

Description
A 32-year-old man presented to our emergency department, with pain, swelling and a dorsal curvature in his penis. He had severe pain and lost tumescence with a snapping sound during vigorous sexual intercourse. On examination, he had a swelling with ecchymosis on the ventral aspect of his penis causing an acute dorsal angulation (figure 1). There was no blood at the meatus/haematuria. Taking the typical history and examination findings into account, the diagnosis of penile fracture was made. Ultrasound showed a focal tear in the medial wall of the right corpora cavernosa with haematoma tracking ventrally and displacing the corpora spongiosa to the other side (figures 2 and 3).
Figure 1.

Penis showing dorsal penile angulation with a ventral swelling and ecchymoses of the shaft, called ‘eggplant deformity’.
Figure 2.

Ultrasound images showing a focal tear (arrow) in the medial wall of right corpora cavernosa (CC) with haematoma (H) tracking ventrally.
Figure 3.
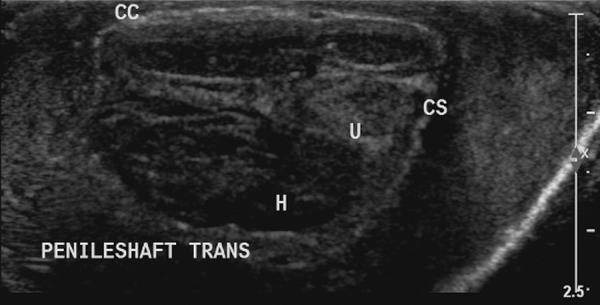
Ultrasound images showing ventral haematoma (H) displacing the corpus spongiosum (CS), and central urethra (U) displaced towards the left with the corpora cavernosa (CC) seen dorsally.
The patient was taken for emergent haematoma evacuation and corporal repair.
Penile fracture occurs when an erect penis undergoes a blunt trauma during sexual intercourse or otherwise, bending the penile shaft and causing a tear/rupture of the tunica albuginea, and tracking of blood from cavernosal sinuses into the subcutaneous plane.1 2 A urethral injury should always be ruled out by asking about any voiding difficulty, history of blood per meatus or haematuria. The diagnosis is usually clinical and requires prompt surgical intervention.3 Sometimes, the presentation may be occult and the patient may present with pain with or without swelling. Point of care ultrasound helps in confirming the diagnosis, aiding the surgeon to locate the site of incision with the least chance of neurovascular injury and skin necrosis. Ruptures of the dorsal penile artery and veins are the most common mimics of penile fracture, and can easily be ruled out by an ultrasound, thus avoiding negative exploration.
Learning points.
Penile fracture has a classical history and examination findings and should be identified and surgically explored at the earliest to avoid residual penile angulation, painful erections or erectile dysfunction.
Point of care ultrasound helps confirm findings and rules out other differentials.
Complete degloving of the penile shaft with its associated complications can be avoided by determining the exact site of tear, by preoperatively using point of care ultrasound.
Footnotes
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Zargooshi J. Penile fracture in Kermanshah, Iran: report of 172 cases. J Urol 2000;164:364–6. 10.1016/S0022-5347(05)67361-2 [DOI] [PubMed] [Google Scholar]
- 2.Eke N. Fracture of the penis. Br J Surg 2002;89:555–65. 10.1046/j.1365-2168.2002.02075.x [DOI] [PubMed] [Google Scholar]
- 3.Al-Shaiji TF, Amann J, Brock GB. Fractured penis: diagnosis and management. J Sex Med 2009;6:3231–40. 10.1111/j.1743-6109.2009.01593.x [DOI] [PubMed] [Google Scholar]