

Abstract
Topical Steroid Damaged/Dependent face (TSDF) is a phenomenon which has been described very recently (2008). It is characterized by a plethora of symptoms caused by an usually unsupervised misuse/abuse/overuse of topical corticosteroid of any potency on the face over an unspecified and/or prolonged period of time. This misuse and damage have a serious effect on the quality of life of the patients in general and the skin of the face in particular. Management is difficult and necessitates psychological counseling as well as physical soothing of the sensitive skin.
Keywords: Face, misuse, steroid dependence, topical steroid, TSDF
What was known?
Topical corticosteroids were introduced in 1952 and since then have been used extensively in various inflammatory disorders.
Physical side-effects and addiction to topical corticosteroids may occur due to overuse and misuse of the drug.
Introduction
Since the introduction of the first topical corticosteroid (TC) in 1952, a number of steroid molecules with potencies varying from super-potent to least potent have been introduced making the task of treating inflammatory dermatological disorders easier for the dermatologists. TCs hold the pride of place in every dermatologist's armory. However, the drug has been misused to varying extents by the pharmaceuticals and pharmacies, by the prescribers (who are not always dermatologists or doctors), and by the users. All this misuse results in severe cutaneous damage characterized by erythema, monomorphic acne, steroid atrophy, steroid rosacea, telangiectasia, perioral dermatitis, striae, and severe addiction to the TC. The face is the most common and most severely affected site of such misuse and steroid dependence resulting in a phenomenon which has been labeled as “Topical steroid-damaged/dependent face (TSDF).”[1]
Definition
TSDF is defined as the semi-permanent or permanent damage to the skin of the face precipitated by the irrational, indiscriminate, unsupervised, or prolonged use of TCs resulting in a plethora of cutaneous signs and symptoms and psychological dependence on the drug.
Historical Perspective
Sulzberger and Witten in 1952 introduced compound F (hydrocortisone), the first TC to the world of dermatology.[2] This discovery revolutionized the treatment of dermatological disorders, particularly inflammatory diseases.[3] The first report of side effects of TCs was published in 1963.[4] Further reports kept trickling in until Burry in 1973 and Kligman in 1976 published the earliest reports of addiction to TCs.[5,6] Kligman and Frosch in 1979 defined the parameters of dependence on the drug and coined the term “steroid addiction.”[7] Further reports of TC addiction on the face were published in subsequent decades under various names such as dermatitis rosaceiformis steroidica,[8] red skin syndrome[9] and steroid-induced rosacea-like dermatitis.[10] TC misuse on face was first reported from India in 2006.[11] Later that year, a proposal named “Stop OTC supply of potent topical steroids” was submitted by us (Lahiri and Coondoo) to the General Body of the Indian Association of Dermatologists, Venereologists, and Leprologists (IADVL), which unanimously passed the proposal at Chennai in January 2007. After observing the alarming rise in the number of cases of TC misuse on face resulting in steroid dependence, the entity was labeled as “Topical steroid-dependent/damaged face” by one of us (Lahiri) in March 2008.[1] Later that year, under the aegis of IADVL, a pan-Indian multi-centric study on TSDF was conducted in 12 centers and the report was presented at an independent scientific session at the national conference of IADVL (DERMACON) at Bengaluru in January 2009. The report was subsequently published in 2011.[12]
Vulnerability of the Facial Skin
The facial skin is thinner than the skin of most other parts of the body. This results in increased percutaneous absorption of drugs. The sebaceous glands on the face are larger than elsewhere, and there is an increased tendency to sweating particularly in hot and humid climates as is prevalent in most parts of India. Hence, it is more liable to the ill-effects of environmental factors such as sunlight and pollution, friction due to cleaning and rubbing, and application of drugs and cosmetics. The face is also the most visible part of the human body making it vulnerable to the ill-effects of beauty consciousness, comments, and “medical advice” from an assortment of laymen throughout life and injudicious use of various substances and drugs such as cosmetics and drugs such as TC.[13]
Ethical Topical Corticosteroid Usage on Face
Judicious use of TC on face depends on a number of factors such as indication, potency of the drug, age of the patient and duration, amount and frequency of application.[14] TCs have an anti-inflammatory, anti-proliferative, immunosuppressive, anti-pruritic, atrophogenic, melanopenic, and sex-hormone-like effect on the skin, and hence are useful in hyperproliferative, inflammatory, and immunologic disorders.[12] The indications of TCs on the face are enumerated in Table 1. The potency of TCs has been determined by measuring their vasoconstrictive effect on the skin. Based on this assay, TCs are classified into seven classes (USA classification) from the super-potent to the least potent. It is important to realize that due to the thinness of the skin of the face, penetrability of TCs is increased considerably. Hence, one should only apply TCs of least potency on the skin of the face. TCs of lower potency are also used in patients who have thinner skin such as children.[15,16] TCs should not be used beyond a certain duration irrespective of the potency; it is advisable not to use TCs on the face beyond a period of 2 weeks.[12] Once-daily application along with proper amount based on fingertip unit is advised by most experts.[17] TCs are also available in combination with other drugs such as antifungals, antibiotics, retinoids, and hydroquinone. Such combinations should be used judiciously or better avoided on the thin skin of the face.[12]
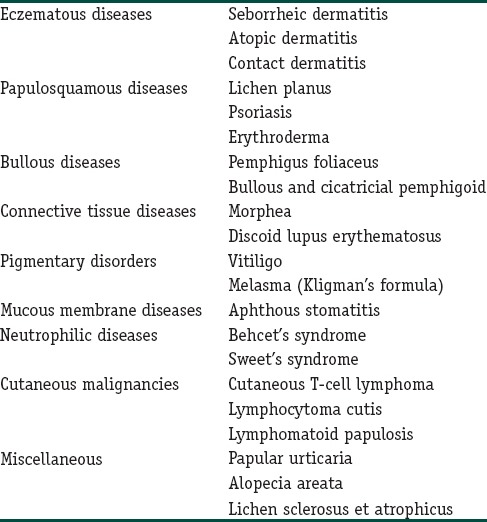
Table 1.
Indications of topical corticosteroids on face
Topical Steroid-Damaged/Dependent Face: Precipitating Factors
Misuse of TC on the face has gradually evolved over the years and has now reached phenomenal proportions due to a number of factors. In India, an apathetic bureaucracy is reluctant to realize the implications and side effects of TC.[18] Pharmaceutical companies market unethical products containing TCs to boost sales. A prime example is the so-called “modified Kligman's formula” containing mometasone. In their attempt to benefit financially, two, three, four, and five drug combinations are marketed unethically.[1] The salesmen of such pharmaceutical concerns solicit the patronage of non-dermatologists, alternative medicine practitioners, and quacks without informing them about the do's and don’ts of TC usage.[1] The prescribers, on the other hand, may not follow the norms of TC usage. Prescriptions of dermatologists may be improperly written with respect to the amount, frequency, and duration of the use of TC.[12] A principal source of misuse of TCs is the salesmen in the chemist shops. The problem in this arena is two fold. First, there is an increasing perception among laymen that such salesmen are equivalent to or even more knowledgeable about drugs than doctors. The salesmen, on the other hand, enjoy this unfounded glory and fame and do nothing to dispel the misconception, as their sales receive an unprecedented boost even without prescriptions. In their enthusiasm for profit, they sell any and every TCs for sundry problems on the face without any consideration for the norms of TC usage (about which they have no knowledge, in any case). The problem is further compounded by the fact that most TCs are available at nominal price as over-the-counter (OTC) products.[18] This results in a two-way economic benefit to the salesmen as well as to the patients who make a saving on the doctor's consultation charges.[1] Apart from these salesmen, patients also apply TCs on the recommendation of friends, neighbors, and relatives without consulting doctors at all. They apply TCs not only on nonsteroid-responsive dermatoses, but also on diseases such as dermatomycoses, which may be aggravated by the TC.[12] Finally, perhaps, the greatest (mis) users of TCs are laymen who are the victims of the wave of fairness craze sweeping across the land. TCs either singly or as components of the “modified Kligman's formula” are used rampantly as fairness creams.[19] This craze is fanned by a general impression particularly in the Indian society that “black is ugly” – a notion fanned by the promotion of fairness creams by a host of celebrities.[11] In its totality, the Indian scenario regarding the misuse of topical steroid on face is very dismal and disturbing.[20]
Pathogenesis
Addiction to TC has been reported to occur not only with short-term usage of more potent TCs, but also with long-term usage of milder TCs. The process of withdrawal and management of the withdrawal symptoms becomes more difficult and time-consuming with increasing potency of TC used. Withdrawal of TC results in the withdrawal of the vasoconstrictive effect of TC causing a fixed vasodilatation, which is responsible for the flare seen on rebound after withdrawal of the drug. Rapaport and Rapaport have postulated that due to repeated application of TC, action of nitrous oxide (NO) is inhibited resulting in chronic vasoconstriction.[9] When the TC is withdrawn, endothelial NO is released causing dilatation of blood vessels and consequent erythema. The erythema is further aggravated by TC-induced dermal atrophy with resultant lack of support to the vasculature.[21] It has also been postulated that TC-induced chronic immunosuppression results in the overgrowth of micro-organisms. These micro-organisms act as superantigens. When the TC is withdrawn, its immunosuppressive effect is also removed resulting in a superantigen-induced inflammatory reaction manifested clinically as inflammatory papules and pustules.[22]
Etiology
TSDF is a complex symptom of various side effects of TC applied on facial skin resulting in total dependence on the TC applied. TSDF is basically a form of drug dependence. Drug dependence has been defined as an adaptive state that develops from repeated drug administration, and which results in withdrawal upon cessation of drug use.[23] Addiction to TC is caused by chronic misuse and overuse of the drug. The patient becomes psychologically and physically dependent on the drug. Attempts to withdraw the drug result in rebound or flare of symptoms causing immense distress to the patient so that the patient resumes the usage of TC and refuses any further to withdraw the drug. The most common site of TC addiction is the face.[22] TC addiction occurs when it is used unsupervised for a prolonged period in the proper indication, but without prescription or is misused for the wrong indication (usually acne vulgaris), wrong potency (mid-or superpotent TC on face), wrong age group (children and geriatric patients), or at the wrong site. The patient usually gives a history of TC usage for a prolonged period.[12]
Clinical Features
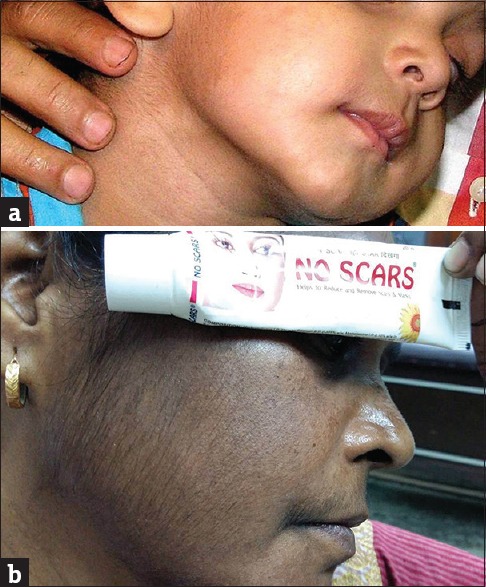
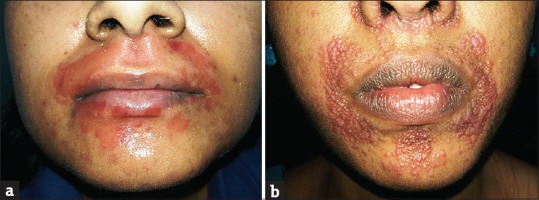
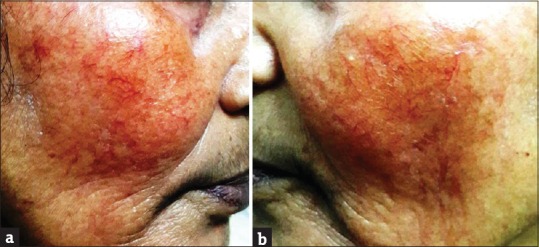
As described earlier, TSDF is caused by patients and laymen applying TCs of wrong potency on the face for the wrong indication and at the wrong age.[12] As the rash for which the TC has been initially applied becomes resistant to the drug, more potent TCs are applied sometimes with increased frequency to control the symptoms. As a result of TC misuse either on diseased skin (acne vulgaris etc.) or normal skin (misuse as fairness creams), the skin of the face develops erythematous papules, pustules, acneiform eruptions, dryness, perioral dermatitis, telangiectasia, rosacea-like features, hypopigmentation, hyperpigmentation, or allergic contact dermatitis [Table 2 and Figures 1–12].[24,25,26] Patients may also present with photosensitivity.[21] Withdrawal of the TC results in erythema (red face) for about 2 weeks followed by desquamation. If the patient does not use the TC again, the flare resolves, but reappears within 2 weeks. Further discontinuation results in a cycle of flare and resolution which continues for some time.[21] However, the flares occur with decreasing intensity and the duration of resolution become increasingly prolonged till the patient becomes completely cured.[9] The rebound phenomenon may sometimes occur in an area which is larger than the original site where TC has been misused or even at distant sites.[9] Some patients may also exhibit symptoms similar to status cosmeticus or chronic actinic dermatitis.[9] The principal clinical feature of TSDF, occurring both as a side effect of the misuse of TC as also due to withdrawal of the offending agent, is a diffuse erythema. Hence, erythema can be said to the hallmark of TSDF, a manifestation which was initially noted as red face syndrome.[9]
Table 2.
Clinical features of topical steroid-damaged/dependent face
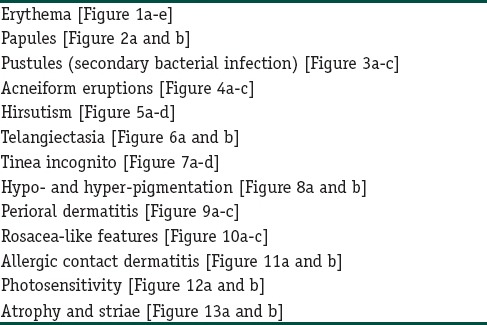
Figure 1.

(a-e) Erythema due to topical steroid abuse
Figure 12.

(a and b) Photosensitivity due to topical steroid abuse
Figure 2.

(a and b) Papules due to topical steroid abuse
Figure 3.
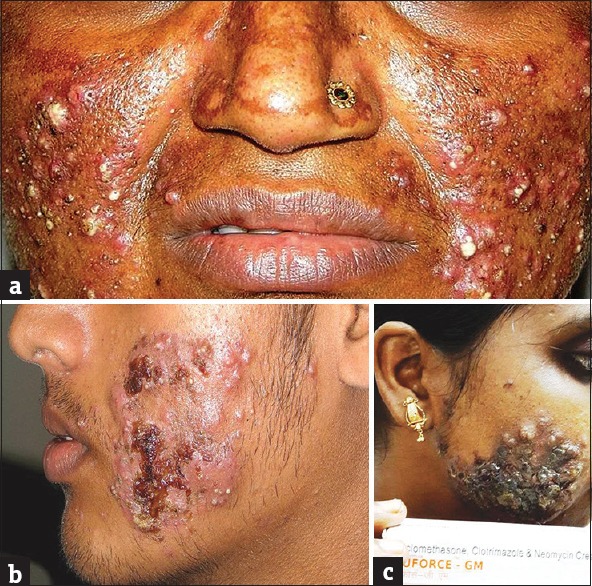
(a-c) Pustules (secondary bacterial infections) due to topical steroid abuse
Figure 4.

(a-c) Acneiform eruptions due to topical steroid abuse
Figure 5.
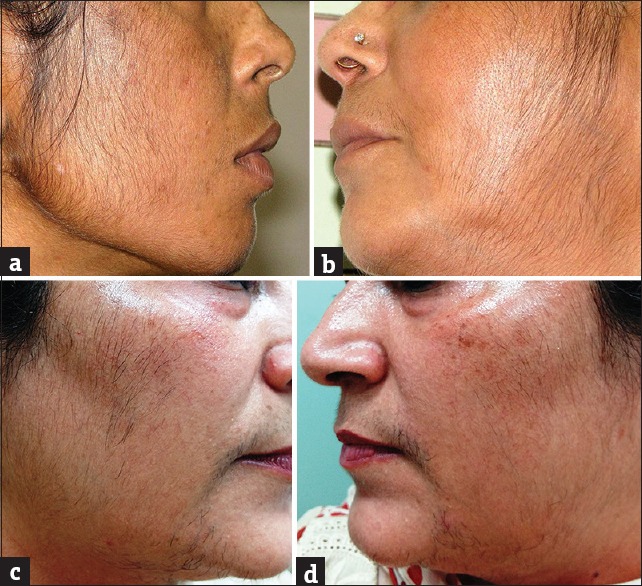
(a-d) Hirsutism due to topical steroid abuse
Figure 6.
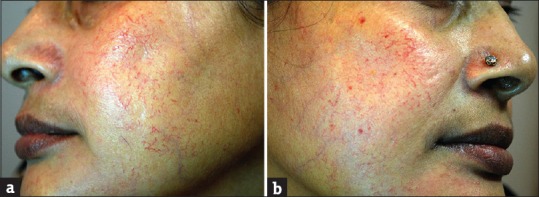
(a and b) Telangiectasia due to topical steroid abuse
Figure 7.

(a-d) Tinea incognito due to topical steroid abuse
Figure 8.
(a and b) Hypo- and hyper-pigmentation due to topical steroid abuse
Figure 9.

(a-c) Perioral dermatitis due to topical steroid abuse
Figure 10.

(a-c) Rosacea-like features due to topical steroid abuse
Figure 11.
(a and b) Allergic contact dermatitis due to topical steroid abuse
Figure 13.
(a and b) Atrophy and striae due to topical steroid abuse
Therapeutic Problems with Topical Corticosteroid
TCs of higher potency and TCs in ointment bases have an increased tendency to produce side effects particularly if used too frequently and inappropriately on sites with thinner stratum corneum such as the face.[7] Though these side effects are quite problematic, of more serious concern in India are the rapidly increasing phenomena of injudicious prescriptions, indiscriminate OTC sale of TCs, and use of steroids as beauty creams leading to steroid dependence and steroid phobia.[1]
Management of Topical Steroid-Damaged/Dependent Face
Management of TSDF is difficult and involves counseling as well as therapy for both the rebound phenomenon as well as reversal of damage caused by the TC. It is important to remember that the patient has to be provided a substantial amount of psychological support. He has to be counseled that he should use medications only as prescribed by dermatologists and other doctors and never on the advice of others. The TC must never be used beyond the prescription period. Cosmetics, soap, and emollients containing glycolic acid and lactic acid, etc., should not be used on the face during flares. The face must be washed with warm water only.[9] The patient must be advised about the ill-effects of the TC that has been used and that on stoppage of the TC, the disease for which the TC is being applied may worsen at first but improve later.[22] There is a controversy regarding the mode of withdrawal of TC – while some authorities advocate gradual withdrawal to minimize the symptoms of the rebound phenomenon,[8] others are in favor of sudden complete stoppage of TC use once the patient presents with TSDF to the physician.[9] Replacement therapy with calcineurin inhibitors has been advocated by some workers.[27,28] However, Rapaport and Rapaport reported burning sensation on application of the drug.[9] Pale sulfonated shale oil cream 4% which has both anti-inflammatory as well as antibacterial properties has been recommended as a safe alternative to TC in case of atopic eczema affecting the face.[29,30] Some other drugs such as doxycycline, minocycline, and metronidazole have also been tried to alleviate the symptoms of rebound phenomenon.[22] Oral antihistaminic has been recommended to control the pruritus associated with the rebound phenomenon.[21] The rebound phenomenon may also be associated with an intense burning sensation for which repeated ice compresses have been recommended. Bland emollients for the dryness and Burrow's solution for weepy lesions have also been used.[9] Oral antifungals have also been used to control the resulting demodex/pityrosporum folliculitis in most of the cases.
Profile of Topical Steroid-Damaged/Dependent Face Patients - Results of a Pan-Indian Study on Topical Steroid-Damaged/Dependent Face
A multicentric study on TSDF in which both the authors participated was conducted under the aegis of IADVL as a follow-up of the proposal of “Stop OTC supply of potent topical steroids” approved by IADVL General Body in 2007 (vide supra) The study was conducted in 12 centers all over India on 2926 cases of facial dermatoses, out of which 433 cases (14.33%) were found to be applying TC on the face. It was found to be used more by semi-literate, urban patients in their third decade of life. Fifty percent of patients were using a brand of betamethasone valerate followed by mometasone furoate (17.8%) and clobetasol propionate (12%). Combinations with antifungals, antibacterials, hydroquinone, retinoids, etc., were being used by 59.6% of the cases. Potent steroids (halobetasol propionate, clobetasol propionate, betamethasone dipropionate, beclomethasone dipropionate, and betamethasone valerate) were being used more in rural and sub-urban areas by patients who were in their second decade of life on the recommendation of nondermatologists (friend, peer, relative, pharmacist, or beautician). Of the remainder 55.7% were from dermatologists, 26.7% from MBBS doctors, 11.3% from other specialists, and 6.3% from practitioners of alternate medicine. TC usage was considered as inappropriate in 403 (93%) cases. An alarming finding was that the TCs were being used as fairness creams in 29% cases and as a skin-lightening agent in melasma and other hyperpigmentary disorders in a further 28.5% cases. Other diseases in which it was inappropriately used were acne vulgaris (24%), rosacea, tinea, facial dermatitides, and undiagnosed rashes (18.5%). Interestingly, 59.3% patients were using TC on the recommendation of nonphysician sources. There was a wide variation of duration of usage from 1 week to 30 years. Adverse effects were observed in as many as 90.2% cases. More than one lesion was seen in 32.6% cases. Acneiform lesions either arose de novo or occurred as aggravation due to misuse in acne vulgaris. Other significant adverse effects were telangiectasia, atrophy, hypopigmentation, perioral dermatitis, rosacea, tinea incognito, and hirsutism.[12]
Topical Steroid-Damaged/Dependent Face: The Financial Impact
As mentioned earlier, the use of TC in India is not restricted to dermatological disorders; it is mostly based on nonphysician, nondermatologists’ prescription, and this disturbing trend is growing alarmingly in recent years leading to situation which can only be compared to a silent and ugly epidemic of astronomical magnitude. The sale of TC accounts for 82% of sale of all topical drugs in India. The financial stakes can be easily gauged from the sales figures of TC in 2013 which stood at Rs. 1400 crores (approximately $233 million).[18] Hence, TCs have become the milking cow of the dermatological divisions of the Indian pharmaceutical industry, which naturally enjoy the fiscal benefits without consideration for the therapeutic and ethical aspect. This attitude is manifested by unethical two, three, four, and even five drug combinations of TC with antifungals, antibiotics, salicylic acid, and other molecules flooding the TC market. In fact, the top three selling TCs are triple, quadruple, and double combinations.[18] Unlimited OTC sale of drugs without proper regulatory control has complicated the situation. According to the pan-Indian multicentric study (vide supra), a staggering total of 73.3% of TCs were not prescribed by dermatologists, of which 59.3% are sold without any doctor's prescription.[8] In spite of a number of TCs appearing in the Schedule H of the Drugs and Cosmetics Control Act of the Government of India, OTC sales of these TC continue unabated.[30] Therefore, in financial terms, approximately, $138 million worth of TCs are sold in India annually OTC without prescription support and on the advice of laymen. It is obvious that the ultimate direct beneficiaries of this huge market are the pharmaceuticals to a large extent and the pharmacies to a smaller extent. The indirect beneficiaries are of course the governments at the state and central level as increased sales translate to increased commercial tax generation. Under these circumstances, the apathy of these agencies to the emerging disaster is, therefore, natural and compounds the complicated situation. However, the ultimate suffers are the patients many of whom, knowingly or unknowingly apply TCs for prolonged periods on diseased and nondiseased skin, with or without proper indications.[11,12]
Conclusion
TSDF is a common entity describing a phenomenon which has of late emerged as a major threat to the health of the facial skin of millions of Indians. Unauthorized, unsupervised, and uncontrolled use of steroids of varying potencies from the mild to the superpotent for prolonged periods for wrong indications and as fairness creams have resulted in an epidemic of rashes which resemble side effects of corticosteroids and TC addiction of the skin of the face. Cosmetic creams which are marketed as fairness creams per se may also produce TSDF-like features such as erythematous papules, acneiform eruptions, telangiectasia, rosacea-like features, pigmentary disturbances, and photosensitivity. Withdrawal of the offending agent is a psychological and physical challenge. This particular entity is now being reported with increased frequency in global literature.[31,32,33,34,35] Management of this epidemic on a war footing has now become an absolute necessity and would require a combined and concerted effort on the part of the government, health authorities, medical professionals, pharmaceutical companies, and chemists.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
What is new?
The phenomenon of “TSDF” which is an acronym for “Topical steroid damaged/dependent face” has been recently described
TSDF is a disease entity which encompasses a plethora of physical signs and symptoms as well as steroid addiction due to unsupervised overuse and misuse of the drug for an unspecified period of time
The drug is easily available in India over the counter and is often applied on the advice of people who are unaware of the ill-effects of such misuse
Withdrawal of the drug is a physical and psychological challenge.
References
- 1.Coondoo A. Topical corticosteroid misuse: The Indian scenario. Indian J Dermatol. 2014;59:451–5. doi: 10.4103/0019-5154.139870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sulzberger MB, Witten VH. The effect of topically applied compound F in selected dermatoses. J Invest Dermatol. 1952;19:101–2. doi: 10.1038/jid.1952.72. [DOI] [PubMed] [Google Scholar]
- 3.Rindani TH. Topical action of steroid hormones on inflammation. Arch Int Pharmacodyn Ther. 1954;99:467–73. [PubMed] [Google Scholar]
- 4.Epstein NN, Epstein WL, Epstein JH. Atrophic striae in patients with inguinal intertrigo. Arch Dermatol. 1963;87:450–7. [Google Scholar]
- 5.Burry JN. Topical drug addiction: Adverse effects of fluorinated corticosteroid creams and ointments. Med J Aust. 1973;1:393–6. doi: 10.5694/j.1326-5377.1973.tb118065.x. [DOI] [PubMed] [Google Scholar]
- 6.Kligman AM. Letter: Topical steroid addicts. JAMA. 1976;235:1550. doi: 10.1001/jama.235.15.1550b. [DOI] [PubMed] [Google Scholar]
- 7.Kligman AM, Frosch PJ. Steroid addiction. Int J Dermatol. 1979;18:23–31. doi: 10.1111/j.1365-4362.1979.tb01905.x. [DOI] [PubMed] [Google Scholar]
- 8.Basta-Juzbasic A, Subic JS, Ljubojevic S. Demodex folliculorum in development of dermatitis rosaceiformis steroidica and rosacea-related diseases. Clin Dermatol. 2002;20:135–40. doi: 10.1016/s0738-081x(01)00244-9. [DOI] [PubMed] [Google Scholar]
- 9.Rapaport MJ, Rapaport V. The Red Skin Syndromes: Corticosteroid addiction and withdrawal. Expert Rev Dermatol. 2006;1:547–61. [Google Scholar]
- 10.Rathi SK, Kumrah L. Topical corticosteroid-induced rosacea-like dermatitis: A clinical study of 110 cases. Indian J Dermatol Venereol Leprol. 2011;77:42–6. doi: 10.4103/0378-6323.74974. [DOI] [PubMed] [Google Scholar]
- 11.Rathi S. Abuse of topical steroid as cosmetic cream: A social background of steroid dermatitis. Indian J Dermatol. 2006;51:154–5. [Google Scholar]
- 12.Saraswat A, Lahiri K, Chatterjee M, Barua S, Coondoo A, Mittal A, et al. Topical corticosteroid abuse on the face: A prospective, multicenter study of dermatology outpatients. Indian J Dermatol Venereol Leprol. 2011;77:160–6. doi: 10.4103/0378-6323.77455. [DOI] [PubMed] [Google Scholar]
- 13.Ambika H, Sujatha VC, Yadalla H, et al. Topical corticosteroid abuse on face: A prospective study on outpatients of dermatology. Our Dermatol Online. 2014;5:5–8. [Google Scholar]
- 14.Rathi SK, D’Souza P. Rational and ethical use of topical corticosteroids based on safety and efficacy. Indian J Dermatol. 2012;57:251–9. doi: 10.4103/0019-5154.97655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Saraswat A. Topical corticosteroid use in children: Adverse effects and how to minimize them. Indian J Dermatol Venereol Leprol. 2010;76:225–8. doi: 10.4103/0378-6323.62959. [DOI] [PubMed] [Google Scholar]
- 16.Coondoo A, Chattopadhyay C. Use and abuse of topical corticosteroids in children. Indian J Paediatr Dermatol. 2014;15:1–4. [Google Scholar]
- 17.Saraswat A. Ethical use of topical corticosteroids. Indian J Dermatol. 2014;59:469–72. doi: 10.4103/0019-5154.139877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Verma SB. Sales, status, prescriptions and regulatory problems with topical steroids in India. Indian J Dermatol Venereol Leprol. 2014;80:201–3. doi: 10.4103/0378-6323.132246. [DOI] [PubMed] [Google Scholar]
- 19.Dey VK. Misuse of topical corticosteroids: A clinical study of adverse effects. Indian Dermatol Online J. 2014;5:436–40. doi: 10.4103/2229-5178.142486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Verma SB. Topical corticosteroid misuse in India is harmful and out of control. BMJ. 2015;351:h6079. doi: 10.1136/bmj.h6079. [DOI] [PubMed] [Google Scholar]
- 21.Fisher M. Steroid-induced rosacealike dermatitis: Case report and review of the literature. Cutis. 2009;83:198–204. [PubMed] [Google Scholar]
- 22.Ghosh A, Sengupta S, Coondoo A, Jana AK. Topical corticosteroid addiction and phobia. Indian J Dermatol. 2014;59:465–8. doi: 10.4103/0019-5154.139876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association; 2013. [Google Scholar]
- 24.Abraham A, Roga G. Topical steroid-damaged skin. Indian J Dermatol. 2014;59:456–9. doi: 10.4103/0019-5154.139872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Coondoo A, Phiske M, Verma S, Lahiri K. Side-effects of topical steroids: A long overdue revisit. Indian Dermatol Online J. 2014;5:416–25. doi: 10.4103/2229-5178.142483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Saraswat A. Contact allergy to topical corticosteroids and sunscreens. Indian J Dermatol Venereol Leprol. 2012;78:552–9. doi: 10.4103/0378-6323.100520. [DOI] [PubMed] [Google Scholar]
- 27.Goldman D. Tacrolimus ointment for the treatment of steroid-induced rosacea: A preliminary report. J Am Acad Dermatol. 2001;44:995–8. doi: 10.1067/mjd.2001.114739. [DOI] [PubMed] [Google Scholar]
- 28.Chu CY. An open-label pilot study to evaluate the safety and efficacy of topically applied pimecrolimus cream for the treatment of steroid-induced rosacea-like eruption. J Eur Acad Dermatol Venereol. 2007;21:484–90. doi: 10.1111/j.1468-3083.2006.01991.x. [DOI] [PubMed] [Google Scholar]
- 29.Warnecke J, Wendt A. Anti-inflammatory action of pale sulfonated shale oil (ICHTHYOL pale) in UVB erythema test. Inflamm Res. 1998;47:75–8. doi: 10.1007/s000110050282. [DOI] [PubMed] [Google Scholar]
- 30.Drugs and Cosmetics (2nd Amendment) Rules, 2006, Ministry of Health and Family Welfare (Department of Health) Notification. New Delhi: 2006. Mar 16th, [Last accessed on 2016 Apr 23]. Available from: http://cdsco.nic.in/writereaddata/Notoifi.pdf . [Google Scholar]
- 31.Korting HC, Schöllmann C, Cholcha W, Wolff L Collaborative Study Group. Efficacy and tolerability of pale sulfonated shale oil cream 4% in the treatment of mild to moderate atopic eczema in children: A multicentre, randomized vehicle-controlled trial. J Eur Acad Dermatol Venereol. 2010;24:1176–82. doi: 10.1111/j.1468-3083.2010.03616.x. [DOI] [PubMed] [Google Scholar]
- 32.Xiao X, Xie H, Jian D, Deng Y, Chen X, Li J, et al. Rebounding triad (severe itching, dryness and burning) after facial corticosteroid discontinuation defines a specific class of corticosteroid-dependent dermatitis. J Dermatol. 2015;42:697–702. doi: 10.1111/1346-8138.12877. [DOI] [PubMed] [Google Scholar]
- 33.Porter G, Grills N. Medication misuse in India: A major public health issue in India. J Public Health (Oxf) 2015 doi: 10.1093/pubmed/fdv072. pii: Fdv072. [DOI] [PubMed] [Google Scholar]
- 34.Hajar T, Leshem YA, Hanifin JM, Nedorost ST, Lio PA, Paller AS, et al. A systematic review of topical corticosteroid withdrawal (“steroid addiction”) in patients with atopic dermatitis and other dermatoses. J Am Acad Dermatol. 2015;72:541–9.e2. doi: 10.1016/j.jaad.2014.11.024. [DOI] [PubMed] [Google Scholar]
- 35.Hameed AF. Steroid dermatitis resembling rosacea: A clinical evaluation of 75 patients. ISRN Dermatol 2013. 2013 doi: 10.1155/2013/491376. 491376. [DOI] [PMC free article] [PubMed] [Google Scholar]