuous Remote Alcohol Monitoring (SCRAM, Alcohol Monitoring 2013) bracelet detects approximately 1 % of ingested alcohol that is excreted through the skin (Swift 2003). Although potentially more costly and invasive, new urine-based biomarkers of alcohol ingestion may increase the time window for detection relative to breath-based markers. For example, McDonell et al. (2012) used ethyl-glucuronide (EtG) in urine, which has a 2-day detection period, in a behavioral intervention to promote abstinence.
Assessing Consequences with Technology
EMA methods have been used to assess potential consequences of unhealthy behavior. For instance, researchers have examined whether automatic negative reinforcement—assessed via self-report of reductions in negative affect—is associated with smoking a cigarette or binge eating (Shiffman 2009a; Haedt-Matt and Keel 2011). Research has not clearly supported a negative reinforcement process in ongoing cigarette smokers (Shiffman 2009a), nor has it revealed a reduction in negative affect following binge eating (Haedt-Matt and Keel 2011). To our knowledge, only a handful of studies have used EMA to examine the consequences after unhealthy behavior (e.g., Mitchell et al. 2014; Piasecki et al. 2008, 2011; Shiffman and Kirchner 2009). Piasecki et al. (2011) used EMA to assess the effects of alcohol consumption on subsequent cigarette smoking and the effects of cigarette smoking on subsequent alcohol consumption. Current smokers who reported frequently drinking alcohol (N = 259) monitored their daily experiences for 21 days. The authors found that alcohol enhanced the pleasurable consequences of smoking more strongly than smoking enhanced the pleasurable consequences of alcohol, but both substances produced small increases in self-reported pleasure derived from the other substance. Given that the effects were small and only group averaged data were evaluated, it would be interesting to examine individual differences in the effects of these substances. Conceptually, even though the EMA method was designed to assess consequences of consumption, these value enhancing effects might be interpreted in light of the MO functions of these substances (Raiff and Dallery 2008).
Assessing the roles of consequences will enrich our understanding of the determinants of health behavior and could lead to more tailored, function-based interventions (Axelrod 1991). Indeed, an operant analysis involves idiographic assessment of the entire functional unit of analysis. Thus far, no technology-based study of health behavior has included idiographic assessment of consequences. Encouragingly, however, and perhaps by virtue of advances in technology, several health behavior researchers have advocated for within-subject analysis of the antecedent and consequent variables governing healthy and unhealthy behavior (Kanning et al. 2013; Riley et al. 2011; Shiffman 2014). Behavior analysts have expertise in using methods to not only detect instances of antecedents, behavior, and consequences, but also to assess whether these instances are functionally related to one another and not merely correlated (e.g., Beavers et al. 2013; Hanley et al. 2003; McComas et al. 2009). For example, contingency space analysis, which is a quantitative approach to identifying contingent relations, may help identify variables maintaining unhealthy behavior in naturalistic environments (see Martens et al. 2014). Moreover, behavior analysts have expertise in linking idiographic assessment to treatment, which is also a growing interest among health behavior researchers (e.g., Heron and Smyth 2010; Kaplan and Stone 2013; Riley et al. 2011). Thus, the extent to which functional assessment could be used to develop more targeted, personalized technology-based treatments is a compelling empirical question for behavior analysts interested in health behavior.
Technology-Based Interventions to Promote Health
Internet and Mobile Interventions
There is growing empirical support for Internet and mobile interventions for smoking (Dallery et al. 2014a), weight loss (Valle and Tate, in press), and physical activity (Davies et al. 2012). These interventions are usually derived from behavioral or cognitive-behavioral therapies and typically are interactive and include feedback, goal setting, and frequent monitoring of progress during treatment. Most systematic studies and meta-analyses have found that these interventions are more efficacious than standard care (nontechnology-based) control conditions.
In an effort to better understand the behavior change components involved in technology-based interventions, Valle and Tate (in press) reviewed 21 studies targeting dietary intake, weight loss, and physical activity. The authors focused on studies that compared technological delivery of treatment components to a technology-based control condition (e.g., a website with and without access to a component such as social support). They found that 19 studies used self-monitoring, 16 used feedback and tailoring (e.g., individualized goal setting based on changes in behavior relative to baseline levels), 14 used social support and social networking, and 19 used reminders or prompts to engage with intervention content. Relatively few interventions (<6) used reinforcement, modeling, contingency contracting, or problem solving. Roughly half of the reviewed studies supported the effects of most of the treatment components compared to control conditions. Many studies involved treatment packages with several components; thus, future component analyses will be valuable to isolate active components (Dallery et al. 2014b). Furthermore, given the mixed results across studies, future work should help illuminate the conditions under which these active components generate positive outcomes. For example, the effects of self-monitoring may depend on the frequency or mode of self-monitoring (e.g., frequent assessment via accelerometers versus intermittent assessment via self-weighing; Valle and Tate, in press).
Many mHealth interventions have relied heavily on antecedent manipulations such as text-based prompts, information, and reminders to promote health behavior (Barclay 2009; Bastawrous and Armstrong 2013; Foreman et al. 2012; Riley et al. 2011; Spring et al. 2012; Wise and Operario 2008). However, Kaplan and Stone (2013) found that of 20 randomized, controlled mHealth studies targeting obesity, smoking, diabetes management, and medication adherence, 55 % failed to show a clear benefit and 15 % had mixed results. Only 30 % (6 out of 20) demonstrated a clear effect of the mHealth intervention. In light of a behavior analytic framework, an antecedent intervention involving prompts and reminders may work if the relevant rule-following repertoire already exists and can be occasioned by the novel technology-based stimulus. In other words, the intervention would rely on generalized rule-following. Given that many of these interventions were unsuccessful, it might be insufficient to rely on generalized rule-following. Instead, embedding an antecedent manipulation with other components of the four-term contingency may be necessary. Tomlinson et al. (2013) noted that one rule of thumb based on the results of text-based interventions is that they work better when behavior is monitored. Although speculative, such monitoring in these interventions may enhance the functioning of the text as ply (i.e., social consequences may be likely for rule-following or breaking). Indeed, one major benefit of technology is that it can be used to monitor behavior for extended durations. A pliance function could be enhanced if behavioral monitoring were explicitly incorporated into the intervention. For example, Meredith et al. 2011 developed an Internet-based intervention in which quantitative measures of smoking status (breath CO in parts per million) were viewable by all members of small teams of smokers. Although this intervention was not combined with an antecedent manipulation involving texts, the point here is that technology-delivered stimuli may come to serve a discriminative function after explicit, behavioral engineering to generate this function (Ducharme and Worling 1994; Mace et al. 1990; Nevin 1996).
Kaplan and Stone (2013) noted that many unsuccessful mHealth interventions lacked an empirical and theoretical framework grounded in behavioral science. In a similar vein, Riley et al. (2011) observed that when a theory was used, the theory relied on dispositional constructs as the potential sources of behavior change (e.g., increases in self-efficacy). Because technology can both assess and adapt to change in health behavior in real-time, Riley et al. argued for alternative conceptual frameworks “that have dynamic, regulatory system components to guide rapid intervention adaptation based on the individual’s current and past behavior and situational context” (Riley et al. 2011, p. 54). One such framework is behavior analysis, in which the regulatory components and situational contexts are the components of the four-term functional unit. Advances in technology might illuminate these components in ways that previous methods have not or could not. In addition, as we suggested above, ongoing assessment of an individual’s health behavior and its antecedents and consequences may reveal functional relations and therefore more targeted treatment possibilities. As one potential point of departure, recent work by Normand and colleagues has revealed functional relations between physical activity and specific environmental contexts (e.g., social and physical environment) in children (Hustyi et al. 2012; Larson et al. 2013). This work did not include technology-based methods, but we could imagine a mobile phone-based method to detect location, social context, and physical activity (Burns et al. 2011; King et al. 2013). Such a method might identify contexts and times when inactivity is likely, which could lead modification of the context to increase activity. Alternatively, it could lead to tailored timings of mobile phone-based prompts and consequences to increase activity in specific situations (e.g., contexts in which sedentary behavior is likely; Fridlund Dunton et al. 2012).
The proposal to tailor the timing of intervention delivery is not novel. An entire class of technology-based interventions, called ecological momentary interventions (EMIs), refer to interventions that can be delivered to patients at specified moments as they go about their daily lives (for a review, see Heron and Smyth 2010). In some cases, EMIs function as behavior therapy extenders (e.g., providing reminders to complete relaxation training), while in others they represent stand-alone treatment packages. EMIs can also deliver “just-in-time” interventions (Heron and Smyth 2010; McClernon and Roy Choudhury 2013). “Just-in-time” refers to vulnerable, high-risk situations, which can be assessed using sensors and/or user input. The Mobilyze! behavioral activation intervention for depression noted above is an example of a just-in-time EMI. In the near future, we will witness an even greater number of EMIs relying on multidimensional assessment of antecedents and health behavior using wearable sensors. Researchers have also developed EMI interventions based on user-initiated input when participants ate a meal, exercised, experienced anxiety, or craved a cigarette (Heron and Smyth 2010). The nature of the EMI content varied across behaviors but typically consisted of behavioral strategies (messages to occasion coping responses based on unpleasant affective states, messages to substitute healthier behavior), cognitive strategies (messages to challenge distorted thinking), or brief counseling sessions enabled via mobile phones. Research suggests that EMIs are both feasible and efficacious for improving a variety of health-related outcomes including smoking cessation, weight loss, anxiety, and diabetes self-management (see Heron and Smyth 2010). Efficacy was generally indexed based on statistical significance, however, and not based on evaluation of the clinical significance of the magnitude of symptom or behavior change (Kazdin 1999). Nevertheless, the strategy underlying EMIs represents an appealing way to change behavior in naturalistic contexts. Behavior analysts could make significant contributions to this area by developing methods to integrate function-based assessment and treatment and by harnessing technology-based methods to introduce immediate consequences based on evidence of behavior change.
Behavior analytic principles have been incorporated more explicitly into several technology-based interventions. In one intervention, the principles underlying the skills component of the community reinforcement approach (CRA) were translated into a computerized intervention, the Therapeutic Education System (TES). CRA is grounded in a behavioral analysis of drug dependence where drugs are viewed as competing with more delayed prosocial reinforcers because of their more immediate reinforcing effects (Higgins et al. 1994; Hunt and Azrin 1973). The skills training component of CRA teaches skills and encourages behaviors that increase nondrug sources of reinforcement. To address these skills, TES employs 65 modules with an optional contingency management component. These modules include improving behavioral skills (refusal skills, managing harmful thoughts, etc.), improving psychosocial functioning (family/social relations, managing negative moods, etc.), and reducing behavior that may place one at risk for HIV, hepatitis, or sexually transmitted infections. TES is self-directed, includes functionality to build individualized treatment plans, assesses a patient’s comprehension of material, and adjusts the pace and level of repetition of material to promote skills mastery. Several randomized trials have found that TES produced outcomes superior to standard substance abuse treatment and improved objectively measured drug abstinence to rates produced by trained clinicians delivering comparable therapy (Bickel et al. 2008; Marsch and Bickel 2004; Marsch et al. 2014).
In addition, Bricker et al. (2013) developed and tested the first web-based acceptance and commitment therapy (ACT) intervention for smoking cessation (WebQuit.org). ACT for smoking focuses on acknowledging and accepting emotions, thoughts, and other antecedents to smoking and weakening their control over subsequent behavior and identifying values and behavior change procedures to commit to these values (e.g., smoking cessation). Core processes of ACT were embedded in the website by using personalized quit plans along with videos of former smokers sharing success stories and modeling acceptance. Relative to another website (Smokefree.gov), cessation rates were higher for the web-based ACT intervention than the control website (23 versus 10 %) at a 3-month follow-up. Interestingly, statistical analysis revealed that these increases were related to ACT theory-based increases in acceptance of physical, cognitive, and emotional cues to smoke.
Contingency Management Interventions
Another clear example of translating behavioral principles into technology-based practices is the development of contingency management (CM) interventions (Dallery and Raiff 2011; Marsch and Dallery 2012). Under CM procedures, individuals receive positive consequences contingent on a target behavior (e.g., objective evidence of drug abstinence, medication adherence). These tangible consequences typically include recreational items, retail goods, or commercial services. A large number of studies over the past 30 years have established the efficacy and versatility of CM (e.g., Higgins et al. 1994; Kidorf and Stitzer 1999; Robles et al. 2000; Silverman et al. 1996a, b, c; Stitzer et al. 1982). The main requirements for any CM intervention include a monitoring system to frequently and objectively detect a target behavior and a delivery system to provide desirable consequences when the target behavior occurs (Dallery and Raiff 2011).
Technology-Based Monitoring and In-Person CM Delivery Systems
Most CM interventions involve some form of technology as part of the monitoring system and in-person methods to deliver consequences based on evidence of the targeted behavior. CM interventions targeting substance abuse, for example, use technology-based methods to detect drug metabolites and research assistants or counselors to deliver monetary consequences based on evidence of abstinence (for a review, see Silverman 2004). In addition to targeting substance use, technology can be used with CM interventions to promote medication adherence (Carroll and Rounsaville 2007). Several randomized clinical trials have demonstrated that CM can promote adherence to HAART based on MEMS cap openings in HIV-infected drug users (Rigsby et al. 2000; Rosen et al. 2007; Sorensen et al. 2007). In Sorensen et al., research assistants met with participants twice weekly for 12 weeks to review MEMS openings and provide vouchers. Vouchers had monetary value and could be exchanged in the community. Similarly, in Rosen et al., counselors met with participants weekly to review MEMS-generated printouts of adherence and provide prizes based on adherence over the 16-week intervention period. The prizes were determined by drawing a card from a bowl containing cards that specified prizes of different magnitudes (e.g., $1, $20, $100). Cards could be redeemed for prizes that were stored in a cabinet and included bus tokens, clothing, small appliances, gift certificates for local stores, and other items. The effect sizes in these CM studies are among the highest produced by behavioral interventions to promote adherence among HIV-infected drug users (Rosen et al. 2007; Sorensen et al. 2007). Moreover, in the Rosen et al. study, patients in the CM group demonstrated lowered viral load compared to the control group. These results are promising, as estimates suggest that at least 50 % of HIV-infected drug users do not adhere consistently with prescribed regimens. Consistent adherence is associated with improved immunological and virologic outcomes, less development of drug-resistant HIV strains, reduced probability of HIV transmission, and slower progression to AIDS.
Volpp et al. (2008) also used CM to promote warfarin adherence. Warfarin is used to manage thromboembolism (Hyers et al. 2001; Gullov et al. 1998), and up to 40 % of warfarin users miss 20 % or more of their doses (Kimmel et al. 2007), which limits the drug’s ability to prevent embolic events. Adherence was monitored and consequences were delivered based on MEMS openings. Upon confirming that the medication was taken as prescribed, participants were eligible to receive payment in a daily lottery with different odds of receiving a small or a large monetary consequence ($10 or $100). Research staff reviewed MEMS reports and conducted lottery procedures in person for 3 months. The MEMS device also emitted a reminder chime for pill-taking. In two experiments, the proportion of time that anticoagulation levels were outside the therapeutic range decreased by 23–25 % (Volpp et al. 2008). Although these reductions are large, it is not clear whether reductions were due to CM, to the use of the audible chime that signaled when pill taking should occur, or to their combined effects.
CM has also been used to increase adherence to regimens that require regular monitoring of health status. For example, measuring lung function using peak expiratory flow (PEF) must occur regularly to prevent asthmatic episodes (Kamps et al. 2001; Legoretta et al. 1998). Burkhart et al. (2007) used an AccuTrax Personal Diary Spirometer (Ferraris Medical and Pulmonary Data Services Instrumentation, Louisville, CO), which is a lightweight, handheld electronic device that contains a microchip to record the date, time, and PEF value each time the device is used. The CM portion of the intervention consisted of children and their parents entering into contingency contracts, as well as parents cuing the children to monitor their PEF and providing verbal praise when the child did so. Adherence to PEF monitoring in the experimental and control groups did not differ at the end of the baseline period or at week 8. However, children in the experimental group demonstrated higher adherence to daily electronically monitored PEF at week 16 (maintenance period). The effects of CM in future research may be enhanced if more valuable reinforcers (e.g., monetary consequences) are delivered contingent on adherence.
As new, low-cost, technology-based monitoring systems are developed, additional possibilities will emerge to link them with CM. For example, Larson et al. (2012) described a promising method to measure lung function using a mobile phone’s microphone. This method could be more accessible and scalable than a separate PEF monitor. As another example, pulse oximetry can be used as part of cardiopulmonary rehabilitation for patients with chronic obstructive pulmonary disease. Like many health regimens, adherence to measuring pulse oximetry is low (Tang et al. 2012). Bluetooth-enabled pulse oximeters provide a relatively simple method to measure adherence, which also could be linked to a CM intervention.
Combined Technology-Based Monitoring and CM Delivery Systems
Dallery and colleagues developed and evaluated an Internet-based CM intervention to promote smoking cessation (Dallery et al. 2007; Dallery et al. 2008; Dallery and Raiff 2011; Stoops et al. 2009). Smokers used web cameras to record themselves blowing into CO monitors twice per day, typically for about 7 weeks, which provided evidence of smoking status (i.e., by meeting CO cutpoints). The CM delivery system also involved technology. Desirable consequences (i.e., money and social feedback) were delivered immediately to individuals who met CO cutpoints for abstinence using an automated, web-based program called Mōtiv8 (in some early versions of the intervention, consequences were delivered via e-mail). Researchers or clinicians were still necessary to monitor and manage the system and to verify the authenticity of the videos, so the system was not fully automated.
The Mōtiv8 system represents an advance in the evolution of CM interventions. A major obstacle in applying CM was obtaining reliable, valid, and frequent measures of health behavior. In the case of cigarette smoking, breath CO samples should be collected at least twice per day to measure smoking status (Javors et al. 2005). In-person methods would entail either clinic staff making visits to patients’ homes (Crowely et al. 1991), or patients making visits to the clinic (e.g., Lamb et al. 2004; Rand et al. 1989). Frequent visits would be necessary for both monitoring of CO and delivery of consequences. These procedures would be too burdensome for practical and effective implementation of CM, particularly for disabled, rural, or low income smokers. Although these challenges apply to smoking, the same issues regarding frequent monitoring and reinforcement apply equally to other health behaviors such as medication adherence, physical activity, illicit drug use, and healthy eating.
In contrast to traditional in-person methods, technology-based methods permit frequent assessment for sustained periods. In several studies using the Mōtiv8 system, adherence to a twice-daily CO regimen was high across a 7-week intervention period, ranging from 67 % (Stoops et al. 2009) to 98 % (Dallery et al. 2007). Results also suggest that Internet-based CM can promote smoking cessation in heavy (Dallery et al. 2007), rural (Stoops et al. 2009), and adolescent (Reynolds et al. 2008) smokers. In one recent randomized clinical trial, Dallery et al. (2013b) found that Internet-based CM promoted higher rates of abstinence (66.7 % negative COs) than a control group (25 % negative COs) during treatment. In addition to efficacy, Raiff et al. (2013) evaluated the social validity of Internet-based CM and found high levels of acceptability among smokers, nonsmokers, and health-care professionals (for details about social validity assessment in clinical research, see Foster and Masch 1999).
The Internet-based CM model has been extended in several ways. First, Hertzberg et al. (2013) demonstrated the feasibility and preliminary efficacy of a mobile phone-based method to collect objective evidence of smoking status via video and deliver CM. Ninety-three percent of the video samples were submitted, and at the end of the 4-week intervention, CO-verified quit rates were 82 % in the CM group and 45 % in the control group. Mobile phone methods have the potential to substantially increase access to CM interventions. Second, Meredith et al. (2011) used the Internet-based CM model and incorporated group contingencies, where small groups of smokers must collectively achieve cessation goals to receive desirable consequences. Participants provided and/or received encouragement, feedback, and support via a discussion board integrated into the Mōtiv8 architecture. Using a multiple baseline design, Meredith et al. found that fewer than 1 % of CO samples submitted during baseline were negative for smoking, compared to 57 % submitted during the treatment phase. In addition, 65 % of participants’ comments on the online peer support forum were rated as positive by independent observers. Third, Dallery et al. (2008) employed Internet-based CM model in combination with a deposit contract procedure. The procedure required an up-front deposit by the participant, which could be earned back based on evidence of abstinence. In this small pilot study, the deposit contract procedure produced equivalent rates of abstinence relative to a group that received a traditional, earnings-only CM procedure, and the deposit procedure resulted in cost savings relative to the earnings-only group.
In addition to smoking cessation, two technology-based CM interventions have been used to promote alcohol abstinence. In the first intervention, Barnett et al. (2011) used SCRAM to monitor alcohol intake. Monetary reinforcement was sent via the Internet based on the SCRAM results. Compared to a SCRAM monitoring phase during the first week of the study, average transdermal alcohol concentrations decreased by 72 % when Internet-based CM was used during the second and third weeks. In the second intervention, Alessi and Petry (2013) used video-based monitoring via mobile phones to assess abstinence from alcohol. For 4 weeks, researchers texted participants one to three times daily to indicate that a breathalyzer test was due within the hour. Participants were randomized to either a monitoring alone or to a monitoring plus CM condition. “Thank you” texts in the CM condition included the monetary amount earned and the amount possible for the next negative sample. Adherence to submitting the videos was high and equivalent between groups (88.6 % of the scheduled videos were submitted), and the CM group submitted significantly more negative breath samples than the monitoring alone group (87.1 versus 66.9 %).
Internet-based CM has also been employed to improve diabetics’ adherence to glucose monitoring (Raiff and Dallery 2010). Internet-based CM, which involved slight modifications to the video confirmation and reinforcement procedure outlined above for the Mōtiv8 program, improved adherence to blood glucose monitoring in four teenagers (aged 12–17) diagnosed with type 1 diabetes. Prior to the Internet-based CM intervention, participants tested their blood glucose an average of 1.7 times per day (range 0–4), which falls below the 4–6 times per day recommended for teenagers (Silverstein et al. 2005). During the intervention, all participants increased their frequency of testing to an average of 5.7 per day (range 4–8). When the intervention was removed, testing decreased to an average of 3.1 tests per day (range 2–5). This experiment was relatively brief, and future work should implement the procedure for a long duration and address longer term outcomes.
Several research groups have capitalized on accelerometer technology to monitor and promote physical activity (Donlin Washington et al. 2014; Van Camp and Hayes 2012). For example, Kurti and Dallery (2013) implemented an Internet-based CM intervention in which monetary consequences were delivered contingent on participants meeting a gradually increasing series of activity goals over successive 5-day blocks. Similar to the smoking intervention described above, participants used web cameras to submit videos of their daily activity totals (steps per day measured by a Fitbit®). All six participants increased their activity according to experimenter-arranged criteria. In addition, King et al. (2013) developed several software applications that use a smartphone’s built-in accelerometer, instead of a separate external accelerometer, to deliver positive consequences (e.g., text-based supportive statements) contingent on meeting activity goals. The software applications included additional treatment components (see King et al. 2013 for details). Overall results indicated that the applications were acceptable to participants and efficacious in increasing moderate-to-vigorous intensity physical activity and decreasing leisure time sitting during the 8-week treatment period.
Challenges and Opportunities Associated with Technology-Based Contingency Management
There are three main challenges associated with technology-based CM interventions: cost, sustainability, and maintenance. Although the cost of monetary incentives is often viewed as a barrier to dissemination (Petry and Simcic 2002), research in the field of substance abuse suggests that CM interventions are cost-effective (Olmstead et al. 2007a, b; Sindelar et al. 2007). No study has assessed the cost-effectiveness of technology-based CM procedures. To the extent that technology lowers personnel and other resources to deliver treatment, costs may prove to be even less of a concern than for equivalent in-person methods. Behavioral monitoring systems for several health behaviors are also becoming more affordable (e.g., Erb et al. 2014; King et al. 2013). Finally, technology can enable lower cost methods to deliver CM such as intermittent, prize-based consequences, group contingencies, or deposit contracting (Dallery and Raiff 2011). Overall, the challenge of costs associated with technology-based CM may become more of a myth than a reality.
Sustainability refers to delivering CM interventions for extended durations. Many behavioral health issues such as drug use, unhealthy eating, and inactivity are enduring response patterns. Therefore, in some cases, achieving enduring change may require enduring interventions. Silverman and colleagues generated an innovative and sustainable model in which access to a workplace was made contingent on drug abstinence (DeFulio et al. 2009; Donlin Washington et al. 2008; Silverman et al. 2005, 2007). This is an excellent example of how a sustainable CM intervention can be “embedded” in a system of care. An intriguing possibility for embedding CM in modern health care stems from the implementation of the Patient Protection and Affordable Care Act. One section of the act specifies that up to 30 % of an employee’s health insurance premium can be used in the form of outcome-based wellness incentives (Madison et al. 2013). Potentially, technology could perform “automated hovering” for extended durations and also perform “automated nudging” by delivering reimbursements or other allowable consequences based on evidence of health behavior.
Maintenance refers to lasting change in behavior following termination of an intervention. Behavior such as drug use, physical activity, and unhealthy eating frequently (but not always: Higgins et al. 1994) reverts to pre-intervention levels after CM is withdrawn (Petry 2010). One area for future research is further translation of behavioral principles and procedures to maintain changes in behavior. Most CM procedures provide consequences for the absence of some behavior (i.e., they are equivalent to the differential reinforcement of other behavior), and they do not explicitly shape or reinforce alternative behavior that is incompatible with unhealthy behavior (cf. Iguchi et al. 1997). Several researches have assessed whether complementary treatments can improve CM outcomes, such as cognitive-behavioral techniques that explicitly target alternative behavior and coping strategies in ways that CM interventions do not. The evidence is mixed, however, as to whether developing these skills promotes more durable changes in behavior relative to CM alone (Carroll et al. 2012; Hall et al. 2011; Silverman 2004). Also, these results apply to substance use outcomes; thus, the generality of these findings to other health behavior should not be assumed.
Another possibility to maintain treatment gains is a greater focus on shifting from the contrived consequences associated with CM to more natural consequences. Such a strategy might work for environments in which previously untapped reinforcing consequences already exist or can be developed (Stokes and Baer 1977). For example, during and following a CM intervention, family members, significant others, or online communities could be enlisted to detect and reinforce instances of healthy eating or physical activity with the help of technology-based systems (Meredith et al. 2011). Several systems already exist that perform many of these functions, most notably for physical activity via accelerometers and online communities. The line between maintenance and sustainability may become increasingly blurred as technology-based systems for health behavior “weave themselves into the fabric of everyday life until they are indistinguishable from it” (Weiser 1991, p. 94; Kumar et al. 2013a).
Behavior Analysis and Technology-Based Assessment and Treatment of Health Behavior
One theme of the current article is that concepts and methods derived from behavior analysis can inform technology-based assessment and intervention. Specifically, technology-based approaches may be improved by concepts and methods that emphasize (a) the role of each component of the four-term unit in influencing health behavior, (b) the importance of idiographic and frequent assessment of these components, (c) the use of assessment to determine the nature of treatment, and (d) the use of empirically supported principles and procedures in developing interventions.
As reviewed above, few of these elements have been translated in the realm of health behavior. One exception is the translation of empirically supported principles and procedures in the development of technology-based CM (see Silverman 2004 for similar discussion). This work relied on behavior analytic research regarding the effects of variables such as reinforcer delay, magnitude, response effort, and the schedule of reinforcement on operant behavior. Knowledge of the basic principles and procedures of operant behavior will help increase the likelihood of choosing parameters that result in good outcomes. Selecting incorrect procedures may render the intervention ineffective, which could lead to the conclusion that the principles underlying the intervention do not work (Dallery et al. 2012; Hand et al. 2014; Meredith et al. 2013). Similarly, a tailored intervention based on the causes for health behavior may fail if the functional determinants are not addressed for each individual. For these reasons, behavior analysts can and should play a critical role in developing, implementing, and evaluating novel technology-based interventions.
Furthermore, technology-based methods entail practical, methodological, and conceptual advantages for behavior analysis. The main practical advantage of using technology to deliver behavioral interventions is dissemination potential. Delivering behavioral treatment in person requires staffing and travel that may be prohibitive in some environments. Technology can circumvent most personnel and geographical restrictions. Additionally, in the USA, the fastest growing users of mobile devices include African American, Hispanic, and low income families (Zickuhr and Smith 2012). Technology has the potential to narrow the “access gap” to behavioral health interventions and reduce health disparities in disadvantaged and hard-to-reach populations (Gibbons et al. 2011). A second practical advantage of technology is its ability to broaden the scope of behavior and client populations that behavior analysts can reach with treatment. Indeed, many researchers and clinicians have lamented the limited scope of behavioral interventions, despite their potential to address a wide range of socially relevant behavior (e.g., Friman 2010; Normand and Kohn 2013).
An additional advantage of technology is that it facilitates the use of research designs that focus on changing an individual’s behavior over time (Dallery et al. 2013a; Dallery and Raiff 2014). For example, single-case research designs require frequent assessment of health behavior, which is more feasible with technology than traditional, in-person methods. In fact, a number of health behavior scientists and engineers have lauded the merits of single-case designs to evaluate technology-based interventions (Duan et al. 2013; Kumar et al. 2013b; Lillie et al. 2011). In addition to single-case experiments, technology-based assessment has led researchers to propose novel research methods relative to standard randomized, controlled trials. Many of these methods embrace individual differences in ways that standard randomized clinical trials do not. Collins et al. (2005, 2007) have suggested designs derived from engineering, such as sequential multiphase optimization treatment (SMART) designs. These designs allow for adaptive interventions, in which the type or dosage of a treatment is altered based on patient characteristics or responses. The intervention entails a series of decision rules about when and how to modify the intervention. These rules often involve individual differences between participants to optimize outcomes, for example increasing the dose of an intervention for a nonresponsive participant or decreasing the dose for a responsive participant to reduce cost. As with single-case designs, these designs can be applied without technology, but both designs are more easily achieved with technology-enabled, frequent assessment of behavior.
Another advantage of technology is more conceptual, but it stems from advances in assessment afforded by technology. That is, because technology-based assessment can generate a continuous time series of behavior, conceptual accounts of health behavior may increasingly emphasize environmental causation. Hineline (1990) discussed how continuous monitoring of behavior across changes in environmental conditions leads “inexorably to an environment-based account” of the causes of behavior. In contrast, assessment methods that take only a snapshot of behavior in time are more likely to engender dispositional, internal causes of behavior. An observer who lacks information about the relations between environmental events and behavior over time is likely to make the “fundamental attribution error” and incorrectly posit dispositional causes of behavior (Hineline 1990). A version of this error may become tempting as technological methods to assess sequences between endogenous events (e.g., stress) and unhealthy behavior become more ubiquitous. Avoiding this error will involve awareness and assessment of the four-term unit of analysis and contextualizing the endogenous event as part of this unit. Interestingly, environment-based accounts may be gaining traction in the health behavior literature. The recommendation of Riley et al. (2011) for conceptual frameworks with “dynamic, regulatory system components…based on the individual’s current and past behavior and situational context” (p. 54) is a good example. An increased focus on technological assessment of dynamic environment-behavior relations, as opposed to dispositional accounts of behavior, will lead to novel insights into the causes of health behavior and therefore more effective interventions.
A New Frontier
Twyman (2011) called the growing use of technology a behavioral cusp for the field of behavior analysis. A behavioral cusp occurs when behavior change like learning to walk or talk results in “new contingencies that have even more far reaching consequences” (Rosales‐Ruiz and Baer 1997). When behavioral technology and digital technology are more fully integrated, the consequences for behavior analysis could be far reaching indeed. Topol (2012) outlined a similar outcome in The Creative Destruction of Medicine: How the Digital Revolution Will Create Better Health Care. He described how the emergence of mobile phones, Internet connectivity, digital sensors, social networks, and other advances in medicine such as genomics have created a “super-convergence” of technology and medical science. He predicted that the super-convergence will lead to a new medical science focused on personalized diagnostics and treatment in real time and with minimal geographical restrictions. A similar possibility exists for behavioral science. Behavior analysis already embraces personalized, idiographic assessment and treatment, as well as real-time modification of environment-behavior relations. Thus, rather than a destruction of behavioral science, we could witness a “super-expansion” as technology and behavior analysis converge.
Acknowledgments
The preparation of this paper was supported in part by Grants P30DA029926 and R01DA023469 from the National Institute on Drug Abuse. We thank Brantley Jarvis and Paul Soto for helpful comments on a previous draft of this manuscript.
Footnotes
Distinguishing between the discriminative, motivative, and other functions of verbal stimuli is beyond the scope of this paper; for a discussion of alternative functions of verbal stimuli, see Schlinger (1993).
References
- Acosta FJ, Bosch E, Sarmiento G, Juanes N, Caballero-Hidalgo A, Mayans T. Evaluation of noncompliance in schizophrenia patients using electronic monitoring (MEMS®) and its relationship to sociodemographic, clinical and psychopatholoigcal variables. Schizophrenia Research. 2009;107:213–217. doi: 10.1016/j.schres.2008.09.007. [DOI] [PubMed] [Google Scholar]
- Alcohol Monitoring Systems (2013). Retrieved from http://www.alcoholmonitoring.com/index/scram/scram-remote-breath
- Alessi SM, Petry NM. A randomized study of cellphone technology to reinforce alcohol abstinence in the natural environment. Addiction. 2013;108(5):900–909. doi: 10.1111/add.12093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ali, A. A., Hossain, S. M., Hovsepian, K., Rahman, M. M., Plarre, K., & Kumar, S. (2012). mPuff: automated detection of cigarette smoking puffs from respiration measurements. Paper presented at the Proceedings of the 11th International Conference on Information Processing in Sensor Networks, 269–280.
- Anderson CM, Hawkins RP, Freeman KA, Scotti JR. Private events: do they belong in a science of human behavior? The Behavior Analyst. 2000;23(1):1. doi: 10.1007/BF03391995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anestis MD, Silva C, Lavender JM, Crosby RD, Wonderlich SA, Engel SG, Joiner TE. Predicting nonsuicidal self-injury episodes over a discrete period of time in a sample of women diagnosed with bulimia nervosa: an analysis of self-reported trait and ecological momentary assessment based affective lability and previous suicide attempts. The International Journal of Eating Disorders. 2012;45(6):808–811. doi: 10.1002/eat.20947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Armey MF, Crowther JH, Miller IW. Changes in ecological momentary assessment reported affect associated with episodes of nonsuicidal self-injury. Behavior Therapy. 2011;42(4):579–588. doi: 10.1016/j.beth.2011.01.002. [DOI] [PubMed] [Google Scholar]
- Asch DA, Muller RW, Volpp KG. Automated hovering in health care—watching over the 5,000 hours. The New England Journal of Medicine. 2012;367(1):1–3. doi: 10.1056/NEJMp1203869. [DOI] [PubMed] [Google Scholar]
- Axelrod S. Smoking cessation through functional analysis. Journal of Applied Behavior Analysis. 1991;24:717–718. doi: 10.1901/jaba.1991.24-717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barclay E. Text messages could hasten tuberculosis drug compliance. The Lancet. 2009;373(9657):15–16. doi: 10.1016/s0140-6736(08)61938-8. [DOI] [PubMed] [Google Scholar]
- Barnett NP, Tidey J, Murphy JG, Swift R, Colby SM. Contingency management for alcohol use reduction: a pilot study using a transdermal alcohol sensor. Drug and Alcohol Dependence. 2011;118(2):391–399. doi: 10.1016/j.drugalcdep.2011.04.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bastawrous A, Armstrong MJ. Mobile health use in low- and high-income countries: an overview of the peer-reviewed literature. Journal of the Royal Society of Medicine. 2013;106(4):130–142. doi: 10.1177/0141076812472620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beavers GA, Iwata BA, Lerman DC. Thirty years of research on the functional analysis of problem behavior. Journal of Applied Behavior Analysis. 2013;46:1–21. doi: 10.1002/jaba.30. [DOI] [PubMed] [Google Scholar]
- Bickel WK, DeGrandpre RJ, Higgins ST. Behavioral economics: a novel experimental approach to the study of drug dependence. Drug and Alcohol Dependence. 1993;33(2):173–192. doi: 10.1016/0376-8716(93)90059-y. [DOI] [PubMed] [Google Scholar]
- Bickel WK, Marsch LA, Buchhalter AR, Badger GJ. Computerized behavior therapy for opioid-dependent outpatients: a randomized controlled trial. Experimental and Clinical Psychopharmacology. 2008;16(2):132–143. doi: 10.1037/1064-1297.16.2.132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bigelow GE, Brooner RK, Silverman K. Competing motivations: drug reinforcement vs non-drug reinforcement. Journal of Psychopharmacology (Oxford, England) 1998;12(1):8–14. doi: 10.1177/026988119801200102. [DOI] [PubMed] [Google Scholar]
- Bosworth HB. How can innovative uses of technology be harnessed to improve medication adherence? Expert Review of Pharmacoeconomics & Outcomes Research. 2012;12(2):133–135. doi: 10.1586/erp.12.6. [DOI] [PubMed] [Google Scholar]
- Bough KJ, Lerman C, Rose JE, McClernon FJ, Kenny PJ, Tyndale RF, Amur S. Biomarkers for smoking cessation. Clinical Pharmacology and Therapeutics. 2013;93(6):526–538. doi: 10.1038/clpt.2013.57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boyer EW, Fletcher R, Fay RJ, Smelson D, Ziedonis D, Picard RW. Preliminary efforts directed toward the detection of craving of illicit substances: the iHeal project. Journal of Medical Toxicology : Official Journal of the American College of Medical Toxicology. 2012;8(1):5–9. doi: 10.1007/s13181-011-0200-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brennan, J. (2013) Pew Internet: mobile. Retrieved from www.pewinternet.org.
- Bricker J, Wyszynski C, Comstock B, Heffner JL. Pilot randomized controlled trial of web-based acceptance and commitment therapy for smoking cessation. Nicotine & Tobacco Research. 2013;15(10):1756–1764. doi: 10.1093/ntr/ntt056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown I, Sheeran P, Reuber M. Enhancing antiepileptic drug adherence: a randomized controlled trial. Epilepsy & Behavior. 2009;16(4):634–639. doi: 10.1016/j.yebeh.2009.09.014. [DOI] [PubMed] [Google Scholar]
- Buckner JD, Crosby RD, Silgado J, Wonderlich SA, Schmidt NB. Immediate antecedents of marijuana use: an analysis from ecological momentary assessment. Journal of Behavior Therapy and Experimental Psychiatry. 2012;43(1):647–655. doi: 10.1016/j.jbtep.2011.09.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burkhart PV, Rayens MK, Oakley MG, Abshire DA, Zhang M. Testing an intervention to promote children’s adherence to asthma self-management. Journal of Nursing Scholarship: An Official Publication of Sigma Theta Tau International Honor Society of Nursing/Sigma Theta Tau. 2007;39(2):133–140. doi: 10.1111/j.1547-5069.2007.00158.x. [DOI] [PubMed] [Google Scholar]
- Burns MN, Begale M, Duffecy J, Gergle D, Karr CJ, Giangrande E, Mohr DC. Harnessing context sensing to develop a mobile intervention for depression. Journal of Medical Internet Research. 2011;13(3):158–174. doi: 10.2196/jmir.1838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cain AE, Depp CA, Jeste DV. Ecological momentary assessment in aging research: a critical review. Journal of Psychiatric Research. 2009;43:987–996. doi: 10.1016/j.jpsychires.2009.01.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carroll KM, Rounsaville BJ. A perfect platform: combining contingency management with medications for drug abuse. The American Journal of Drug and Alcohol Abuse. 2007;33(3):343–365. doi: 10.1080/00952990701301319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carroll KM, Nich C, Lapaglia DM, Peters EN, Easton CJ, Petry NM. Combining cognitive behavioral therapy and contingency management to enhance their effects in treating cannabis dependence: less can be more, more or less. Addiction (Abingdon, England) 2012;107(9):1650–1659. doi: 10.1111/j.1360-0443.2012.03877.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Charach A, Gajaria A, Skyba A, Chen S. Documenting adherence to psychostimulants in children with ADHD. Journal of the Canadian Academy of Child and Adolescent Psychiatry/Journal De l’Académie Canadienne De Psychiatrie De l’Enfant Et De l’Adolescent. 2008;17(3):131–136. [PMC free article] [PubMed] [Google Scholar]
- Collins LM, Murphy SA, Nair VN, Strecher VJ. A strategy for optimizing and evaluating behavioral interventions. Annals of Behavioral Medicine: A Publication of the Society of Behavioral Medicine. 2005;30(1):65–73. doi: 10.1207/s15324796abm3001_8. [DOI] [PubMed] [Google Scholar]
- Collins LM, Murphy SA, Strecher V. The multiphase optimization strategy (MOST) and the sequential multiple assignment randomized trial (SMART): new methods for more potent eHealth interventions. American Journal of Preventive Medicine. 2007;32(5):S112–S118. doi: 10.1016/j.amepre.2007.01.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Critchfield TS, Tucker JA, Vuchinich RE. Self-report methods. In: Lattal KA, Perone M, editors. Handbook of methods for the experimental analysis of human behavior. New York: Plenum; 1998. pp. 435–470. [Google Scholar]
- Crowely TJ, MacDonald MJ, Zerbe GO, Petty TL. Reinforcing breath carbon monoxide reductions in chronic obstructive pulmonary disease. Drug and Alcohol Dependence. 1991;29:47–62. doi: 10.1016/0376-8716(91)90021-p. [DOI] [PubMed] [Google Scholar]
- Crowley-Koch B, Van Houten R. Automated measurement in applied behavior analysis: a review. Behavioral Interventions. 2013;28(3):225–240. [Google Scholar]
- Dallery J, Raiff BR. Contingency management in the 21st century: technological innovations to promote smoking cessation. Substance Use & Misuse. 2011;46(1):10–22. doi: 10.3109/10826084.2011.521067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dallery, J, & Raiff, B. R. (2014). Optimizing behavioral health interventions with single-case designs: from development to dissemination. Translational Behavioral Medicine. doi: 10.1007/s13142-014-0258-z [DOI] [PMC free article] [PubMed]
- Dallery J, Glenn IM, Raiff BR. An internet-based abstinence reinforcement treatment for cigarette smoking. Drug and Alcohol Dependence. 2007;86(2–3):230–238. doi: 10.1016/j.drugalcdep.2006.06.013. [DOI] [PubMed] [Google Scholar]
- Dallery J, Meredith S, Glenn IM. A deposit contract method to deliver abstinence reinforcement for cigarette smoking. Journal of Applied Behavior Analysis. 2008;41(4):609–615. doi: 10.1901/jaba.2008.41-609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dallery J, Meredith SM, Budney A. Contingency management in the substance abuse treatment clinic. In: Walters ST, Rotgers F, editors. Treating substance abuse. 3. New York: Guilford; 2012. [Google Scholar]
- Dallery, J., Cassidy, R. N., & Raiff, B. R. (2013). Single-case experimental designs to evaluate novel technology-based health interventions. Journal of Medical Internet Research, 15(2). doi:10.2196/jmir.2227. [DOI] [PMC free article] [PubMed]
- Dallery J, Raiff BR, Grabinski M. Internet-based contingency management to promote smoking cessation: a randomized, controlled study. Journal of Applied Behavior Analysis. 2013;46:750–764. doi: 10.1002/jaba.89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dallery J, Kurti A, Martner S. Technological methods to assess and treat cigarette smoking. In: Marsch L, Lord S, Dallery J, editors. Behavioral health care and technology: using science-based innovations to transform practice. Oxford: Oxford University Press; 2014. [Google Scholar]
- Dallery J, Riley WT, Nahum-Shani I. Research designs to develop and evaluate technology-based health behavior interventions. In: Marsch L, Lord S, Dallery J, editors. Behavioral health care and technology: using science-based innovations to transform practice. Oxford: Oxford University Press; 2014. [Google Scholar]
- Davies CA, Spence JC, Vandelanotte C, Caperchione CM, Mummery WK. Meta-analysis of internet-delivered interventions to increase physical activity levels. International Journal of Behavioral Nutrition and Physical Activity. 2012;9:52. doi: 10.1186/1479-5868-9-52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeFulio A, Donlin WD, Wong CJ, Silverman K. Employment-based abstinence reinforcement as a maintenance intervention for the treatment of cocaine dependence: a randomized controlled trial. Addiction. 2009;104(9):1530–1538. doi: 10.1111/j.1360-0443.2009.02657.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeMaio J, Schwartz L, Cooley P, Tice A. The application of telemedicine technology to a directly observed therapy program for tuberculosis: a pilot project. Clinical Infectious Diseases. 2001;33(12):2082–2084. doi: 10.1086/324506. [DOI] [PubMed] [Google Scholar]
- Denhaerynck, K., Schäfer-Keller, P., Young, J., Steiger, J., Bock, A., & De Geest, S. (2008). Examining assumptions regarding valid electronic monitoring of medication therapy: development of a validation framework and its application on a European sample of kidney transplant patients. BMC Medical Research Methodology, 8, doi:10.1186/1471-2288-8-5 [DOI] [PMC free article] [PubMed]
- Donlin Washington W, Knealing TW, Needham M, Wong CJ, Silverman K. Attendance rates in a workplace predict subsequent outcome of employment-based reinforcement of cocaine abstinence in methadone patients. Journal of Applied Behavior Analysis. 2008;41(4):499–516. doi: 10.1901/jaba.2008.41-499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Donlin Washington W, Banna KM, Gibson AL. Preliminary efficacy of prize-based contingency management to increase activity levels in healthy adults. Journal of Applied Behavior Analysis. 2014;47:231–245. doi: 10.1002/jaba.119. [DOI] [PubMed] [Google Scholar]
- Dougher MJ, Hackbert L. Establishing operations, cognition, and emotion. The Behavior Analyst. 2000;23(1):11–24. doi: 10.1007/BF03391996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duan N, Kravitz RL, Schmid CH. Single-patient (n-of-1) trials: a pragmatic clinical decision methodology for patient-centered comparative effectiveness research. Journal of Clinical Epidemiology. 2013;66(8 Suppl):S21–S28. doi: 10.1016/j.jclinepi.2013.04.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ducharme JM, Worling DE. Behavioral momentum and stimulus fading in the acquisition and maintenance of child compliance in the home. Journal of Applied Behavior Analysis. 1994;27(4):639–647. doi: 10.1901/jaba.1994.27-639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Erb P, Meredith SE, Raiff BR, Dallery J. The accuracy of a lower-cost breath carbon monoxide meter in distinguishing smokers from nonsmokers. Journal of Smoking Cessation. 2014 [Google Scholar]
- Ertin, E., Stohs, N., Kumar, S., Raij, A., al’Absi, M., & Shah, S. (2011). AutoSense: unobtrusively wearable sensor suite for inferencing of onset, causality, and consequences of stress in the field. Proceedings of 9th ACM Conference on Embedded Networked Sensing Systems, 274–287.
- Forbes EE, Stepp SD, Dahl RE, Ryan ND, Whalen D, Axelson DA, Silk JS. Real-world affect and social context as predictors of treatment response in child and adolescent depression and anxiety: an ecological momentary assessment study. Journal of Child and Adolescent Psychopharmacology. 2012;22(1):37–47. doi: 10.1089/cap.2011.0085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foreman KF, Stockl KM, Le LB, Fisk E, Shah SM, Lew HC, Curtis BS. Impact of a text messaging pilot program on patient medication adherence. Clinical Therapeutics. 2012;34(5):1084–1091. doi: 10.1016/j.clinthera.2012.04.007. [DOI] [PubMed] [Google Scholar]
- Foster SL, Masch EJ. Assessing social validity in clinical treatment research: issues and procedures. Journal of Consulting and Clinical Psychology. 1999;67:308–319. doi: 10.1037//0022-006x.67.3.308. [DOI] [PubMed] [Google Scholar]
- Fridlund Dunton, G., Liao, Y., Kawabata, K., Intille, S. (2012). Momentary assessment of adults’ physical activity and sedentary behavior: feasibility and validity. Frontiers in Psychology, 3, doi: 10.3389/fpsyg.2012.00260. [DOI] [PMC free article] [PubMed]
- Friman PC. Come on in, the water is fine: achieving mainstream relevance through integration with primary medical care. The Behavior Analyst. 2010;33:19–36. doi: 10.1007/BF03392201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gambelunghe C, Rossi R, Aroni K, Bacci M, Lazzarini A, De Giovanni N, Fucci N. Sweat testing to monitor drug exposure. Annals of Clinical & Laboratory Science. 2013;43(1):22–30. [PubMed] [Google Scholar]
- Gibbons MC, Fleisher L, Slamon RE, Bass S, Kandadai V, Beck JR. Exploring the potential of web 2.0 to address health disparities. Journal of Health Communication. 2011;16(Suppl 1):77–89. doi: 10.1080/10810730.2011.596916. [DOI] [PubMed] [Google Scholar]
- Glenn SS, Ellis J, Greenspoon J. On the revolutionary nature of the operant as a unit of behavioral selection. American Psychologist. 1992;47(11):1329–1336. [Google Scholar]
- Granger BB, Bosworth HB. Medication adherence: emerging use of technology. Current Opinion in Cardiology. 2011;26(4):279–287. doi: 10.1097/HCO.0b013e328347c150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gullov AL, Koefoed BG, Petersen P, Pedersen TS, Andersen ED, Godtfredsen J, Boysen G. Fixed minidose warfarin and aspirin alone and in combination vs adjusted-dose warfarin for stroke prevention in atrial fibrillation: second Copenhagen atrial fibrillation, aspirin, and anticoagulation study. Archives of Internal Medicine. 1998;158(14):1513. doi: 10.1001/archinte.158.14.1513. [DOI] [PubMed] [Google Scholar]
- Gustafson DH, McTavish FM, Chih MY, Atwood AK, Johnson RA, Boyle MG, Shah D. A smartphone application to support recovery from alcoholism: a randomized clinical trial. Journal of the American Medical Association Psychiatry. 2014;71(5):566–572. doi: 10.1001/jamapsychiatry.2013.4642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hackenberg TD. Token reinforcement: a review and analysis. Journal of the Experimental Analysis of Behavior. 2009;91(2):257–286. doi: 10.1901/jeab.2009.91-257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haedt-Matt AA, Keel PK. Revisiting the affect regulation model of binge eating: a meta-analysis of studies using ecological momentary assessment. Psychological Bulletin. 2011;137(4):660–681. doi: 10.1037/a0023660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hall SM, Humfleet GL, Munoz RF, Reus VI, Prochaska JJ, Robbins JA. Using extended cognitive behavioral treatment and medication to treat dependent smokers. American Journal of Public Health. 2011;101(12):2349–2356. doi: 10.2105/AJPH.2010.300084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hand, D. J., Heil, S. H., Sigmon, S. C., & Higgins. S. T. (2014). Improving medicaid health incentives programs: Lessons from substance abuse treatment research. Preventive Medicine, 63, 87–89. [DOI] [PMC free article] [PubMed]
- Hanley GP. Functional assessment of problem behavior: dispelling myths, overcoming implementation obstacles, and developing new lore. Behavior Analysis in Practice. 2012;5(1):54–72. doi: 10.1007/BF03391818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hanley GP, Iwata BA, McCord BE. Functional analysis of problem behavior: a review. Journal of Applied Behavior Analysis. 2003;36(2):147–185. doi: 10.1901/jaba.2003.36-147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayes SC, Brownstein AJ, Zettle RD, Rosenfarb I. Rule-governed behavior and sensitivity to changing consequences of responding. Journal of the Experimental Analysis of Behavior. 1986;45(3):237–256. doi: 10.1901/jeab.1986.45-237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heron KE, Smyth JM. Ecological momentary interventions: incorporating mobile technology into psychosocial and health behaviour treatments. British Journal of Health Psychology. 2010;15(1):1–39. doi: 10.1348/135910709X466063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hertzberg JS, Carpenter VL, Kirby AC, Calhoun PS, Moore SD, Dennis MF, Beckham JC. Mobile contingency management as an adjunctive smoking cessation treatment for smokers with posttraumatic stress disorder. Nicotine & Tobacco Research. 2013;15:1934–1938. doi: 10.1093/ntr/ntt060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heyman GM. Addiction: a disorder of choice. Cambridge: Harvard University Press; 2009. [Google Scholar]
- Higgins ST, Budney AJ, Bickel WK, Foerg FE, Donham R, Badger GJ. Incentives improve outcome in outpatient behavioral treatment of cocaine dependence. Archives of General Psychiatry. 1994;51(7):568–576. doi: 10.1001/archpsyc.1994.03950070060011. [DOI] [PubMed] [Google Scholar]
- Higgins ST, Silverman K, Heil SH. Contingency management in substance abuse treatment. New York: Guilford; 2008. [Google Scholar]
- Hineline PN. The origins of environment-based psychological theory. Journal of the Experimental Analysis of Behavior. 1990;53(2):305–320. doi: 10.1901/jeab.1990.53-305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoffman JA, Cunningham JR, Suleh AJ, Sundsmo A, Dekker D, Vago F, Hunt-Glassman J. Mobile direct observation treatment for tuberculosis patients: a technical feasibility pilot using mobile phones in Nairobi, Kenya. American Journal of Preventive Medicine. 2010;39(1):78–80. doi: 10.1016/j.amepre.2010.02.018. [DOI] [PubMed] [Google Scholar]
- Hunt GM, Azrin NH. A community-reinforcement approach to alcoholism. Behaviour Research and Therapy. 1973;11(1):91–104. doi: 10.1016/0005-7967(73)90072-7. [DOI] [PubMed] [Google Scholar]
- Hustyi KM, Normand MP, Larson TA, Morley AJ. The effect of outdoor activity context on physical activity in preschool children. Journal of Applied Behavior Analysis. 2012;45:401–405. doi: 10.1901/jaba.2012.45-401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hyers TM, Agnelli G, Hull RD, Morris TA, Samama M, Tapson V, Weg JG. Antithrombotic therapy for venous thromboembolic disease. Chest. 2001;119(1):176S–193S. doi: 10.1378/chest.119.1_suppl.176s. [DOI] [PubMed] [Google Scholar]
- Iguchi MY, Belding MA, Morral AR, Lamb RJ, Husband SD. Reinforcing operants other than abstinence in drug abuse treatment: an effective alternative for reducing drug use. Journal of Consulting and Clinical Psychology. 1997;65:421–428. doi: 10.1037//0022-006x.65.3.421. [DOI] [PubMed] [Google Scholar]
- International Telecommunications Union. (2011). Retrieved from http://www.itu.int/en/ITU-D/Statistics/Pages/stat/default.aspx, 11/11/13.
- Intille, S. S., Albinali, F., Mota, S., Kuris, B., Botana, P., & Haskell, W. L. (2011). Design of a wearable physical activity monitoring system using mobile phones and accelerometers. Conference Proceedings: Annual International Conference of the IEEE Engineering in Medicine and Biology Society, 3,636–3,639. [DOI] [PMC free article] [PubMed]
- Iwata BA, Dorsey MF, Slifer KJ, Bauman KE, Richman GS. Toward a functional analysis of self-injury. Journal of Applied Behavior Analysis. 1994;27(2):197–209. doi: 10.1901/jaba.1994.27-197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Javors MA, Hatch JP, Lamb RJ. Cut-off levels for breath carbon monoxide as a marker for cigarette smoking. Addiction. 2005;100:159–167. doi: 10.1111/j.1360-0443.2004.00957.x. [DOI] [PubMed] [Google Scholar]
- Kamps A, Roorda R, Brand P. Peak flow diaries in childhood asthma are unreliable. Thorax. 2001;56(3):180–182. doi: 10.1136/thorax.56.3.180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kanning, M.K., Ebner-Priemer, U. W., & Schlicht, W. M. (2013). How to investigate within-subject associations between physical activity and momentary affective states in everyday life: a position statement based on a literature overview. Frontiers in Psychology, 29. doi: 10.3389/fpsyg.2013.00187. [DOI] [PMC free article] [PubMed]
- Kaplan RM, Stone AA. Bringing the laboratory and clinic to the community: mobile technologies for health promotion and disease prevention. Annual Review of Psychology. 2013;64:471–498. doi: 10.1146/annurev-psych-113011-143736. [DOI] [PubMed] [Google Scholar]
- Kazdin AE. The meanings and measurement of clinical significance. Journal of Consulting and Clinical Psychology. 1999;67:332–339. doi: 10.1037//0022-006x.67.3.332. [DOI] [PubMed] [Google Scholar]
- Kerr J, Duncan S, Schipperijn J. Using global positioning systems in health research: a practical approach to data collection and processing. American Journal of Preventive Medicine. 2011;41(5):532–540. doi: 10.1016/j.amepre.2011.07.017. [DOI] [PubMed] [Google Scholar]
- Kidorf M, Stitzer ML. Contingent access to clinic privileges reduces drug abuse in methadone maintenance patients. In: Silverman K, editor. Motivating behavior change among illicit-drug abusers: research on contingency management interventions. Washington: American Psychological Association; 1999. pp. 221–241. [Google Scholar]
- Kimmel SE, Chen Z, Price M, Parker CS, Metlay JP, Christie JD, Gross R. The influence of patient adherence on anticoagulation control with warfarin: results from the International Normalized Ratio Adherence and Genetics (IN-RANGE) study. Archives of Internal Medicine. 2007;167(3):229. doi: 10.1001/archinte.167.3.229. [DOI] [PubMed] [Google Scholar]
- King, A. C., Hekler, E. B., Grieco, L. A., Winter, S. J., Sheats, J. L., Buman, M. P., Cirimele, J. (2013). Harnessing different motivational frames via mobile phones to promote daily physical activity and reduce sedentary behavior in aging adults. PloS One, 8(4), doi: 10.1371/journal.pone.0062613. [DOI] [PMC free article] [PubMed]
- Krummenacher I, Cavassini M, Bugnon O, Schneider MP. An interdisciplinary HIV-adherence program combining motivational interviewing and electronic antiretroviral drug monitoring. AIDS Care. 2011;23(5):550–561. doi: 10.1080/09540121.2010.525613. [DOI] [PubMed] [Google Scholar]
- Kumar S, Nilsen W, Pavel M, Srivastava M. Mobile health: revolutionizing healthcare through transdisciplinary research. Computer. 2013;46(1):28–35. [Google Scholar]
- Kumar S, Nilsen WJ, Abernethy A, Atienza A, Patrick K, Pavel M, Swendeman D. Mobile health technology evaluation: the mHealth evidence workshop. American Journal of Preventive Medicine. 2013;45(2):228–236. doi: 10.1016/j.amepre.2013.03.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kurti, A. N., & Dallery, J. (2013). Internet‐based contingency management increases walking in sedentary adults. Journal of Applied Behavior Analysis. [DOI] [PubMed]
- Lamb RJ, Kirby KC, Morral AR, Galbicka G, Iguchi MY. Improving contingency management programs for addiction. Addictive Behaviors. 2004;29:507–523. doi: 10.1016/j.addbeh.2003.08.021. [DOI] [PubMed] [Google Scholar]
- Lane, N. D., Mohammod, M., Lin, M., Yang, X., Lu, H., Ali, S., Campbell, A. (2011). BeWell: a smartphone application to monitor, model and promote wellbeing. Paper presented at the 5th International Conference on Pervasive Computing Technologies for Healthcare.
- Laraway S, Snycerski S, Michael J, Poling A. Motivating operations and terms to describe them: some further refinements. Journal of Applied Behavior Analysis. 2003;36(3):407–414. doi: 10.1901/jaba.2003.36-407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Larson, E. C., Goel, M., Boriello, G., Heltshe, S., Rosenfeld, M., & Patel, S. N. (2012). SpiroSmart: using a microphone to measure lung function on a mobile phone. Paper presented at the Proceedings of the 2012 ACM Conference on Ubiquitous Computing, 280–289.
- Larson TA, Normand MP, Morley AJ, Miller BG. A functional analysis of moderate-to-vigorous physical activity in young children. Journal of Applied Behavior Analysis. 2013;46:199–207. doi: 10.1002/jaba.8. [DOI] [PubMed] [Google Scholar]
- Lee M, Lee H, Kang S, Yang J, Ahn H, Rhee M, Kim S. Variables influencing antidepressant medication adherence for treating outpatients with depressive disorders. Journal of Affective Disorders. 2010;123(1):216–221. doi: 10.1016/j.jad.2009.10.002. [DOI] [PubMed] [Google Scholar]
- Lee WG, Kim YG, Chung BG, Demirci U, Khademhosseini A. Nano/microfluidics for diagnosis of infectious diseases in developing countries. Advanced Drug Delivery Reviews. 2010;62(4–5):449–457. doi: 10.1016/j.addr.2009.11.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leffingwell TR, Cooney NJ, Murphy JG, Luczak S, Rosen G, Dougherty DM, Barnett NP. Continuous objective monitoring of alcohol use: twenty‐first century measurement using transdermal sensors. Alcoholism: Clinical and Experimental Research. 2013;37(1):16–22. doi: 10.1111/j.1530-0277.2012.01869.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Legorreta, A. P., Christian-Herman, J., O'Connor, R. D., Hasan, M. M., Evans, R., & Leung, K. (1998). Compliance with national asthma management guidelines and specialty care: A health maintenance organization experience. Archives of Internal Medicine, 158(5), 457. [DOI] [PubMed]
- Li X, Ballerini DR, Shen W. A perspective on paper-based microfluidics: current status and future trends. Biomicrofluidics. 2012;6:011301. doi: 10.1063/1.3687398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lillie EO, Patay B, Diamant J, Issell B, Topol EJ, Schork NJ. The n-of-1 clinical trial: the ultimate strategy for individualizing medicine? Personalized Medicine. 2011;8(2):161–173. doi: 10.2217/pme.11.7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lotfizadeh AD, Edwards TL, Redner R, Poling A. Motivating operations affect stimulus control: a largely overlooked phenomenon in discrimination learning. The Behavior Analyst. 2012;35(1):89–100. doi: 10.1007/BF03392268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mace FC, Lalli JS, Shea MC, Lalli EP, West BJ, Roberts M, Nevin JA. The momentum of human behavior in a natural setting. Journal of the Experimental Analysis of Behavior. 1990;54(3):163–172. doi: 10.1901/jeab.1990.54-163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Madison K, Schmidt H, Volpp KG. Smoking, obesity, health insurance, and health incentives in the affordable care act. Journal of the American Medical Association. 2013;310(2):143–144. doi: 10.1001/jama.2013.7617. [DOI] [PubMed] [Google Scholar]
- Makeyev O, Lopez-Meyer P, Schuckers S, Besio W, Sazonov E. Automatic food intake detection based on swallowing sounds. Biomedical Signal Processing and Control. 2012;7(6):649–656. doi: 10.1016/j.bspc.2012.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marhe R, Waters AJ, van de Wetering BJ, Franken IH. Implicit and explicit drug-related cognitions during detoxification treatment are associated with drug relapse: an ecological momentary assessment study. Journal of Consulting and Clinical Psychology. 2013;81(1):1–12. doi: 10.1037/a0030754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marsch LA, Bickel WK. The efficacy of computer-based HIV/AIDS education for injection drug users. American Journal of Health Behavior. 2004;28:316–27. doi: 10.5993/ajhb.28.4.3. [DOI] [PubMed] [Google Scholar]
- Marsch LA, Dallery J. Advances in the psychosocial treatment of addiction: the role of technology in the delivery of evidence-based psychosocial treatment. Psychiatric Clinics of North America. 2012;35(2):481–493. doi: 10.1016/j.psc.2012.03.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marsch LA, Guarino H, Acosta M, Aponte-Melendez Y, Cleland C, Grabinski M, Edwards JJ. Web-based behavioral treatment for substance use disorders as a partial replacement of standard methadone maintenance treatment. Journal of Substance Abuse and Treatment. 2014;46(1):43–51. doi: 10.1016/j.jsat.2013.08.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martens, B. K., Gertza, L. E., Werdera, C. S., Rymanowskia, J. L., & Shankarb, K. H. (2014). Measures of association in contingency space analysis. Journal of Mathematical Psychology.
- McClernon FJ, Roy Choudhury R. I am your smartphone and I know you are about to smoke: the application of mobile sensing and computing approaches to smoking research and treatment. Nicotine & Tobacco Research. 2013;5(10):1651–1654. doi: 10.1093/ntr/ntt054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McComas JJ, Vollmer TR, Kennedy C. Descriptive analysis: quantification and examination of behavior-environment interactions. Journal of Applied Behavior Analysis. 2009;42:411–412. doi: 10.1901/jaba.2009.42-411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McDonell MG, Howell DN, McPherson S, Cameron JM, Srebnik D, Roll JM, Ries RK. Voucher-based reinforcement for alcohol abstinence using the ethyl-glucuronide alcohol biomarker. Journal of Applied Behavior Analysis. 2012;45(1):161–165. doi: 10.1901/jaba.2012.45-161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meredith SE, Grabinski MJ, Dallery J. Internet-based group contingency management to promote abstinence from cigarette smoking: a feasibility study. Drug and Alcohol Dependence. 2011;118(1):23–30. doi: 10.1016/j.drugalcdep.2011.02.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meredith SE, Robinson A, Erb P, Spieler C, Klugman N, Dutta P, Dallery J. A mobile-phone-based breath carbon monoxide meter to detect cigarette smoking. Nicotine and Tobacco Research. 2013;16:766–773. doi: 10.1093/ntr/ntt275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meredith SE, Jarvis BP, Raiff BR, Rojewski A, Kurti A, Cassidy RN, Dallery J. The ABCs of incentive-based treatment in health care: a behavior analytic framework to inform research and practice. Psychology Research and Behavior Management. 2014;2014(7):103–114. doi: 10.2147/PRBM.S59792. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michael J. Implications and refinements of the establishing operation concept. Journal of Applied Behavior Analysis. 2000;33(4):401–410. doi: 10.1901/jaba.2000.33-401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mitchell, J. T., Dennis, M. F., English, J. S., Dennis, P. A., Brightwood, A., Beckham, J. C., Kollins, S. H. (2014). Ecological momentary assessment of antecedents and consequences of smoking in adults with attention-deficit/hyperactivity disorder. Substance Use and Misuse. [DOI] [PMC free article] [PubMed]
- Morey TE, Booth M, Wasdo S, Wishin J, Quinn B, Gonzalez D, Melker RJ. Oral adherence monitoring using a breath test to supplement highly active antiretroviral therapy. AIDS and Behavior. 2013;17(1):298–306. doi: 10.1007/s10461-012-0318-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morford ZH, Witts BN, Killingsworth KJ, Alavosius MP. Gamification: the intersection between behavior analysis and game design technologies. The Behavior Analyst. 2014;37:25–40. doi: 10.1007/s40614-014-0006-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mulvaney SA, Rothman RL, Dietrich MS, Wallston KA, Grove E, Elasy TA, Johnson KB. Using mobile phones to measure adolescent diabetes adherence. Health Psychology. 2012;31(1):43–50. doi: 10.1037/a0025543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nevin J. The momentum of compliance. Journal of Applied Behavior Analysis. 1996;29(4):535–547. doi: 10.1901/jaba.1996.29-535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Normand MP, Kohn CS. Don’t wag the dog: extending the reach of applied behavior analysis. The Behavior Analyst. 2013;36:109–122. doi: 10.1007/BF03392294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oldenmenger WH, Echteld MA, de Wit R, Sillevis Smitt PA, Stronks DL, Stoter G, van der Rijt CC. Analgesic adherence measurement in cancer patients: comparison between electronic monitoring and diary. Journal of Pain and Symptom Management. 2007;34(6):639–647. doi: 10.1016/j.jpainsymman.2007.01.015. [DOI] [PubMed] [Google Scholar]
- Olmstead TA, Sindelar JL, Petry NM. Clinic variation in the cost-effectiveness of contingency management. The American Journal on Addictions/American Academy of Psychiatrists in Alcoholism and Addictions. 2007;16(6):457–460. doi: 10.1080/10550490701643062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olmstead TA, Sindelar JL, Petry NM. Cost-effectiveness of prize-based incentives for stimulant abusers in outpatient psychosocial treatment programs. Drug and Alcohol Dependence. 2007;87(2–3):175–182. doi: 10.1016/j.drugalcdep.2006.08.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Palmer DC. The role of atomic repertoires in complex behavior. The Behavior Analyst. 2012;35(1):59–73. doi: 10.1007/BF03392266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perrine MW, Mundt JC, Searles JS, Lester LS. Validation of daily self-reported alcohol consumption using interactive voice response (IVR) technology. Journal of Studies on Alcohol. 1995;56(5):487–490. doi: 10.15288/jsa.1995.56.487. [DOI] [PubMed] [Google Scholar]
- Petry NM. Contingency management treatments: controversies and challenges. Addiction. 2010;105(9):1507–1509. doi: 10.1111/j.1360-0443.2009.02879.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petry NM, Simcic F., Jr Recent advances in the dissemination of contingency management techniques: clinical and research perspectives. Journal of Substance Abuse Treatment. 2002;23(2):81–86. doi: 10.1016/s0740-5472(02)00251-9. [DOI] [PubMed] [Google Scholar]
- Piasecki TM, McCarthy DE, Fiore MC, Baker TB. Alcohol consumption, smoking urge, and the reinforcing effects of cigarettes: an ecological study. Psychology of Addictive Behaviors. 2008;22:230–239. doi: 10.1037/0893-164X.22.2.230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piasecki TM, Jahng S, Wood PK, Robertson BM, Epler AJ, Cronk NJ, Sher KJ. The subjective effects of alcohol-tobacco co-use: an ecological momentary assessment investigation. Journal of Abnormal Psychology. 2011;120:557–571. doi: 10.1037/a0023033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Plarre, K., Raij, A., Hossain, S. M., Ali, A. A., Nakajima, M., al’Absi, M., Scott, M. (2011). Continuous inference of psychological stress from sensory measurements collected in the natural environment. Paper presented at the Information Processing in Sensor Networks (IPSN), 2011 10th International Conference, 97–108.
- Plasqui G, Bonomi AG, Westerterp KR. Daily physical activity assessment with accelerometers: new insights and validation studies. Obesity Reviews. 2013;14(6):451–462. doi: 10.1111/obr.12021. [DOI] [PubMed] [Google Scholar]
- Raiff BR, Dallery J. The generality of nicotine as a reinforcer-enhancer in rats: effects on responding maintained by primary and conditioned reinforcers and resistance to extinction. Psychopharmacology. 2008;201:305–14. doi: 10.1007/s00213-008-1282-9. [DOI] [PubMed] [Google Scholar]
- Raiff BR, Dallery J. Internet-based contingency management to improve adherence with blood glucose testing recommendations for teens with type 1 diabetes. Journal of Applied Behavior Analysis. 2010;43(3):487–491. doi: 10.1901/jaba.2010.43-487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raiff BR, Jarvis BP, Rapoza D. Prevalence of video game use, cigarette smoking, and acceptability of a video game-based smoking cessation intervention among online adults. Nicotine & Tobacco Research. 2012;14(12):1453–1457. doi: 10.1093/ntr/nts079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raiff BR, Jarvis BP, Turturici M, Dallery D. Acceptability of an Internet-based contingency management intervention for smoking cessation: the views of smokers, nonsmokers, and healthcare professionals. Experimental and Clinical Psychopharmacology. 2013;21:204–13. doi: 10.1037/a0032451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rand CS, Stitzer ML, Bigelow GE, Mead AM. The effects of contingent payment and frequent workplace monitoring on smoking abstinence. Addictive Behaviors. 1989;14:121–128. doi: 10.1016/0306-4603(89)90041-5. [DOI] [PubMed] [Google Scholar]
- Remington G, Teo C, Mann S, Hahn M, Foussias G, Agid O. Examining levels of antipsychotic adherence to better understand nonadherence. Journal of Clinical Psychopharmacology. 2013;33(2):261–263. doi: 10.1097/JCP.0b013e31828568bc. [DOI] [PubMed] [Google Scholar]
- Reynolds B, Dallery J, Shroff P, Patak M, Leraas K. A web-based contingency management program with adolescent smokers. Journal of Applied Behavior Analysis. 2008;41(4):597–601. doi: 10.1901/jaba.2008.41-597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Riekert KA, Rand CS. Electronic monitoring of medication adherence: when is high-tech best? Journal of Clinical Psychology in Medical Settings. 2002;9(1):25–32. [Google Scholar]
- Rigsby MO, Rosen MI, Beauvais JE, Cramer JA, Rainey PM, O’Malley SS, Rounsaville BJ. Cue-dose training with monetary reinforcement: pilot study of an antiretroviral adherence intervention. Journal of General Internal Medicine. 2000;15(12):841–847. doi: 10.1046/j.1525-1497.2000.00127.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Riley WT, Rivera DE, Atienza AA, Nilsen W, Allison SM, Mermelstein R. Health behavior models in the age of mobile interventions: are our theories up to the task? Translational Behavioral Medicine. 2011;1(1):53–71. doi: 10.1007/s13142-011-0021-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robles E, Silverman K, Preston KL, Cone EJ, Katz E, Bigelow GE, Stitzer ML. The brief abstinence test: voucher-based reinforcement of cocaine abstinence. Drug and Alcohol Dependence. 2000;58(1–2):205–212. doi: 10.1016/s0376-8716(99)00090-3. [DOI] [PubMed] [Google Scholar]
- Rosales‐Ruiz J, Baer DM. Behavioral cusps: a developmental and pragmatic concept for behavior analysis. Journal of Applied Behavior Analysis. 1997;30(3):533–544. doi: 10.1901/jaba.1997.30-533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosen MI, Dieckhaus K, McMahon TJ, Valdes B, Petry NM, Cramer J, Rounsaville B. Improved adherence with contingency management. AIDS Patient Care and STDs. 2007;21(1):30–40. doi: 10.1089/apc.2006.0028. [DOI] [PubMed] [Google Scholar]
- Rothney MP, Schaefer EV, Neumann MM, Choi L, Chen KY. Validity of physical activity intensity predictions by ActiGraph, Actical, and RT3 accelerometers. Obesity. 2008;16:1946–1952. doi: 10.1038/oby.2008.279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schlinger HD. Separating discriminative and function-altering effects of verbal stimuli. The Behavior Analyst. 1993;16:9–23. doi: 10.1007/BF03392605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schroeder SA. Shattuck lecture. We can do better—improving the health of the American people. The New England Journal of Medicine. 2007;357(12):1221–1228. doi: 10.1056/NEJMsa073350. [DOI] [PubMed] [Google Scholar]
- Shiffman S. Ecological momentary assessment (EMA) in studies of substance use. Psychological Assessment. 2009;21(4):486. doi: 10.1037/a0017074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiffman S. How many cigarettes did you smoke? Assessing cigarette consumption by global report, time-line follow-back, and ecological momentary assessment. Health Psychology. 2009;28:519–526. doi: 10.1037/a0015197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiffman, S. (2014). Conceptualizing analyses of ecological momentary assessment data. Nicotine and Tobacco Research, 16(Suppl 2), S76–S87. [DOI] [PMC free article] [PubMed]
- Shiffman S, Kirchner TR. Cigarette-by-cigarette satisfaction during ad libitum smoking. Journal of Abnormal Psychology. 2009;118:348–359. doi: 10.1037/a0015620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiffman S, Stone AA, Hufford MR. Ecological momentary assessment. Annual Review of Clinical Psychology. 2008;4:1–32. doi: 10.1146/annurev.clinpsy.3.022806.091415. [DOI] [PubMed] [Google Scholar]
- Silverman K. Exploring the limits and utility of operant conditioning in the treatment of drug addiction. The Behavior Analyst. 2004;27(2):209–230. doi: 10.1007/BF03393181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Silverman K, Chutuape MA, Bigelow GE, Stitzer ML. Voucher-based reinforcement of attendance by unemployed methadone patients in a job skills training program. Drug and Alcohol Dependence. 1996;41(3):197–207. doi: 10.1016/0376-8716(96)01252-5. [DOI] [PubMed] [Google Scholar]
- Silverman K, Higgins ST, Brooner RK, Montoya ID, Cone EJ, Schuster CR, Preston KL. Sustained cocaine abstinence in methadone maintenance patients through voucher-based reinforcement therapy. Archives of General Psychiatry. 1996;53(5):409–415. doi: 10.1001/archpsyc.1996.01830050045007. [DOI] [PubMed] [Google Scholar]
- Silverman K, Wong CJ, Higgins ST, Brooner RK, Montoya ID, Contoreggi C, Preston KL. Increasing opiate abstinence through voucher-based reinforcement therapy. Drug and Alcohol Dependence. 1996;41(2):157–165. doi: 10.1016/0376-8716(96)01246-x. [DOI] [PubMed] [Google Scholar]
- Silverman K, Wong CJ, Grabinski MJ, Hampton J, Sylvest CE, Dillon EM, Wentland RD. A web-based therapeutic workplace for the treatment of drug addiction and chronic unemployment. Behavior Modification. 2005;29(2):417–463. doi: 10.1177/0145445504272600. [DOI] [PubMed] [Google Scholar]
- Silverman K, Wong CJ, Needham M, Diemer KN, Knealing T, Crone-Todd D, Kolodner K. A randomized trial of employment-based reinforcement of cocaine abstinence in injection drug users. Journal of Applied Behavior Analysis. 2007;40(3):387–410. doi: 10.1901/jaba.2007.40-387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Silverstein J, Klingensmith G, Copeland K, Plotnick L, Kaufman F, Laffel L, Holzmeister LA. Care of children and adolescents with type 1 diabetes: a statement of the American Diabetes Association. Diabetes Care. 2005;28(1):186–212. doi: 10.2337/diacare.28.1.186. [DOI] [PubMed] [Google Scholar]
- Sindelar J, Elbel B, Petry NM. What do we get for our money? Cost-effectiveness of adding contingency management. Addiction. 2007;102(2):309–316. doi: 10.1111/j.1360-0443.2006.01689.x. [DOI] [PubMed] [Google Scholar]
- Skinner BF. Science and human behavior. Oxford: Macmillan; 1953. [Google Scholar]
- Sokolovsky AW, Mermelstein RJ, Hedeker D. Factors predicting compliance to ecological momentary assessment among adolescent smokers. Nicotine and Tobacco Research. 2012;16:351–358. doi: 10.1093/ntr/ntt154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sorensen JL, Haug NA, Delucchi KL, Gruber V, Kletter E, Batki SL, Hall S. Voucher reinforcement improves medication adherence in HIV-positive methadone patients: a randomized trial. Drug and Alcohol Dependence. 2007;88(1):54–63. doi: 10.1016/j.drugalcdep.2006.09.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spring B, Schneider K, McFadden HG, Vaughn J, Kozak AT, Smith M, Hedeker D. Multiple behavior changes in diet and activity: a randomized controlled trial using mobile technology. Archives of Internal Medicine. 2012;172(10):789–796. doi: 10.1001/archinternmed.2012.1044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stitzer ML, Bigelow GE, Liebson IA, Hawthorne JW. Contingent reinforcement for benzodiazepine-free urines: evaluation of a drug abuse treatment intervention. Journal of Applied Behavior Analysis. 1982;15(4):493–503. doi: 10.1901/jaba.1982.15-493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stokes, T. F., & Baer, D. M. (1977). An implicit technology of generalization. Journal of Applied Behavior Analysis, 10, 349–367. [DOI] [PMC free article] [PubMed]
- Stoops WW, Dallery J, Fields NM, Nuzzo PA, Schoenberg NE, Martin CA, Wong CJ. An internet-based abstinence reinforcement smoking cessation intervention in rural smokers. Drug and Alcohol Dependence. 2009;105(1–2):56–62. doi: 10.1016/j.drugalcdep.2009.06.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sun F, Kuo C, Cheng H, Buthpitiya S, Collins P, Griss M. Activity-aware mental stress detection using physiological sensors. Mobile computing, applications, and services. 2012;76:211–230. [Google Scholar]
- Sundberg ML. Thirty points about motivation from Skinner’s book verbal behavior. Analysis of Verbal Behavior. 2013;29:13–40. doi: 10.1007/bf03393120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swift R. Direct measurement of alcohol and its metabolites. Addiction. 2003;98(s2):73–80. doi: 10.1046/j.1359-6357.2003.00605.x. [DOI] [PubMed] [Google Scholar]
- Tang J, Mandrusiak A, Russell T. The feasibility and validity of a remote pulse oximetry system for pulmonary rehabilitation: a pilot study. International Journal of Telemedicine and Applications. 2012;2012:11. doi: 10.1155/2012/798791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tapper K. Motivating operations in appetite research. Appetite. 2005;45:95–107. doi: 10.1016/j.appet.2005.05.002. [DOI] [PubMed] [Google Scholar]
- Thompson T. Relations among functional systems in behavior analysis. Journal of the Experimental Analysis of Behavior. 2007;87(3):423–440. doi: 10.1901/jeab.2007.21-06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thompson RH, Borrero JC. Direct observation. In: Fisher WW, Piazza CC, Roane HS, editors. Handbook of applied behavior analysis. New York: Guilford; 2011. pp. 191–205. [Google Scholar]
- Todd M, Armeli S, Tennen H. Interpersonal problems and negative mood as predictors of within-day time to drinking. Psychology of Addictive Behaviors. 2009;23(2):205. doi: 10.1037/a0014792. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tomlinson M, Rotheram-Borus MJ, Swartz L, Tsai AC. Scaling up mHealth: where is the evidence? PLoS Medicine. 2013;10(2) doi: 10.1371/journal.pmed.1001382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Topol, E. J. (2012). The creative destruction of medicine how the digital revolution will create better health care. New York: Basic Books.
- Twyman JS. Emerging technologies and behavioral cusps: a new era for behaviour analysis? European Journal of Behavior Analysis. 2011;12:461–482. [Google Scholar]
- Valdovinos MG, Kennedy CH. A behavior-analytic conceptualization of the side effects of psychotropic medication. The Behavior Analyst. 2004;27:231–238. doi: 10.1007/BF03393182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van Camp CM, Hayes LB. Assessing and increasing physical activity. Journal of Applied Behavior Analysis. 2012;45(4):871. doi: 10.1901/jaba.2012.45-871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Onzenoort HA, Neef C, Verberk WW, van Iperen HP, de Leeuw PW, van der Kuy PH. Determining the feasibility of objective adherence measurement with blister packaging smart technology. American Journal of Health-System Pharmacy: AJHP: Official Journal of the American Society of Health-System Pharmacists. 2012;69(10):872–879. doi: 10.2146/ajhp100592. [DOI] [PubMed] [Google Scholar]
- Volpp, K. G., Loewenstein, G., Troxel, A. B., Doshi, J., Price, M., Laskin, M., & Kimmel, S. E. (2008). A test of financial incentives to improve warfarin adherence. BMC Health Services Research, 8(1), 272. [DOI] [PMC free article] [PubMed]
- Wade, V. A., Karnon, J., Eliott, J. A., & Hiller, J. E. (2012). Home videophones improve direct observation in tuberculosis treatment: a mixed methods evaluation. PloS One, 7(11). doi:10.1371/journal.pone.0050155. [DOI] [PMC free article] [PubMed]
- Weiser, M. (1994). The computer for the 21st century. Scientific American, September, 94-104.
- Williams AB, Amico KR, Bova C, Womack JA. A proposal for quality standards for measuring medication adherence in research. AIDS and Behavior. 2013;17(1):284–97. doi: 10.1007/s10461-012-0172-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wise J, Operario D. Use of electronic reminder devices to improve adherence to antiretroviral therapy: a systematic review. AIDS Patient Care and STDs. 2008;22(6):495–504. doi: 10.1089/apc.2007.0180. [DOI] [PubMed] [Google Scholar]
- Zeller A, Schroeder K, Peters TJ. Electronic pillboxes (MEMS) to assess the relationship between medication adherence and blood pressure control in primary care. Scandinavian Journal of Primary Health Care. 2007;25(4):202–207. doi: 10.1080/02813430701651954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zickuhr, K., & Smith, A. (2012). Digital differences. Washington: Pew Charitable Trust. Retrieved from http://www.pewinternet.org/2012/04/13/digital-differences/.
- Zullig LL, Shaw RJ, Bosworth HB. Applying technology to medication management and adherence. In: Marsch L, Lord S, Dallery J, editors. Behavioral health care and technology: using science-based innovations to transform practice. Oxford: Oxford University Press; 2014. [Google Scholar]