

Abstract
An 89-year-old woman with severe aortic valve stenosis and bradycardia presented with circulatory shock due to cardiac tamponade. We performed pericardiocentesis, and then diagnosed right ventricular perforation by echocardiography with microcavitation contrast medium just before inserting a drainage tube. We then inserted the drainage tube in the appropriate position and withdrew blood-filled fluid. The patient was haemodynamically stabilised, but haemorrhage from the perforation site continued for a few days. We injected fibrin glue into the pericardial space through the drainage tube and achieved haemostasis. Thus, we avoided surgery to close the perforation in this high-risk patient. There was no recurrence of haemorrhage. She subsequently had elective aortic valve replacement at another hospital. No adhesions in the pericardial space were seen during surgery.
Background
Cardiac perforation is a rare but major complication of pericardiocentesis. We diagnosed perforation by echocardiography with microcavitation contrast medium just before inserting a drainage tube. Although the perforation was minimal, bleeding continued for a few days. Injection of fibrin glue into the pericardial space, a minimally invasive procedure, produced haemostasis. In this case, the patient was of advanced age and had severe aortic stenosis. It is important to learn how to manage cardiac perforation in such high-risk patients.
Case presentation
An 89-year-old woman was transferred to our emergency department because of circulatory shock. She had severe aortic valve stenosis and bradycardia. Chest radiography showed cardiac dilation, and the cardiothoracic ratio was 70%. Transthoracic echocardiography showed a large pericardial effusion. We diagnosed cardiac tamponade. Pericardiocentesis was performed, and blood-filled fluid was aspirated just after the puncture. We suspected that the outer needle tip had reached the right ventricular cavity. Immediately, microcavitation contrast medium was carefully injected through the outer needle under observation by echocardiography. The right ventricular cavity was contrasted. A small amount of microbubbles leaked into the pericardial cavity (figure 1, video 1). We reattempted pericardiocentesis. The pericardial space was contrasted and the drainage tube properly inserted (figure 2, video 2).
Figure 1.
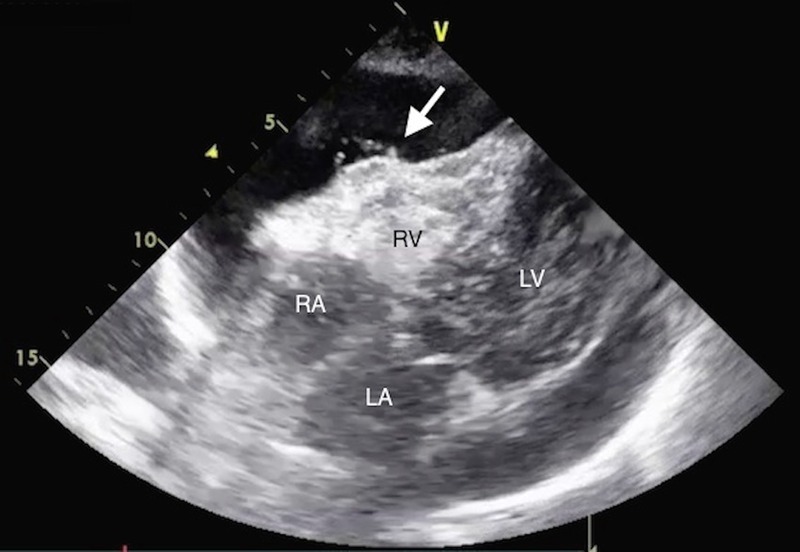
Diagnosis of right ventricular perforation using microcavitation contrast medium. Echocardiographic view of the epigastric area. Microcavitation contrast from the outer needle and right ventricle is injected. The white arrow indicates microbubbles that leaked into the pericardial cavity. RV, right ventricle; RA, right atrium; LV, left ventricle; LA, left atrium.
Figure 2.
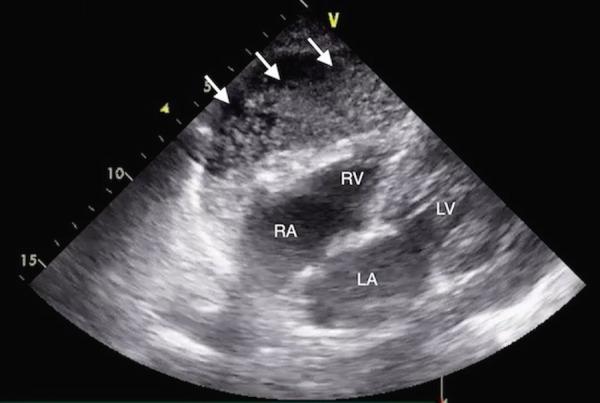
Microcavitation contrast method after second pericardiocentesis. Microcavitation contrast is injected after second pericardiocentesis. The pericardial cavity is contrasted. RV, right ventricle; RA, right atrium; LV, left ventricle; LA, left atrium.
Video 1.
Diagnosis of right ventricular perforation using microcavitation contrast medium. Echocardiographic view of the epigastric area. Microcavitation contrast from the outer needle and right ventricle is injected. The white arrow indicates microbubbles that leaked into the pericardial cavity. RV, right ventricle; RA, right atrium; LV, left ventricle; LA, left atrium.
Video 2.
Microcavitation contrast method after second pericardiocentesis. Microcavitation contrast is injected after second pericardiocentesis. The pericardial cavity is contrasted. RV, right ventricle; RA, right atrium; LV, left ventricle; LA, left atrium.
Treatment
Although the pericardial effusion was removed, it subsequently recurred, probably due to bleeding from the perforation. There was no improvement on observation for a few days, so we decided to inject fibrin glue into the pericardial space for haemostasis. We first confirmed the absence of intercommunication between the pericardial space and right ventricular cavity after injecting microcavitation contrast medium intravenously (figure 3, video 3), and then through the pericardial tube (figure 4, video 4). We injected fibrin glue through the pericardial tube after completely removing the pericardial fluid. No immediate pericardial effusion was noted, and haemostasis was achieved (figure 5, video 5).
Figure 3.
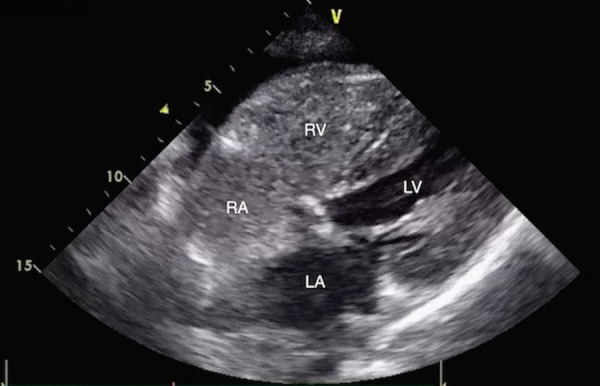
Assessment of intercommunication between the right ventricle and pericardial cavity. Microcavitation contrast is injected intravenously to assess intercommunication between the right ventricle and pericardial cavity. There is no leakage from the right ventricle into the pericardial cavity. RV, right ventricle; RA, right atrium; LV, left ventricle; LA, left atrium.
Figure 4.
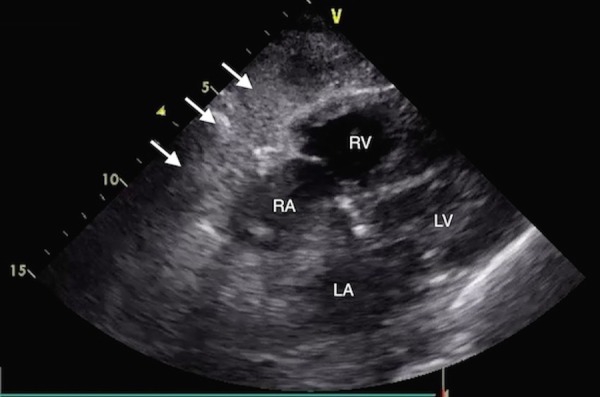
Assessment of intercommunication between the right ventricle and pericardial cavity. Microcavitation contrast is injected through the drainage tube to assess intercommunication between the right ventricle and pericardial cavity. There is no inflow from the pericardial cavity to the right ventricle (white arrow indicates the pericardial cavity). RV, right ventricle; RA, right atrium; LV, left ventricle; LA, left atrium.
Figure 5.

Echocardiography after percutaneous intrapericardial fibrin glue injection therapy. We injected fibrin glue into the pericardial space after removing almost all of the pericardial fluid. There was no recurrence of pericardial effusion. RV, right ventricle; RA, right atrium; LV, left ventricle; LA, left atrium.
Video 3.
Assessment of intercommunication between the right ventricle and pericardial cavity. Microcavitation contrast is injected intravenously to assess intercommunication between the right ventricle and pericardial cavity. There is no leakage from the right ventricle into the pericardial cavity. RV, right ventricle; RA, right atrium; LV, left ventricle; LA, left atrium.
Video 4.
Assessment of intercommunication between the right ventricle and pericardial cavity. Microcavitation contrast is injected through the drainage tube to assess intercommunication between the right ventricle and pericardial cavity. There is no inflow from the pericardial cavity to the right ventricle (white arrow indicates the pericardial cavity). RV, right ventricle; RA, right atrium; LV, left ventricle; LA, left atrium.
Video 5.
Echocardiography after percutaneous intrapericardial fibrin glue injection therapy. We injected fibrin glue into the pericardial space after removing almost all of the pericardial fluid. There was no recurrence of pericardial effusion. RV, right ventricle; RA, right atrium; LV, left ventricle; LA, left atrium.
Outcome and follow-up
No recurrence of pericardial effusion was noted over the next few days after injection of fibrin glue. The patient was transferred to another hospital on day 17. She was operated on for severe aortic valve stenosis electively, with no reported adhesions in the pericardial space at surgery.
Discussion
There is one case report describing the use of a microcavitation contrast method for the drainage of blood-filled pericardial effusion.1 This method proved that the drainage tube was properly placed in the pericardial space. We used this method because we observed blood-filled fluid, and diagnosed right ventricular perforation just before inserting a drainage tube. We thus avoided enlarging the perforation.
Haemostasis with fibrin glue injection into the pericardial space is used in oozing-type cardiac ruptures. There are some reports suggesting good outcomes.2–5 Some reports have shown that there were no subsequent adhesions in the pericardial space with echocardiography3 and cardiac MRI,4 nor at autopsy.5 Reiji H et al reported on the pharmacokinetics of fibrin glue in the pericardial space in a rat. A fibrin network was seen on day 1, and disappeared within 7 days with collagen fibre formation.6 In our case, the patient had severe aortic stenosis and underwent subsequent aortic valve replacement. Pericardial space adhesions were also not seen in our case.
Haemostasis with fibrin glue is minimally invasive compared with surgery. It is useful in critical patients and does not interfere with subsequent surgery.
Learning points.
Cardiac perforation is a rare but major complication of pericardiocentesis.
The microcavitation contrast method is useful to confirm the location of the needle tip and enables early diagnosis of cardiac perforation.
Percutaneous intrapericardial fibrin glue injection is effective in the treatment of cardiac perforation.
Footnotes
Contributors: HA, TM and NH were responsible for study conception and design; acquisition of data; analysis and interpretation of data. HA, TM and TO were responsible for drafting of manuscript and critical revision of the manuscript.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Miyamoto T, Watanabe S Obayashi T. Microcavitation contrast method for the drainage of bloody pericardial effusion. Circulation 2009;120:e166 10.1161/CIRCULATIONAHA.109.896563 [DOI] [PubMed] [Google Scholar]
- 2.Shuji J, Hidetsugu A, Masao S et al. Long-term usefulness of percutaneous intrapericardial fibrin glue fixation therapy for oozing type of left ventricular free wall rupture. Circ J 2002;66:705–6. 10.1253/circj.66.705 [DOI] [PubMed] [Google Scholar]
- 3.Terashima M, Fujiwara S, Yaginuma GY, et al. Outcome of percutaneous intrapericardial fibrin-glue injection therapy for left ventricular free wall rupture secondary to acute myocardial infarction. Am J Cardiol 2008;101:419–21. 10.1016/j.amjcard.2007.09.086 [DOI] [PubMed] [Google Scholar]
- 4.Okonogi T, Otsuka Y, Saito T. Repaired left ventricular free wall rupture after acute myocardial infarction by percutaneous intrapericardial fibrin-glue injection therapy. J Invasive Cardiol 2013;25:E186–7. [PubMed] [Google Scholar]
- 5.Hiroshi M, Masatoshi M, Hiroshi Y et al. Oozing type cardiac rupture repaired with percutaneous injection of fibrin-glue into pericardial space. Jpn Circ J 2000;64:312–5. 10.1253/jcj.64.312 [DOI] [PubMed] [Google Scholar]
- 6.Reiji H, Hajime O, Hideyasu O et al. Fate of fibrin sealant in pericardial space. Ann Thorac Surg 2000;70:2132–6. 10.1016/S0003-4975(00)02126-3 [DOI] [PubMed] [Google Scholar]