

Abstract
Background:
Ligamentous injury associated with isolated coronoid fracture had been sparingly reported. Concealed or unclear fractures and ligamentous or articular cartilage lesions are promptly acknowledged by magnetic resonance imaging (MRI) but cannot be entirely pictured in regular radiological assessments. In isolated coronoid fracture, the fragment size is very small and due to the complex anatomy surrounding the coronoid radiographic imaging may not be sufficient. The purpose of this study was to evaluate the incidence of combined osteochondral and ligamentous injuries by magnetic resonance imaging (MRI) in 24 patients with an isolated coronoid fracture.
Materials and Methods:
In a retrospective study conducted at tertiary hospital between 2009 and 2011, elbow radiographs (anteroposterior and lateral views), computed tomography scan images, and MRI in the sagittal, coronal, axial, oblique, and coronal oblique planes were collected and reviewed. Musculoskeletal radiologist with subspecialty training in musculoskeletal MR interpretation and a fellowship-trained shoulder and elbow surgeon evaluated the MRI.
Results:
The incidence of associated injuries revealed torn lateral collateral ligament (LCL) in all 24 patients (100%) while 15 patients (62.5%) had common extensor muscle tears. Seven of 24 elbows (29.2%) showed medial collateral ligament (MCL) tear, and 13 of 16 patients (81.3%) with anteromedial facet fracture had MCL attached to the fragment. Five of 24 (20.8%) cases had contusions on the radial head. On the distal humeral side, 15 patients had bone contusions on the posterior inferior of the trochlear on sagittal view. The ligament affections of the LCL were confirmed intraoperatively and repaired.
Conclusion:
LCL injury was consistent in all isolated coronoid fracture. The forces resulting in the injury appear similar to varus distraction forces acting in the knee leading to distraction injuries of the lateral structures of the knee joint. As concurrent osteochondral injuries and ligamentous injuries are not rare, magnetic resonance analysis serves as an excellent tool for analysis of the ligamentous injuries preoperatively and aids in surgical planning.
Keywords: Isolated coronoid fracture, lateral collateral ligament, magnetic resonance imaging
MeSh terms: MRI, fracture, ligaments, elbow
INTRODUCTION
The coronoid process has a critical role for the stability of elbow joint because it is a key bony constraint for the elbow stability during flexion and extension. Regan-Morrey classified coronoid fractures in three categories based on lateral X-ray of the elbow.1 Type 1 involves the tip of coronoid, type 2 involves <50% of the coronoid height, and type 3 involves more than 50% of the coronoid height.2,3 O’Driscoll et al., proposed a classification for coronoid fractures that highlighted the location and size of the fragment, including fractures of the anteromedial facet of the coronoid, based on computed tomography (CT) scan.2,4
The coronoid has multiple soft tissue insertions; the anterior part of the joint capsule, the medial collateral ligament (MCL) and the brachialis muscle. However, the severity of soft tissue injury that occurs with various types of the coronoid fractures has not been fully appreciated. Ligamentous injury associated with isolated coronoid fracture had been sparingly reported.5,7,8,9
Concealed or unclear fractures and ligamentous or articular cartilage lesions are promptly acknowledged by magnetic resonance imaging (MRI) but cannot be entirely pictured in regular radiological assessments.6 In isolated coronoid fracture, the fragment size is very small and due to the complex anatomy surrounding the coronoid radiographic imaging may not be sufficient.2
The purpose of this study was to identify the incidence of associated osteochondral and ligamentous injuries by MRI in patients admitted with isolated coronoid fractures and investigate the mechanism of these associated injuries. In terms of ligament repair could be advised to the patients.
MATERIALS AND METHODS
A retrospective study was undertaken on 24 consecutive patients admitted to a tertiary level trauma center with an acute isolated coronoid fracture identified on the initial anterior-posterior and lateral elbow radiographs.
Axial and longitudinal instability presenting with tenderness at the distal radioulnar joint was an exclusion criterion. In addition, patients with any other fractures around the elbow, such as olecranon, radial head, or capitellum fractures, were excluded. Elbow dislocations were excluded. Patients older than 65 years with the presence of osteoarthritis were excluded.
The initial radiologic evaluation of each elbow was done with standard anteroposterior and lateral radiographs and CT scans that identified the presence of an isolated coronoid fracture. The fracture was classified as per classification established Regan and Morrey1 using plain radiographs [Figure 1a], andO’Driscoll classification2 using the CT scan images [Figure 1b]. MRI evaluation was performed with the affected elbow in a splint in the position of ease in the sagittal, axial, coronal, axial, oblique and coronal oblique planes. MRIs were obtained from a GE Signa LX 1.5T (GE Healthcare Milwaukee, WI, USA). Imaging was done with a 5-inch surface coil. Inversion recovery was used to estimate the bruising in bones. Ligament integrity was verified by the use of gradient echo imaging, whereas fractures were best assessed by the use of T1-images and inversion recovery. Joint alignment was also assessed by the use of T1-images. Adequate MRI images were obtained [Table 1]. The MRI were done once only. Musculoskeletal radiologist with subspecialty training in musculoskeletal MR interpretation and a fellowship-trained shoulder and elbow surgeon then evaluated the MRIs. The observers were blinded regarding patients identity.
Figure 1.
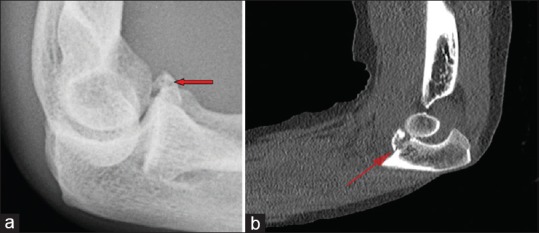
(a) Plain radiograph lateral view of elbow joint showing isolated coronoid fracture. (b) Sagittal computed tomography scan showing the isolated coronoid fracture
Table 1.
Clinical details of the patients
Statistical analysis
To test accuracy, reliability, and repeatability, the original and repeat readings of MRIs were made by 2 independent observers. Intra- and inter-observer reliability in identifying the integrity of the lateral collateral ligament (LCL) was assessed for 5 randomly chosen MRIs from 3 trials with results quantified by the use of a scale ranging from 0 to 5 (0, intact, 5, complete rupture).7 One observer made 3 separate readings of the defined structure, and a second observer made a single measurement to provide assessment of interobserver variation.6
The F-test was performed to test the homogeneity of the variance for interobserver reliability. The coefficient of variance was measured for intra observer reliability.
RESULTS
The patient population consisted of 18 men and 6 women. The average age of the patients was 37 years (range 12–65 years).
The participants did not present with elbow instability at first clinical encounter. The significant clinical observation was pain. On plain radiographs, the Regan-Morrey type 1 fracture was found in 7 patients, type 2 in 14 patients, and type 3 was found in 3 patients.
Based on CT scan, we found that 6 patients had O’Driscoll type 1,16 patients had O’Driscoll type 2 (subtype 1 [n = 3], subtype 2 [n = 9], and subtype 3 [n = 4]). Two patients had O’Driscoll type 3 coronoid fractures.
Of 24 isolated coronoid fractures in this series, regardless of the type of fracture, LCL tear was shown by MRI in all cases (100%) [Figure 2]. Fifteen patients (62.5%) had common extensor muscle tears (four complete tears and 11 partial articular side tears) and one patient had an avulsion fracture of the lateral epicondyle where the common extensor and LCL complex are attached.
Figure 2.
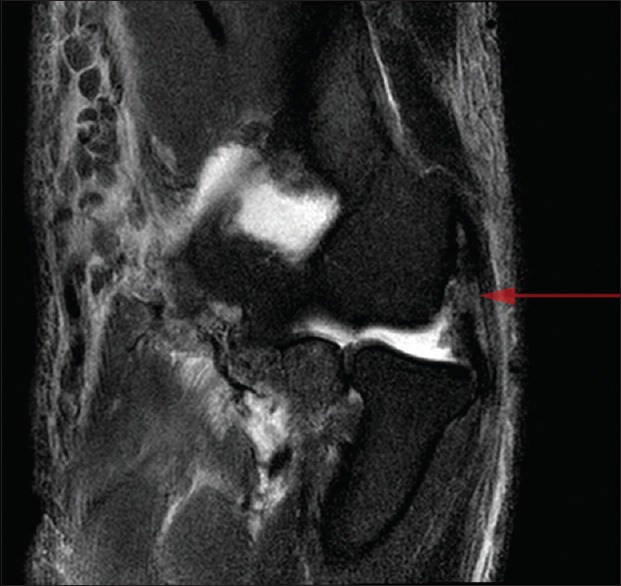
Coronal T2-weighted short tau inversion recovery magnetic resonance imaging showing increased radiocapitelllar distance and ruptured lateral collateral ligament
We found less frequency of medial soft tissue injuries. Seven of the 24 elbows (29.2%) showed MCL tear on MRI, of which two were O’Driscoll type 3, three were type 2 and two were type 1. One case with a type 3 Regan-Morrey and O’Driscoll coronoid fracture also has common flexor origin tear. Thirteen of 16 patients (81.3%) with anteromedial facet fracture had MCL attached to the fracture fragment.
In the plain radiographs and CT scan, we confirmed that none of our patients sustained radial head fractures. MRI evaluation showed that five of the 24 (20.8%) cases had bone contusions on the radial head and all were on the anterolateral side. Two of these cases occurred in type 2 coronoid fracture, one in type 3 and one in type 1.
On the distal humeral side, bone contusion was observed mainly on the trochlear side (66.7%). Only two of the 16 cases had distal humerus bone contusion on the capitellum side, and both also had radial head bone bruises. Fifteen patients had trochlear side bone contusions, which were all on the posterior inferior side on sagittal view.
Anteromedial facet coronoid fractures were found in 14 patients, of which only one patient had a tip fracture.
All of the patients who had LCL lesions on MRI had opening of joint on preoperative fluoroscopic examination (24/24 [100%]). Lateral side opening on clinical examination was not always possible to be documented because of pain and restricted range of motion immediately after the fracture. Elbow examination under GA showed some amount of instability. The coefficient of variation was less than 5% for intraobserver reliability. The F test between the 2 observers was not statistically significant for each MRI set.
DISCUSSION
The degree of ligamentous injury that occurs with an isolated coronoid fracture was not fully appreciated in the literature. Elbow arthrography has been sometimes used to demonstrate capsular or ligamentous disruptions with various types of radial head fractures.1,9
MRI scanning can identify ligamentous or articular cartilage lesions that are not usually identified during radiologic evaluations.6 MRI provides useful information in the evaluation of the LCL and MCL of the elbow.10,11,12 Most radiology anatomy reference texts image the elbow in extension and supination.6,11,12 However, most injured elbows are splinted or casted and subsequently imaged in 90° of flexion with the forearm in the neutral position, making the identification of the collateral ligaments challenging.
If the fracture is complex, the treatment plan is based on the associated injury. In this study, seemingly uncomplicated isolated coronoid fractures were found to have a high incidence of LCL tear, which is an important stabilize for posterolateral rotatory instability of the elbow joint.13,14
Detailed MR analysis can provide some information regarding the mechanism of the injury. According to the observation of the study, we can concur that isolated coronoid fractures may occur due to an axial load or severe varus stress, causing lateral tension and subsequent concurrent rupture or partial tear of the LCL. This suggested pathomechanics is illustrated in Figure 3.
Figure 3.
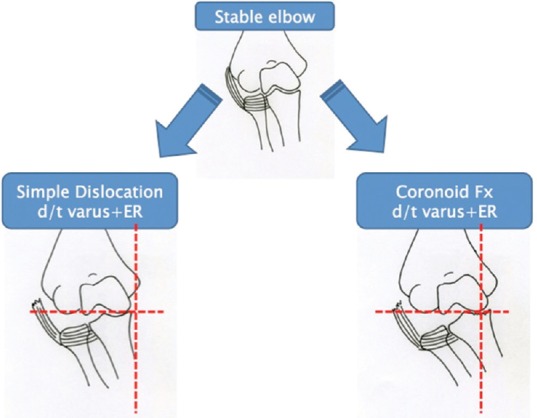
Suggested mechanism of isolated coronoid fracture is varus external rotation with posterior directed force. The hinge point is placed at medial coronoid facet when the fracture occurs
Our results showed that isolated coronoid fractures that were advised to be treated conservatively often have associated ligamentous and/or osteochondral injuries that may have significant implications on prognosis and appropriate treatment protocols are needed to be designed.14 We strongly recommend a detailed clinical and radiographic examination in every case of isolated coronoid fracture. Careful examination under fluoroscopy should be performed and may be helpful in determining the presence of associated ligamentous injuries. MRI should be reserved for those cases that present any type of pathology after the initial radiologic and fluoroscopic evaluation. A high level of suspicion should be used when one is treating these type of fractures, because osteochondral, and/or ligamentous injuries are present. These associated injuries may have important treatment implications such as recurrent subluxation and instability. Being retrospective in nature, the study has some inherent limitations. As to date, the quantification of the elbow instability remains elusive. When to decide whether the instability is significant enough to operate requires long term followup and a randomized control trial with patients with only the LCL injury treated conservatively and surgically. The amount of instability due to the LCL injury can be further investigated in a biomechanical setup in the presence and absences of coronoid fracture.
Financial support and sponsorship
This work was supported by the Global Frontier R and D Program on <Human-centered Interaction for Coexistence> funded by the National Research Foundation of Korea grant funded by the Korean Government (MSIP) (NRF-M1AXA003-2010-0029748).
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Regan W, Morrey B. Fractures of the coronoid process of the ulna. J Bone Joint Surg Am. 1989;71:1348–54. [PubMed] [Google Scholar]
- 2.O’Driscoll SW, Jupiter JB, Cohen MS, Ring D, McKee MD. Difficult elbow fractures: Pearls and pitfalls. Instr Course Lect. 2003;52:113–34. [PubMed] [Google Scholar]
- 3.Steinmann SP. Coronoid process fracture. J Am Acad Orthop Surg. 2008;16:519–29. [PubMed] [Google Scholar]
- 4.Fitzpatrick MJ, Diltz M, McGarry MH, Lee TQ. A new fracture model for “terrible triad” injuries of the elbow: Influence of forearm rotation on injury patterns. J Orthop Trauma. 2012;26:591–6. doi: 10.1097/BOT.0b013e31824135af. [DOI] [PubMed] [Google Scholar]
- 5.Mirowitz SA, London SL. Ulnar collateral ligament injury in baseball pitchers: MR imaging evaluation. Radiology. 1992;185:573–6. doi: 10.1148/radiology.185.2.1410375. [DOI] [PubMed] [Google Scholar]
- 6.Itamura J, Roidis N, Mirzayan R, Vaishnav S, Learch T, Shean C. Radial head fractures: MRI evaluation of associated injuries. J Shoulder Elbow Surg. 2005;14:421–4. doi: 10.1016/j.jse.2004.11.003. [DOI] [PubMed] [Google Scholar]
- 7.Carrino JA, Morrison WB, Zou KH, Steffen RT, Snearly WN, Murray PM. Lateral ulnar collateral ligament of the elbow: Optimization of evaluation with two-dimensional MR imaging. Radiology. 2001;218:118–25. doi: 10.1148/radiology.218.1.r01ja52118. [DOI] [PubMed] [Google Scholar]
- 8.Gómez Navalón LA, ZorrillaRibot P, Salido Valle JA. Isolated fracture of the coronoid process. Acta Orthop Belg. 2005;71:615–7. [PubMed] [Google Scholar]
- 9.Davidson PA, Moseley JB, Jr, Tullos HS. Radial head fracture. A potentially complex injury. Clin Orthop Relat Res. 1993;297:224–30. [PubMed] [Google Scholar]
- 10.Hill NB, Jr, Bucchieri JS, Shon F, Miller TT, Rosenwasser MP. Magnetic resonance imaging of injury to the medial collateral ligament of the elbow: A cadaver model. J Shoulder Elbow Surg. 2000;9:418–22. doi: 10.1067/mse.2000.107392. [DOI] [PubMed] [Google Scholar]
- 11.Kaplan LJ, Potter HG. MR imaging of ligament injuries to the elbow. RadiolClin North Am. 2006;44:583–94. doi: 10.1016/j.rcl.2006.04.007. ix. [DOI] [PubMed] [Google Scholar]
- 12.O’Driscoll SW, Morrey BF, Korinek S, An KN. Elbow subluxation and dislocation. A spectrum of instability. Clin Orthop Relat Res. 1992;280:186–97. [PubMed] [Google Scholar]
- 13.Potter HG, Weiland AJ, Schatz JA, Paletta GA, Hotchkiss RN. Posterolateral rotatory instability of the elbow: Usefulness of MR imaging in diagnosis. Radiology. 1997;204:185–9. doi: 10.1148/radiology.204.1.9205244. [DOI] [PubMed] [Google Scholar]
- 14.Pollock JW, Pichora J, Brownhill J, Ferreira LM, McDonald CP, Johnson JA, et al. The influence of type II coronoid fractures, collateral ligament injuries, and surgical repair on the kinematics and stability of the elbow: An in vitro biomechanical study. J Shoulder Elbow Surg. 2009;18:408–17. doi: 10.1016/j.jse.2009.01.009. [DOI] [PubMed] [Google Scholar]