

Abstract
The increasing number of new cases of cancer highlights the relevance of primary prevention for cancer control, which is influenced, among other factors, by the population’s health-related knowledge. Therefore, we aimed to describe cancer-related knowledge in Portugal, including perception of risk, awareness of cancer causes and preventive behaviours. We evaluated 1624 Portuguese-speaking dwellers, aged between 16 and 79 years, through face-to-face interviews conducted using a structured questionnaire. We computed adjusted (sex, age, education) regression coefficients and prevalence ratios, using linear and Poisson regression, respectively, to quantify associations with cancer-specific knowledge. The proportions of nonresponse ranged from 13.4 to 63.5% for the most frequent cancer in Portugal and the leading cause of cancer, respectively. The mean of the estimated lifetime risk of cancer in the Portuguese population was 37.0%. A total of 47.5% of the respondents identified breast cancer as the most frequent in Portugal, 72.0% named lifestyles as the leading cause of cancer and 40.2% selected not smoking as the most important preventive behaviour. Lower levels of education were associated with higher proportions of nonresponse, but not consistently with inaccurate knowledge. Men provided lower estimates of the lifetime risk of cancer, indicated breast cancer less frequently and more often lung cancer as the most frequent, and were more likely to select not smoking as the most important preventive behaviour. The present study provides relevant data on knowledge of cancer prevention, which may be used for the planning and evaluation of awareness-raising and primary prevention interventions in Portugal.
Keywords: cancer, health knowledge, primary prevention
Introduction
Worldwide, more than 14 million new cases of cancer were diagnosed in 2012 (Ferlay et al., 2013), and the annual number of incident cancers is expected to reach 24 million in the next two decades, reflecting population ageing, trends towards earlier detection and increasing exposure to risk factors.
It is estimated that between a third and a half of all cases are preventable through reduction of modifiable exposures, including smoking, unhealthy diet, physical inactivity, alcohol consumption, infections or occupational hazards (Vineis and Wild, 2014). However, the translation of available evidence on the causes of cancer into preventive action will also depend on the population’s health-related beliefs, including the perception of susceptibility to the disease, as well as specific knowledge of its determinants and preventive measures (Sarafino and Smith, 2011).
This study aims to describe different aspects of health-related knowledge of cancer in the Portuguese population, including the perception of risk and knowledge of the leading causes of cancer and the main preventive behaviours.
Methods
The present analysis was based on a national survey conducted in 2012, aiming to assess knowledge and health behaviours of the Portuguese population aged between 16 and 79 years.
The study evaluated a representative sample of Portuguese-speaking dwellers in mainland Portugal. A stratified probabilistic sampling procedure was used to identify 150 geographical units, among which a total of 585 starting points were designated for the selection of households through standard random route procedures. All of the potentially eligible dwellers were identified in each selected household and only the one whose previous birthday was closest to the date of this contact was invited; a total of 1624 valid interviews were obtained (response rate: 70.8%). Participants were evaluated through face-to-face interviews conducted using a structured questionnaire.
Statistical analyses were carried out using STATA, version 11.1 (Stata Corp LP, College Station, Texas, USA). The associations between explanatory variables and cancer-related knowledge were estimated through adjusted (sex, age, education) regression coefficients or prevalence ratios (PR), with 95% confidence intervals (95% CI), using linear and Poisson regression, respectively. All estimates were weighted to be representative of the Portuguese population.
The survey was approved by the Ethics Committee of the University of Porto, and all participants provided written informed consent.
Results
The proportion of nonrespondents ranged from 13.4%, when participants were asked to select the most frequent cancer in Portugal (Fig. 1a), to 63.5%, when the leading cause of cancer was to be named (Fig. 1b). For all questions, the frequency of nonresponse decreased with education, and older participants were less likely to estimate the lifetime risk of cancer (P for trend=0.001).
Fig. 1.
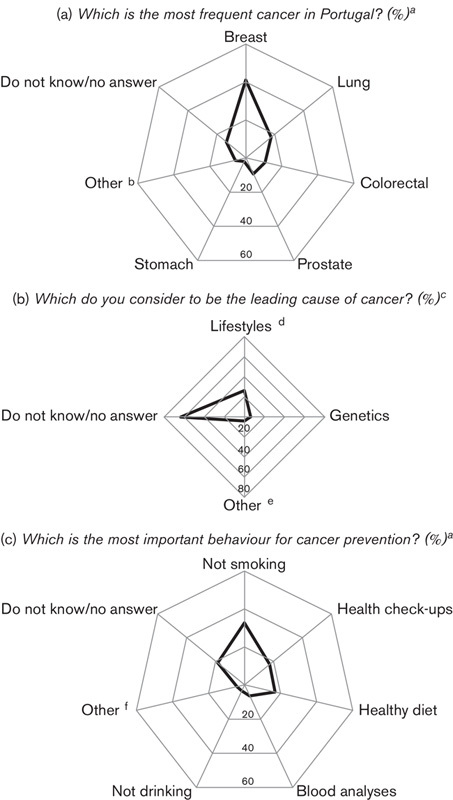
Knowledge of cancer frequency (a), leading cause of cancer (b) and behaviours for cancer prevention (c). aPercentage of participants selecting each option from a list of possible answers. bIncludes skin (melanoma), skin (with no other specification), liver, oesophagus, pancreas, leukaemia and ‘other’ cancers. cPercentage of participants naming each cause of cancer (open question), on the basis of a qualitative data analysis (thematic coding), defined to include the most frequent answers. dIncludes smoking, unhealthy diet, consumption of alcoholic beverages, sun exposure, overweight/obesity, lack of physical activity and other unhealthy lifestyles. eIncludes poor medical care, air pollution, exposure to chemicals or toxic products, consumption of medicines and other diseases. fIncludes doing regular physical activity, taking multivitamins, being weighed regularly, taking regular measurements of blood pressure and ‘other’ behaviours.
The mean estimate for the lifetime risk of cancer was 37.0%, being lower in men (β=−6.93, 95% CI: −10.74 to −3.12) (Fig. 2).
Fig. 2.
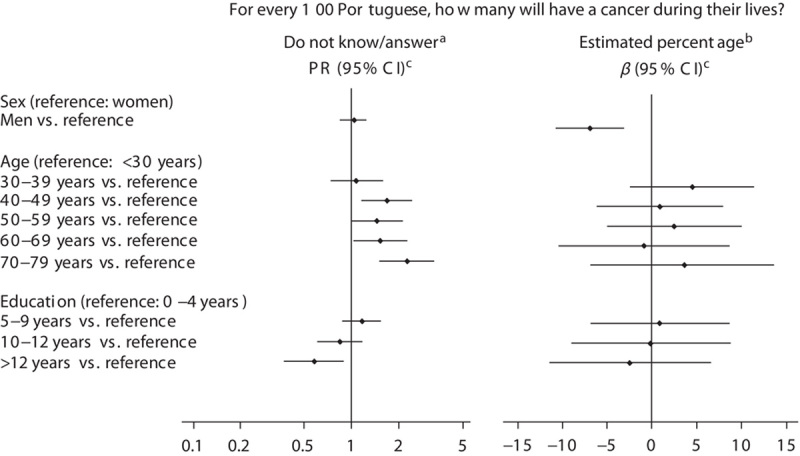
Perception of lifetime risk of cancer according to sociodemographic characteristics. aOverall, 33.7% of participants do not know/gave no answer. bDifference in the estimated percentage in relation to the reference category. cAdjusted for all variables in the figure. CI, confidence interval; PR, prevalence ratio.
Breast cancer was identified as the most frequent in Portugal (47.5% among respondents) (Fig. 1a). Men were less likely to mention breast cancer (PR=0.68, 95% CI: 0.56–0.81) and more likely to refer to lung cancer as the most frequent (PR=2.05, 95% CI: 1.49–2.82). The most educated participants referred to prostate cancer less often (>12 vs. 0–4 years: PR=0.36, 95% CI: 0.14–0.93).
In terms of the leading cause of cancer, lifestyles (mostly smoking) were the most frequently referred to (72.0% among respondents) (Fig. 1b). Those with higher educational levels were less likely to report lifestyles (>12 vs. 0–4 years: PR=0.71, 95% CI: 0.58–0.88) and more likely to mention genetics (>12 vs. 0–4 years: PR=3.37, 95% CI: 1.79–6.37). Reference to genetic causes increased with age, up to the 60–69 year age group.
Not smoking was identified as the most important preventive behaviour by 40.2% of the respondents (Fig. 1c). Men were more likely to select not smoking (PR=1.32, 95% CI: 1.08–1.60) and less likely to indicate having regular blood analysis (PR=0.51, 95% CI: 0.29–0.88). More educated participants (>12 vs. 0–4 years) were less likely to select not smoking (PR=0.65, 95% CI: 0.46–0.90) and having regular blood analysis (PR=0.37, 95% CI: 0.14–0.99), and more likely to choose a healthy diet (PR=1.58, 95% CI: 1.00–2.51) and having regular health check-ups (PR=2.11, 95% CI: 1.33–3.34). A more frequent reference to a healthy diet was observed with increasing age (P for trend=0.008).
Discussion
Our results show gaps in specific knowledge related to cancer and, therefore, a large potential for improvement, as observed previously (Adlard and Hume, 2003). However, the interpretation of these results is subjective and needs to consider that the different dimensions of cancer-related knowledge may have distinct implications for prevention efforts. For instance, compared with limited perception of the population’s risk, the high proportions of nonresponse or inaccurate answers in terms of preventive behaviours are likely to reflect more relevant gaps in knowledge.
Cancer is estimated to affect approximately one-quarter of the Portuguese population before age 75 (Ferlay et al., 2013), which is less than the estimated by the participants in our study, although the lifetime risk may be higher as the overall incidence of cancer further increases after 75 years of age. The use of an open-ended numeric scale may have inflated the estimates and contributed towards higher proportions of nonresponse (Woloshin et al., 1999). Our findings may also reflect the increasing number of survivors (Pacheco-Figueiredo et al., 2013), who may share their experience with others, and the negative perception of cancer by the general population. The sex differences observed may result from the fact that men are less likely to search for cancer-specific information (Rutten et al., 2006), despite having a higher risk of cancer (Ferlay et al., 2013).
Among the most frequent malignancies, breast cancer was identified as the most common in Portugal, which may reflect the existence of screening programmes and the large coverage of breast cancer by the mass media (Lewison et al., 2008).
The high proportion of participants identifying lifestyles as the leading cause of cancer or not smoking as the most important preventive behaviour, especially among men, is in accordance with the global efforts at tobacco control observed in Europe in the last few years, as well as with the higher prevalence of smoking in men (Carreira et al., 2012).
The increasing use of sophisticated technologies for the detection of asymptomatic diseases at early stages (Webster, 2002), as well as misconceptions on the effectiveness of some screening procedures, may have contributed towards blood analysis and regular check-ups being often identified as preventive behaviours, and may reflect a blurring of the boundaries between primary and secondary prevention.
Previous investigations have shown that more educated individuals were more likely to seek cancer-related information (Rutten et al., 2006), including about hereditary cancers, which is in accordance with the patterns observed in our study on the variation in cancer-related knowledge according to education.
Conclusion
The present study provides baseline data on health-related knowledge of cancer prevention, which may be used for the planning and evaluation of awareness-raising and primary prevention interventions in Portugal.
Acknowledgements
This work was supported by a grant from Fundação para a Ciência e a Tecnologia (HMSP-IISE/SAU-ICT/0004/2009).
Conflicts of interest
There are no conflicts of interest.
References
- Adlard JW, Hume MJ. (2003). Cancer knowledge of the general public in the United Kingdom: survey in a primary care setting and review of the literature. Clin Oncol (R Coll Radiol) 15:174–180. [DOI] [PubMed] [Google Scholar]
- Carreira H, Pereira M, Azevedo A, Lunet N. (2012). Trends in the prevalence of smoking in Portugal: a systematic review. BMC Public Health 12:958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, et al. (2013). GLOBOCAN 2012 v10, Cancer Incidence and Mortality Worldwide: IARC CancerBase No 11 [Internet]. Lyon, France: International Agency for Research on Cancer; Available at: http://globocan.iarc.fr. [Accessed 07 January 2014]. [Google Scholar]
- Lewison G, Tootell S, Roe P, Sullivan R. (2008). How do the media report cancer research? A study of the UK’s BBC website. Br J Cancer 99:569–576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pacheco-Figueiredo L, Antunes L, Bento MJ, Lunet N. (2013). Evaluation of the frequency of and survival from second primary cancers in North Portugal: a population-based study. Eur J Cancer Prev 22:599–606. [DOI] [PubMed] [Google Scholar]
- Rutten LJ, Squiers L, Hesse B. (2006). Cancer-related information seeking: hints from the 2003 Health Information National Trends Survey (HINTS). J Health Commun 11 (Suppl 1):147–156. [DOI] [PubMed] [Google Scholar]
- Sarafino EP, Smith TW. (2011). Health psychology: biopsychosocial interactions, 7th ed New Jersey, USA: John Wiley & Sons Inc. [Google Scholar]
- Vineis P, Wild CP. (2014). Global cancer patterns: causes and prevention. Lancet 383:549–557. [DOI] [PubMed] [Google Scholar]
- Webster A. (2002). Innovative health technologies and the social: redefining health, medicine and the body. Curr Sociol 50:443–457. [Google Scholar]
- Woloshin S, Schwartz LM, Black WC, Welch HG. (1999). Women’s perceptions of breast cancer risk: how you ask matters. Med Decis Making 19:221–229. [DOI] [PubMed] [Google Scholar]